
Abstract
Background
Despite the prevalence and impacts of pregnancy loss, there is a lack of statutory or workplace-based supports for workers experiencing pregnancy loss, especially before the point of viability. As reproductive and working ages overlap, workplaces can play a significant role in pregnancy loss experiences.
Objective
The aim of this study is to map the available literature on workplace supports for pregnancy loss before viability.
Methods
We conducted a scoping review following JBI Guidance and a pre-registered protocol. We searched eight academic databases/platforms, grey literature sources, and reference lists for eligible documents (2012–2022).
Results
Following title and abstract screening and full-text review, 48 records were included for analysis: 18 reports, 15 journal articles, 6 guides/codes of practice, 3 theses, 2 book/book chapters, and 4 other narrative records. Secondary research was the most common methodology employed (n = 16) followed by primary research (n = 14). Reports mainly originated from South-East Asia, while all empirical studies took place in high-income, English-speaking countries. Leave from work was the most discussed/important form of workplace support. Helpful organisational measures were also identified.
Conclusions
Our review found a lack of empirical research on workplace supports and experiences of pregnancy loss. Further research is needed to understand experiences and develop and implement appropriate supports.
Introduction
Between one in four and one in five pregnancies end in miscarriage, stillbirth or neonatal death. Impacts–physical, psychological, and economic–can be significant, for individuals who experience pregnancy loss and societies.1,2 As reproductive years significantly overlap with working years, workplace environments play an important role in experiences of pregnancy loss.
While many countries offer mandatory workplace leave for people who experience the loss of a pregnancy from the point of ‘viability’ (i.e., a stillbirth), similar provisions often do not extend to earlier pregnancy losses, in the form of first and second trimester miscarriage, ectopic pregnancy, molar pregnancy, or termination of pregnancy/abortion. Approximately one in ten women will experience one miscarriage in their lifetime, 2 while globally the rate of abortions is 39 per 1000 women aged 15–49 years. 3 Though many first trimester miscarriages resolve without treatment, sometimes medical or surgical management is required to remove fetal tissue, which can result in days of bleeding, pelvic pain, and admission to hospital, amongst other side effects.2,4,5 Similar is observed for termination of pregnancy given the overlapping medical management strategies.
In recent years, a number of countries have recognised the impacts of such earlier pregnancy losses, and the need for greater supports within the workplace. In 2021, New Zealand introduced three days paid bereavement leave for women and their partners who have experienced a miscarriage, but not a termination of pregnancy. 6 Later that year, the Australian Government passed an amendment to the Fair Work Act 2009 which provides for two days of compassionate leave for those experiencing a pregnancy loss under 20 weeks’ gestation. 7 Countries such as the Republic of Ireland8,9 and the United Kingdom 10 are also exploring such leave provisions.
A scoping review of the scientific literature on the experiences of workers coping with perinatal loss and the resulting bereavement by Meunier and colleagues 11 found qualitative research describing the experiences of returning to work following a perinatal loss, but it primarily included participants experiencing late perinatal loss (20 weeks’ gestation or more). Some studies have since been published which report experiences of miscarriage in the workplace and associated supports.12–14 These note that support can often be informally received from colleagues and managers, rather than formally provided through the organisation. 13 In addition, people report taking leave around the time of miscarriage (a median of seven days reported in an Australian study), with many using paid sick or annual leave for this. 13 Barriers to taking leave include inadequate resources, poor support from managers, or stigma; professional consequences; and personal feelings associated with taking leave, such as guilt and shame. 12 Additional organisational supports can include referral to Employee Assistance Programmes or counselling, and flexible working arrangements. 14
To inform discussions relating to the types of supports needed within workplaces for people who experience earlier pregnancy loss (i.e., before the point of viability and/or stillbirth, where mandatory leave may be provided), a review of existing literature is warranted, one which adopts a systematic approach to identifying and describing literature that meets the inclusion criteria. Specifically, this review needs to address the following research questions, to examine the scope of the available evidence and any gaps:
Which workplace supports (e.g., legislative, policy, psychological, social) are, or should be, available for people who experience pregnancy loss before viability? What are people's experiences of workplace supports for pregnancy loss before viability?
We use the term ‘pregnancy loss before viability’ to be as specific as possible about our area of focus. It is not ideal, and not without critique. 15 We are particularly interested in pregnancies that end before this period, and which are not classified as ‘stillbirth’. Internationally, definitions of miscarriage, stillbirth and viability vary, by gestational age and/or fetal weight. 2 Miscarriage is generally defined as the loss of pregnancy before viability – this can range from 20 to 28 weeks of gestation, depending on geographical region. 16 For the purpose of this review, a pregnancy loss is defined by any form of pregnancy loss (e.g., miscarriage, termination of pregnancy), before the point at which it would be considered a stillbirth in the country it occurred in. In Ireland, a pregnancy loss is considered a stillbirth at 24 weeks gestation and/or with a fetal weight of 500 grammes or more. 16
Methods
Protocol and registration
We conducted a scoping review according to a pre-registered protocol 17 following JBI guidance.18–21 A scoping review ‘addresses an exploratory research question aimed at mapping key concepts, types of evidence, and gaps in research related to a defined area or field’ [ 22 :1292–1294] and thus was appropriate to address our aim and research questions. We followed the five stages as per this guidance: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, and (5) collating, summarising and reporting the results. We report our scoping review in line with the PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines; 23 see Supplementary File A. This study, as a scoping review of literature, did not require ethical approval.
Knowledge user engagement
This work was conducted as part of the PLACES (Pregnancy Loss in Workplaces: Informing policymakers on support mechanisms) Project which was commissioned and funded by the Department of Children, Equality, Disability, Integration and Youth in the Republic of Ireland. 9 Decision-makers from the Department, in addition to people with lived experience, were involved in discussions which informed the conduct and reporting of this scoping review. In addition, members of the research team (KOD, DN) are involved in the care of people–including workers–who experience pregnancy loss. The team engaged in reflexivity throughout the study, individually and during group discussions. This included reflecting on their positionality and assumptions and how they might affect the research process.
Eligibility criteria
Our inclusion and exclusion criteria are detailed in our protocol. 17 In brief, included documents addressed pregnancy loss before viability in the context of paid employment/work, in terms of experiences and/or supports. The search covered the publication period from 2012 to 2022, given the increasing attention on this issue in recent years. We did not restrict by study design, language or geographical location.
Information sources
We searched the following databases/platforms in December 2022 to identify potentially relevant records: EMBASE (Elsevier), CINAHL Plus with Full Text (EBSCOhost), Business Source Complete (EBSCOhost), MEDLINE (Ovid), SCOPUS (Elsevier), Academic Search Complete (EBSCOhost), ProQuest Dissertations and Theses (Clarivate), PsycINFO (APA), and Web of Science (Clarivate). We also searched for grey literature via Google Scholar and relevant organisational websites encompassing Human Resources/Occupational Health (n = 11), Miscarriage/Early Pregnancy Loss (n = 8) and General (n = 2) (detailed in Protocol 17 ). Finally, we conducted backward and forward citation searches (via hand searches of citation lists and Google Scholar, respectively) on all included documents.
Search strategy
We developed our search strategy using the PCC (population, concept, and context) framework. 19 Search terms were informed by previous reviews.11,24 We developed the search strategy in EMBASE and adapted it for each included information source. We adapted searches for each organisational website, depending on the functionality of the website. Full search strategies for each source are available in Supplementary File B.
Selection of sources of evidence
Identified records were downloaded to Endnote X9 and duplicates automatically identified and removed before being imported into Rayyan software. 25 Two reviewers (RKH and MH) independently screened the titles and abstracts of 25 randomly selected records against the inclusion criteria; 96% agreement was reached and conflicts were resolved through discussion. The remaining titles and abstracts were then screened by the first author, in line with the review protocol. Full texts were subsequently retrieved and independently screened by two reviewers (RKH and MH); conflicts were resolved through discussion with a third reviewer (SL), where necessary.
Data extraction/charting process
Information was extracted and documented from included records in a data extraction table, including specific details about the participants, concept, context, study methods, and key findings relevant to the review questions. Initially two reviewers (RKH and MH) independently extracted data from 10% of included records and met to determine whether approach to data extraction was consistent with the research question and purpose, and captured the data appropriately. One reviewer (RKH) then extracted the remaining data, and these were independently checked by a second reviewer (MH).
Critical appraisal of sources of evidence
In line with guidance on scoping review conduct, we did not appraise the methodological quality or risk of bias of included articles. 19
Collating, summarising, and reporting the results
For quantitative data, descriptives of concepts, populations, or locations, and other data categories were created and are presented within tables, accompanied by narrative summaries. Selected characteristics of included records are presented in graphs and maps, using Excel. For qualitative results, conventional content analysis 26 was used across studies to identify key characteristics.
Results
We identified 26,013 records following database/platform and website searches. Following title and abstract screening (n = 10,938), and subsequent full text review (n = 95), we included 46 records in our review. We identified a further five records following backward and forward citation searches, two of which were included, resulting in the final inclusion of 48 records. Full details are available in the PRISMA flow diagram in Supplementary File C. Excluded records are detailed in Supplementary File D.
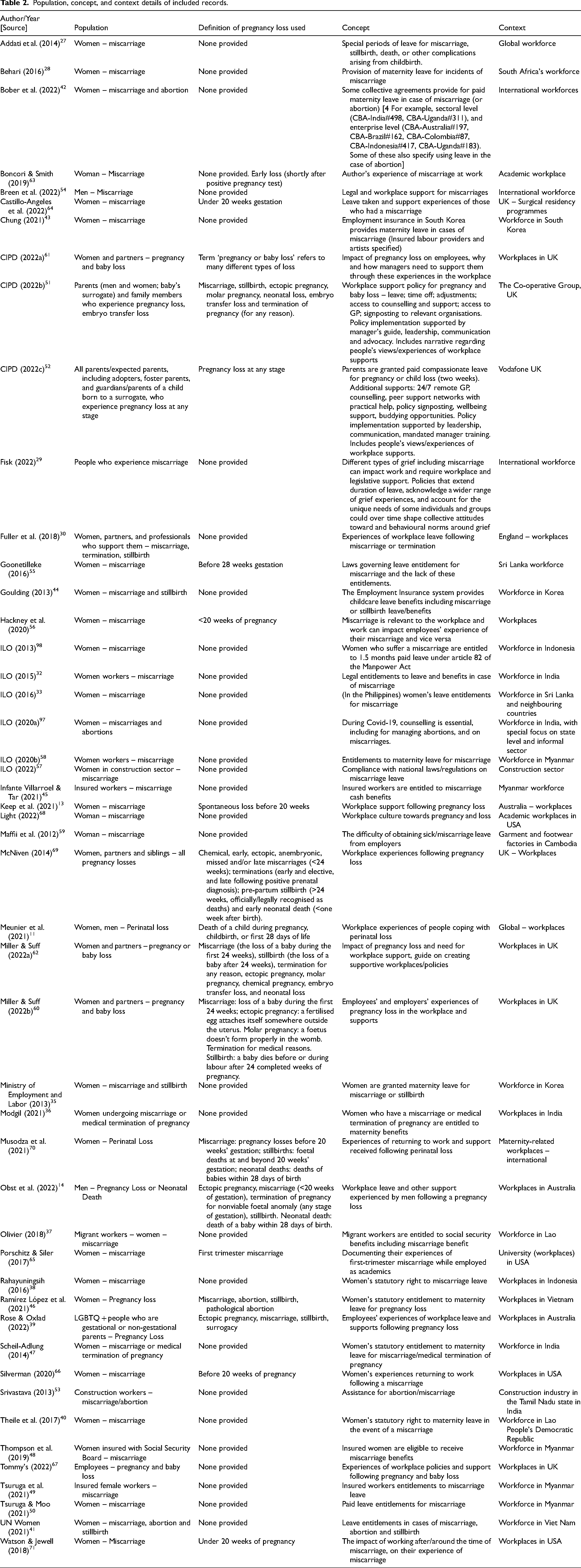
Table 1 provides an overview of the characteristics of included records, by year of publication, country of publication, focus/aim, and methodology, while Table 2 displays the population, concept, and context details of included records.
Characteristics of included records.

Population, concept, and context details of included records.
Characteristics of included records
Records included were published between 2012 and 2022, with an increase in publications in the past three years; 2012–2015 (n = 9); 2016–2019 (n = 11); 2020–2023 (n = 28) (see Figure 1). The majority of records were published in and/or focused on the UK (n = 9), North America (n = 8) and Southeast Asia (n = 13) (Figure 2). Publication types included reports (n = 18), journal articles (n = 15), codes of practice or guides (n = 6), books/book chapters (n = 2), theses (n = 3), and other: case study, note, and training module (n = 4) (see Table 1). Secondary research, including scoping reviews, literature reviews, documentary analysis, and other methods, was the most common type of methodology employed (n = 16). Primary research (n = 13) included qualitative interview studies, quantitative surveys, mixed method surveys, and autoethnographies. Some records (n = 5) employed both primary and secondary research methods, such as desk research and focus groups, or case studies with interviews. The remaining records (n = 14) did not utilise scientific research methods and included narratives, guides, codes of practice, a note and a training module.
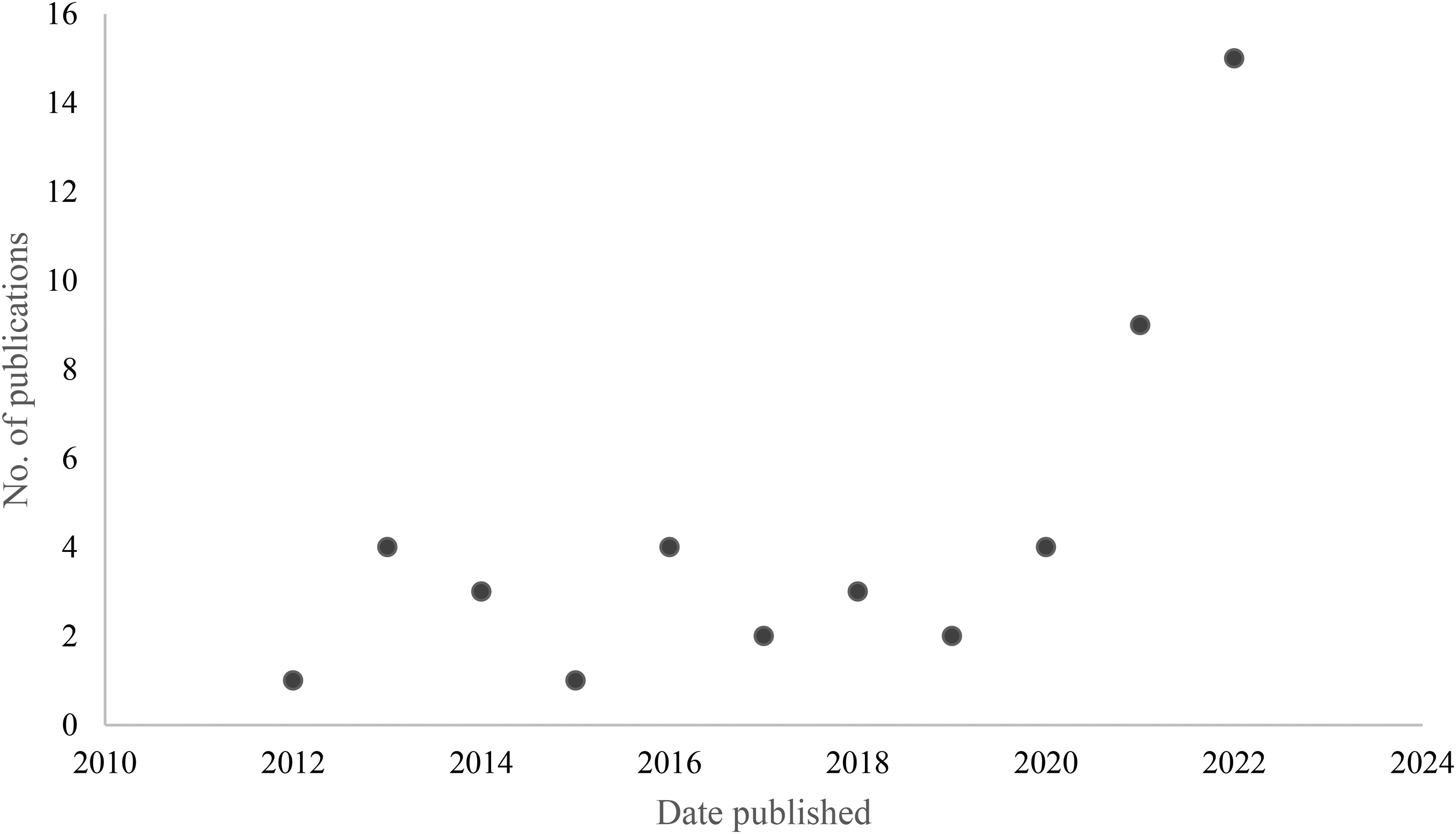
Publication dates of included records (N = 48).

Country of origin of included records (N = 48).
Context
As seen in Table 1 and Figure 2, records spanned most continents, with a concentration of research in Asia (n = 20), North America (n = 7) and Europe (n = 9). Primary research was mainly conducted in high-income countries, while most reports focused on middle-and-lower income countries. As per this review's inclusion criteria, all records included workplace contexts. These included international, national, or industry workforces; workplaces within a particular country, and specific industry workplaces including academia (n = 3), healthcare (n = 2), garment and footwear factories (n = 1), and construction (n = 2) (see Table 2).
Population
Miscarriage was the form of pregnancy loss most commonly discussed in included records (n = 29), though miscarriage was only defined within six records. Among these, ‘less than 20 weeks of pregnancy’ was the most common definition used (n = 5), and one record defined miscarriage as ‘the loss of a pregnancy before 28 weeks gestation’. Some records included all types of pregnancy loss, i.e., losses before and after viability (n = 19). Most records included women experiencing pregnancy loss (n = 33); a minority focused on and/or included men (n = 2). The remainder either included both (n = 9) or did not specify (n = 4).
Concept
Many reports stated or discussed legal rights to time off work or cash benefits following a miscarriage or other pregnancy loss (n = 24). Other records discussed the impact of workplace experiences on pregnancy loss and the need for support and policies (n = 6) or supports for pregnancy loss in specific workforces or workplaces (n = 3). Most records utilising primary research methods, and both scoping reviews, explored participants’ experiences of workplaces and workplace supports following a pregnancy loss (n = 15).
Addressing our research questions
In this review, we first aimed to map the literature with regards to publication characteristics. Secondly, we wanted to examine the literature in relation to two specific issues – workplace supports and experiences of these supports. The results below are presented according to the findings for each research question.
Research question 1: Which workplace supports (e.g., legislative, policy, psychological, social) are, or should be, available to people experiencing pregnancy loss?
Our first research question was addressed by most included records, either through describing or noting existing supports, or illustrating the need for workplace supports to be introduced. Most leave and benefits discussed were a statutory entitlement (n = 15)27–41 while some were achieved through collective agreements (negotiated agreements between trade unions and employers) (n = 2)11,42 and others are available through social insurance and/or only available to insured workers (n = 8).43–50 Certain sectors or workplaces created/implemented their own pregnancy loss supports, as discussed by three records.51–53
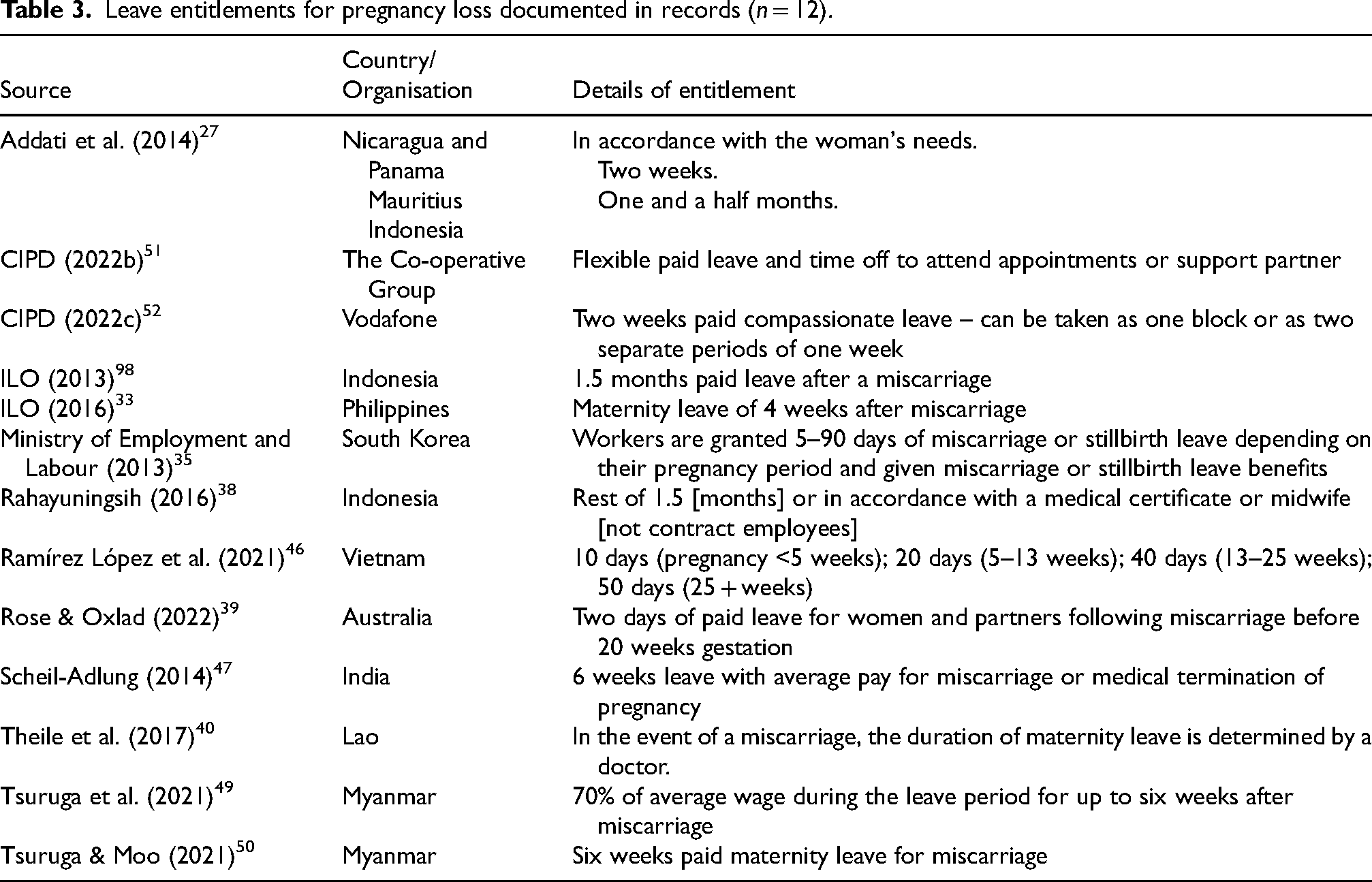
The most common types of supports discussed were leave from work (n = 30)11,27–33,35–38,40–44,46,47,49–52,54–60 and benefits or cash benefits (n = 9).32,36,37,44,45,47–49,57 Many records stated the provision of leave entitlements or benefits in the case of miscarriage with no further detail; where provided, specific information provided is summarised in Table 3 (n = 12 records).
Leave entitlements for pregnancy loss documented in records (n = 12).
Records which discussed workplace policies or collective agreements identified organisational supports such as gradual return to work (n = 2),11,60 flexibility and reasonable adjustments (n = 2),51,60 and training for managers (n = 4).32,51,61,62 Emotional/psychological supports such as counselling, referral to GP, or signposting to peer support groups or relevant organisations were identified by five records.51,52,60,61,62 A minority of records noted or described the need for unspecified supports, provisions, or assistance (n = 3).29,53,55
Research question 2: What are people's views and experiences of workplace supports for pregnancy loss before viability?
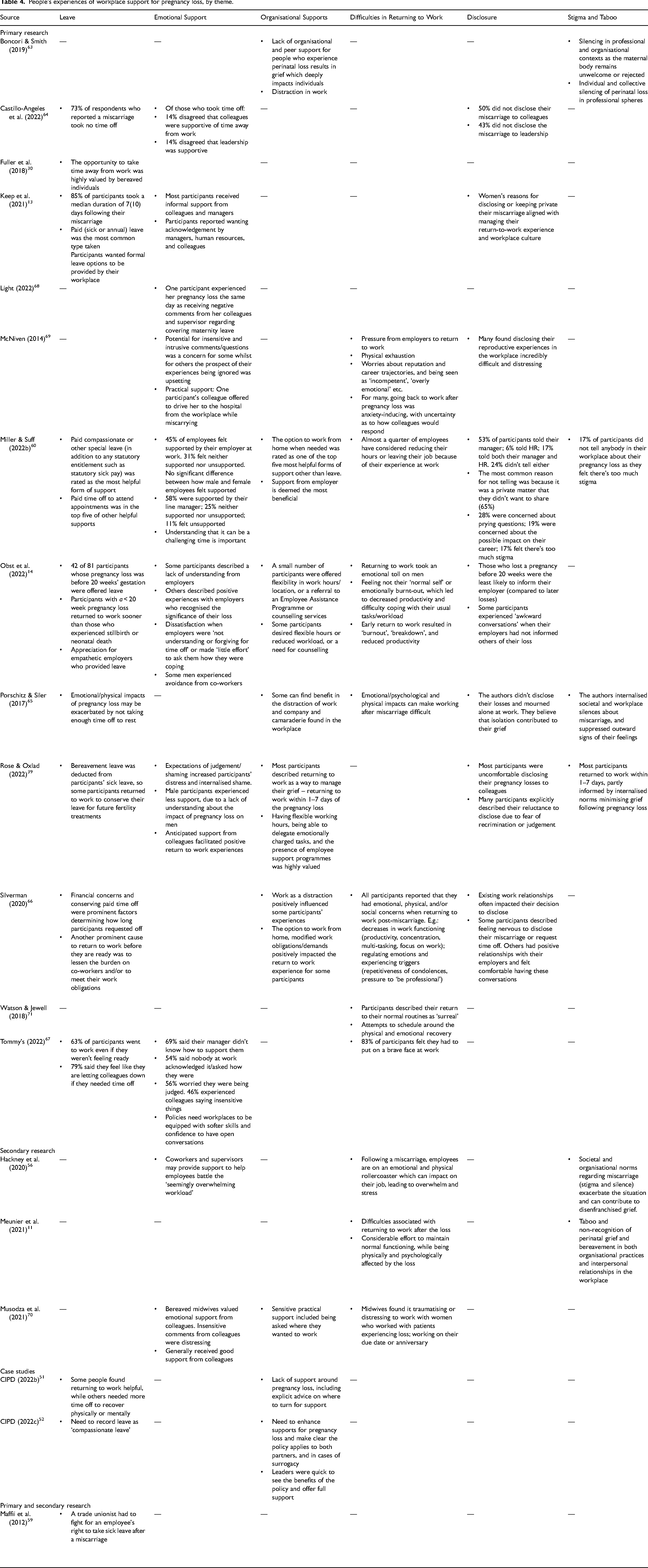
A number of included records utilised primary research methods including–but not limited to–surveys, interviews, and focus groups with people who had lived experience of pregnancy loss (n = 14). These studies examined people's experiences of workplace supports (or lack thereof) for pregnancy loss, and views on these supports. Records utilising secondary research methods including scoping reviews, literature reviews, and case studies (n = 5) also included results or discussion pertaining to experiences of support. The most common themes addressed in the literature, drawing on qualitative and/or quantitative data, are described below and findings from individual records are summarised in Table 4.
People's experiences of workplace support for pregnancy loss, by theme.
Leave from work
Most (n = 13) records explored participants experiences of taking leave from work13,14,30,39,51,52,59,60,63–67 (Table 4). There was heterogeneity in how these records collected data on how much leave participants took, due to methodology used (e.g., quantitative/qualitative) and research focus. Therefore, there is no clear view from the literature of how much leave is needed, or an average of how much is taken. Across records, some participants found returning to work helpful, while others needed time away from work to physically or emotionally recover. Participants generally did not have access to appropriate leave entitlements, and many participants took sick leave, unpaid leave, or were unable to take any leave at all. Participants across the research expressed a desire for paid specific leave.
Emotional support in the workplace
Experiences of collegial or managerial support were reported by 11 records.13,14,39,56,60,64,66–70 The literature found both positive and negative influences that colleagues, supervisors, managers, and employers, could have on participants’ pregnancy loss experiences (Table 4). Sympathy, understanding, and support with workload was valued, while insensitive comments, judgement, or lack of acknowledgement added to participants’ distress.
Organisational supports
Organisational supports were noted by nine records14,39,51,52,56,60,63,66,70 (Table 4). Psychological or medical support through referral to GP, counselling, or Employee Assistance Programmes, were discussed in two records (see Table 4). Records presented available supports, participants’ experiences of these supports, and/or the lack of or need for organisational supports. Generally there is a lack of workplace supports for pregnancy loss, and participants highlighted the need for having the option to work from home, flexibility in hours or workload, and access to counselling.
Difficulties in returning to work
In addition to workplace supports, many studies (n = 10) reported on the difficulties participants faced on returning to work following pregnancy loss.11,14,56,60,65–67,69–71 Physical symptoms, emotional impacts, and interactions in the workplace were cited as impacting the return-to-work experience (Table 4). Attempting to act professional and hide emotions relating to the pregnancy loss was a common difficulty experienced.
Disclosure
Among primary research records, the majority (n = 8) examined participants’ experiences of disclosing their pregnancy loss in their workplace, or choosing to not share it.13,14,39,60,64–66,69 Factors influencing this decision, and responses to disclosure, were discussed across the literature. Many participants did not tell anybody in their workplace about their pregnancy loss, meaning no-one at work knew what they were experiencing. Reasons for non-disclosure included privacy, fear of impact on career, and stigma. Other participants disclosed their pregnancy loss at work, and often found this experience to be uncomfortable or distressing. Participants were motivated to share to access leave or supports, to counteract stigma, or because they had positive relationships in the workplace.
Stigma and taboo
The prevalence and impact of the silence, stigma, and taboo surrounding pregnancy loss was noted in several records (n = 6).11,39,56,60,63,65 Pregnancy loss, especially early pregnancy loss, is often not discussed in society, and particularly not in workplaces. The lack of knowledge, understanding, and conversations surrounding pregnancy loss is posed as a barrier to support across the literature. Included studies show how stigma can enhance difficulties surrounding disclosure, accessing leave, acknowledgement from colleagues, and managing emotions upon return to work.39,60,63,65
Discussion
The aim of this scoping review was to examine the literature pertaining to workplace supports for pregnancy loss before viability, and to identify gaps in the literature. We found a lack of empirical work on this topic, although there has been a notable increase in primary studies in the past five years. Most included records were reports or narratives, many of which concentrated on South-East Asia. Records utilising primary research methods were mainly from Australia and North America, and thus have particular relevance to high-income countries.
Research question 1: Which workplace supports (e.g., legislative, policy, psychological, social) are, or should be, available for people who experience pregnancy loss before viability?
Our findings show that more is needed to adequately respond to workers’ needs. Empirical studies included in this review demonstrate the range and extent of concerns that workers face when returning to the workplace following pregnancy loss, including dealing with the physical and emotional impacts of pregnancy loss, navigating conversations and relationships in the workplace, and managing the workload while potentially feeling unwell or distressed. Pregnancy loss affects many workers throughout the world. Women who carry the pregnancy can face ongoing physical effects including cramping and bleeding, 72 and further complications if medical or surgical management is required. 73 Additionally, both women and men can experience emotional, psychological, and social impacts of pregnancy loss. It is common to experience a period of grief; 74 intense sadness; 75 and isolation. 76 Pregnancy loss also increases the risk of anxiety, depression, and post-traumatic stress disorder.1,2,77–79 Because of the prevalence and extent of these impacts, it is important that people are supported by their workplaces at a time of potential physical and/or emotional suffering.
Legislative supports for pregnancy loss, in the form of leave and benefits, are primarily found in middle-and-lower income countries, according to the records included in this review. This is reflective of international legislation, whereby high-income countries such as New Zealand and Australia have recently introduced statutory pregnancy loss leave, while lower-and-middle income countries such as China 80 and India 81 have had miscarriage leave since the 1950s and 1960s. 82 Recent years have seen a growing awareness of early pregnancy loss and its impacts, which has resulted in several jurisdictions considering the introduction of pregnancy loss leave; these include Northern Ireland, 83 Alberta, 84 Nova Scotia 85 and Catalunya. 86 As such, further research will be needed to explore the efficacy of newly introduced leave.
Companies and organisations are increasingly investing in workers’ health through workplace adaptation and provision of healthcare, which can save costs through preventing sickness absence, presenteeism, turnover, and loss of creativity.
87
In addition to, or in the absence of, statutory supports, individual workplaces can create pregnancy loss policies which include leave entitlements, practical supports and accommodations for employees returning to work, and training and awareness raising for management or staff. Practical supports found in this review include working from home; flexible working hours; being able to change the location where they work/delegate emotionally charged tasks; reduced workload; modified work demands. Psychological supports for pregnancy loss were infrequently found within this literature, but participants expressed a need for counselling or peer support through Employee Assistance Programmes. This is reflective of the psychological impact of pregnancy loss and the increased risk of depression and anxiety.
2
Social support from management and colleagues were hampered by a lack of awareness and understanding of early pregnancy loss experiences. The lack of understanding about pregnancy loss faced by workers may be alleviated by joining peer support groups, which some workplaces provide referrals to.
52
Taboo and stigma was a factor which reduced the likelihood of disclosure of pregnancy loss, which is often required to access support. Alongside organisational and professional supports, education and awareness-raising in workplaces is essential to support workers’ who are returning to work following a pregnancy loss.
Research question 2: What are people's experiences of workplace supports for pregnancy loss before viability?
While there is a general lack of research in this area, recent primary studies have investigated participants’ experiences of leave provisions or supports in their workplace following a pregnancy loss. Across workplaces and countries, participants’ experiences reported in the publications in this review vary from a total lack of support from their workplace, to a positive return to work. There is variation in the type and length of leave available; the option of working accommodations; and the reactions and support from colleagues and management towards employees who experience pregnancy loss. Recently published and ongoing studies will further inform the growing evidence base in this area.88,89
In addition to the benefits of support policies and programmes to employees, it is important to highlight the advantages to workplaces of supporting and promoting their workers’ health and wellbeing. Poor physical or mental health can result in presenteeism, loss of productivity, reduced creativity, and increased absence, all of which is costly to companies. Conversely, improving work conditions or offering health initiatives results in productivity gains and sickness absence reduction. 87 A meta-analysis of a variety of workplace health promotion programmes found small improvements in outcomes such as sickness absence, work productivity, and work ability. 90 The World Health Organisation recognises the strategic advantage to workplaces of promoting and supporting workers’ health, alongside the moral and sometimes legal obligation to do so. 91 The EU Occupational Safety and Health Association has also found that poor workplace safety and health costs money, and it is worthwhile for companies to invest in their workers’ health. 92
What is the scope of the current evidence and are there any gaps in the research?
While our search strategy yielded over 10,000 results and this review includes 48 records, there is a lack of empirical evidence examining workplace supports for pregnancy loss and people's experiences thereof. Furthermore, of the small number of empirical studies included in this review, 11 included participants who had experienced all types of pregnancy loss, which further limits the extent of evidence available for workplace experiences of pregnancy loss before viability. Many of these studies are very recent (within the past three years), which illustrates the growing awareness and attention on early pregnancy loss worldwide. While many of the reports addressed low-and-middle-income countries, all of the included empirical work was conducted in high-income countries. Furthermore, most reports were examining workers’ rights across all aspects of working life, not focusing specifically on pregnancy loss; as such, the information pertaining to pregnancy loss supports was often vague or brief. Many journal articles included discuss the lack of awareness, discussion, and education surrounding pregnancy loss. The lack of research in this area supports this finding.
In addition to the lack of research in this area, pregnancy loss in the workplace would not appear to be given due attention by organisations which focus on occupational health, given that we did not identify any eligible records from the websites of European Union 93 and United States of America 94 occupational health bodies. However, an exception – and example of guidance for workplaces in Canada – describes what a miscarriage is and what workplaces can do to support workers’ experiencing pregnancy loss. 95 Following on from new research and legislation, guidance from national and international organisations is needed to promote workplace policies and training.
Future research needs to examine the need for, implementation, and impact of workplace supports such as leave (including the optimum duration of same), practical accommodations, and training and education of managers and colleagues about pregnancy loss experiences.
Strengths and limitations
A strength of this work is the involvement of knowledge users, from inception, in the review; such engagement improves the relevance of the research and will also enhance the dissemination and implementation of research findings. 96 Furthermore, we did not restrict by language or geographical location, and included grey literature sources. Our results demonstrate the importance of the latter, given the dearth of empirical work identified. There are some limitations, however. We did not include media reports within our scoping review, in order to keep our review manageable, within the available resources and timelines. We have observed much media reporting of issues relating to pregnancy loss in the workplace in recent years, and this is indeed an area for future research. In addition, we did not conduct general internet searches to identify company policies/supports, or searches of legislative sources; we will examine these separately. 9
Conclusion
Our scoping review of literature published in the past 10 years, has identified a lack of research and broader literature internationally on workplace supports and experiences of early pregnancy loss. Most reports included in our review focused on middle-and-lower-income countries. In recent years, there has been an increase in primary research on workplace experiences of pregnancy loss in high-income countries. This highlights various issues that workers face when returning to work following pregnancy loss, including navigating the physical and emotional impacts, workplace conversations and relationships, and workloads. Our review identified measures such as leave, flexible working arrangements, and access to support, which organisations can implement to support their employees experiencing pregnancy loss. Education and awareness-raising initiatives in workplaces are also required to enable supportive cultures. Further qualitative and quantitative primary research is needed to understand workplace experiences of pregnancy loss, to inform the development and implementation of supports, including appropriate legislation and guidance for organisations on the introduction of pregnancy loss supports to the workplace.
Supplemental Material
sj-docx-1-wor-10.1177_10519815241305007 - Supplemental material for Workplace supports for early pregnancy loss: A scoping review of international literature
Supplemental material, sj-docx-1-wor-10.1177_10519815241305007 for Workplace supports for early pregnancy loss: A scoping review of international literature by Ruadh Kelly-Harrington, Sara Leitao, Keelin O'Donoghue, Caroline Dalton-O'Connor, Mary Donnelly, Claire Murray, Daniel Nuzum, Maeve O'Sullivan and Marita Hennessy in WORK
Footnotes
Acknowledgements
Not applicable.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Funding
This work was supported by the Department of Children, Equality, Disability, Integration and Youth, Ireland. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.