
Abstract
Background:
Firefighting's physically demanding and hazardous nature requires firefighters to maintain optimal cardiometabolic and musculoskeletal health. It is suspected that metabolic syndrome (MetS) may contribute significantly to both sudden cardiac arrest and debilitating injury in firefighters, however, there are no studies investigating this relation.
Objective:
The objective of this study was to investigate the relationship between MetS and Musculoskeletal Health (MSH) in Firefighters.
Methods:
Using systemic sampling, 309 firefighters were recruited to participate. Using physical measures and questionnaires, risk factors for MetS were assessed. MSH was classified as musculoskeletal injuries and musculoskeletal discomfort, and assessed using the Nordic and Cornell musculoskeletal discomfort questionnaires. Logistic and multinomial regressions were used to assess the relationship between variables.
Results:
MetS was significantly associated with injuries in firefighters (p = 0.026). Healthy firefighters experienced more musculoskeletal discomfort than firefighters with metabolic syndrome (p = 0.045). Triglyceride and blood glucose concentrations were significantly associated with musculoskeletal injuries (p = 0.038) and musculoskeletal discomfort (p = 0.035). Multinomial regression indicated that firefighters with one, two and three risk factors were at increased odds of 5.01, 2.40, and 2.36 times than healthy firefighters.
Conclusion:
This study suggests that cardiometabolic health may directly affect the musculoskeletal health of firefighters and may play a crucial role in their overall health and well-being.
Introduction
Firefighting is regarded as a physically demanding and hazardous occupation that requires the protection of the safety and well-being of civilians, as well as the maintenance of critical infrastructure.1–3 However, the leading cause of death among firefighters is attributed to underlying cardiometabolic conditions, most prominently hypertension, diabetes, and hypercholesterolemia, leading to sudden cardiac death.4,5 In addition, a significant number of firefighters sustain severe musculoskeletal injuries, which lead to early retirement.6–8
Metabolic syndrome (MetS) is characterised as a clustering of cardiovascular risk factors which increases an individual's risk for developing cardiovascular and cerebrovascular disease.2,3,9 Most studies have investigated the relationship between physical fitness and musculoskeletal disorders in firefighters; however, there have not been many studies conducted investigating the relationship between MetS and musculoskeletal injuries in firefighters. Previous studies have indicated that a progressive deterioration in musculoskeletal health is an important factor leading to firefighters sustaining injuries while on duty.6,7 Injury-related absenteeism has a significant and negative effect on the fire departments and places a substantial financial burden on firefighters. 10 Recent literature has suggested that MetS may significantly contribute to deteriorating musculoskeletal health through increased oxidative stress, lipid metabolism dysregulation, inflammation, endothelial dysfunction and tendon injury.11–14 Central obesity has been shown to cause unequal weight distribution, placing significant strain on the lower back.10,15,16 In addition, the increase in weight burdens the musculoskeletal system, predisposing firefighters to injury. It is hypothesised that high concentrations of triglycerides alter lipid metabolism, resulting in the formation and deposition of foam cells within tendons, which manifests most frequently in the gastrocnemius tendon,13,17 which has been reported to be a common injury site in firefighters.6,15,18 Higher insulin resistance concentrations have been proposed to reduce the protective effect of insulin within the joint capsule, possibly weakening the synovial joint, leading to injury.11,14
Firefighting is a strenuous occupation that significantly strains the cardiovascular and musculoskeletal systems, which are significantly increased when cardiometabolic conditions are present,16,19 which may also increase their risk for severe debilitating musculoskeletal injury. There have not been any studies conducted on firefighters where the relationship between MetS and musculoskeletal health was investigated, leaving a significant gap in the literature. Therefore, this study aims to investigate the relationship between MetS and musculoskeletal health in firefighters.
Methods
Study design and population
This cross-sectional study gathered data on metabolic syndrome (MetS) risk factors and physical fitness between June and August 2022. A total of 309 full-time male and female firefighters from the City of Cape Town Fire and Rescue Service (CoCTFRS) participated. Each volunteer provided written informed consent before participating. The study received ethical approval from the University of the Western Cape (ethical clearance number: BM21/10/9). In addition, the Chief Fire Officer and the research division of the City of Cape Town's Department of Policy and Strategy granted approval to conduct the study.
Sampling and participant recruitment
Data collection was conducted during the annual physical fitness assessment by the CoCTFRS at a standardized fire station in the Cape Town metropolitan area. Systematic random sampling was used, and every third firefighter was selected for participation. The study included all full-time firefighters aged 20 to 65 years from 32 fire stations across four regional districts, each having up to three platoons with an average of 8 to 12 firefighters per platoon. Exclusions were made for firefighters on administrative duty, sick leave, part-time or seasonal employment, or those not participating in the physical ability test (PAT) on the assessment day. The mean years of experience of firefighters were 14.8 ± 10.6 years with a minimum and maximum years of experience of 1 to 40 yearss
Physical measures and cardiometabolic risk factors
Height was measured using a standardized portable stadiometer (Seca portable stadiometer), with firefighters barefoot and heads positioned in the Frankfort plane. 20 Body mass and lean body mass (LBM) were measured with minimal clothing (shorts for males and shorts and t-shirts for females) using a bioelectrical impedance analysis scale (Tanita© BC-1000 Plus, Tokyo, Japan). 20 Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. 21 Waist circumference (WC) was measured at the navel, and hip circumference (HC) was measured at the widest point of the buttocks. 21 Following standardised procedures, blood pressure (BP) was taken using an automatic monitor (Omron Healthcare Co., Ltd, Hoofddorp, Netherlands). Blood tests for glucose and lipid profiles were conducted using a CardioChek® Plus analyzer (PTS Diagnostics, Indiana, USA). 22 The blood test procedure involved pricking the finger, discarding the first blood drop, and testing the second. Blood measures were taken in a non-fasted state as firefighters needed to be ready for emergencies.
Classification of metabolic syndrome
Firefighters were identified as having MetS if they exhibited at least three of the following criteria: abdominal obesity, indicated by a waist circumference exceeding 94 cm for males and 80 cm for females; a non-fasting blood glucose (NFBG) level of 7.7 mmol/L or higher; triglyceride levels of 1.7 mmol/L or above; high-density lipoprotein (HDL) levels below 1.0 mmol/L; and blood pressure readings with a systolic value of 130 mmHg or more, or a diastolic value of at least 85 mmHg.1,23,24
Classification of musculoskeletal health
Musculoskeletal health was categorized into musculoskeletal injuries, musculoskeletal discomfort and musculoskeletal disorders. The Nordic Musculoskeletal Questionnaire (NMQ) and Cornell Musculoskeletal Discomfort Questionnaires (CMDQ)20,25 were used to identify and classify musculoskeletal injuries and discomfort, respectively. The NMQ 26 and CMDQ 27 was shown to be reliable and valid used for research purposes. For musculoskeletal disorders, firefighters were asked to indicate if they are currently diagnosed with a musculoskeletal disorder, such as osteoarthritis, rheumatoid arthritis, gout, back pain and back problems such as scoliosis and lupus, which was classified under the category of having a musculoskeletal disorder. For the Nordic musculoskeletal questionnaire, it was used to assess the prevalence, frequency, and severity of musculoskeletal discomfort across nine body regions, which included the neck, shoulders, upper back, elbows, lower back, wrists/hands, hips/thighs, knees, and ankles/feet. Participants were asked whether they had experienced discomfort in these regions during the past 12 months, past 4 weeks and then today (the day of testing), with supplementary/additional questions addressing the age of the firefighter at the time of ache, pain or discomfort, frequency, intensity, and impact of the ache, pain or discomfort, such as work restrictions or medical attention sought. 20 The questionnaire used visual aids highlighting the affected area, where firefighters were required to answer in simple yes/no answers. The CMDQ was used to assess participants’ musculoskeletal discomfort in relation to their occupational activities. 25 The CMDQ evaluated the discomfort levels across multiple body regions, including the neck, shoulders, back, arms, wrists/hands, hips, thighs, knees, lower legs, and feet. 25 Firefighters rated the frequency and intensity of discomfort on a Likert scale and provided information on how discomfort impacted their work performance in the final section of the questionnaire. For injuries, firefighters were considered to have an injury if formally diagnosed withtin the last 12 months by a physician or had taken extended time off work due to the injury. For the discomfort score, each body region was given a weighted score by multiplying the numerical values for frequency, severity, and work interference. 25 The following calculation was used:
Score for a region = (Frequency Score) × (Severity Score) × (Work Interference Score) = cumulative score
Statistical analysis
The data were cleaned using the double-entry method in Microsoft Excel. After that, the data were coded and imported into the Statistical Package for the Social Sciences (SPSS) software, version 29 (Chicago, Illinois, USA), for analysis. To assess the distribution of the data, the Shapiro-Wilks test was used which indicated that the data were not normally distributed. Categorical variables were summarised as percentages and continuous variable were summarised as means, standard deviations, and percentages. The Chi-squared test was used to assess the association between the categorical variables (musculoskeletal injury and musculoskeletal discomfort categories). Group comparisons were conducted using the Mann-Whitney U test, due to the data not being normally distributed. Spearman's rank correlations were conducted between continuous variables, such as age, years of experience, MetS and the number of risk factors and the musculoskeletal discomfort score for each body region. Univariable and multivariable regressions were conducted with musculoskeletal injuries and discomfort, and each region was investigated as the dependent variable. MetS and each risk factor were used as the independent variable. In the multivariable models, the independent variables were adjusted for age, sex and BMI, which has been shown to be significantly associated with musculoskeletal health in firefighters.6,7 In addition, multinomial regressions were performed to ascertain the relationship between musculoskeletal health and the number of positive MetS risk factors. The multinomial regressions were adjusted for age, sex and BMI. The musculoskeletal disorder score was normalized using the two-step normalization transformation, where data were fractionally ranked and normalized using the inverse DF, IDF.NORMAL transformation. 28 An alpha of <0.05 indicated statistical significance.
Results
Table 1 describes the prevalence of musculoskeletal injuries and discomfort according to metabolic syndrome in firefighters. Firefighters with MetS reported an injury prevalence of 49.3% and healthy firefighters reported an injury prevalence of 42.9%. In addition, MetS was found to be significantly associated with injuries in firefighters (p = 0.026). Healthy firefighters had a higher prevalence of upper body injuries (21.8% vs 14.1%), whereas lower body injuries were more prevalent in firefighters with metabolic syndrome (23.5% vs 25.4%). Healthy firefighters experienced more musculoskeletal discomfort compared to firefighters with metabolic syndrome (43.7% vs 36.6%) and reported a higher discomfort score which was reported to be significant (p = 0.045). Healthy firefighters reported a significantly higher shoulder (p = 0.030) and upper back discomfort score (p = 0.039).
Demographic characteristics of firefighters according to metabolic syndrome and musculoskeletal discomfort.
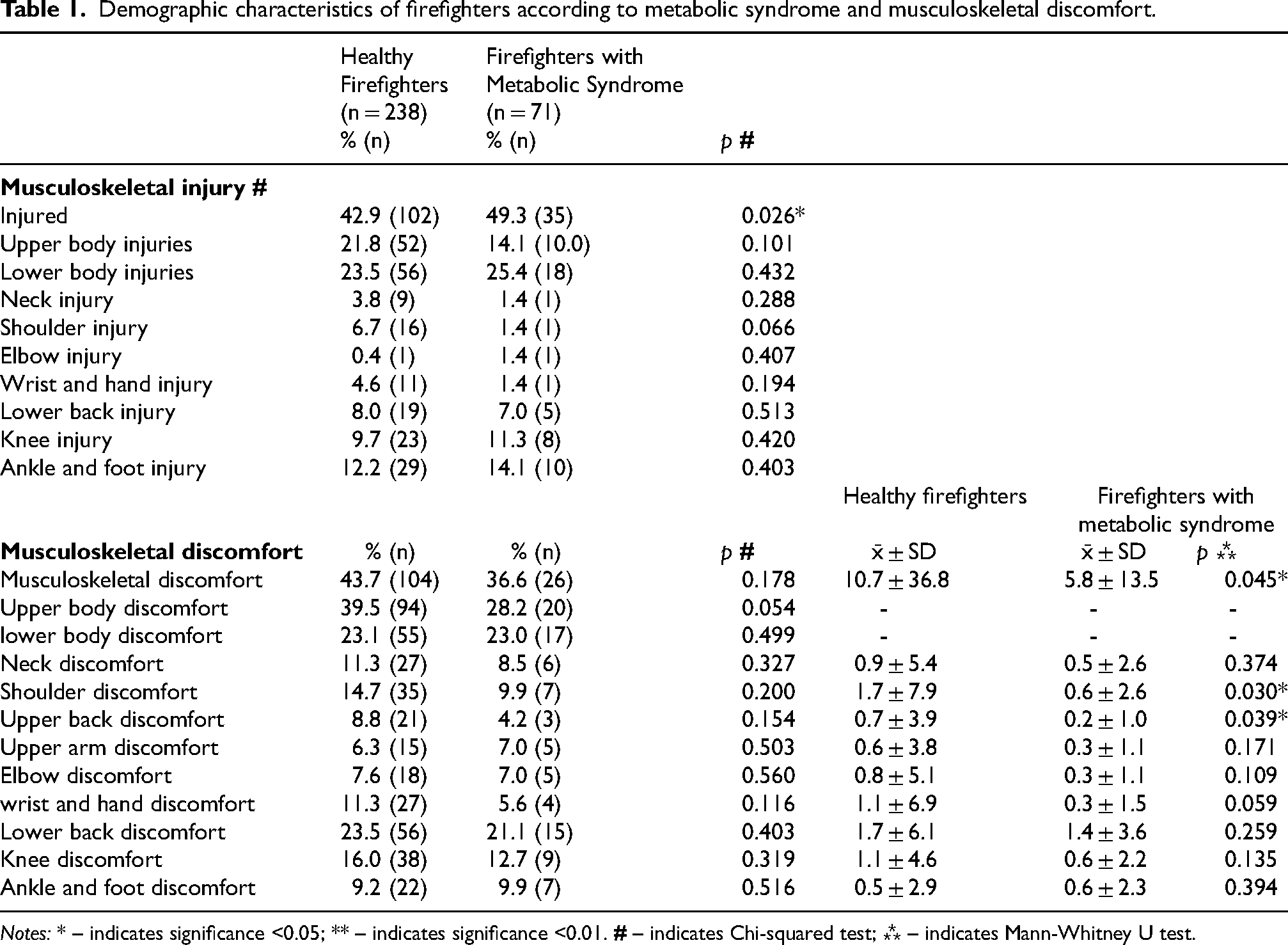
Notes: * – indicates significance <0.05; ** – indicates significance <0.01.
Table 2 describes the correlation between age, years of experience, metabolic syndrome, and musculoskeletal health in firefighters. The results indicated there was a moderate correlation between age and MetS (r = 0.311, p < 0.001) and the number of MetS risk factors (r = 0.386, p < 0.001). There were moderate to strong positive correlations between all injury sites (all p < 0.001). A strong positive correlation was found between upper arm discomfort and elbow and forearm discomfort (r = 0.828, p < 0.001), thigh discomfort (r = 0.724, p < 0.001), and lower leg discomfort (r = 0.718, p < 0.001). Thigh discomfort had a strong positive correlation between thigh and lower leg discomfort (r = 0.822, p < 0.001).
Correlations between age, metabolic syndrome and musculoskeletal discomfort in firefighters.
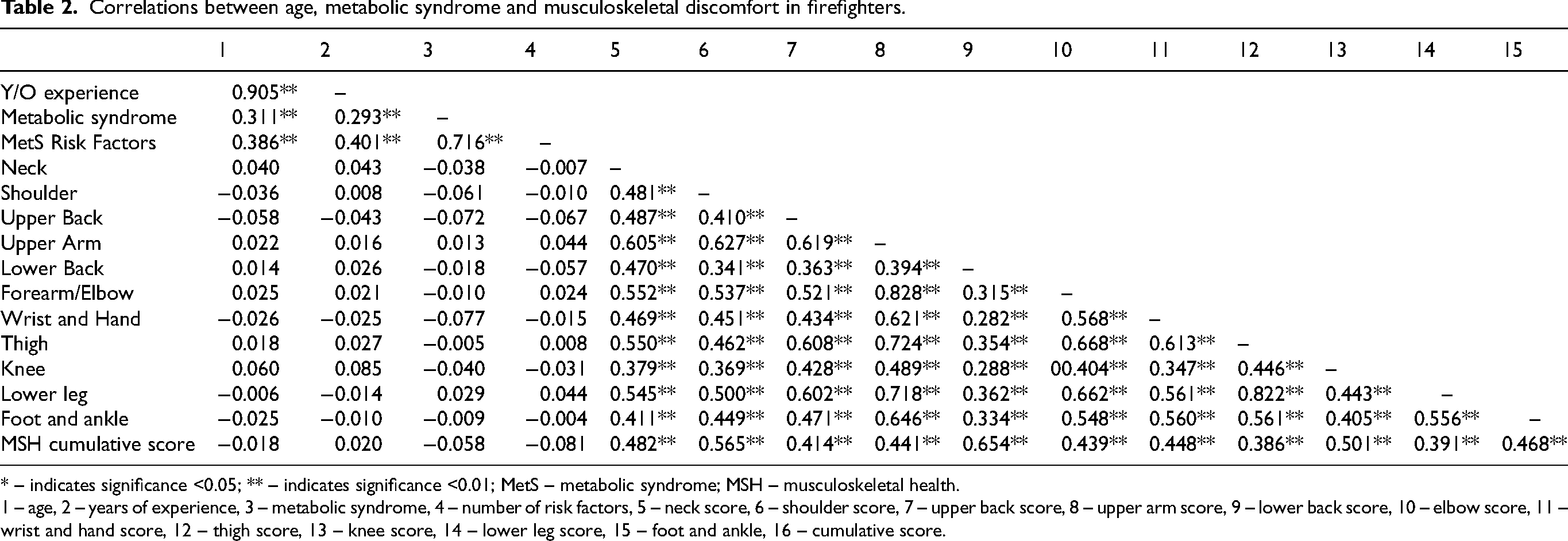
* – indicates significance <0.05; ** – indicates significance <0.01; MetS – metabolic syndrome; MSH – musculoskeletal health.
1 – age, 2 – years of experience, 3 – metabolic syndrome, 4 – number of risk factors, 5 – neck score, 6 – shoulder score, 7 – upper back score, 8 – upper arm score, 9 – lower back score, 10 – elbow score, 11 – wrist and hand score, 12 – thigh score, 13 – knee score, 14 – lower leg score, 15 – foot and ankle, 16 – cumulative score.
Table 3 delineates the relationship between MetS and musculoskeletal injuries and musculoskeletal discomfort in firefighters. Univariable analysis indicated that MetS increased the odds of firefighters reporting musculoskeletal injuries by an odds of 1.77 times over healthy firefighters. An increase in the number of MetS risk factors increased the odds by 1.22 of firefighters reporting musculoskeletal injuries compared to healthy firefighters. An increase in triglyceride concentration increased the odds of firefighters reporting musculoskeletal injuries by 1.89 times over healthy firefighters. An increase in blood glucose concentration increased the odds of firefighters reporting musculoskeletal discomfort by 2.81 times over healthy firefighters. In the multivariable analysis, after adjustment for age, sex and BMI, MetS and the number of MetS risk factors were no longer associated with musculoskeletal injuries. An increase in triglyceride and blood glucose concentrations remained significantly associated with musculoskeletal injuries (p = 0.038) and musculoskeletal discomfort (p = 0.035), respectively.
Logistic regression indicating the relationship between metabolic syndrome and musculoskeletal injuries and discomfort in firefighters.
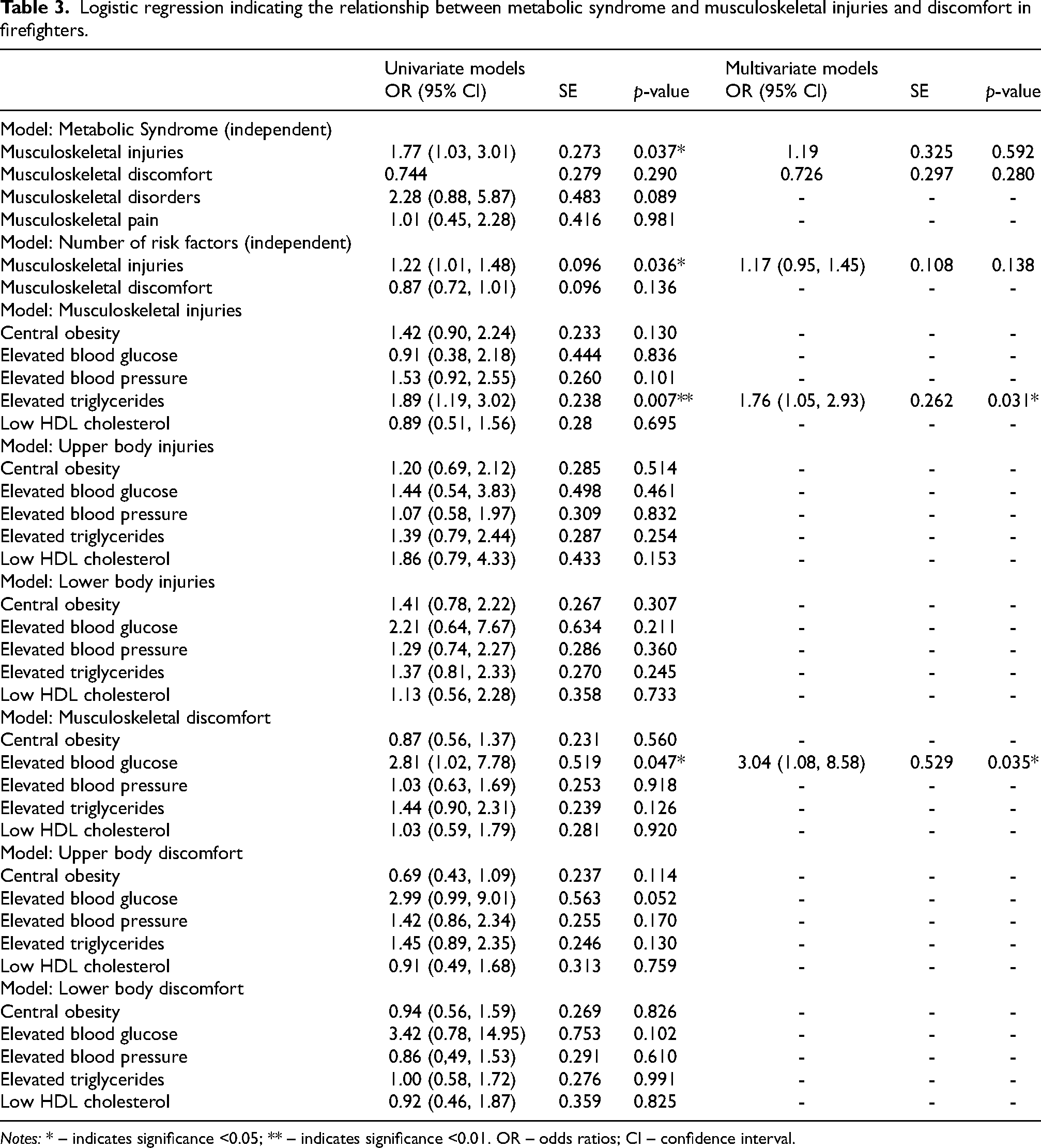
Notes: * – indicates significance <0.05; ** – indicates significance <0.01. OR – odds ratios; CI – confidence interval.
Table 4 describes the relationship between musculoskeletal injuries and musculoskeletal discomfort and MetS in firefighters. Firefighters with one, two and three risk factors were at an increase in odds of 7.04, 5.94 and 1.75 of firefighters reporting neck injuries over healthy firefighters. In addition, firefighters with one, two and three risk factors were at increased odds of 5.01, 2.40, 2.36 times than healthy firefighters. In the multivariable analysis, after adjustment for age, sex and BMI, firefighters who had one (p < 0.001), two (p < 0.001) and three (p < 0.001) risk factors remained at risk for reporting musculoskeletal discomfort.
Multinomial regression indicating the relationship between musculoskeletal injuries and musculoskeletal discomfort and metabolic syndrome risk factors in firefighters.
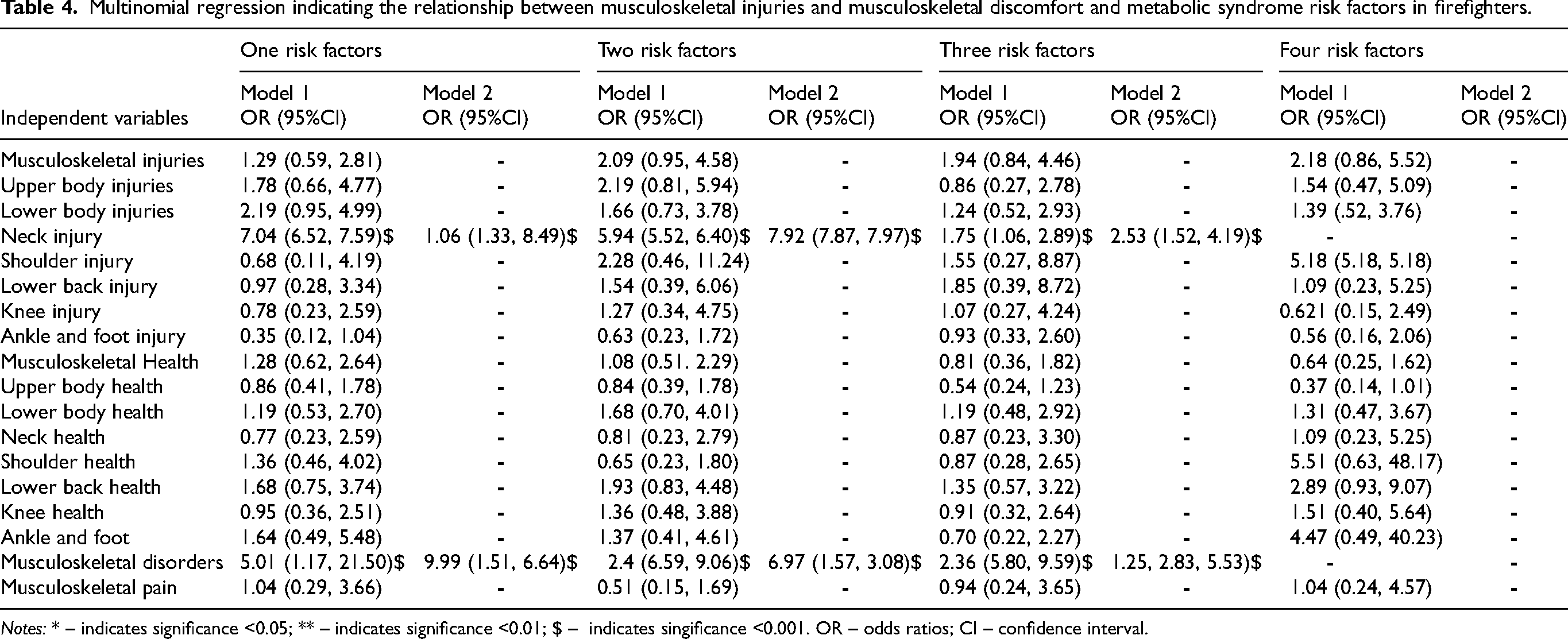
Notes: * – indicates significance <0.05; ** – indicates significance <0.01; $ – indicates singificance <0.001. OR – odds ratios; CI – confidence interval.
Discussion
In a cross-sectional study among firefighters from the City of Cape Town Fire and Rescue Service, the most important finding was that firefighters with MetS had a higher prevalence of musculoskeletal injuries than healthy firefighters and significantly increased the odds of firefighters reporting musculoskeletal injuries, In addition, healthy firefighters had a higher prevalence of upper body injuries (21.8% vs 14.1%), whereas lower body injuries were more prevalent in firefighters with metabolic syndrome (23.5% vs 25.4%). These results were similar to previous studies, which indicated that individuals with metabolic syndrome tended to report more injuries than their healthier counterparts.29–31 Healthy firefighters experienced more musculoskeletal discomfort compared to firefighters with metabolic syndrome (43.7% vs 36.6%) and reported a higher discomfort score, which was reported to be significant (p = 0.045). In contrast, previous studies29,32 reported that MetS was associated with feelings of pain and discomfort in individuals. It is suspected that healthy firefighters perform their duties with greater vigor and intensity which then predisposes them to overuse injuries, ultimately manifesting as musculoskeletal discomfort, however, were less likely to sustain serious injury.33–35 The results of the current study remained significant after after adjustment for age and sex. Previous research has indicated that as firefighters age their odds of developing injuries and discomfort increases as part of the physical nature of the occupation.6,7 In addition, the second confounder, sex, has been shown to be significantly associated with injuries, where female firefighters tended to be more prone to injury and musculoskeletal discomfort16,33
MetS increased the odds of firefighters reporting musculoskeletal injuries by an odds of 1.77 times over healthy firefighters. An increase in the number of MetS risk factors increased the odds by 1.22 of firefighters reporting musculoskeletal injuries than healthy firefighters. A study conducted by Yoshimura et al. 36 found similar results, where risk factors associated with metabolic syndrome significantly increased the odds of musculoskeletal injuries and disorders. Similarly, a study by Xie et al. 29 reported that MetS was associated with knee osteoarthritis in firefighters. This is further corroborated by Pan et al. 37 reported that MetS and its components were significantly associated with worse pain trajectories and increased when central obesity was present. The study concluded that the development and maintenance of worse pain trajectories may be caused by MetS. 37 In contrast, a study by Ibrahim et al. 38 found that MetS was not associated with musculoskeletal pain or worse symptoms. A recent study hypothesised that common pathways related to MetS mediated damage to musculoskeletal tissues, where studies have linked the relationship between adipose-based inflammation, MetS, and musculoskeletal tissue damage. 14 In addition, hypertension may cause tissue damage due to vasoconstriction, depriving musculoskeletal tissue of sufficient nutrient exchange. 39 Furthermore, altered cholesterol may be linked to lipid metabolism dysregulation and endothelial dysfunction, linked to tissue damage in tendons. 40 We found that an increase in the number of MetS risk factors was associated with increased odds of firefighters reporting musculoskeletal disorders. As suggested by previous studies, each risk factor for MetS has its own pathway for causing deterioration in musculoskeletal health.14,39,40 This would suggest that having multiple or all risk factors may increase your risk of musculoskeletal injuries and discomfort significantly,14,41 providing a possible explanation for the results of the current study.
The results indicated that an increase in the number of MetS risk factors increased the odds of firefighters reporting neck injuries. Similarly, a study conducted by Mäntyselkä et al. 32 reported that MetS was significantly associated with neck pain in participants. The study also reported that the relationship between MetS and neck pain was stronger in males, however, the prevalence of neck pain in the current study was higher in females. Skovgaard et al. 13 corroborated these findings, where their study reported that firefighters with metabolic syndrome were 2.5 times more likely yo report a tendon injury in both upper and lower extremities. A study by Kumagai et al. 42 reported that LDL cholesterol was significantly correlated to neck pain symptoms. Comparably, a study by Ahorukomeye et al. 43 found a significantly higher prevalence of neck pain in individuals with hypercholesterolemia compared to healthy individuals. As triglyceride concentrations are a risk factor for MetS, it may provide a possible explanation for the current relationship found. Studies17,41,44 have shown that altered lipid concentrations may disrupt cholesterol synthesis negatively impacting cholesterol and lipid homeostasis. This may, unintendedly, result in an increase in oxidative stress, leading to neuropathic pain, axonal degeneration and myelin degeneration. 43 Moreover, reactive oxygen species (ROS) stimulate the production of chemotactic molecules and inflammatory cytokines, which draw and activate leukocytes and exacerbate nerve inflammation.17,43,44
We found that an increase in triglyceride concentration increased the odds of firefighters reporting musculoskeletal injuries. A study conducted by Djade et al. 44 found that triglycerides was one of the biomarkers that were reported to be significantly associated with musculoskeletal health in individuals. Similarly, Gold et al. 17 conducted a systematic review and reported that an increase in triglycerides was present in individuals with adhesive capsulitis, those suffering from myofascial pain and those with musculoskeletal discomfort, increasing the pain intensity experienced. Another systematic review by Tilley et al. 40 reported that higher blood lipid concentrations were associated with musculoskeletal injuries. Specifically, triglyceride concentration was significantly higher among individuals with tendon pain or rupture. The study noted that tendons respond similarly to vascular tissues, having an affinity for cholesterol deposition, along with the shear forces and compression forces that alter the proteoglycan profile of the tendons and aggregation of pro-inflammatory macrophages, weakening the tendon structure. 40 The macrophages form foam cells, forming atherosclerotic lesions, further weakening the tendon structure. 40 These foam cell deposits may form xanthomas, which research has found especially prominent in the gastrocnemius tendon,45,46 predisposing tendons to sudden rupture.
The current results indicated that an increase in blood glucose concentration increased the odds of firefighters reporting musculoskeletal discomfort. Skovgaard et al. 13 reported that individuals with elevated HbA1c had a threefold higher risk of tendon injury in the lower extremities compared to healthy individuals. Similarly, Yoshimura et al. 36 found that higher impaired fasting glucose increased the odds of firefighters reporting knee osteoarthritis by 1.9 times compared to healthy firefighters. This was further supported by Chiba et al. 11 who found that higher fasting glucose worsened knee symptoms of osteoarthritis. Similarly, a study by Csonka et al. 12 found that three to eight out of ten individuals with diabetes mellitus suffered musculoskeletal complications. In addition, the study noted that the most common complications were osteoarthritis, adhesive capsulitis of the shoulder, carpel tunnel syndrome and Dupuytren contracture. Diabetes mellitus and insulin resistance have been proposed to negatively impact the joint organ system negatively, being linked to chondrocyte dysfunction. 14 In addition, insulin seems to have a protective role for synoviocytes, blunting the TNF-induced matrix metalloproteinase release.14,47 However, diabetics have shown an increase in synovial levels of TNF-a and macrophages, indicating that diabetes and insulin resistance may blunt the protective effect of insulin in the joint.14,47 In addition, a study found that higher levels of insulin resistance were related to lower femoral neck strength, which may significantly predispose individuals to injury. 48
Strengths and limitations
This was the first study conducted investigating the relationship between MetS and musculoskeletal disorders in firefighters. The number of participants recruited met the minimum sample size required and probability sampling was used, which strengthened the study's findings. There are several limitations in the present study. This study used a cross-sectional design, which precludes the inference of causal relationships. In addition, musculoskeletal injuries, musculoskeletal discomfort and musculoskeletal disorders were self-reported, which may have introduced recall bias and subjective bias when reporting their injury status. Lastly, female firefighters were under-represented, limiting the generalizability to the female firefighter population.
Recommendations
A longitudinal study design should be used in future research to determine the causative causes of MSIs and MSD in firefighters. A more representative sample of female firefighters should be included to improve generalizability to the female firefighter population.
Conclusion
The results of the study showed that firefighters with MetS had a significantly higher prevalence of musculoskeletal injuries, while healthy firefighters experienced more musculoskeletal discomfort compared to firefighters with metabolic syndrome. In addition, risk factors for MetS, specifically triglycerides and blood glucose were significantly associated with a higher musculoskeletal injury and discomfort in firefighters. This study suggests that cardiometabolic health may directly affect the musculoskeletal health of firefighters and may play a crucial role in their overall health and well-being. Local and international fire departments should prioritize maintaining ideal cardiometabolic health as this may positively affect injury rates in firefighters.
Supplemental Material
sj-jpg-1-wor-10.1177_10519815251324367 - Supplemental material for Relationship between metabolic syndrome and musculoskeletal health in firefighters
Supplemental material, sj-jpg-1-wor-10.1177_10519815251324367 for Relationship between metabolic syndrome and musculoskeletal health in firefighters by Jaron Ras and Jeanne Grace in WORK
Footnotes
Acknowledgments
We want to thank every firefighter who voluntarily agreed to participate in the current study.
Ethical approval
Ethical clearance was provided by the University of the Western Cape (ethical clearance number: BM21/10/9).
Informed consent
All participants gave their written informed consent before participation in the study.
Author contributions
JR contributed to conceptualizing, writing the original draft, reviewing and editing the manuscript, and visualization. JG contributed to the manuscript's conceptualization, reviewing, and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statements
Due to the agreement between the researcher and the City of Cape Town Fire and Rescue Service, the data cannot be made publicly available. However, if researchers are interested in accessing the data, approval will be requested from the City of Cape Town Fire and Rescue Service to disclose it to the interested researcher/s.
Supplementary material
Supplemental material for this article is available online.