
Abstract
Background
Surgical management of rotator cuff syndrome (RCS) is increasingly common in the world. After surgery, the return to work (RTW) process is often difficult for many patients, indicating the presence of factors that facilitate or delay this process.
Objective
To identify factors influencing RTW after rotator cuff (RC) surgery.
Methods
Articles regarding RTW after RC surgery were systematically searched via PubMed, Embase, and ScienceDirect databases. The review was performed according to the Joanna Briggs Institute (JBI) methodology for scoping reviews.
Results
Of the 323 initial studies, 21 were included in the final analysis. These data represented 5445 patients, the RTW rate was 80.72%, and the time to return was 6.23 ± 1.41 months. Several individual factors are associated with poorer RTW: female sex, dominant limb injuries, surgical complications, and mental health disorders. The workload was the occupational factor with the greatest influence on the RTW process. Heavy manual work and traumatic or load-handling injury had a negative influence, whereas sedentary work, repetitive motion injury and less strenuous work had positive influences. Patients under the workers’ compensation system were significantly associated with difficulty returning to work, but their return rates were not different.
Conclusions
There is no single factor that indicates the success of the RTW process within the evidence analyzed. On the contrary, several patient-related and work-related factors can positively or negatively influence this process. These findings are essential for understanding differences in RTW times among workers and for designing better return strategies.
Keywords
Introduction
Rotator cuff syndrome (RCS) affects millions of patients worldwide. 1 RCS includes shoulder impingement syndrome, subacromial bursitis, long head of the biceps tendinopathy, rotator cuff (RC) tendonitis, and partial and full RC tears.2,3 The prevalence of RC tears is estimated to be >10% in the general population of developed countries, and cause pain or disability of the shoulder that can lead to weeks or months away from work. 4 Long-term sickness absence often leads to unemployment and is a major predictor of all types of exits from the labor market, including disability pensions and early retirement. 5
The treatment of RCS starts with conservative management (anti-inflammatory drugs, physiotherapy, and intra-articular steroid injections), but in the most complex cases, it involves surgery and subsequent rehabilitation.6–8 After rehabilitation, the return to work (RTW) process begins when the patient is part of the economically active population. RTW is defined as a process that is intended to facilitate the workplace reintegration of workers who experience a reduction in work capacity, whether this is due to invalidity, illness, or aging. 5
Many factors have been shown to influence outcomes after surgery or noninvasive treatment of musculoskeletal disorders (MSDs). Longer waiting times to see a specialist or receive surgery are linearly related to chronic disability and lower rates of successful RTW. 9 Patients with anxiety or depressive disorders have worse outcomes after hip or knee surgery.10,11 After rotator cuff repair (RCR), several factors have been linked to patient dissatisfaction and low rates of RTW, including anatomic factors (tendon nonhealing), 12 clinical factors (persistent pain and loss of strength), 13 and occupational factors (labor-intensive occupation, private sector employed, workers’ compensation status).1,14
Patients under workers’ compensation (WC) claims usually have worse outcomes than patients with private insurance. In patients with RCR, these unsatisfactory results are related to persistent pain, complications after surgery, increased time off from work, and difficulties in performing full-duty RTW. 15 RTW in the WC population is expected within 6 months of shoulder injury because delays are associated with low return rates. 16 However, some workers remain permanently disabled and never return or return with work restrictions. Haunschild et al. 17 reported that 35% of patients are unable to return to their previous level of work after primary RCR. Under this panorama of uncertainty about RTW for employees and employers, a scoping review was carried out to understand the factors that influence the RTW process after RC surgery.
Methods
Methodological framework
This scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews, 18 and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist 19 was used to guide the reporting (see Appendix 1 of Supplementary material); a review protocol was not published. The research question was developed as a broad framing of the population (workforce with RC surgery), the concept (return-to-work) and the context (individual, clinical, and occupational factors) to be explored and mapped to the objective of the review. The broad research question for this review is: What are the factors that influence returning to work after RC surgery?
Eligibility criteria
The inclusion criteria to guide the assessment of each article were established in relation to the research question and the PCC framework. The articles included the following: (1) the population included workers of any age 18 + and any sex who received surgery as a treatment for RCS; (2) the primary research focused on RTW; and (3) the factors influencing the RTW process were described; the articles had to meet all three PCC criteria to be included. On the basis of these, articles were excluded if they (1) had no clear evidence of factor influence; (2) focused on return-to-play or return-to-sport; (3) were design studies such as reviews, commentaries, editorials, letters to the editor, case reports or animal studies; (4) were populations different from workers; (5) focused on treatments other than surgery; or (6) were full texts in languages other than English or Spanish.
Search strategy
The search strategy was formulated based on the application of the key terms “return to work [Mesh]” AND “rotator cuff [Mesh]”. Search was carried out in the following databases: PubMed, Embase and Science Direct from 16 October to 22 October 2024. The search was limited to the period from January 2014 until October 2024. The final search results were uploaded into Mendeley (Mendeley Ltd, Elsevier, The Netherlands), and duplicates were manually removed.
Data analysis
Microsoft Excel software was used to manage the data during the review and statistical analysis of the quantitative variables (see Appendix 2 and 3 of Supplementary material). The extracted data included participant information, the core concept, context, study methods, and other relevant findings for the analysis. After the data analysis was conducted, a PRISMA flow chart was generated to present the search strategy. There was no use of artificial intelligence (AI) in any phase of this study.
Results
The PRISMA flow chart summarizes the process of study selection (Figure 1). The search retrieved 323 articles from PubMed, Embase and ScienceDirect. After the titles and abstracts were reviewed, 283 (87.6%) studies were excluded on the basis of the exclusion criteria. A total of 40 (12.3%) articles underwent a full-text review after removing duplicates, 19 (5.8%) of which did not meet the inclusion criteria, leaving 21 (6.5%) for final analysis. All studies included in the review are summarized in Table 1. Appendix 2 of Supplementary material provides a full description of the studies included in this review.
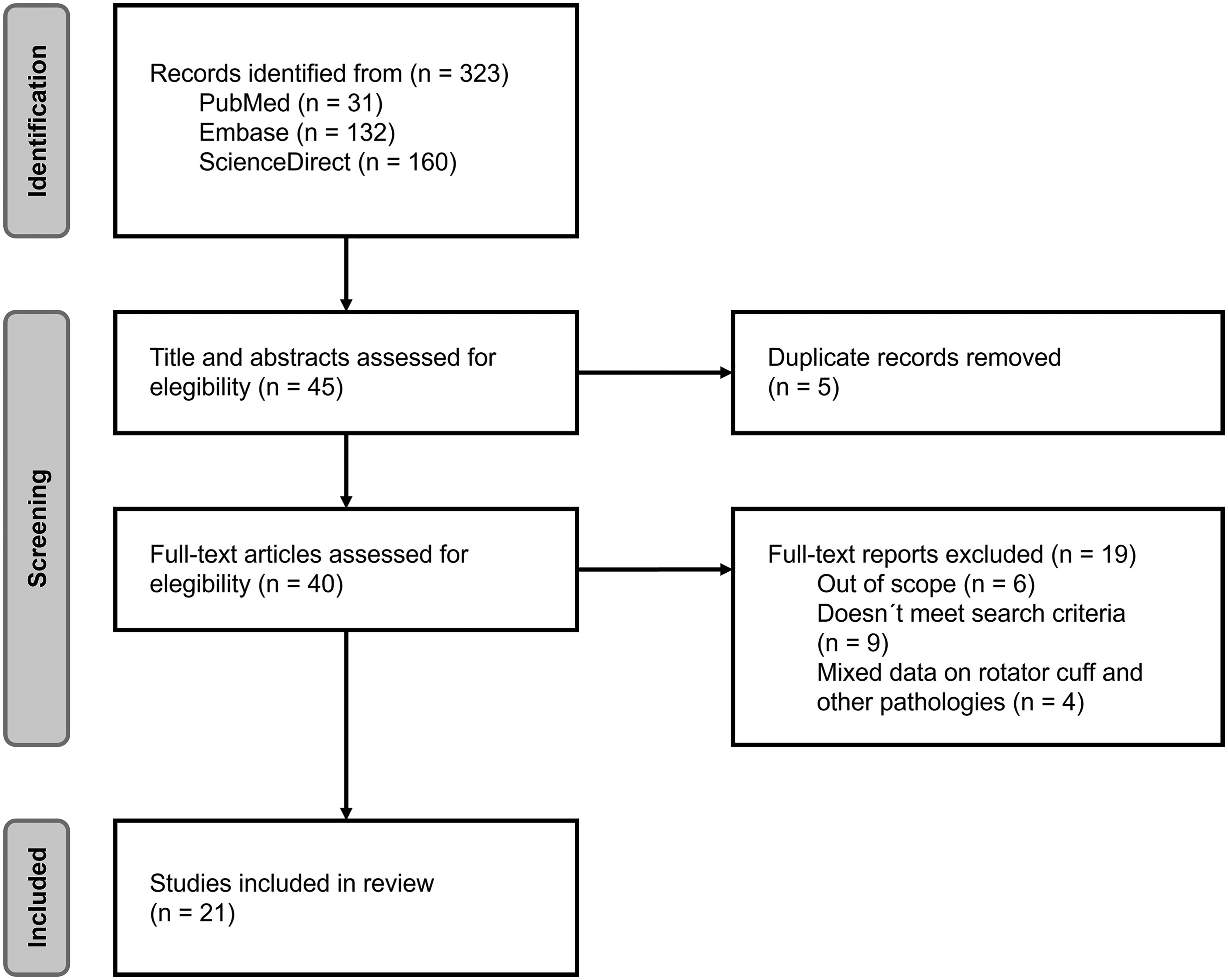
The preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow chart.
Data extraction chart organized by type of surgery.
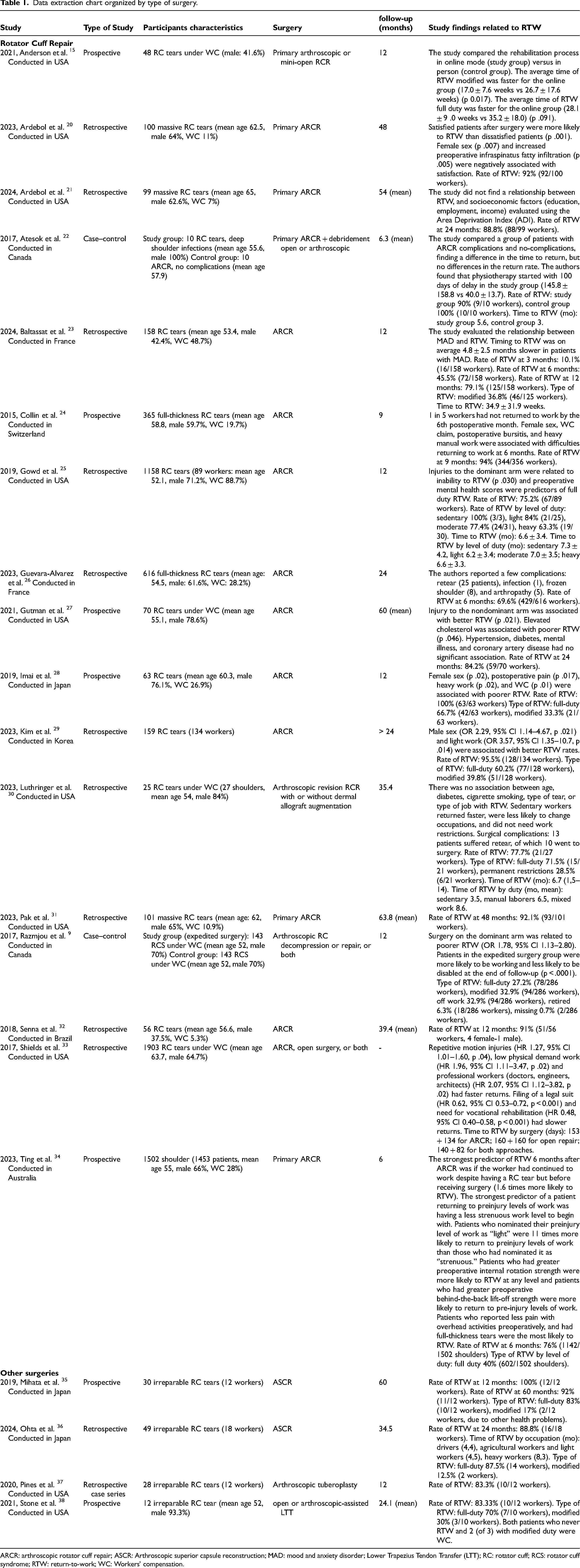
ARCR: arthroscopic rotator cuff repair; ASCR: Arthroscopic superior capsule reconstruction; MAD: mood and anxiety disorder; Lower Trapezius Tendon Transfer (LTT); RC: rotator cuff; RCS: rotator cuff syndrome; RTW: return-to-work; WC: Workers' compensation.
Characteristics of the studies
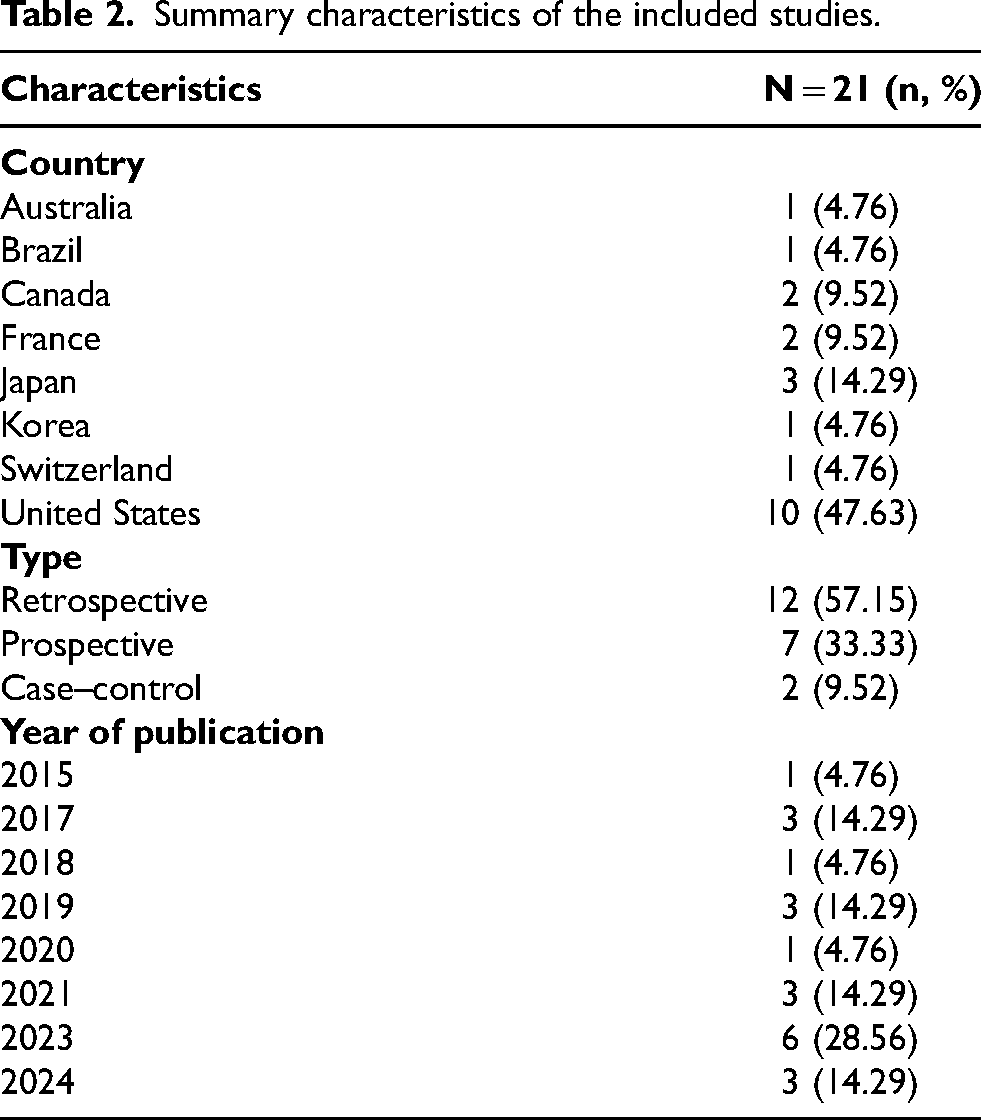
The studies were conducted in only eight countries (Figure 2), and the majority were conducted in health centers in the United States (n = 10), Japan (n = 3), Canada (n = 2), or France (n = 2). The other countries with one study each were Australia, Brazil, Korea, and Switzerland. The most common type of study was retrospective (57.15%, n = 12), and 61.90% (n = 13) were published in the last five years (2020–2024). Details about the studies (country, type, and year of publication) are provided in Table 2.
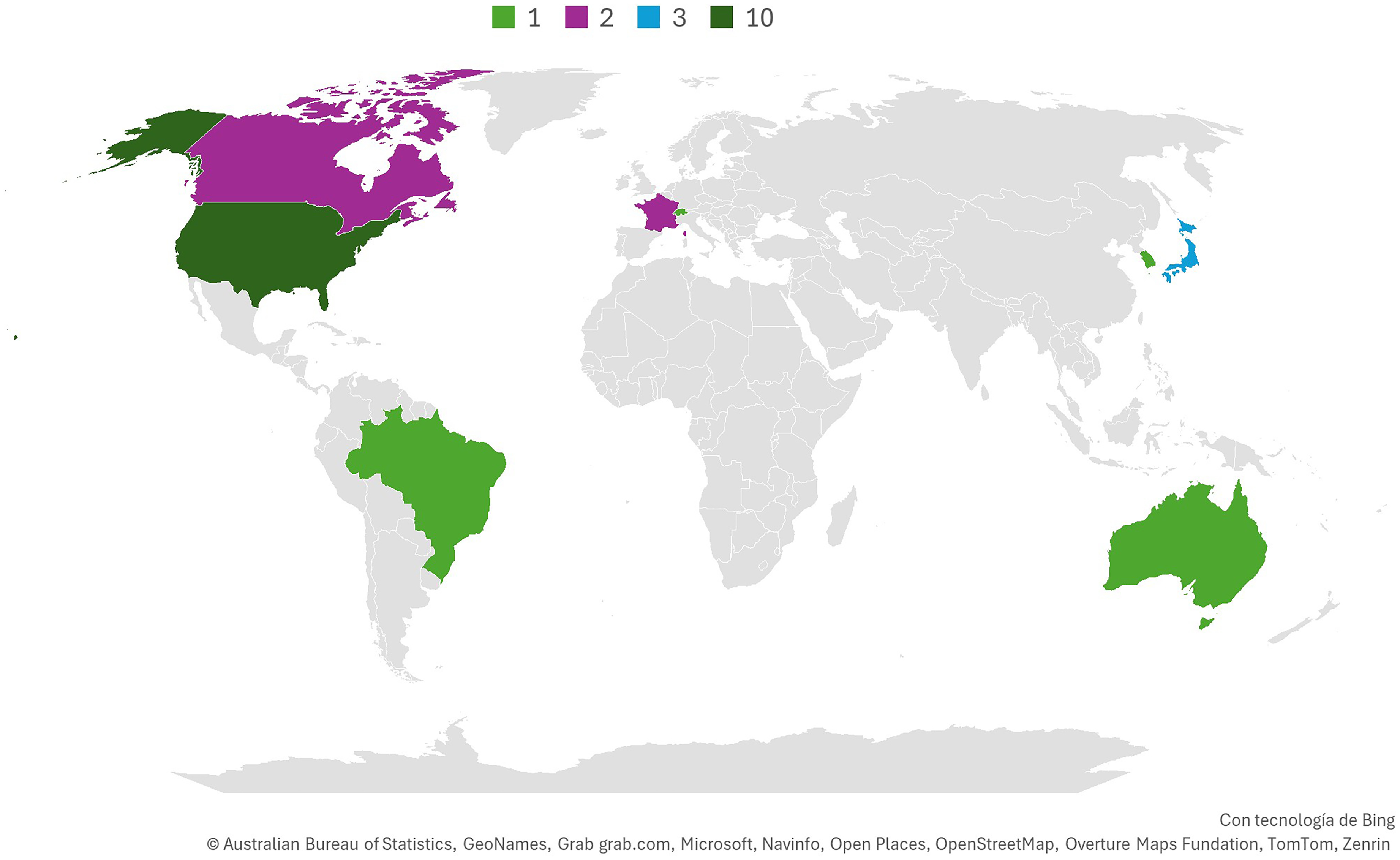
Geographical distribution of studies.
Summary characteristics of the included studies.
Global RTW data
Nineteen studies reported the number of workers who returned to work. A total of 2940 of 3642 workers returned at any time during the follow-up, indicating an overall RTW rate of 80.72%. However, the follow-up rates differed across investigations; the mean RTW rates at the 6th month,22,23,26,34 12th month22,25,28,32,35,37 and 24th month 21,27,29,36,38 were 80.0%, 88.10% and 88.76%, respectively (Figure 3).
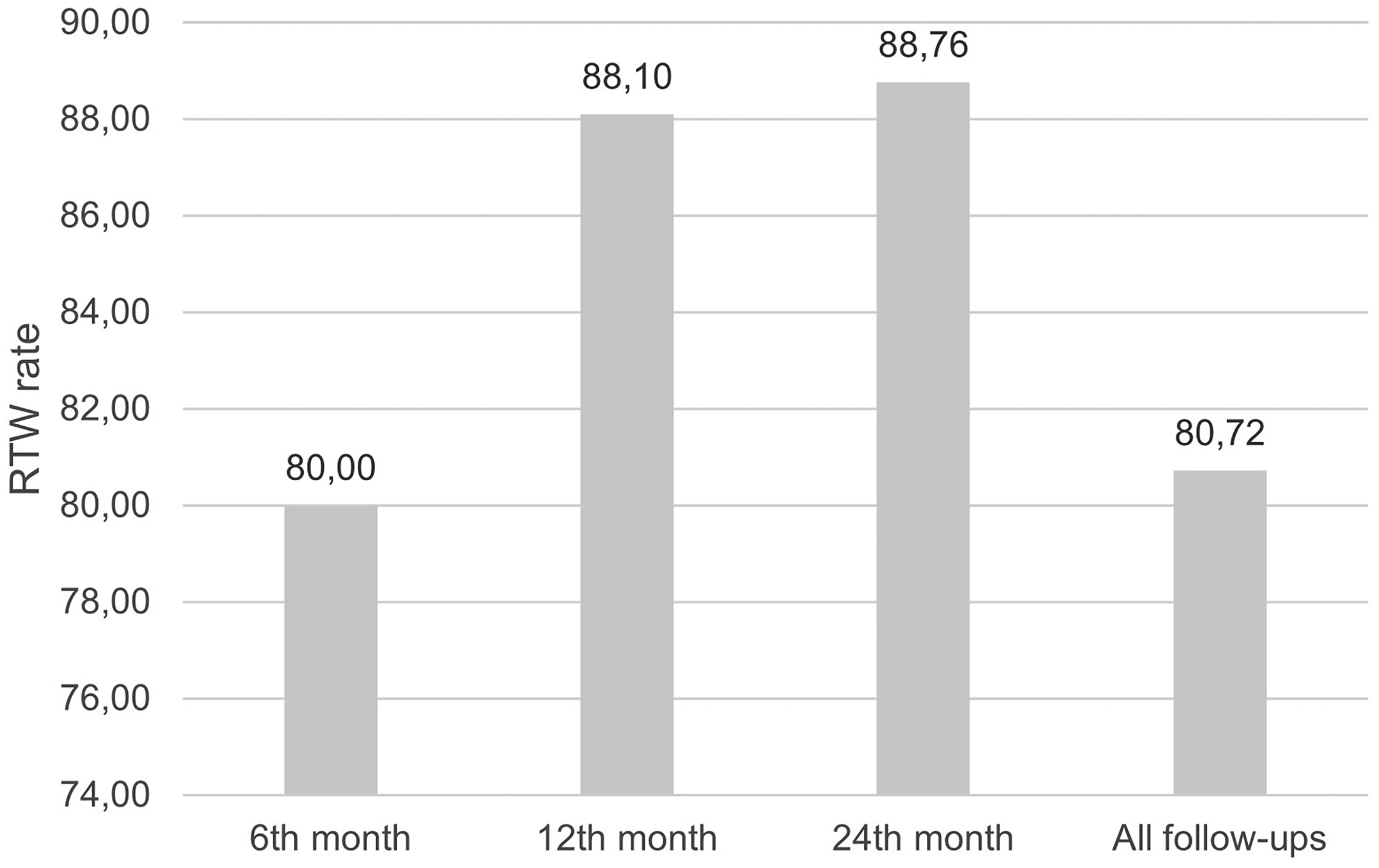
RTW rate for each follow-up period.
Data on time to RTW were standardized in months for analysis. Seven studies quantified these data15,22,23,25,30,33,36 and reported a minimum of 4.3 months and a maximum of 8.7 months, with an average of 6.23 ± 1.41 months for this group of workers (n = 3330).
Age and gender
The number of workers included in this review reached 5445. Among the studies that presented data on the sex of the workers, male sex was on average 66.96%; the sex of the workers could not be known in four studies29,35–37 because the data on the working population were part of the total number of patients. Two studies reported a relationship between female sex and difficulties with RTW,24,28 and Ardebol et al. 20 reported that female sex was negatively associated with satisfaction after surgery, a factor that increased the probability of RTW in their study. Kim et al. 29 reported that male sex workers had better rates of RTW (OR 2.29, 95% CI 1.14–4.67; p .021). The average age of the workers was 57.04 years (range: 52–65). None of the included studies reported a statistically significant association between age and RTW, but the Pearson coefficient showed a moderate positive correlation (0.64) in the data of this review.
Dominant side
Razmjou et al. 9 and Gowd et al. 25 reported that surgery on the dominant arm was significantly associated with lower RTW rates (p .030), whereas Gutman et al. 27 reported that injuries in the nondominant arm improved RTW rates (p .021).
Comorbidities
Diabetes, hypertension, and coronary heart disease are not associated with RTW.27,30 Gutman et al. 27 reported poorer RTW among workers with high cholesterol, and Baltassat et al. 23 reported that RTW was delayed by 4.8 ± 2.5 months among workers diagnosed with mood and anxiety disorders (MAD). In this research, heavy laborers with MAD had a 99% probability of returning to work 4 weeks late.
Type of RC tears and type of surgery
ARCR was the procedure chosen for surgery in 4467 shoulders. Other surgeries used to treat RC tears include open or mini-open RCR and arthroscopic decompression. In the case of irreparable RC tears, patients underwent arthroscopic superior capsule reconstruction (ASCR) (n = 30 patients), arthroscopic tuberoplasty (n = 12), or lower trapezius tendon transfer (LTT) (n = 12). The average RTW rate after ARCR (at the end of all follow-ups) was 86.46% (range: 69.9–100), and the average time to RTW was 6.6 ± 1.19 months. For irreparable RC tear surgeries, the RTW rate was 86.85%, and Ohta et al. 36 reported an average RTW of 5.7 months.
With respect to the type of tear, Ting et al. 34 reported that workers who had full-thickness tears were the most likely to RTW 6 months after primary ARCR and concluded that subscapularis function is important in the RTW process because workers who had greater behind-the-back lift-off strength were more likely to RTW (p .004). Razmjou et al. 9 evaluated the influence of expedited RC surgery on RTW. Workers in the expedited surgery group were more likely to be working and less likely to be disabled at the end of follow-up (p < .0001).
Postoperative complications
Atesok et al. 22 compared the RTW of workers with or without deep shoulder infections after ARCR. Compared with the control group, the infection group returned later (5.6 vs 3 months), underwent debridement surgery and experienced 100 days of delay in physiotherapy. Postoperative pain and bursitis are significantly associated with poorer RTW.24,28 Thirteen of 27 workers in the study by Luthringer et al. 30 and 25 of 616 in the study by Guevara-Alvarez et al. 26 had new ruptures, and some of them underwent new surgery, which implies prolonged RTW. Studies on irreparable RC have not reported postoperative complications.
Occupational factors
The studies reviewed show occupational factors with negative and positive influences on RTW (Table 3). Heavy manual work is associated with difficulty returning to work,24,28,29 whereas sedentary or low physical demand work is significantly associated with faster and less complicated returns to work.29,30,33,36 In the research of Ting et al., 34 the strongest predictor of a worker returning to pre-injury levels of work was having a less strenuous work level to begin after surgery. Gowd et al. 25 reported that heavy workers had lower return rates (63.3 vs 100%) and faster RTW times (6.6 ± 3.3 vs 7.3 ± 4.2 months) than sedentary workers did, but the findings were not statistically significant.
Occupational factors influencing RTW.
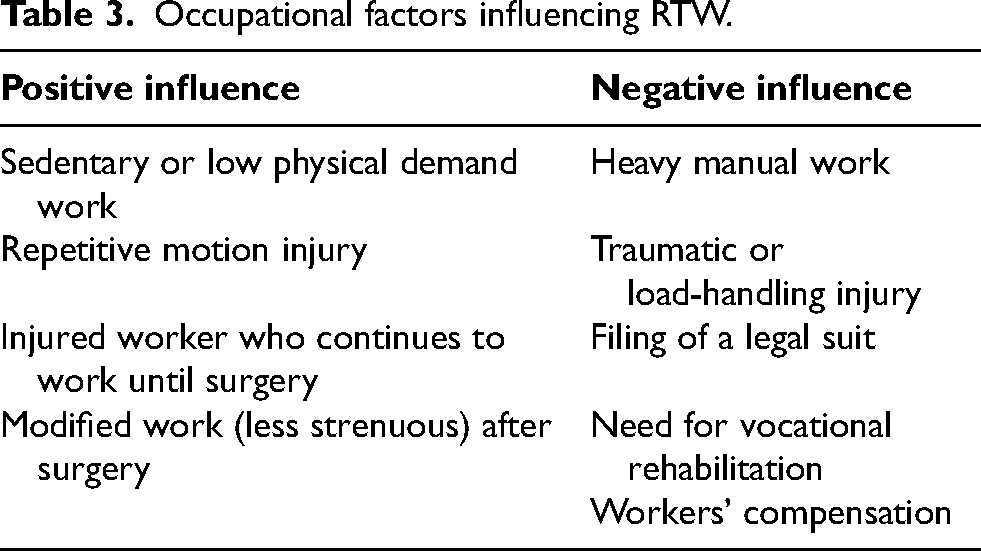
An important number of workers returned to work with modifications or permanent restrictions (mean 28.81%, range 12.5–39.8).9,23,29,30,35,36,38 Luthringer et al. 30 reported that sedentary workers were less likely to change occupations and did not need restrictions at work after surgery. Shields et al. 33 reported that repetitive motion injuries had better RTW rates than traumatic or load-handling injuries did (HR 1.27, 95% CI 1.01–1.60, p .04) in a cohort of 1903 patients, and filing a legal suit (HR 0.62, 95% CI 0.53–0.72, p < 0.0) or the need for vocational rehabilitation services (HR 0.48, 95% CI 0.40–0.58, p < 0.001) had slower returns. Ting et al. 34 reported that the strongest predictor of RTW 6 months after ARCR was whether the worker had continued to work before receiving surgery (1.6 times more likely to RTW).
Four studies9,15,27,30 included entire populations of workers under the WC system (n = 389). The RTW rate, obtained with data from two studies,27,30 was 80.9%, whereas the average return to work was 6.6 months.9,15 Only two studies24,28 reported that WC was significantly associated with difficulty returning to work.
Discussion
This scoping review aimed to report the overall factors that can influence the RTW process after RC surgery. For this purpose, this study reviewed the evidence reported in 21 primary studies and identified a complex network of individual and occupational factors that must be considered in the analysis of the RTW process. Notably, the RTW rate was 80.72%, which means that two of ten workers did not return to work. The surgical treatment of RCS usually has excellent RTW rates. Kalejman et al. 39 reported an RTW rate of 98.8% after ARCR, but Nové-Josserand et al., 40 in a cohort of 262 workers with work-related RC tears, reported that four out of ten were unable to RTW after surgery.
The average time to RTW was 6.2 months, a month later than that reported by Aagaard et al. 41 in a cohort of patients with traumatic RCS but similar to the 6.5 months to return-to-activities (RTA) reported by Kholinne et al. 42 in 1065 patients who underwent ARCR. However, it should be noted that RTW occurs long before maximum medical improvement (MMI) is achieved, which occurs approximately 12 months after RCR. 43 RTW should not occur long after surgery because longer times of absence of work are linked with lower rates of return, and early RTW has been associated with a successful return process. 44
In terms of patient factors, female sex, dominant shoulder injuries, and injuries in younger patients are related to poorer RTW. Chronic diseases were not associated with RTW in the studies reviewed, but Baltassat et al. 23 reported an association between mental disorders and delayed RTW. Several studies have shown the negative effects of mental health problems on shoulder surgery recovery.45–47 The diagnosis or feelings of depression or anxiety are related to worse outcomes after ARCR.48,49 This highlights the need to improve the management of patients with mental health disorders and RC tears when they undergo surgery.
ARCR was the most frequent surgery, but the RTW rates were similar for all types of procedures. Expedited surgery was significantly associated with better RTW rates. 9 In contrast to previous publications, complete tears were associated with better rates of return. Importantly, irreparable RC surgeries had RTW rates > 80%.
The workload is the occupational factor with the greatest influence on RTW. Manual workers and strenuous work before and after surgery had a negative influence on RTW, whereas sedentary workers returned faster and usually had no need for restrictions on full-duty returns. It is well known that manual workers have poorer outcomes after RCR, 50 and heavy manual labor is a risk factor for not returning to work or having prolonged RTW.51,52 Haunschild et al. 17 noted that the RTW rate improves when the workload decreases.
Other factors with a negative influence on RTW were identified: WC, lawsuits against the employer, and the need for vocational rehabilitation. WC was significantly associated with difficulty returning to work in two studies.24,28 Despite this, the time and rate of RTW among these workers were similar to those reported for all workers in the studies reviewed. Some authors have reported worse RTW rates and longer recovery times in WC vs non-WC patients,53,54 but Bhatia et al. 55 reported that 88.5% of workers under WC claims returned to their preoperative level of work at a mean time of 7.6 months after RCR, which was slightly longer than the findings of our study but with a high return rate.
The experts consulted by Peters et al. 44 also noted that other factors have an impact on RTW: the availability of job modifications and suitable duties, employers’ decisions regarding the availability of duties, fear of reinjury, and coworkers’ support. Those factors were not studied in the research reviewed.
Limitations
This research has several limitations that must be considered in the analysis of its results. First, the research was carried out in a small number of countries, located mostly in the northern hemisphere. The factors influencing RTW in other regions of the world could not be identified. Second, this review was limited to articles in English and Spanish. Research on RTW after RC surgery may have been conducted in other languages. Third, few investigations have provided specific information on workers’ occupation or the characteristics of the work, limiting themselves to classifying the work as light or heavy. This aspect was limiting in identifying the factors that influence the RTW of workers with specific professions, such as health professionals or drivers. Finally, as this is a scoping review, no quality assessment of the reviewed sources was conducted. Future systematic reviews and meta-analyses should examine the quality of studies based on primary study methodology.
Conclusions
This scoping review highlights the diverse landscape of factors influencing the RTW process after RC surgery, there is no single factor that indicates the success of the RTW process within the evidence analyzed. Several intrinsic patient factors, such as female sex, dominant limb injuries, surgical complications, and mental health disorders, negatively influence RTW. Within the work context, workload has a marked influence, such that the greater the workload is, the lower the return rates and the longer the RTW times. In contrast, light-duty workers, and sedentary workers, as well as manual workers who returned to work with a lower workload, returned more quickly and easily. Other factors that must be considered are the type of injury, time between injury and surgery, WC, filing of a lawsuit, and vocational rehabilitation. These findings are essential for understanding differences in RTW times among workers and for designing leans, worker-centered RTW processes and ultimately enhancing return rates among companies.
Supplemental Material
sj-pdf-1-wor-10.1177_10519815251353764 - Supplemental material for Factors influencing return to work after rotator cuff surgery: A scoping review
Supplemental material, sj-pdf-1-wor-10.1177_10519815251353764 for Factors influencing return to work after rotator cuff surgery: A scoping review by Luis Ignacio Lopez Michelena in WORK
Supplemental Material
sj-xlsx-2-wor-10.1177_10519815251353764 - Supplemental material for Factors influencing return to work after rotator cuff surgery: A scoping review
Supplemental material, sj-xlsx-2-wor-10.1177_10519815251353764 for Factors influencing return to work after rotator cuff surgery: A scoping review by Luis Ignacio Lopez Michelena in WORK
Footnotes
Ethical considerations
This study, as a scoping review, is exempt from Institutional Review Board approval.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.