
Abstract
Background
The Danish return-to-work (RTW) program was a coordinated, tailored and multidisciplinary intervention aimed at improving sickness benefit management at municipal jobs and benefits offices in Denmark.
Objective
To estimate long-term effects of the Danish RTW program for participants with mental ill health.
Methods
The study population consisted of 8655 20–54 year-old citizens in 21 Danish municipalities who were sick-listed due to self-reported mental health problems (anxiety (4%), depression (47%), stress/ burnout (37%), or other (12%)) in 2010–2012. Of these, 5252 received the intervention while 3403 (the control group) received ordinary case management. Multinomial logistic regression was used to estimate odds ratios (intervention vs. control) for health and non-health related welfare dependency at a 1, 3 and 5-year follow-up in national registers.
Results
We did not find effects on the odds of receiving health related welfare benefits at 1 (OR = 0.90, 99% CI: 0.78–1.05), 3 (1.00, 0.85–1.17) and 5 years (0.98, 0.85–1.14). We did also not find effects on the odds of receiving non-health related welfare benefits at 1 (1.11, 0.95–1.29) and 3 years (0.94, 0.81–1.09), but found an effect at the 5-year follow-up OR = 0.81 (0.69–0.96).
Conclusion
For persons with mental ill health at baseline, a structured RTW program reduced the risk of unemployment at 5-year follow-up, suggesting an impact on a process that can only be measured after several years. The intervention did not have long-term effects on the odds of receiving health related welfare benefits.
Keywords
Introduction
Many European countries are confronted with rising costs due to disability retirement of employees because of mental health problems. The newest available numbers from Denmark show that in 2015, 41% of all new cases of disability retirement were related to mental ill health 1 and the cost of reduced employment and productivity due to mental ill health was estimated at 2.1% of the gross domestic product (GDP). 2 At the same time, the combined costs of health care, social security programs and lost productivity among people with mental ill health were estimated at 4.1% of GDP across the EU-28 nations and at 5.4% of GDP in Denmark. 2
Mental ill health affects not only society but also individuals and their families, especially if it leads to long-term sickness absence, unemployment and labor market exclusion. A swift return to stable employment would reduce costs for social security programs and lost productivity. Moreover, according to time-honored psychological theories 3 as well as recent empirical work,4,5 a return to stable employment may lead to improved mental health and thereby reduced costs for mental health care. Consequently, a multitude of interventions aimed at facilitating return to work (RTW) among people who are sick-listed due to mental ill health, have been designed and tested. The interventions typically consist of contact to the workplace, graded RTW, psychological treatment, and/or RTW coordination programs designed to improve collaboration between involved parties e.g., social insurance offices, the healthcare sector, occupational rehabilitation services and the workplace. 6
A systematic review by Mikkelsen and Rosholm (2018), which included 42 intervention studies aimed at enhancing return to work for sick-listed workers with common mental disorders, stress-related disorders, somatoform disorders and personality disorders, found strong evidence for an effect of interventions that involved the workplace and moderate evidence for an effect of graded RTW. 6 They did not find any evidence of an effect on RTW from psychological treatment as a single component intervention. However, a large Norwegian randomized controlled trial indicates that a combination of work-focused cognitive behavioral therapy and individual job support may improve work participation, RTW rates, mental health, and health-related quality of life among citizens with common mental disorders. 7
A recent scoping review by MacEachen and colleagues, which aimed at exploring the role and impact of RTW coordinator on individuals suffering from common mental ill-health conditions, did not find any evidence of a beneficiary effect of RTW-coordinators. 8 The review included two relevant longitudinal intervention studies.9–11 Both interventions were multidisciplinary and conducted in Denmark and based on small samples (n < 200), and both studies observed a slower RTW in the intervention group vs. a control group who received conventional case management. MacEachen and colleagues concluded that the available studies were too few and too small to allow firm judgement on the impact of RTW-coordinators on rates and sustainability of RTW among individuals with common mental disorders. They proposed that an increased time to RTW during an intervention might be associated with a more sustainable return and recommended that further research should be conducted to evaluate long-term effects of RTW coordination.
In this article, we present results from a long-term follow up of participants in the Danish RTW-program, where a coordinated, tailored and multidisciplinary intervention (CTMI) was tested in a set of Danish municipalities in 2010–2012.
The background of the Danish RTW-program
Due to high costs for long-term sickness absence, the Danish government launched an action plan in 2008, which contained a series of initiatives aimed at reducing sickness absence and improving labor market participation in the general working population of Denmark. One of the initiatives was the Danish RTW program, which comprised the development, implementation and evaluation of a CTMI aimed at improving sickness benefit management at municipal jobs and benefits offices in Denmark. The program was designed and implemented (from April 2010 to September 2012) by the Danish National Research Centre for the Working Environment (NRCWE) and was funded with 32 million Euros (240 million DKK) from the Danish National Prevention Fund and 4.3 million euros (32.5 million DKK) from the Ministry of Employment. 12 The design of the intervention was guided by two white papers, which summarized knowledge on RTW after sickness absence due to musculoskeletal 13 and mental health problems. 14
The setting of the trial
In Denmark, the municipal jobs and benefits offices play a key role in the efforts to help unemployed and sick-listed citizens back to work, and they decide whether a person is entitled to sickness benefits. At the time of trial, the first four weeks (three weeks, prior to 2012) of sickness absence were paid by the employer. The remaining period, up to 52 weeks, were paid by the municipality via the jobs- and benefits office. Moreover, the jobs and benefits offices were responsible for the administration of social welfare benefits, disability pensions, wage subsidy schemes and vocational rehabilitation.
15
Regular follow-up consultations with the sickness beneficiaries were mandated. As part of standard case management, the first consultation was supposed to take place within eight weeks of the inception of the concerned sickness absence episode.
16
During the first consultation, the case managers were obligated to develop a plan, which included RTW activities and goals. Case managers had to classify each of the sick-listed persons into one of the following three RTW categories:
Likely to return to the labor force within three months, Unlikely to return to the labor force within three months but able to participate in activities aimed at facilitating a return to the labor force, Unlikely to return to the labor force within three months and unable to participate in activities.
According to the sickness benefit legislation, sick-listed persons in RTW category 2 should be followed up at least once every fourth week. The legislation mandated all sick-listed persons in RTW category 2 to participate in RTW activities, which could include RTW counseling, stress- and pain-management, workability training, gradual RTW, and/or work modifications. 12 The legislation also recommended the case managers to coordinate the RTW activities with relevant stakeholders, such as employers and health professionals, and at the time of the trial, the jobs and benefits offices were required to contact the employer of the beneficiaries whenever it was relevant to do so.
The design of the intervention
The core elements of the CTMI consisted of (i) multidisciplinary RTW teams, (ii) standardized procedures for workability assessments, and (iii) a comprehensive training course for all members of the RTW teams. Each team consisted of two RTW-coordinators (case managers employed at municipal jobs and benefits offices), a psychologist, a physical therapist, a psychiatrist, and an occupational, social- or general medicine physician. 12 The standardized workability assessment tools consisted of a series of guidelines to structured interviews and procedures aimed at (i) assessing the workability of the sick-listed individual and (ii) identifying biological, psychological, and social facilitators and obstacles to returning to work. 17 Further details about these tools are given in the appendix [Additional file #1]. The purpose of the training course was to provide the RTW-teams with the skills necessary to deliver the program. The aim of the RTW-program was to improve workability assessments and RTW-plans for all participants regardless of their reason for sickness absence. It was, however, reasonable to expect that some of the components would be especially advantageous when applied to participants with mental ill health. For example, when needed, the sick-listed citizen could be assessed through a consultation with the psychiatrist from the interdisciplinary team with only a short waiting time. Such assessments could otherwise take months to obtain, due to extraordinary long waiting lists for appointments with practicing psychiatrists outside the municipal jobs and benefits offices. 17 In addition, a significant part the training was aimed at teaching RTW-coordinators about mental health problems and how to conduct interviews with people on sick leave due mental health problems, as this was assessed to be an area where more knowledge and better tools were needed. 12 Another important difference between the CTMI and ordinary case management (OCM) was that more money per capita was available for RTW-consultations and RTW-promoting activities among the beneficiaries who were allocated to the CTMI. The added financial resources were indeed an essential part of the intervention. A priori, no drawbacks of the intervention were expected other than the added costs. The expected effects of the intervention are outlined in Figure 1.
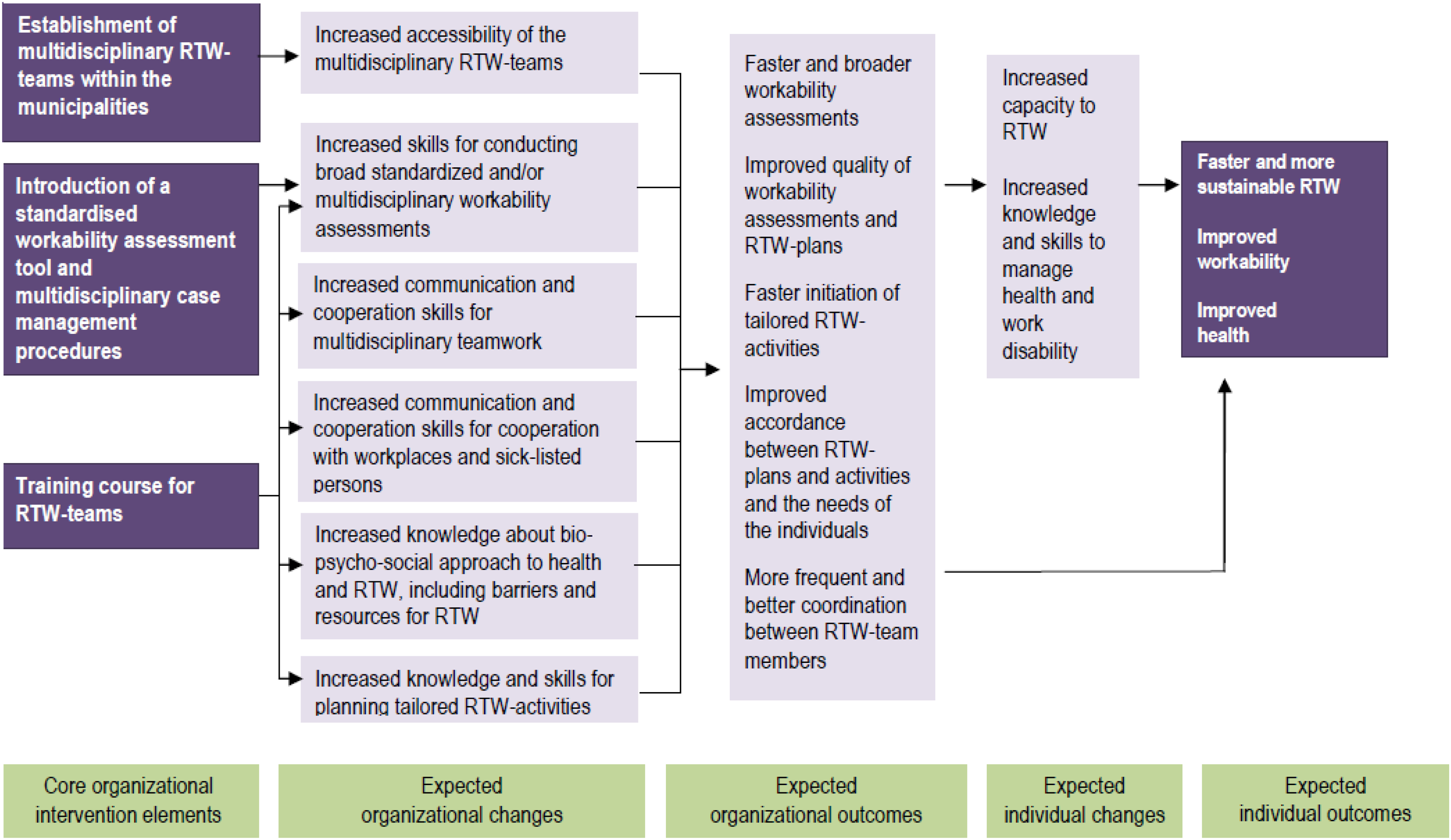
“Core program elements and expected pathways to return to work (RTW), workability, and health”. Reproduced from Aust et al. (2012). 12
The design of the trial
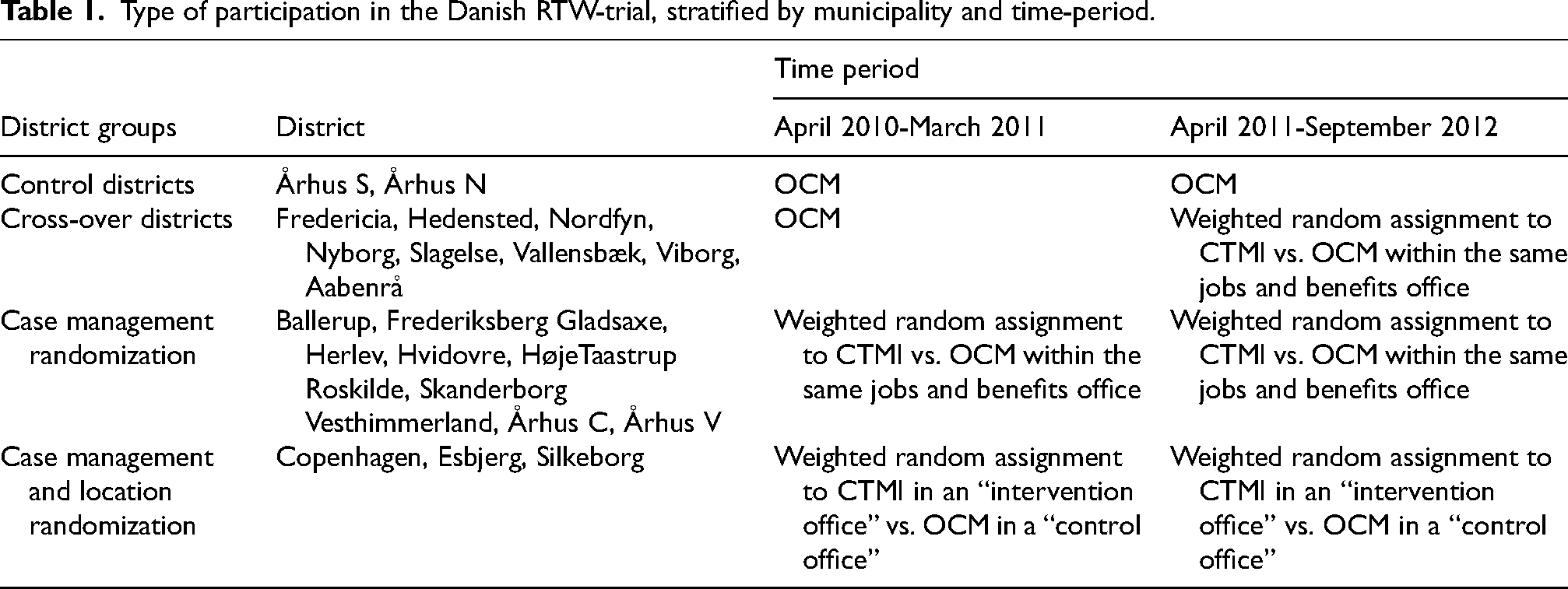
The trial included only sick-listed persons in RTW category 2. To compare effects of CTMI with OCM, trial data were collected from April 2010 to September 2012, where some individuals received the CTMI, while others received OCM. In total, 21 out of 98 Danish municipalities participated in the trial. One of the municipalities was divided into four districts, which gives a total of 24 participating districts (the other 20 municipalities each forming their own district). Two districts were assigned to deliver OCM during the entire trial period (Control districts). Eight districts were assigned to deliver OCM during the first year of the trial period and CTMI or OCM (determined through individual randomization) during the second year of the trial period (Cross-over districts). In eleven districts, during the entire trial period individuals were randomly assigned to receive either CTMI or OCM – administered by the same teams (Case management randomization).
Finally, three districts had geographically separated intervention and control offices. Throughout the trial period, they randomized individual beneficiaries into “CTMI in an intervention office” vs. “OCM in a control office”12,15,18 (Case management and location randomization). An overview of the participating districts and their role in the project is given in Table 1.
Type of participation in the Danish RTW-trial, stratified by municipality and time-period.
The aim of the present study
The Danish RTW-program included participants with all types of health problems. In contrast, the aim of the present study was to estimate the long-term effects of the program among participants who at baseline were sick-listed due to mental health problems. We chose to focus on this group of participants because long-term sick leave due to mental health problems increases the risk of future sick leave and unemployment, as well as disability retirement and thereby a permanent exit from the labor market.19–22 It is therefore particularly important to find out what can be done for people with mental health problems to continue participating in the labor market despite their health problems. The outcomes of the study are health and non-health related welfare benefits at 1, 3 and 5 years after the allocation to the intervention vs. control group. Sickness absence benefits and disability pension are examples of health related benefits. Unemployment benefits and social security cash benefits are examples of non-health related benefits.
Material and methods of the present study
The current secondary analysis of a controlled trial was nested within a larger cohort study that aimed to investigate occupational and demographic predictors of welfare dependency, at 1, 3 and 5 years after the first visit to a jobs and benefits office due to mental health related sickness absence 23 (Figure 2). The study population of the cohort study partly overlapped the study population of the controlled trial but included data from all three RTW categories. On the other hand, the cohort study was restricted to persons listing mental health problems as their primary reason for sick leave (Figure 2). A detailed description of the data material, statistical methods and inclusion criteria of the present secondary analysis of a controlled trial as well as the larger cohort study in which it was nested is given in the attached study protocol [Additional file #2]. A brief description is presented below.
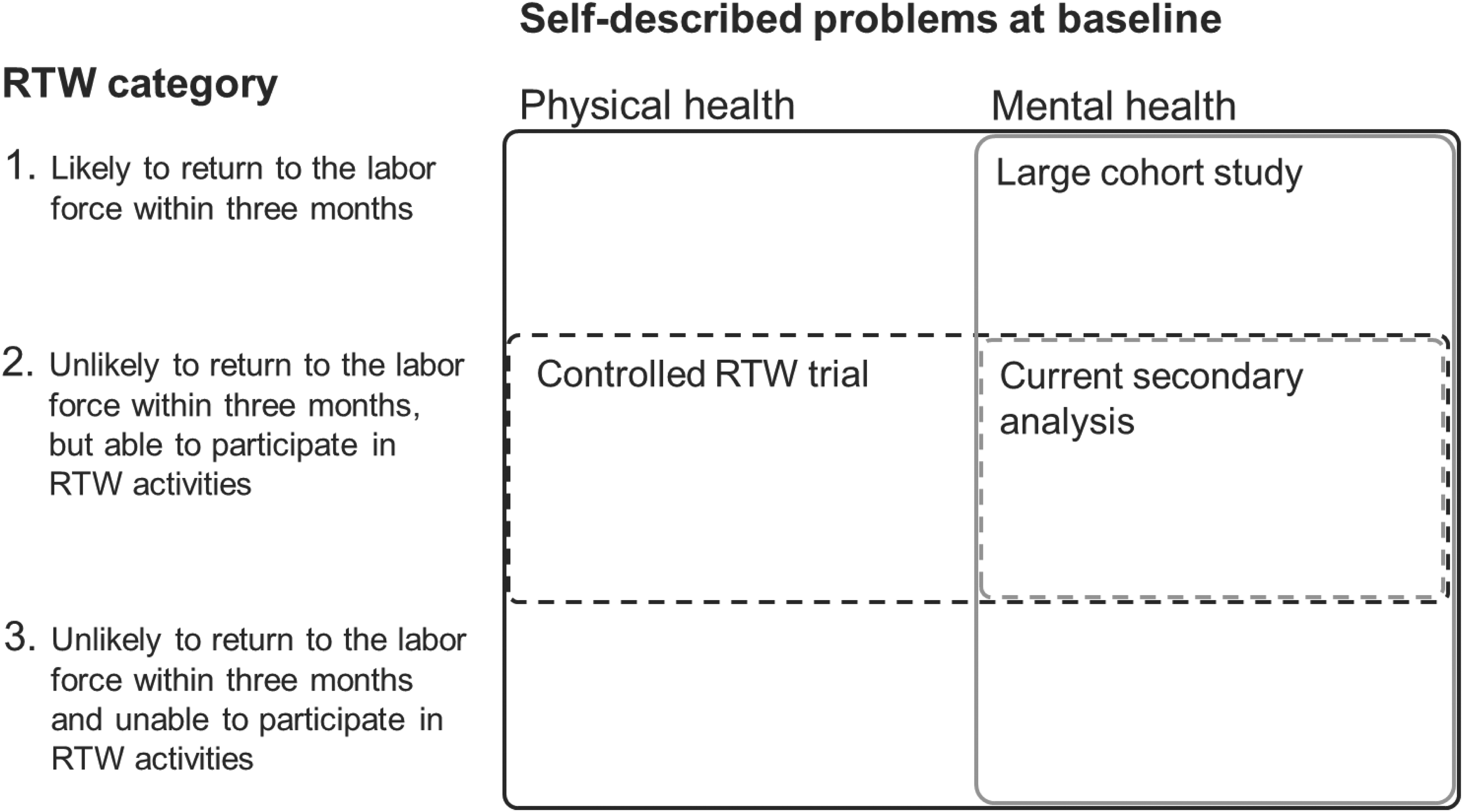
Summary of the two previous studies and the data for the current secondary analysis.
Sources of data
The municipal jobs and benefits offices provided person-based data on participation in the Danish RTW-program (intervention group; control group; not eligible for participation), RTW category, employment status, self-rated reasons for sickness absence, dates of the inceptions of the sickness absence, dates of first consultations and personal identification numbers, which enabled linkage to data in national registers.
The data from the jobs and benefits offices were linked to data from the Central Person Register (CPR), 24 the Employment Classification Module (ECM) 25 and the Danish Register for Evaluation of Marginalization (DREAM). 26 The CPR contains information on gender, family type, addresses and dates of birth, death and migrations for every person who is or has been an inhabitant of Denmark sometime between 1968 and present time. The ECM contains annual person-based information on the socio-economic status, occupation, and industry of the inhabitants of Denmark. DREAM contains weekly person-based information on social transfer payments, such as maternity/paternity benefits, sickness-absence benefits, unemployment benefits, social security cash benefits, and state educational grants. DREAM covers all inhabitants of Denmark who have received social transfers since 1993. The weekly benefits data are recorded if the person has received social transfer payments for one or more days of the week. However, since only one type of social transfer payment can be registered per week, types of benefits are prioritized in case of data overlap. The above-mentioned social transfer payments are prioritized in the order listed above, i.e., maternity/paternity benefits have higher priority than sickness-absence benefits, which in turn have higher priority than unemployment benefits and so on.
Inclusion criteria
As previously mentioned, the current secondary analysis of a controlled trial was nested within a larger cohort study (Figure 2). The cohort study included all 20–54 year old employed or unemployed people who (according to the jobs and benefits offices in the 21 participating municipalities) were on long-term sickness-absence due to self-reported depression, anxiety, stress, burnout or mental ill health without further specification, sometime during the period 26 April 2010–30 September 2012. The diagnoses in Danish sickness-absence data are based on self-reported conditions and do not contain any ICD-10 codes. Persons were excluded from the study if they immigrated or emigrated from two years prior to the concerned sickness absence episode until five years after the first visit to the jobs and benefits office. In total, 19,660 observations/persons fulfilled the criteria for inclusion in the cohort study. Of these, 8655 persons were RTW category 2 beneficiaries and thus eligible for inclusion in the current secondary analysis. There were observations with missing values on industry and job group skill-level, in the intervention as well as in the control group. These observations were, however, included in the analyses through the definition of the industry and job group categories “missing industry” and “missing job group skill-level”, respectively (cf. Table 2). Figure 3 presents a flow-chart of inclusions/exclusions. As seen in the flow-chart, two observations were excluded from the larger study due to missing dates on the start of the sickness absence period and four observations were excluded due to missing information on family type and citizenship. None of these observations were among the RTW category 2 beneficiaries. Hence, none of the observations of the present secondary analysis of a controlled trial were excluded due to missing covariates.
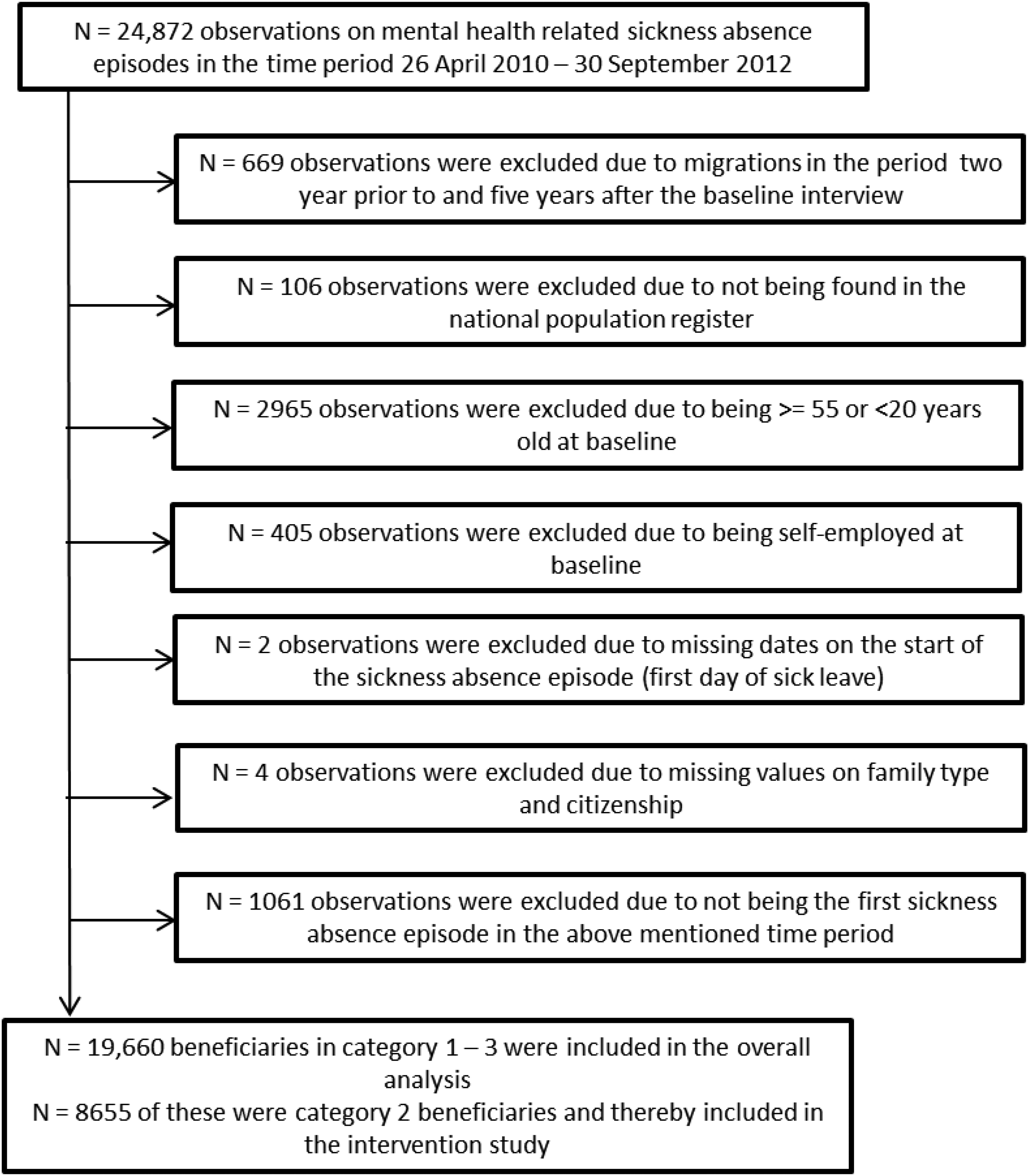
Flow-chart for inclusion and exclusions of participants in the present study.
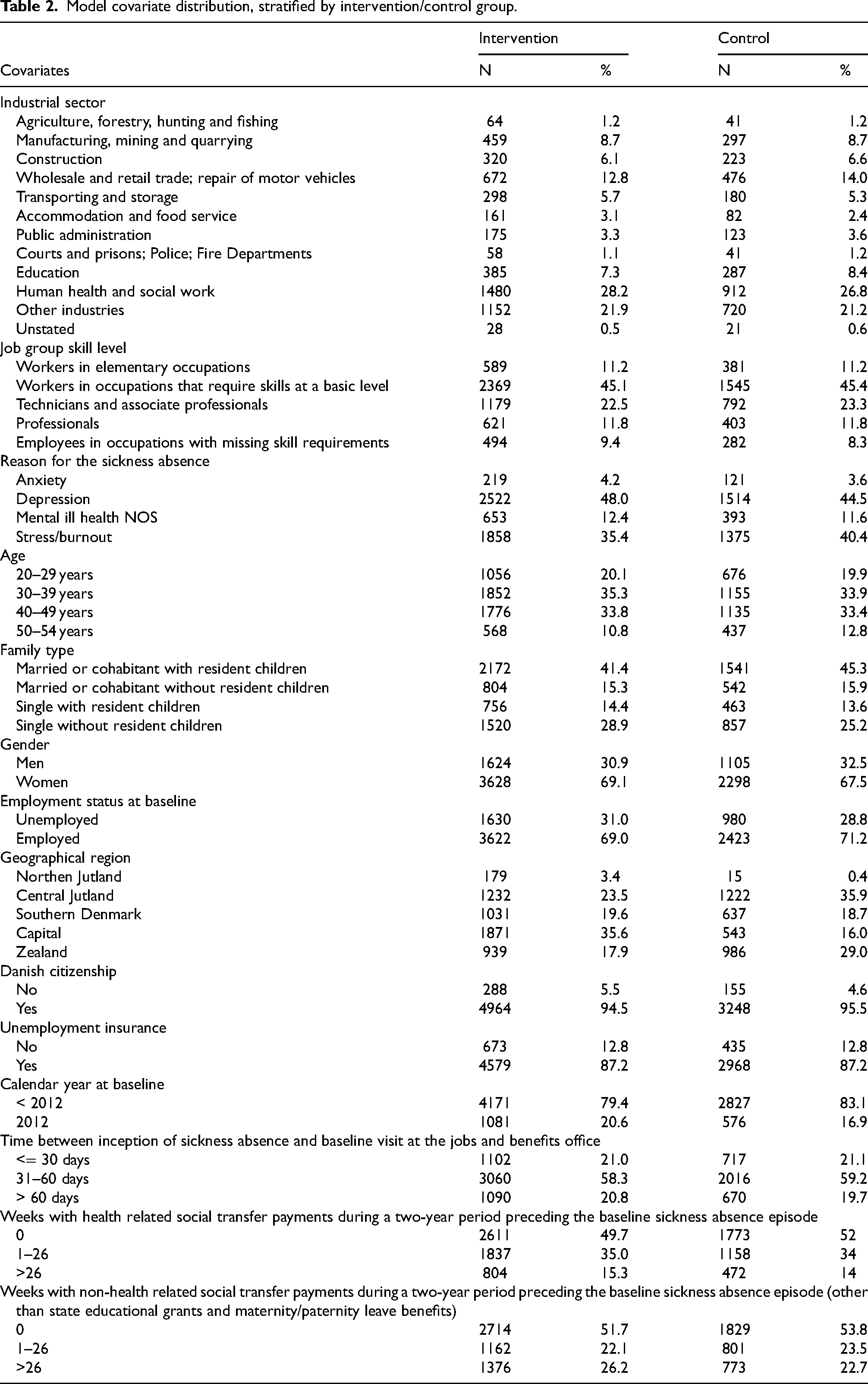
Model covariate distribution, stratified by intervention/control group.
Welfare benefits at follow-up
The outcome variable is multinomial and divided into the following categories:
No social transfer payments other than holiday allowance (DREAM-code: 121), state educational grants (DREAM-codes: 651, 652, 661) or maternity/paternity leave benefits (DREAM-code: 881) Deceased or recipient of health-related social transfer payments (e.g., sickness absence benefits, disability pension) Recipient of other social transfer payments (e.g., unemployment benefits, social security cash benefits)
The social transfer payments are based on registrations in DREAM. The social transfer payments of outcome 2 and 3 are considered adverse outcomes (welfare benefits received due to unfortunate circumstances). Since death is also an adverse (health-related) outcome, it is included in outcome 2. The odds of outcome 2 can thereby be interpreted as a proxy measure for the odds of being temporarily or permanently out of the labor force due to health issues. Maternity benefits, state educational grants and holiday allowance are not considered adverse outcomes and are therefore included in outcome 1. 23 In keeping with Hannerz and Flyvholm, 23 we will refer to outcome 1, 2 and 3 as “self-reliant”, “deceased or recipient of health related welfare benefits” and “recipient of non-health related welfare benefits”, respectively.
As seen in Figure 1, the expected effects of the Danish RTW program were i) faster and more sustainable RTW, ii) improved workability and iii) improved health. Improved health is likely to be associated with decreased odds of health related welfare benefits at follow-up. Improved workability is likely to be associated with decreased odds of health related and/or non-health related welfare benefits at follow-up. Faster RTW is likely to be associated with increased odds of being self-reliant at the 1-year follow-up. A more sustainable RTW is likely to be associated with increased odds of being self-reliant at 3- and/or 5-year follow-up. The three original outcomes are therefore also highly relevant for the current secondary analysis that investigates the long-term effects of the intervention.
Apart from state educational grants and maternity/paternity leave, there are five main types of welfare benefits in Denmark, namely, sickness absence benefits (as described in section 1.2), flexible employment, disability pension, social security cash benefits and unemployment benefits. Flexible employment is a Danish labor market policy initiative targeted at citizens who cannot cope with ordinary work due to illness, but who are not ill enough to be entitled to disability pension. Disability Pension may be granted to Danish citizens if their work capacity is permanently reduced to such a degree that they are unable to work under ordinary terms or in flexible employment.
Legal residents in Denmark may apply for social security cash benefits if they fulfill the following criteria:
They have experienced a change in their living circumstances, such as illness, unemployment or the termination of cohabitation, which has deprived them of the possibility of providing what is needed for themselves or their family. They are not supported by others. Their need for support cannot be covered by other benefits, such as unemployment benefits or a pension. They are registered at their local jobs and benefits office where they cannot refuse any jobs or RTW-promoting activities that are offered by the office.
Cash benefits that are paid to citizens whose work capacity is restricted due to health problems are classified as rehabilitation or pre-rehabilitation benefits in DREAM and are thereby classified as health-related welfare benefits in the present study. Cash benefits that are paid to citizens who are able and ready to work are classified as cash benefits for unemployed people in DREAM and are thereby classified as non-health related welfare benefits in the present study.
The normal requirements for unemployment benefits in Denmark are i) membership of an unemployment insurance fund during the past twelve months ii) a certain income during the last three years, and iii) registration as a jobseeker at the jobs and benefits office. A citizen may receive unemployment benefits for a maximum of two years within a 3-year period, calculated in hours. Further details about these welfare benefits can be found at, inter alia, the website “Living in Denmark” [https://lifeindenmark.borger.dk].
Primary statistical analysis
As seen in Table 1, the procedures used to assign individuals to CTM intervention vs. OCM were very complicated. Moreover, the intervention vs. control offices in the three municipalities in the last row of the table were not assigned at random. The data for the present secondary analysis of a controlled trial has therefore been treated and interpreted as coming from an observational study.
With outcome 1 (self-reliant) as reference, multinomial logistic regression was used to model the odds of outcome 2 and 3 (“deceased or recipient of health-related welfare benefits” and “recipient of non-health related welfare benefits”) at 1, 3 and 5 years (52, 156 and 260 weeks) after the baseline interview, as a function of the CTMI vs. OCM. The analyses were conducted by use of the GENMOD procedure in SAS version 9.4. We fitted a separate model per time point. The analyses were adjusted for the covariates given in Table 2. We selected these covariates since we, a priori, could not rule out the possibility that the analyses could be biased by differences in their distributions. E.g. if RTW rates differ between citizens with and without a Danish citizenship and the proportion of Danish citizens differs between the intervention and control group then the trial would be biased without the adjustment for Danish citizenship. Further details about the covariates are given in the appended study protocol [Additional file #2].
Data from all the participating districts were included in our primary statistical analysis. We also conducted a series of post hoc sensitivity analyses on various subsets of the data material [cf. Additional file #3].
Ethical considerations
The study complies with The Act on Processing of Personal Data, Denmark (Act No. 429 of May 31, 2000), which implements the European Union Directive 95/46/EC on the protection of individuals. The data usage was approved by the Danish Data Protection Agency (file number 2001-54-0180). The data used in this study was anonymized before its use. The ethical and legal aspects of the project were approved by Statistics Denmark, account number 708291. In Denmark, register studies, which do not include the collection and analysis of biomedical material, are not part of the ethical committee system.
Results
A total of 8655 participants were included in the present study. Of these 5252 (69% women) belonged to the intervention group and 3403 (68% women) belonged to the control group. The mean ages at baseline were 38.5 (StdDev 8.9) years in the intervention group and 38.6 (StdDev 9.0) years in the control group. The model covariate distributions are given in Table 2, for the intervention and control group, respectively.
In the intervention group, at the respective follow-ups at 1, 3 and 5 years, 44.4, 54.6 and 56.3% were self-reliant, 26.5, 21.0 and 25.5% were either deceased or received health related welfare benefits, and 29.1, 24.4 and 18.1% received non-health related welfare benefits. In the control group, 46.7, 55.2 and 55.5% were self-reliant, 28.7, 20.6 and 25.0% were either deceased or received health related welfare benefits, and 24.6, 24.1 and 19.5% received non-health related welfare benefits. At the respective follow-ups, 5, 20 and 38 persons in the intervention group and 8, 19 and 28 persons in the control group were deceased.
Table 3 shows the estimated odds ratios of the primary analysis with 99% confidence intervals. Hence, the confidence level for a single comparison is 99%. It should, however, be noted that the simultaneous confidence level i.e., the confidence that none of the true odds ratios lies outside of their 99% confidence interval is approximately equal to 94% (100 times (0.99 raised to the power of six)). As seen in the table, there were no signs of an intervention effect on the odds of health related welfare benefits at any of the three follow-up periods. The estimated odds ratio for non-health related welfare benefits was slightly higher than one at the 1-year follow-up, slightly lower than one at the 3-year follow-up, and markedly lower than one at the 5-year follow-up, which suggests that the intervention may have had a beneficial effect on long-term employability. In the sensitivity analyses [Additional file #3], results were robust to exclusion of data from the three districts that performed Case management and location randomization (Table S1). A separate analysis of data from these three districts showed smaller and non-significant reductions in odds of receiving non-health related benefits in the intervention group at year 3 and 5 and increased odds (although non-significant) of receiving non-health related benefits at year 1. Adjustment for jobs and benefits office as a random effect led to large confidence intervals and lack of significant effects [Additional file #3].
Odds ratio (OR) with 99% confidence interval (CI) for two types of welfare dependency at 1, 3 and 5 years after first visit to a jobs and benefits office due to mental health related sickness absence in Denmark, 2010–2012 as function of the Danish RTW program.
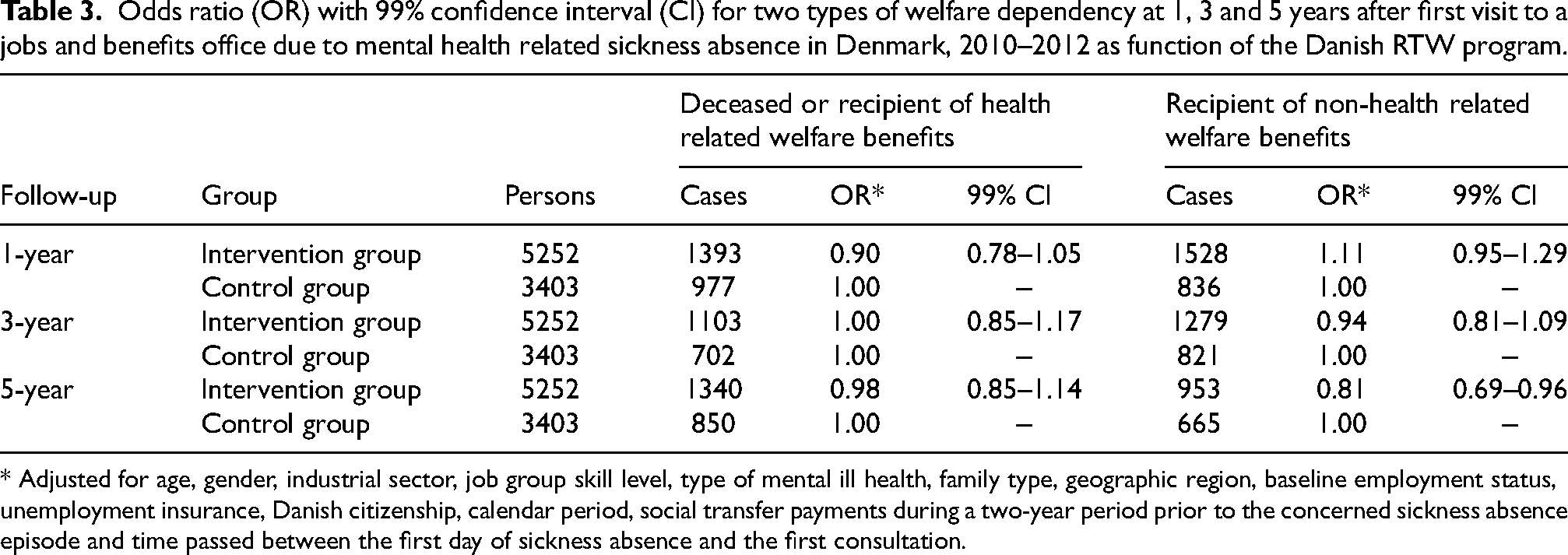
* Adjusted for age, gender, industrial sector, job group skill level, type of mental ill health, family type, geographic region, baseline employment status, unemployment insurance, Danish citizenship, calendar period, social transfer payments during a two-year period prior to the concerned sickness absence episode and time passed between the first day of sickness absence and the first consultation.
Discussion
In the present study, we estimated odds ratios of being i) deceased or recipient of health related welfare benefits and ii) recipient of non-health related welfare benefits, compared to being alive and self-reliant at 1, 3 and 5 years after being allocated to the intervention/control group in the Danish RTW-trial. We focused solely on participants who were sick-listed due to mental ill health. As shown in Figure 1, it was assumed that the implementation of the three intervention components (multidisciplinary RTW teams, standardized procedures for workability assessments, and a comprehensive training course for all members of the RTW teams) would lead to improved workability assessments and more coordinated and tailored RTW plans [cf. Figure 1].
Despite the many theoretical advantages of the intervention, we did not find any signs of an effect on the odds of death or health related welfare benefits at any of the three follow-up periods. We found, however, a significantly decreased risk for non-health related welfare benefits in the CTMI group at the 5-year follow-up, suggesting that the intervention had a beneficial effect on long-term employability.
Our results in the context of previous research
The absence of beneficial effects on RTW at the one-year follow-up in the present study aligns well with results obtained in previous evaluations of the Danish RTW program17,27 and in earlier similar studies on effects of multidisciplinary, coordinated and tailored interventions on RTW.9–11,28 A short description of these studies are given below.
Nielsen et al. (2014) 27 conducted an effect evaluation of the RTW program on time to self-support, with a maximum follow-up period of 1 year. Their study concerned “sickness absence due to any cause” and included observations from the three municipalities in the district type “Case management and location randomization”. The authors estimated the rate ratio for self-support between the CTMI and OCM group at 1.01 (95% CI: 0.71–1.43), and concluded that the “study was clearly underpowered to detect a shared effect across the three included municipalities”.
Winzor and colleagues 17 conducted an evaluation of the RTW program on duration of sickness absence and on time to self-support, which included all observations from all districts. Their analyses were adjusted for cause of sickness absence, age, gender, education, history of sickness absence and unemployment, baseline employment status, and utilization of general practitioners, hospitals, and medicine. The maximum follow-up period was one year. The rate ratios between the CTMI and OCM group were estimated at 1.02 (95% CI: 0.86–1.21) for time to self-support and 1.02 (95% CI: 0.80–1.31) for time to the end of sickness absence. Moreover, Winzor and colleagues evaluated the effects of the RTW program on the development of overall physical health, overall mental health, self-rated health, sleep quality and self-rated workability. These evaluations were based on questionnaire data at baseline and at a follow-up six months later. The authors did not find any statistically significant effect of the RTW program on overall physical health, self-rated health, sleep quality and self-rated workability. They found, however, that the improvement of self-rated mental health was statistically significantly greater in the CTMI than in the OCM-group. Hence, there might have been some improvements for people with mental health problems, although not shown in faster RTW at the one-year follow-up.
When interventions do not or only partly lead to the results that were expected, it is very important to check for implementation problems. The process evaluation of the trial concluded that the basic features of the RTW program were implemented to an acceptable degree (i.e., all municipalities established RTW teams, all RTW team members participated in the training courses, and all RTW teams followed the general procedures of the program). However, the process evaluation also showed large variation in the quality of the implementation between the municipalities. For example, half of the first consultations with the RTW coordinator were conducted later than the end of the 9th week, which means the supposed starting point for the RTW-process was delayed for half of the sick-listed participants. In addition, the rates by which RTW-coordinators referred sick-listed persons to the interdisciplinary teams varied considerably between municipalities, resulting in potential under-use or over-use of the expertise of the other RTW team members. The actual experience of the RTW program for sick-listed persons might therefore have been very different between municipalities making it difficult to assess what impact the program had when assessed across all municipalities. 15
A qualitative study based on in-depth interviews with persons on sick leave who participated in the RTW intervention found that the workability assessment and RTW activities could result in sustained RTW, in premature RTW and in delayed RTW. 29 The study found that the persons on sick leave needed an individual approach where they experienced ‘being seen’ and ‘being met’ by RTW professionals in order for the RTW intervention to be successful. Possibly, the structured approach and standardized assessment developed for the CMTI might have been counterproductive by focusing on the “right” thing to do rather than on the needs of the sick-listed person.29,30 In addition, the study pointed out that the fact that RTW professionals are both the facilitators and the controllers of the sick-listed persons’ RTW process is an inherent paradox in the intervention, which can also impede the necessary establishment of a high-quality relationship between the sick-listed persons and RTW professionals. These challenges and variations in the extent to which high-quality relationships were established might have contributed to the absence of larger effects of the RTW intervention in the present study.
As mentioned in the introduction, the review by MacEachen and colleagues 8 identified two multidisciplinary RTW-interventions conducted in Denmark that also did not find any effects. One intervention 9 focused on citizens who were sick-listed due to stress-related disorders and consisted of psychoeducative treatment combined with comprehensive coordinative efforts among stakeholders at the workplace, municipal case workers, and GPs. The psychoeducative treatment was primarily aimed at activating and supporting the sick-listed citizens’ efforts to adopt a problem-solving approach to their problems. Contrary to expectation, the intervention led to a slower return in the intervention group. The rate ratio for return to the labor market in the intervention vs. a control group with conventional case management was estimated at 0.84 (95% CI: 0.60 to 1.19).
Also, another multidisciplinary, coordinated and tailored intervention with many similarities to the Danish RTW program did not find the expected positive effects for the intervention group.10,11,28 The study was conducted with citizens at a job and benefits office, who were sick-listed due to mild mental health problems. The intervention consisted of i) an assessment of disability, functioning, barriers and resources for RTW by a multi-disciplinary rehabilitation team (occupational physician, physiotherapist, psychologist, social worker), ii) an action plan for RTW to overcome barriers and strengthen resources iii) implementation of the action plan and iv) psychological consultation if it was deemed necessary. The rate ratio for return to the labor market in the intervention vs. a control group with conventional case management was estimated at 0.50 (95% CI: 0.34 to 0.75) after accounting for measured confounding 10 and fewer were self-supported (52% vs. 69%; p = 0.02) two years after the initial sickness absence episode. 11 An additional analysis of the implementation processes of the intervention 28 identified several barriers that might have contributed to these negative outcomes, e.g., those responsible for recruitment of participants assessed the inclusion criteria as too narrow, waiting lists occurred and the included participants had more severe mental health problems than expected.
To summarize, we as well as other similar studies did not find any evidence of faster RTW-rates from multidisciplinary, coordinated and tailored interventions in the short- or medium-term. However, none of the previous studies used a follow-up period that was as long as we did, i.e., after 5 years. Hence, we do not know if the other similar interventions maybe had long-term effects that have not been assessed. Our study suggests that beneficial effects may appear several years after the intervention.
Strength and weaknesses
The design of the Danish RTW study aimed to counter different risks of confounding and bias. Individual randomization to CTMI vs. OCM within the same offices (Case management randomization) protects against non-comparability of the intervention and control group. However, a major component of the CTMI is a comprehensive training course for all members of the RTW team. If both CTMI and OCM are performed by the same persons or in the same office, this training effort is likely to also benefit persons randomized to OCM (i.e., a learning cross-over effect) – potentially causing bias (towards a null effect) in the estimation of intervention impact. For these reasons, three districts carried out CTMI in offices at other locations than the regular OCM offices (Case management and location randomization). The CTMI teams were generally established by recruiting new employees for this project, although in some cases existing employees applied for – or were assigned to – being a part of these teams. This design provides better protection against learning cross-over effects but on the other hand raises the potential criticism that the CTMI teams may attract employees with a skill set and motivation that is different from the employees performing OCM. A cross-over design, where districts performed OCM the first year and transition to case management randomization for the second year (Cross-over districts) may solve some of these issues but is open to calendar time effects. Also, districts where an individual randomization do not take place (Control districts or a control phase) may be prone to selection bias effects. It is not thoroughly documented how the assignments of the districts into Control, Cross-over and Case management randomization districts were done.
All long-term sickness beneficiaries were assigned to one of three RTW categories, of which only category 2 qualified for the RTW study. Since significant extra resources followed each person assigned to CTMI there might have been an incentive to classify persons into category 2 if there was a significant chance that they might be assigned to CTMI. This incentive is not present in the Control districts or in year one of the Cross-over districts. Thus, some risk of bias is present for all four district groups, but the type of potential bias differs between district groups. Considering these potential biases, we decided to do the present analyses as if data stemmed from an observational study, statistically controlling for a number of factors that might have caused non-comparability between the intervention and control groups. Also, we performed a series of sensitivity analyses using data from different district groups [Additional file #3]. Results that are robust across these different analyses are less likely to be caused by bias.
Recommendations for future research
In Denmark, entitlement to sickness absence benefits requires that a person is unfit for work due to his/her own illness. The decision as to whether a person is considered unfit for work is made by the case manager at the municipal jobs and benefits office. According to the law, the decision should be based on an overall assessment of the illness and its impact on the sick-listed person's ability to work. 31 Work ability is not a completely objective measure. 32 Hence, the decision to reject or approve (continued) sickness absence benefits may depend not only on the condition and circumstances of the sick-listed citizen but also on the skills, experience, attitudes, values and opinions of the case manager, which in turn may depend on the culture, norms and practices at the jobs and benefit office in which they work.
It was hypothesized that the intervention of the present study would lead to faster as well as better work ability assessments (Figure 1). We have not investigated if this was the case. It was however reasonable to believe that it would lead to faster assessments, since waiting times for the expert opinions that might be needed in order to reach a decision about whether or not a sick-listed citizen is unfit for work, most probably was reduced considerably by the case workers immediate access to a psychologist, psychiatrist, physiotherapist and occupational physician. It was also reasonable to believe that the research-based workability assessment tools and the assistance of the experts in the multi-disciplinary RTW-team would lead to an improved quality of workability assessments and return to work plans. It is however far from certain that an improvement of workability assessments leads to faster RTW-rates. A workability assessor may err in two ways; i) by declaring a person who is unfit for work due to his/her own illness as being fit for work and ii) by declaring a person who is fit for work as being unfit for work due to his/her own illness. Hence, the effect of an improved work ability assessment on e.g., the average duration of sickness absence benefits would depend on the pre-existing prevalence and distribution of these two types of errors.
It is possible that some jobs and benefits offices tend to withdraw sickness benefits too soon while others tend to withdraw them too late, and that a successful implementation of a standardized work ability assessment tool thereby would lead to increased sickness benefits expenditures in some municipalities and decreased expenditures in others. It is moreover reasonable to believe that a successful implementation of a standardized workability assessment tool would lead to decreased regional inequalities in decisions to grant or deny sickness absence benefits. We propose that this is an interesting aspect of workability assessment and recommend that future evaluations of RTW interventions should focus not only on their effects on average rates of RTW but also on their effects on regional inequalities in decisions to grant or deny sickness absence benefits.
Conclusions
The results of the present study do not support the hypothesis that the Danish RTW program leads to faster RTW-rates among citizens who are sick-listed due to mental ill health in the general population of Denmark. The estimated odds ratio for non-health related welfare benefits at the 5-year follow-up suggests, however, that the intervention had a weak beneficial effect on long-term employability.
Supplemental Material
sj-docx-1-wor-10.1177_10519815251344932 - Supplemental material for Long-term follow-up of participants with mental ill health in the Danish return-to-work program: A secondary analysis of a controlled trial
Supplemental material, sj-docx-1-wor-10.1177_10519815251344932 for Long-term follow-up of participants with mental ill health in the Danish return-to-work program: A secondary analysis of a controlled trial by Harald Hannerz, Malene Friis Andersen, Maj Britt Dahl Nielsen, Birgit Aust, Jørgen Vinsløv Hansen1, Jakob Bue Bjørner1 and Mari-Ann Flyvholm in WORK
Supplemental Material
sj-pdf-2-wor-10.1177_10519815251344932 - Supplemental material for Long-term follow-up of participants with mental ill health in the Danish return-to-work program: A secondary analysis of a controlled trial
Supplemental material, sj-pdf-2-wor-10.1177_10519815251344932 for Long-term follow-up of participants with mental ill health in the Danish return-to-work program: A secondary analysis of a controlled trial by Harald Hannerz, Malene Friis Andersen, Maj Britt Dahl Nielsen, Birgit Aust, Jørgen Vinsløv Hansen1, Jakob Bue Bjørner1 and Mari-Ann Flyvholm in WORK
Supplemental Material
sj-docx-3-wor-10.1177_10519815251344932 - Supplemental material for Long-term follow-up of participants with mental ill health in the Danish return-to-work program: A secondary analysis of a controlled trial
Supplemental material, sj-docx-3-wor-10.1177_10519815251344932 for Long-term follow-up of participants with mental ill health in the Danish return-to-work program: A secondary analysis of a controlled trial by Harald Hannerz, Malene Friis Andersen, Maj Britt Dahl Nielsen, Birgit Aust, Jørgen Vinsløv Hansen1, Jakob Bue Bjørner1 and Mari-Ann Flyvholm in WORK
Footnotes
Acknowledgments
The study was funded by the Danish Ministry of Employment. The data of the project were provided by the municipalities involved in the project, the National Research Centre for the Working Environment and Statistics Denmark. We would like to thank all researchers and participants in the Danish national return-to-work (RTW) program for their contribution to the data collection.
Ethical consideration
The study complies with The Act on Processing of Personal Data, Denmark (Act No. 429 of May 31, 2000), which implements the European Union Directive 95/46/EC on the protection of individuals. The data usage was approved by the Danish Data Protection Agency (file number 2001-54-0180). The data used in this study was anonymized before its use. The ethical and legal aspects of the project were approved by Statistics Denmark, account number 708291. In Denmark, register studies, which do not include the collection and analysis of biomedical material, are not part of the ethical committee system.
Funding
The Danish National Prevention Fund financed the implementation of the intervention in the participating municipalities. The Danish Ministry of Employment financed the design and evaluation of the intervention.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.