
Abstract
Background
Work disability due to musculoskeletal and mental health disorders constitutes one of the greatest social and labor market challenges. There is a need to investigate the long-term impact of interventions provided to employees.
Objective
To investigate if a brief work-oriented intervention targeting musculoskeletal and mental health disorders affected the risk of work disability.
Methods
A prospective study using national register data was designed. The intervention group consisted of all patients (n = 6348) who in the years 2008–2017 participated in a brief intervention at an outpatient clinic in the secondary health care service. The comparison group (n = 25,354) consisted of employees sick-listed for musculoskeletal or mental health disorders in the same years as the intervention group. Cox proportional hazard regression was used to model the effect of the intervention on the risk of future disability pension. Overall and subgroup analyses for gender and diagnoses were conducted for various categories of full-time equivalent number of days lost to work.
Results
Generally, there was a pattern of increased risk of disability among patients in the intervention group if they participated in the intervention in an early phase of sick leave. This pattern was found in the overall analysis, for males, females, and patients with musculoskeletal disorders. Except for patients with only musculoskeletal disorders, there was a pattern of reduced risk of disability with sick leave of between three and six months.
Conclusions
Overall, the intervention did not reduce the risk of disability. However, the results do indicate that intervention timing may be of significance.
Introduction
Work disability due to musculoskeletal and mental health disorders constitutes one of the greatest social and labor market challenges across the Organisation for Economic Co-operation and Development (OECD) countries.1,2 In Norway, 11% of the working-age population receive disability benefits, 3 with mental health disorders as the most common primary diagnosis for being granted disability pension (DP), followed by musculoskeletal disorders. 4 A significant proportion of these disorders are likely to represent common subjective health complaints, such as unspecific back pain, tiredness, and anxiety and depression complaints. 5 These may in time have turned into chronic and intolerable conditions affecting employees’ work ability.6,7 In addition to the economic cost for society, 8 and the fact that organizations are experiencing production constraints due to labor shortage, 9 work disability has large consequences for the individual (e.g., increased morbidity and mortality rates and reduced quality of life).10–13 It is of foremost importance to prevent the transition from short-term sick leave (SL) to long-term or permanent disability, both from a societal, organizational, and individual perspective.
Work is generally healthy and the positive effects of work are usually larger than any negative health effects.14–16 The risk of permanent labor market exclusion increases for persons on SL, and it is argued that with longer SL it becomes less likely for that person to return to work.17–19 Access to effective treatment in the early phase of SL, or even before SL is needed, may be a way to prevent work exclusion. Data from the Norwegian population-based HUNT-2 study, published in 2007, indicated that around one-third of persons receiving DP for mental health disorders never had sought treatment for their mental health problems. 20 The authors highlighted the need for improved access to treatment, 20 and improved access to treatment for employees with health complaints was at the heart of the agenda when the Norwegian government, in 2007, launched the national “Rapid return to work” (RRW) project. The project involved closer monitoring of SL practices and focused on quick referral from primary to secondary healthcare, thereby aiming to prevent the transition from short-term to long-term SL or permanent work exclusion. Several outpatient clinics were established in the secondary healthcare service to accommodate this aim.
The outpatient clinic and intervention investigated in the current study was a part of this government-initiated and financed RRW project. It provided rapid clarification and healthcare for employees experiencing musculoskeletal and mental health disorders, aiming to prevent the transition from acute/sub-acute and tolerable complaints to chronic and intolerable complaints with long-term negative effects on work ability. Even though the RRW project mainly focused on reducing SL, it is reasonable to assume that rapid clarification and treatment for employees experiencing musculoskeletal and/or mental health disorders may contribute to preventing work disability. As prevention of work disability is an important public health goal, there is a need to investigate the long-term impact of interventions provided to employees. Furthermore, the initiatives that focused on musculoskeletal and mental health disorders in the RRW project, were integrated into the standard operations of Norwegian secondary health care institutions after the project period, leading to the establishment of “Health and Work” clinics. The “Health and Work” clinics continue to offer interventions to the same patient groups, and examining the initiative's potential impact on work disability is of current interest. By utilizing national register data on patients receiving a brief work-oriented intervention during the defined RRW project period, the study aims to examine if the provided intervention affected work disability.
Methods
Study design and data collection
This prospective study used national register data, obtained from the Norwegian National Insurance Administration (NAV). This national database includes information on all physician-certified SL and grants of DP, and is essential for the reimbursements paid by NAV. In addition to recurrent and longitudinal data on SL-episodes and DP, the dataset included demographic information on age, gender, ICPC-diagnosis for SL, and occupation.
Sample
The intervention group consisted of all patients (n = 6348) who in the ten-year RRW project period (2008–2017) were enrolled at the RRW outpatient clinic at Vestfold Hospital Trust. Patients were identified through the clinical register at the outpatient clinic. Register data on SL and DP were linked to patients using the 11-digit personal identification number in Norway 21 and extracted from the national register database by NAV.
For each patient in the intervention group, NAV was asked to identify four comparators (i.e., 1:4 ratio) from the national register (a treatment as usual group, i.e., not receiving the investigated RRW intervention). The selection of comparators was based on calendar year of intervention enrollment for patients in the intervention groups, in addition to musculoskeletal or mental health disorders as the SL diagnoses. Year of enrollment to the intervention was chosen as reference to obtain comparators who were most likely to be in a similar situation as the patients in the intervention group, in the same period. The ICPC diagnoses for SL were used to only include comparators who matched the focus of the intervention (musculoskeletal or mental health disorders). As we did not have data to perform a propensity score matching on severity of complaints, we constructed categories of days lost to work in the year prior to and the year of the intervention, used in the analyses, to adjust for differences in sick leave length, and potential severity of complaints, between groups. The total sample of comparators consisted of 25,354 sick-listed individuals.
Intervention
The RRW outpatient clinic provided a work-oriented intervention aiming to contribute to better health and work ability among employees experiencing musculoskeletal and/or mental health disorders. It differed from traditional work rehabilitation programs by applying a brief intervention (BI), focusing on rapid clarification. The BI approach, where common health complaints are viewed as a normal part of life and rarely a sign of injury or “harmful” behavior, has been superior in facilitating return to work compared to more comprehensive interventions both when targeting back pain 22 and mental health disorders. 23
The main focus of the BI at the RRW outpatient clinic was to normalize common health complaints and increase patients’ health literacy (HL) to facilitate coping. Coping was defined as a positive response outcome expectancy, the belief that your actions will lead to a positive result, as described in the Cognitive Activation Theory of Stress (CATS). 24 Positive response outcome expectancies are developed through learning and experiences, 24 and through normalization, health education, and guidance the BI approach aimed to strengthen patients’ positive response outcome expectancies regarding their health complaints and work ability. A non-directive communication approach25,26 was applied to support patients’ autonomy and reinforce confidence in their capacity to discover and implement solutions to their challenges. On this foundation, the BI intended to influence patients’ behavior and reduce long-term negative consequences, such as sick leave and work disability.
The intervention took place in the secondary health care service, at an outpatient clinic with multidisciplinary staff, involving medical doctors, physiotherapists, psychologists, and health educators. Patients were referred to the clinic after medical examination by their general practitioner, or other health professionals with referral rights (e.g., chiropractor). The intervention was organized in a flexible and patient-centered manner and involved both individual and group sessions. Based on the patients’ preferences they could choose individual examination/guidance by a physiotherapist or a medical doctor (1–2 h) or individual brief psychotherapy sessions with a psychologist (4–6 h). All patients referred to the intervention were thoroughly examined to rule out serious pathology. 5 All patients were recommended to participate in a health education course (4 h), focusing on debunking common myths about musculoskeletal and mental health disorders and how to cope with their work and health situation. Patients who needed additional follow-up could choose to participate in a mastery-oriented guidance course (20 h), followed by individual guidance sessions if needed (2–6 h). Although individual adjustments were made, some core elements were consistent across the different sessions and courses: normalizing symptoms, increasing HL, creating confidence in the ability to produce a positive result, and enhancing awareness of resources, possibilities, and the importance of work for health.
Outcome variable
Disability pension status
Disability pension status represents the occurrence of DP in the NAV-database among employees in the study population and includes both partial and full-time disability. The criterion for awarding DPs in Norway is an application stating cause-specific and lasting reduced functional ability due to an acknowledged medical condition, contributing to at least 50% permanent reduced earning capacity. 27 The records are highly accurate as correct registration is essential for reimbursement from NAV.
Explanatory variables
Full-time equivalent number of days lost to work
Full-time equivalent (FTE) number of days lost to work represents the integer number of SL days, adjusted for percentage of full-time position and SL rate. The FTE days will hence be less than the number of SL days, but still between 0 and 365 days. For individuals with less than 1 day of FTE, FTE was set to 0. For analytic purposes, FTE days for the year prior to enrollment and the intervention year was categorized as 0–29, 30–89, 90–181, and 182–365 days.
Sick leave days
SL days represent the number of days absent from work. Normally, SL shorter than 16 days is not registered in the NAV register (the employer pays for the first 16 days of SL). For SL periods of more than 16 days, the total days of SL, including the first 16 days, is registered. SL days for patients at the outpatient clinic range from 0 (i.e., those not yet on SL) to 365 days. For the comparators SL days ranged from 1 to 365 since these were identified from the NAV register. As for FTE days, SL for the year prior to enrollment and the intervention year was categorized as 0–29, 30–89, 90–181, and 182–365 days and used in the analyses.
Age and gender
Age at time of enrollment (continuous variable) and sex (male/female obtained as part of the national identification number) were available for all individuals.
Sick leave diagnosis
Diagnoses represent the SL diagnoses (musculoskeletal (L) or psychological (P), set according to the International Classification of Primary Care (ICPC)) registered for each of the available SL episodes in the intervention year and the preceding year.
Occupation
Occupation was registered according to the Standard Classification of Occupations (ISCO-08) 28 and obtained from the State Register of Employers and Employees. The occupation registered at time of inclusion in the study was used for the analyses. First, the occupational codes were organized into ten categories, based on ISCO-08 major group classification (1. Managers, 2. Professionals, 3. Technicians and Associate Professionals, 4. Clerical Support Workers, 5. Services and Sales Workers, 6. Skilled Agricultural, Forestry and Fishery Workers, 7. Craft and Related Trade Workers, 8. Plant and Machine Operators, and Assemblers, 9. Elementary Occupations, 10. Armed Forces Occupations). 28 Four main categories were then defined for use in the analyses. The four categories were managers/professionals (ISCO major groups 1 and 2), associate professionals (ISCO major group 3), routine non-manual (ISCO major groups 4 and 5) and manual (ISCO major groups 6, 7, 8, and 9). None of the participants had Armed Forces Occupations at time of inclusion.
Statistical analysis
Descriptive analyses were performed, providing proportions for categorical variables and mean and standard deviation (SD) values for continuous variables. Hazard Ratios (HR), with 95% confidence intervals (CI), were estimated using Cox proportional hazard regression to model the effect of the intervention on the risk of DP. Number of FTE days in the year prior to and the year of the intervention was categorized into four groups, 0–29 days, 30–89 days, 90–181 days, and 182–365 days, and used in the Cox regression analyses. Overall analyses, providing both unadjusted and adjusted HRs (adjusted for age, gender, occupation, and diagnosis) for each category of FTE days, were performed. In addition, subgroup analyses for gender and diagnoses were conducted. To study if there were non-linear effects of the RRW intervention, functional form of the effect of the RRW was constructed. In these analyses, HRs are presented as curves from Generalized Additive Cox Models (GAMs) with 95% confidence intervals (CIs). Since the risk for DP increases with increasing days of SL (i.e., FTE), the excess effect of the RRW over the duration of FTE, was estimated as an interaction term between FTE-days and RRW, in a model also including the main effect of FTE-days. GAMs stratified by gender and diagnoses were also created. The statistical analyses were performed using STATA version 18.0 (Stata Corp, College Station, TX, USA) and R version 4.2.2 (R Foundation for Statistical Computing). P-values less than 0.05 were considered statistically significant.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. 29 Approval was granted by the Regional Committee for Ethics in Medical Research (02.12.2021/REK sør-øst D, 283547) and the Norwegian Social Science Data Services (01.11.2021/NSD, ID 306154). Dispensation from the obligation of confidentiality has been granted for the provision and use of health information during the implementation of the project based on the Health Personnel Act §29 first paragraph, cf. regulation of 27 May 2021 no. 1725.
Results
Characteristics of study participants, stratified by group (intervention and comparison) are presented in Table 1. Mean age of the patients who received the RRW intervention was 41 years, approximately two-thirds were women, and about half had lower education occupations (manual and routine non-manual). About half of the patients in the intervention group had SL due to mental health disorders, while in the comparison group, musculoskeletal disorders were the most prevalent SL diagnosis (74%). Compared to the intervention group, the comparison group had significantly fewer SL days and FTE days lost to work the year before inclusion and the intervention year (Table 1). All further analyses were thus performed for categories of FTE days.
Characteristics of the study population, stratified by group.
At time of inclusion.
Persons sick-listed with musculoskeletal or mental disorder the year before inclusion and the intervention year.
Sum of full-time equivalent number of days lost to work the year before inclusion and the intervention year.
Sum of days of sick leave the year before inclusion and the intervention year.
Overall
In the unadjusted Cox regression analyses, patients in the intervention group with 0–29 FTE days lost to work had an increased risk of DP (HR = 1.58, p < 0.001) compared to persons with equal FTE days lost to work in the comparison group. Patients in the intervention group with 90–181 FTE days lost to work had a reduced risk of DP (HR = 0.71, p < 0.001) compared to the comparison group. In the adjusted Cox regression analyses, patients in the intervention group with 0–29 and 30–89 FTE days lost to work had an increased risk of DP (HR = 1.85, p < 0.001 and HR = 1.34, p = 0.006 respectively) compared to persons with equal FTE days lost to work in the comparison group (Table 2 and Figure 1).
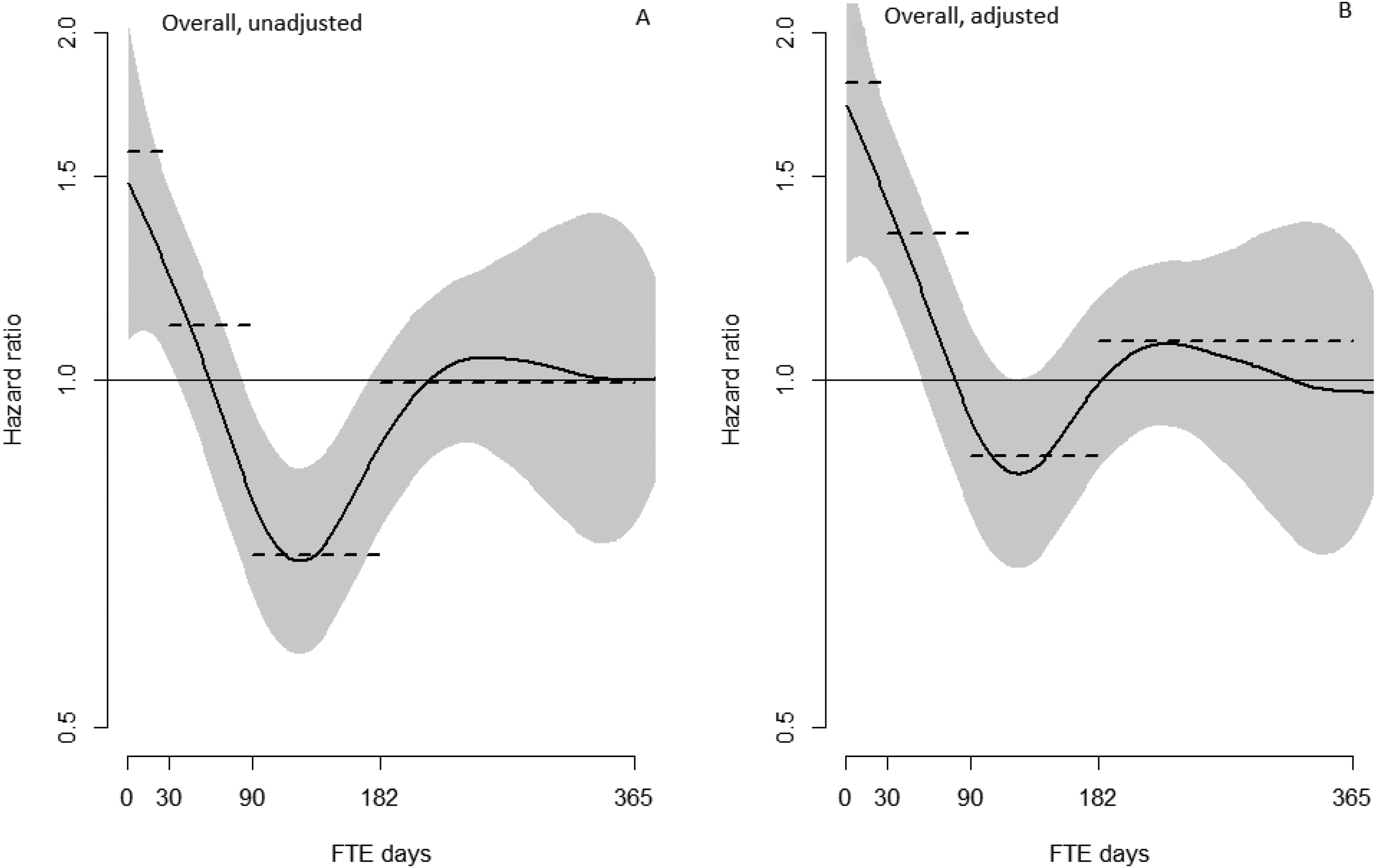
Generalized additive cox model curves demonstrating the intervention group's risk of disability pension, compared to the comparison group, as a function of full-time equivalent (FTE) days lost to work in the year before inclusion and the intervention year. BAdjusted for age, gender, occupation, and diagnosis. Grey bands represent 95% confidence intervals. Dotted lines represent the hazard ratios from the Cox-regression analysis.
Risk of disability pension (HRs and 95% CIs) among patients in the intervention group compared to the comparison group, for different categories of full-time equivalent (FTE) number of days lost to work the year before the intervention and the intervention year.
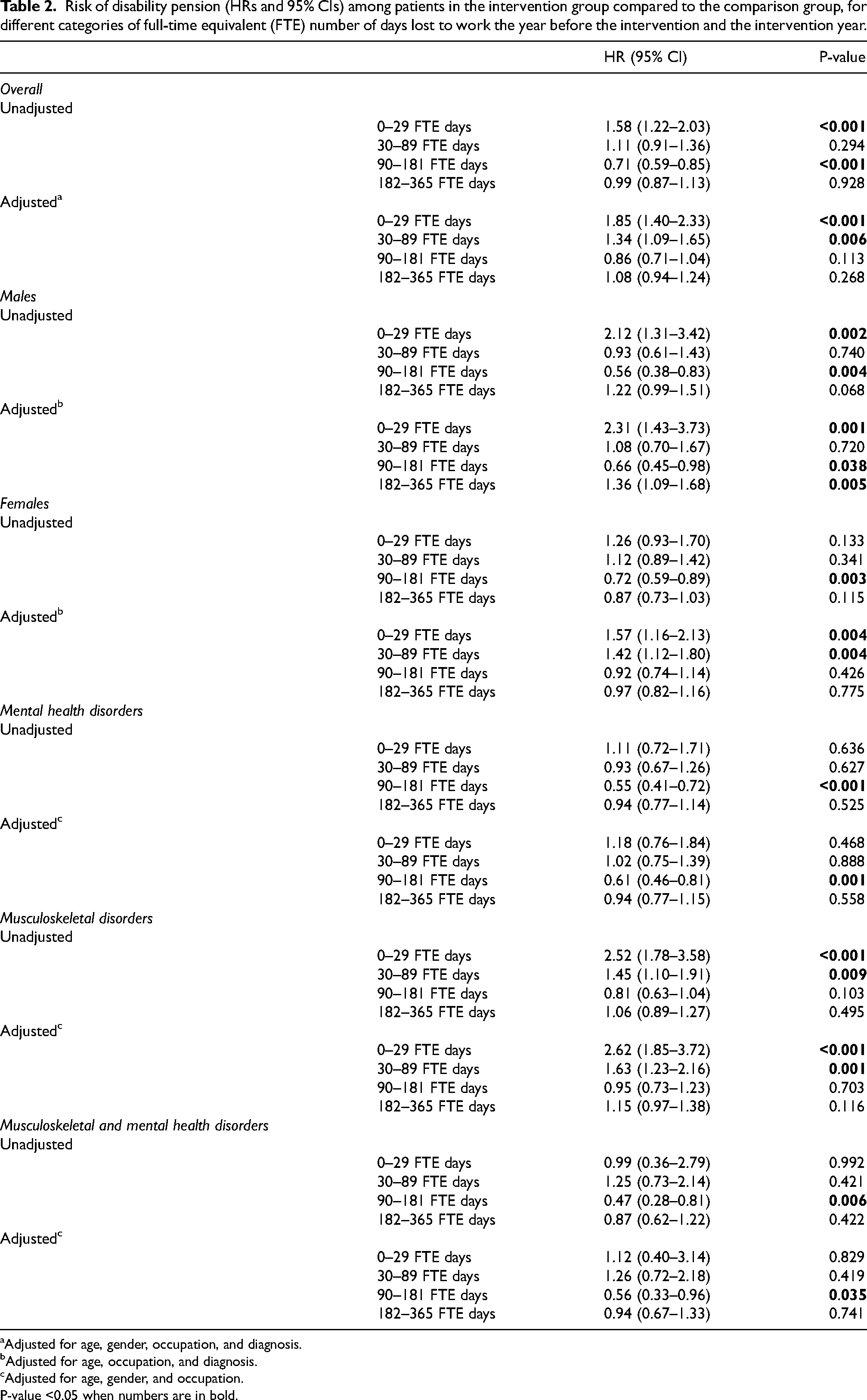
Adjusted for age, gender, occupation, and diagnosis.
Adjusted for age, occupation, and diagnosis.
Adjusted for age, gender, and occupation.
P-value <0.05 when numbers are in bold.
Gender
In the unadjusted analyses, men in the intervention group with 0–29 FTE days lost to work had an increased risk of DP (HR = 2.12, p = 0.002) and men with 90–181 FTE days lost to work had a reduced risk of DP (HR = 0.56, p = 0.004) compared to men with equal FTE days lost to work in the comparison group. The adjusted analyses followed the same pattern but also showed that men in the intervention group with 182–365 FTE days lost to work had an increased risk of DP (HR = 1.36, p = 0.005) compared to men with equal FTE days lost to work in the comparison group. For females, the unadjusted analyses showed that women in the intervention group with 90–181 FTE days lost to work had a reduced risk of DP (HR = 0.72, p = 0.003) compared to women with equal FTE days lost to work in the comparison group. In the adjusted analyses, women in the intervention group with 0–29 and 30–89 FTE days lost to work had a higher risk of DP (HR = 1.57, p = 0.004 and HR = 1.42, p = 0.004 respectively) compared to women with equal FTE days lost to work in the comparison group (Table 2 and Figure 2).
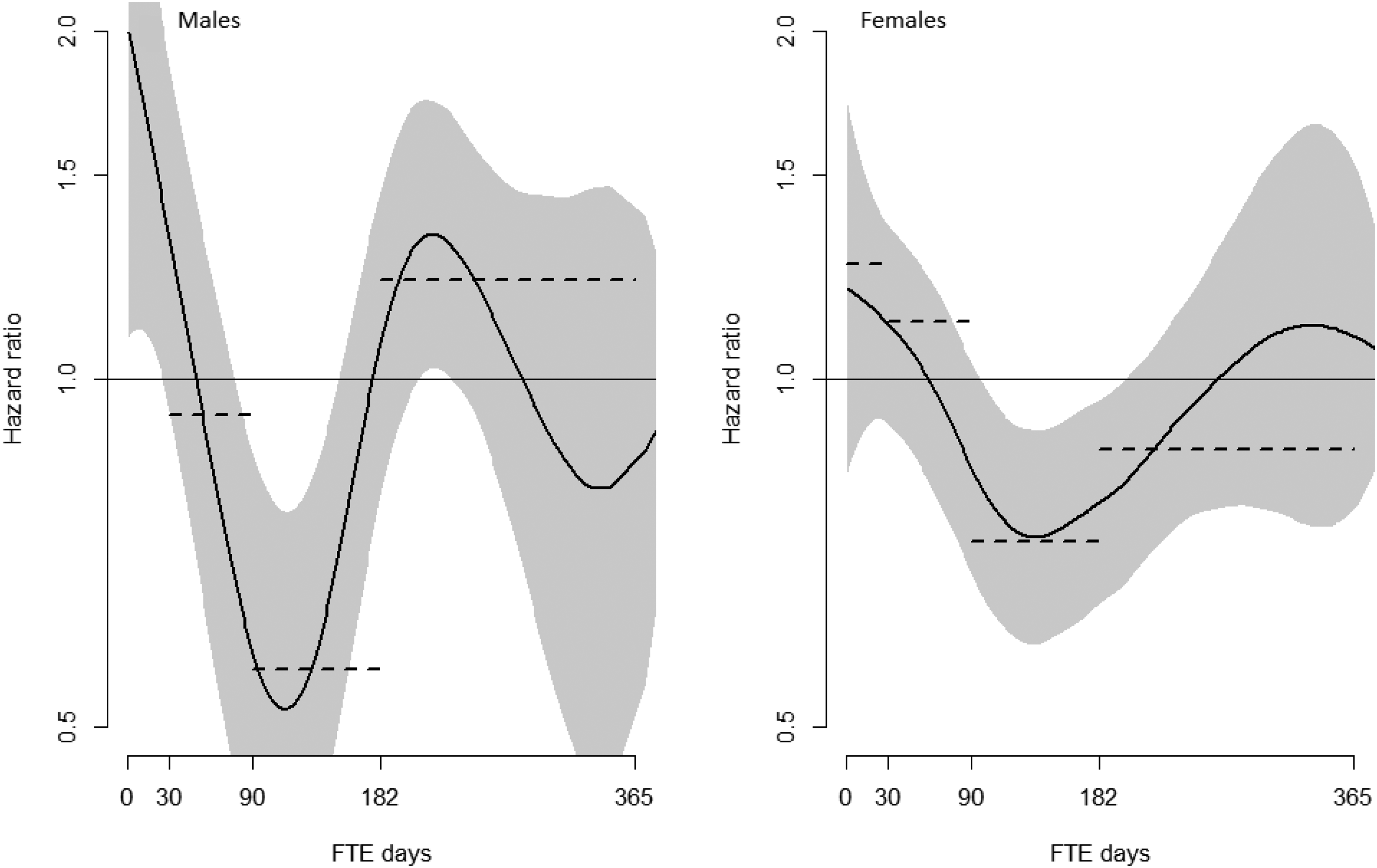
Generalized additive cox model curves demonstrating the intervention group's risk of disability pension, compared to the comparison group, as a function of full-time equivalent (FTE) days lost to work in the year before inclusion and the intervention year. Split by gender. Grey bands represent 95% confidence intervals. Dotted lines represent the hazard ratios from the Cox-regression analysis.
Diagnosis
For patients with mental health disorders, both the unadjusted and adjusted analyses showed that patients in the intervention group with 90–181 FTE days lost to work had a reduced risk of DP (unadjusted HR = 0.55, p < 0.001, adjusted HR = 0.61, p < 0.001) compared to persons with equal FTE days lost to work in the comparison group. For patients with musculoskeletal disorders, both the unadjusted and adjusted Cox regression analyses showed that patients in the intervention group with 0–29 and 30–89 FTE days lost to work had an increased risk of DP (unadjusted HRs = 2.52, p < 0.001 and 1.45, p = 0.009, adjusted HRs = 2.62, p < 0.001 and 1.63, p < 0.001 respectively) compared to persons with equal FTE days lost to work in the comparison group. For patients who had SL with both musculoskeletal and mental health disorders in the year prior to and the year of the intervention, the results were similar to those for patients with mental health disorders. The unadjusted and adjusted analyses showed that patients in the intervention group with 90–181 FTE days lost to work had a reduced risk of DP (unadjusted HR = 0.47, p = 0.006, adjusted HR = 0.56, p = 0.035) compared to persons with equal FTE days lost to work in the comparison group (Table 2 and Figure 3).
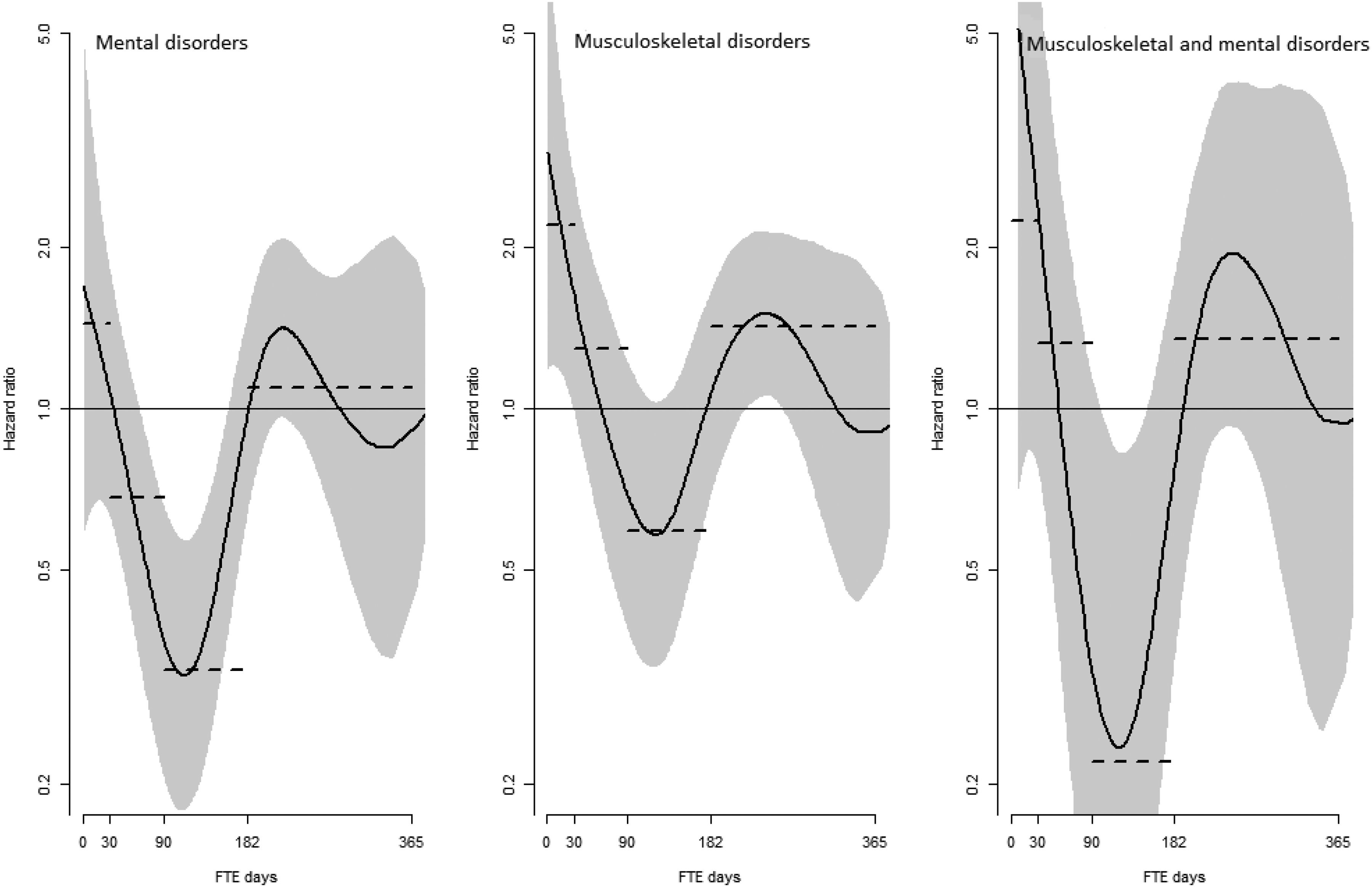
Generalized additive cox model curves demonstrating the intervention group's risk of disability pension, compared to the comparison group, as a function of full-time equivalent (FTE) days lost to work in the year before inclusion and the intervention year. Split by diagnosis. Grey bands represent 95% confidence intervals. Dotted lines represent the hazard ratios from the Cox-regression analysis.
Cox regression analyses using categories of SL days (and SL as a continuous variable in GAM analyses) were also performed, providing a similar pattern as in the presented analyses with categories of FTE days lost to work.
Discussion
In this prospective study, the overall results do not support the assumption that the RRW intervention contributed to reducing the risk of DP. However, the results do indicate that the timing of the RRW intervention was of significance. There were different risks for DP depending on category of FTE days lost to work. Patients who received the RRW intervention in an early phase, meaning they had less than a month and in some analyses under three months of registered FTE days, had an increased risk of DP compared to the comparison group. This pattern was found in the overall analysis, for males, for females, and for patients with musculoskeletal disorders. However, patients with mental health disorders or with both musculoskeletal and mental health disorders did not have an increased risk of DP if they received the intervention in an early phase. There was also a consistent pattern of reduced risk of DP among patients who received the intervention when having FTE days between three and six months, except for patients with musculoskeletal disorders. For males, there was also an increased risk of DP with FTE days over six months, but this was the only analysis providing this result.
The national RRW project mainly focused on reducing SL. Even though SL is on the pathway to DP, 30 it is important to acknowledge that most of the patients who received the RRW intervention in this study were far away from receiving a DP and that the process from SL to DP is complex. 31 Hence, the risk of DP can be classified as both a rare and a hard outcome in this study. If the focus had been on the risk of future SL the results might have been different, but regarding DP, the results do indicate that early intervention, i.e., SL under three months, not is preferred. This was an unexpected result and does not correspond with the intention of the national RRW project. A plausible interpretation of this finding might be that the patients with less than three months of SL, who were referred to the specialist health care service and received the intervention, had a higher symptom load and more health complaints than the randomly drawn comparison group. As previously mentioned, we did not have data to perform a propensity score matching on severity of complaints, and it might be that differences in symptom load between groups are the reason behind this unexpected result. However, we did adjust for SL length, and another possible interpretation of this finding that also should be discussed is overmedicalization (normal health complaints are medicalized) and/or overtreatment (interventions are not beneficial to the patients, interventions have a higher risk of harm than benefit). Overmedicalization and overtreatment are considered destructive and costly for both the individual and society and may disempower people and decontextualize personal experiences.32–34 It could be that the patients with short-term SL in the intervention group were too healthy to receive a consultation in the secondary health care service, and by providing it, one contributes to overmedicalization and overtreatment, resulting in negative outcomes. This assumption does however not correspond with the results from the interview studies performed among patients receiving this type of intervention,35,36 where normalization and demedicalization were described as one of the most helpful elements. However, those studies were based on strategic sampling and included patients who had found the intervention helpful, as opposed to the present study which included all patients who received the intervention in the RRW project period.
Furthermore, the results provided a quite consistent pattern as to when the RRW-intervention reduced the risk of DP: the most successful outcome occurred when patients had SL between three and six months. As described by Aasdahl and Fimland, 37 there might not be a “golden hour” for work disability prevention, but the question is rather what type of intervention to provide at different time points. For this intervention, and regarding DP prevention, the preferred period seems to be between three and six months of SL.
In light of previous results highlighting the positive effects of BI for patients with musculoskeletal disorders22,38,39 and the fact that the BI originally was developed for persons with musculoskeletal complaints, it was also a bit surprising that the intervention did not have a favorable effect on DP for patients with only musculoskeletal disorders. The only statistically significant finding for this group was an increased risk of DP for patients with less than three months of SL. On the contrary, for patients with mental health disorders, and patients having both musculoskeletal and mental health disorders, there was no increased risk of DP for any of the SL categories, only a reduced risk of DP for patients with three to six months of SL. Acute musculoskeletal complaints, like unspecific low-back pain, are recommended to be handled in primary care and may be easier to accommodate in the limited time a general practitioner has available per patient, while more persistent pain conditions may need to be referred to specialist health care. 40 It may thus be that the sample of patients with only musculoskeletal disorders in the intervention group differs considerably from the comparison group in regard to severity, which might contribute to explaining the lack of favorable effect for this group.
Strengths and limitations
The study's main strength is the prospective design, involving a large sample of the working-age population, with several years of longitudinal observations. Furthermore, the measure of SL and DP stems from a routinely collected national registry providing a high level of accuracy and the study included all patients who received the RRW intervention in the RRW project period. A limitation of this study was the lack of data on symptom severity and the unequal distribution of SL between the intervention group and the comparison group. The groups were not matched on SL length, leaving us with a comparison group that overall had less SL than the intervention group, indicating lower severity of complaints among the employees in the comparison group. In managing this issue, we hence found it best to perform the analyses for different categories of days lost to work. Furthermore, since long-term SL increases the risk of DP, it is sensible to explore the differences in risk of DP for various categories of SL length. However, due to variations within the sick-leave categories, residual confounding may lead to uncertainties in regard to how accurately the controls match the patients in the intervention group, providing uncertainties in the interpretation of the results.
Conclusion
Overall, the investigated RRW intervention did not contribute to a reduced risk of DP. However, several differences between the intervention and the comparison group were found. There was a pattern of increased risk of DP if the intervention was provided in an early phase of SL, and a decreased risk of DP if the intervention was provided in the phase between three and six months of SL. The study's lack of propensity score matching on severity of complaints does provide uncertainties in the conclusion, but the results indicate that intervention timing may be of significance in disability prevention. When possible, future longitudinal studies using register data should strive to reduce selection bias by incorporating propensity score matching methods on relevant covariates in the construction of the comparison group.
Footnotes
Acknowledgements
The authors want to thank Vestfold Hospital Trust for supporting the study.
Ethical considerations
Approval was granted by the Regional Committee for Ethics in Medical Research (02.12.2021/REK sør-øst D, 283547) and the Norwegian Social Science Data Services (01.11.2021/NSD, ID 306154).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Vestfold Hospital Trust.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Dispensation from the obligation of confidentiality has been granted for the provision and use of health information during the implementation of the project based on the Health Personnel Act §29 first paragraph, cf. regulation of 27 May 2021 no. 1725.