
Abstract
Background
Olive pickers confront ergonomic hazards when performing work activities that may lead to musculoskeletal pain (MSK) that must be adequately managed. The success of MSK pain prevention and treatment strategies is linked to olive pickers’ state of empowerment, shaped by expectations and beliefs.
Objective
This study highlighted the prevalence of MSK pain among Italian olive pickers and explored their attitudes, expectations, and beliefs about MSK pain prevention and care.
Methods
A web-based cross-sectional survey instrument was developed to collect data from an Italian olive pickers’ cohort in the Liguria region. The survey investigated the sample on (1) MSK pain prevalence and characteristics, (2) preventive and treatment activities for MSK pain, (3) expectations about MSK pain treatments, and (4) beliefs about their job and MSK pain onset.
Results
From January to July 2021, we collected data from 127 participants (78% men); mean age 52 ± 13). Prevalence of MSK pain over one month, six months, and one year was 61.6%, 77.8%, and 84.8%, respectively. The most affected joints were the lumbar spine (61%), the shoulders (57%), and the cervical spine (46%). To prevent the onset of MSK pain, 44% of participants did nothing, and 94% of them never attended any preventive physical activity.
Conclusions
MSK pain strongly impacts Ligurian olive pickers, as three out of four experienced it during the last six months. Participants emphasised the need to be educated on working ergonomics and the perceived importance of physical activity for health.
Keywords
Introduction
Olive oil is a cornerstone of the Mediterranean diet, and its consumption is associated with increased longevity and a lower incidence of chronic diseases, including cardiovascular diseases and cancer.1–3 Italy ranks as the second largest producer of olive oil in the European Union, contributing 17% of the total production, 4 counting 619.375 olive oil agriculture businesses across the country. 5 Specifically, one of the Italian regions, Liguria, stands out as a major producer of the “Taggiasca” olive type globally, yielding approximately 22.000 quintals of these olives per year 5 and 7.333 olive oil agricultural businesses. 5 The unique characteristics of the Ligurian terrain, comprised of both mountainous and hilly lands, make the use and transport of machines impractical, requiring predominantly manual labour for harvesting.
Olive pickers, responsible for harvesting olives, routinely face ergonomic hazards 6 such as repeatedly moving weights around 20 Kg, sustaining postures with arms overhead, and exposure to vibrations produced by the hands-held olive harvester.7,8 Therefore, olive picking is a strenuous work characterised by manual handling of loads often not performed with the proper technique, repetitive movements, and vibrations9–14 that in the long run may lead to worse frailty even if active during retirement. 15 Consequently, these risks may elevate the likelihood of developing musculoskeletal (MSK) pain, which is the result of different rheumatic and musculoskeletal conditions, including rheumatoid arthritis, osteoarthritis, low back, shoulder, and knee pain.8,16 These conditions affect 27.7% of the population, totalling 17.3 million people. 17 They contribute to years lived with disability (YLD) 9 and have substantial social and economic implications for society. 18 Nevertheless, few studies have yet explored the prevalence of MSK pain in olive pickers.
Barneo-Alcantara M. et al., Proto A.R. and Zimbalatti G. have explored the risks of biomechanical overload that olive pickers run during their daily work, highlighting how different types of ailments are frequent in this population.7,8 Specifically, Barneo-Alcantara M. et al. evaluated musculoskeletal risks among olive pickers in Jaén, Spain, identifying high-risk tasks such as pruning and harvesting and adopting the ‘Standardised Nordic Questionnaire’ (NMQ). They highlighted prevalent neck, back, and knee pain, with mechanisation reducing some physical load. 8 Proto A.R. and Zimbalatti G., instead, analysed the risk of repetitive manual operations by interviewing 430 olive pickers in Calabria, Italy, using the Occupational Repetitive Actions checklist (OCRA). They found that activities such as harvesting and pruning are at high risk of exposure to MSK pain due to repetitive movements and awkward postures. 7 Both studies emphasised the implementation of interventions to prevent MSK pain.
The non-pharmacological management and prevention of MSK pain is based on education for acquiring self-management skills, including diet adjustments, physical activity, and exercise.19–21 These strategies need to be intertwined in everyday life, making individuals empowered by encouraging the adoption of virtuous behaviours and actions affecting both health and life control. 22 Personal expectations and beliefs about one's capability and MSK pain treatments shape individual empowerment, affecting the capacity to self-manage one's own health.21,22 Thus, this study focused on exploring the prevalence of MSK pain among Italian olive pickers and their attitudes, expectations, and beliefs about MSK pain care. Exploring these constructs may, in the future, inform the development of tailored educational programmes to improve the empowerment and care of MSK pain.
Methods
The report of this observational study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations. 23
Survey development and dissemination
A quantitative web-based cross-sectional survey instrument was developed according to the ‘International Handbook of Survey Methodology’. 24 Specifically, the development process followed the ‘Three stages of testing’. The choice to adopt an Internet survey was driven by the need to reach as many participants as possible due to the explorative aim of this study. Since no literature on our topic of interest was found, SB, MT, and LS co-created the survey with patient and public involvement. They contacted ten olive pickers and met them to discuss the most relevant aspects of their job and the most common pains they experienced during the harvesting (‘Developmental Stage’). Based on these results, SB, MT, and LS created the first survey instrument with RG, who played the role of patient partner, participating in all phases of the survey's development (planning, development, and dissemination of the online questionnaire) and assessing its relevance (‘Question Testing Stage’). The writing questions phase design followed the framework of Roger T. et al.: (a) understand the question; (b) Have or retrieve information needed to answer the question; (c) translate relevant information into the form required to answer the question; (d) provide the answer by entering it into a computer. 25 Then, the draft was presented again to the participants of the previous meeting to test its relevance and understandability (‘Dress Rehearsal Stage’). Their feedback was then included in a new draft tested on a sample of five physiotherapists experts in rehabilitation for rheumatic and musculoskeletal diseases to ensure the clinicians’ perspective. After including the clinicians’ feedback, the final draft was compiled and disseminated online by ‘Microsoft Forms Suite Office 365’, a secure and safe application that respects the European General Data Protection Regulations. The ten olive pickers who participated in the development of the survey did not compile the survey and were not included among the participants’ results of this study. The questionnaire proposed to participants was delivered in Italian and included a brief cover letter, the data treatment, and the informed consent highlighting the study's aims.
Survey characteristics
The survey investigated (1) the prevalence and characteristics of MSK pain among Italian olive pickers, (2) whether they did any activities to prevent the onset of MSK pain and how they managed it once it developed, and (3) the sample's beliefs and expectations about the relationship between their job and MSK pain. Specifically, the survey included 47 questions divided into seven sections (Supplementary File 1). Questions 1–3 corresponded to the subscription of the informed consent. Questions 4–12 (1st section – Descriptive analysis) investigated the participants’ sociodemographic characteristics (e.g., gender they identified with, age, nationality, years of experience). Questions 13–26 (2nd section – Participants’ working characteristics and preparation) investigated the job characteristics of the participants (e.g., working position, work experience, daily working hours, etc.) and how they prepared themselves for their work routine (e.g., preliminary physical preparation). Questions 27–34 (3rd section – Prevalence of MSK pain) investigated the prevalence over one month, six months and one year, and the characteristics of MSK pain, such as the body part of interest and the characteristics of the experienced pain and its intensity addressed with a Numeric Rating Scale 0–10. 26 Questions 34–44 (4th section – Workers’ attitudes towards MSK pain and coping strategies) investigated the strategies adopted by olive pickers to manage or prevent MSK pain (e.g., if they referred to a health professional, what were their treatments if they tended to avoid some movements, etc.). Question 45 (5th section – Expectations towards health professionals) investigated the participants’ expectations when they were referred to a health professional. Question 46 (6th section – Beliefs towards olive picker work) and question 47 (7th section – Beliefs about the cure of MSK pain) presented respectively seven statements regarding the beliefs of olive pickers towards their work attitudes and nine statements about their management of MSK pain. In both sections, the participants indicated to what extent they agreed with those statements through a 5-point Likert scale (0: Strongly disagree; 1: Partially disagree; 2: Neither agree nor disagree; 3: Partially Agree; 4: Strongly Agree).
Participants
This online questionnaire was addressed to Italian olive pickers based in Imperia, a province of the “Liguria” region. Inclusion criteria required to be olive pickers working in the Liguria region, in Italy, regardless of their working experience, gender, or nationality. No specific exclusion criteria were set. Participants were informed in advance both about the time required to complete the questionnaire (15–20 min) and the anonymity of the information collected. Olive pickers were reached thanks to the collaboration of the Italian labour union “Confederation of Agricultural Producers – Italian Farmers of Imperia” (CAP) in Imperia. This modality prevented any coverage error, as there was a clear population target. 24 Filling in the questionnaire was entirely voluntary, and no incentives were provided. Participants who declared not to give their digital consent were excluded and could not proceed with the compilation of the survey.
Data analysis
For the analysis of the results, continuous variables were reported as mean ± standard deviation (SD), while categorical variables were reported as absolute and frequency percentages. Descriptive statistics were performed to identify sociodemographic and working characteristics (1st and 2nd section) and highlight our sample's demographic, clinical, and working features. For MSK pain prevalence (3rd section), a point prevalence estimation and the 95% confidence intervals were calculated over the total olive pickers using the Stata command ‘proportion’. The prevalence was estimated at one month, six months and one year. These times were chosen to try to understand the frequency of MSK pain over one year. We performed a descriptive analysis to investigate what olive pickers did to prevent and manage MSK pain (4th section). The sample's expectations towards health professionals (5th section) were analysed with a frequency descriptive analysis, and the results were reported in percentages. To analyse the sample's beliefs (6th and 7th section), we conducted a descriptive analysis reporting the percentage of participants’ agreement and visualising it with bar charts for each statement. Participants who partially or totally agreed on a Likert scale (score 4–5) were considered to agree with the statements. In line with Delphi studies, 70% of the consensus was the agreement threshold.27–29 No missing or dropout data were found, as Microsoft Forms does not allow recording participants’ data unless they answered all the questions.
Results
From January to July 2021 the survey was distributed to the 512 olive pickers located in Imperia and affiliated with the CAP labour union. A total number of 127 participants (response rate: 25%) partook in the study (99 men (78%); 28 women (22); mean age 52 ± 13). The sociodemographic data of the sample is reported in Table 1.
Participants’ sociodemographic characteristics.
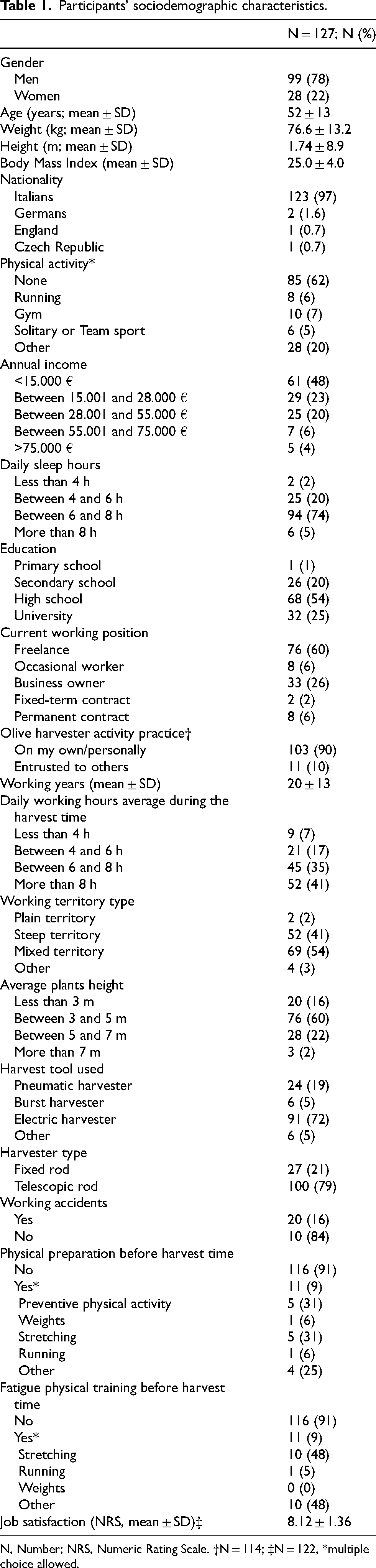
N, Number; NRS, Numeric Rating Scale. †N = 114; ‡N = 122, *multiple choice allowed.
Table 2 reports the prevalence and other characteristics of MSK pain. Prevalence of MSK pain over one month, six months, and one year were respectively 61.6% (95% confidence interval [51.3%–71.2%]), 77.8% [68.3%–85.5%], and 84.8% [76.3%–91.2%]. The most affected joints were the lumbar spine (62.5%), the shoulders (57%), and the cervical spine (46.1%). The pain was experienced during the harvesting period and at the end of it, respectively, by 63% and 30% of the participants.
Prevalence and characteristics of MSK pain.
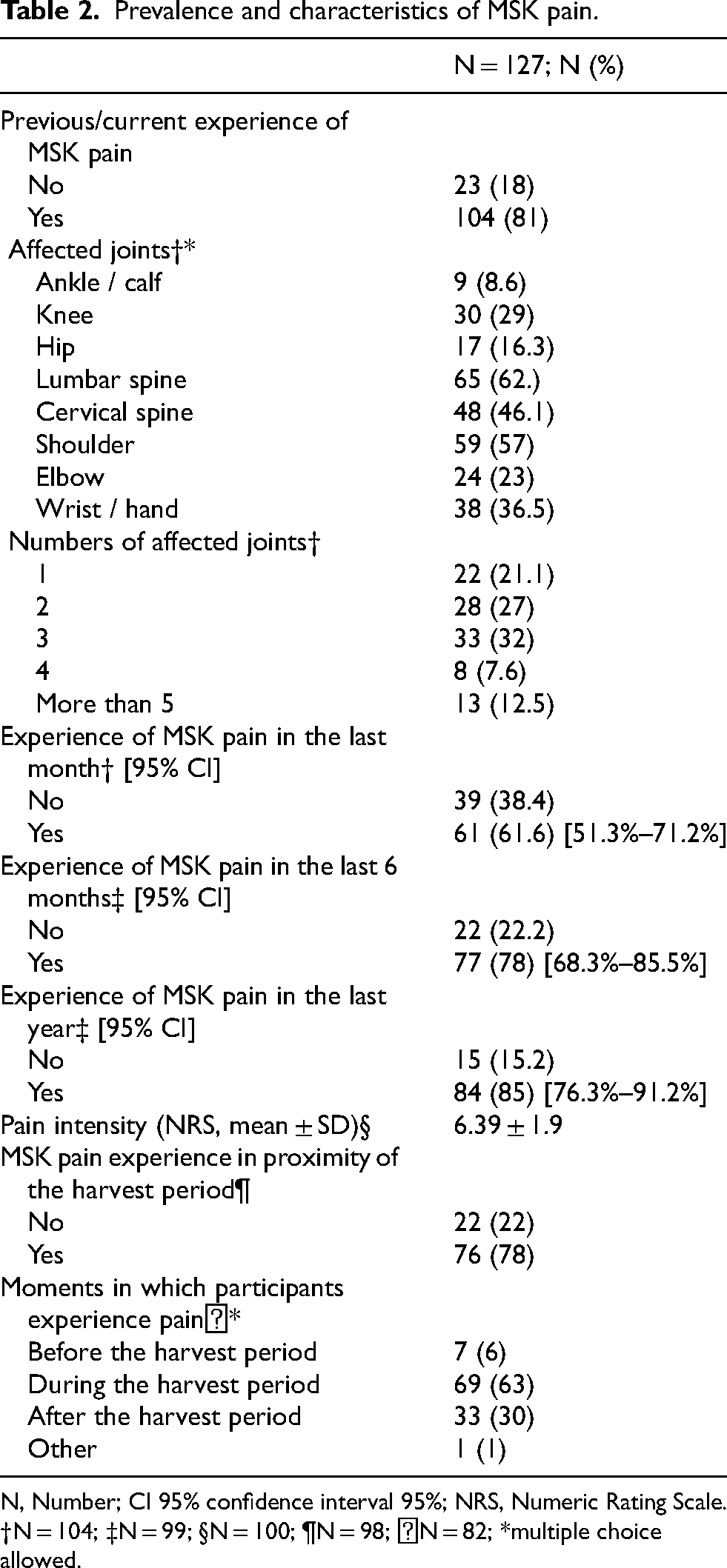
N, Number; CI 95% confidence interval 95%; NRS, Numeric Rating Scale. †N = 104; ‡N = 99; §N = 100; ¶N = 98; ꬷN = 82; *multiple choice allowed.
Table 3 reports the workers’ attitudes towards MSK pain and their coping strategies. Among all participants, due to pain, 62% decided to consult a healthcare professional. Notably, 44% of participants did nothing to prevent the onset of MSK pain, while 94% never attended a preventive physical activity course for their profession. To reduce pain, 41% of participants took painkillers or anti-inflammatory drugs, while 32% used natural creams (e.g., arnica, devil's claw). Roughly 63% of the participants reported avoiding specific movements, and 40% were afraid that movement could enhance their pain.
Workers’ attitudes towards MSK pain and coping strategies.
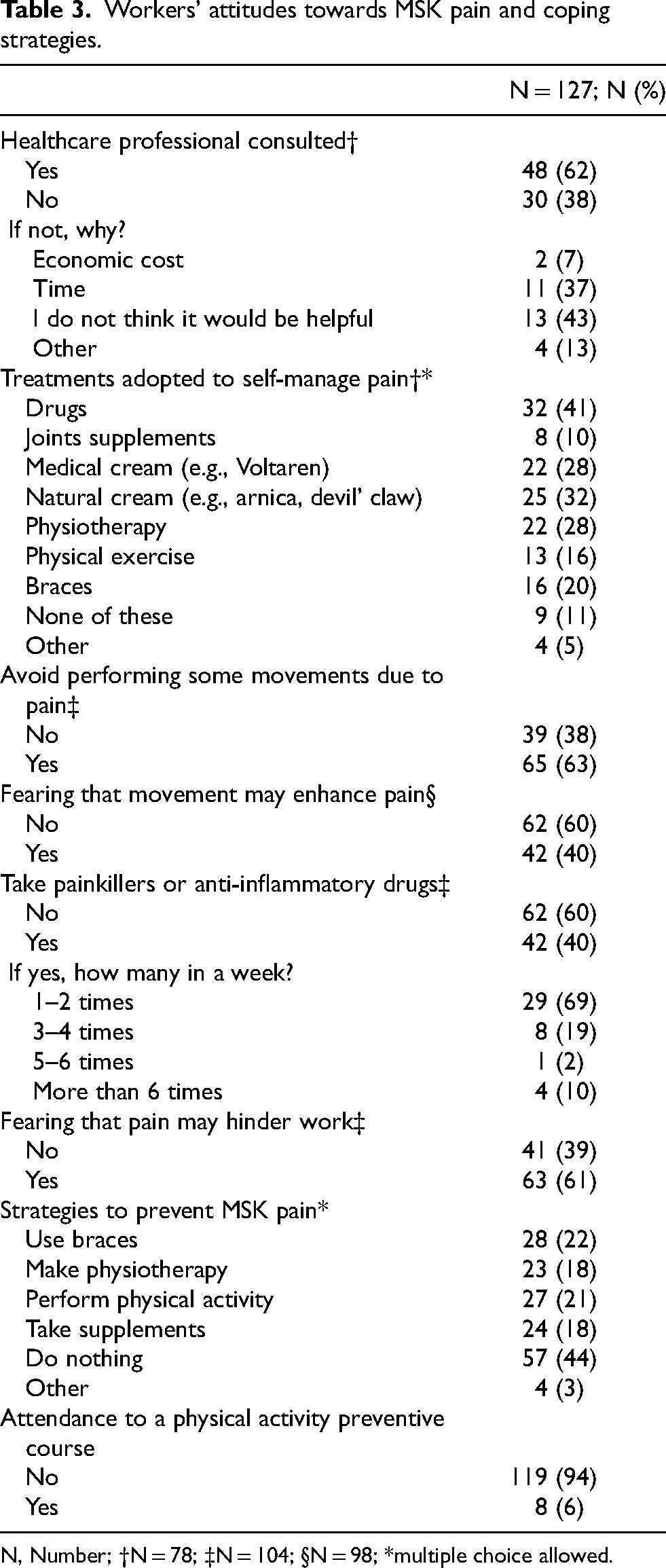
N, Number; †N = 78; ‡N = 104; §N = 98; *multiple choice allowed.
Table 4 reports the participants’ expectations towards health professionals. Specifically, participants expected to be educated on the correct movements to perform (62%) and to receive manual treatments (46%) from health professionals.
Participants’ expectations towards health professionals (multiple answers).
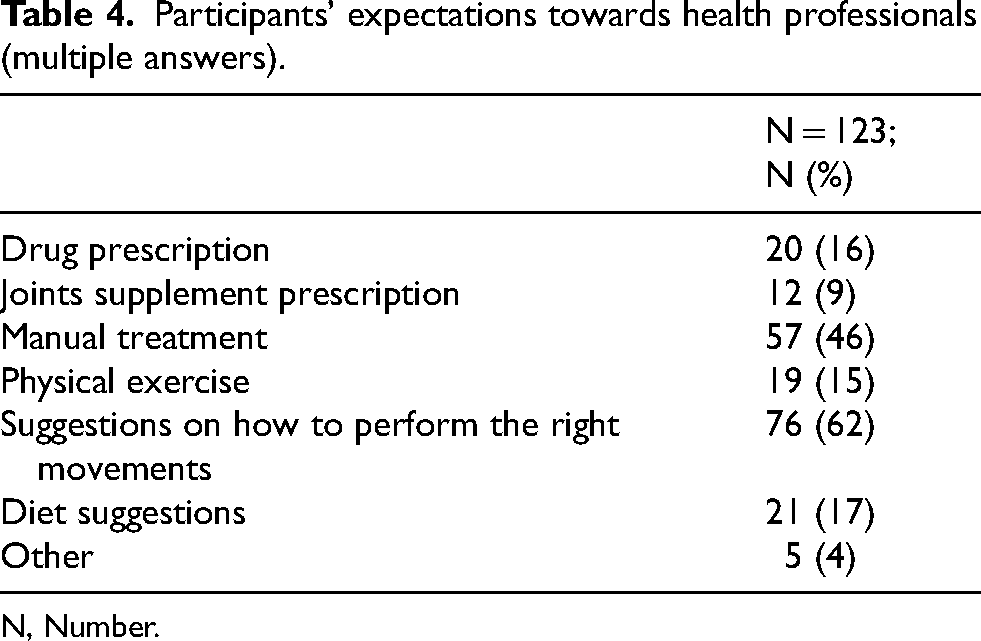
N, Number.
Figures 1 and 2 report the charts of participants’ beliefs towards olive pickers’ work and MSK pain care. Distinctly, the participants agreed for more than 70% that a straight spine was crucial for their health (89%), that during their work, they had to take uncomfortable but necessary postures (77.9%), and that their job was tiring for their joints (73.3%). As far as beliefs about MSK pain care, participants believed that physical activity was important for their joint wellness (82%), that prevention of MSK pain (i.e., physical activity, ergonomics) is important for their health (77.9%), and that taking care of their joints pain was necessary (72.4%). Notably, the participants disagreed with identifying the costs of healthcare as a barrier to referring to a clinician or a physiotherapist (81% of disagreement).
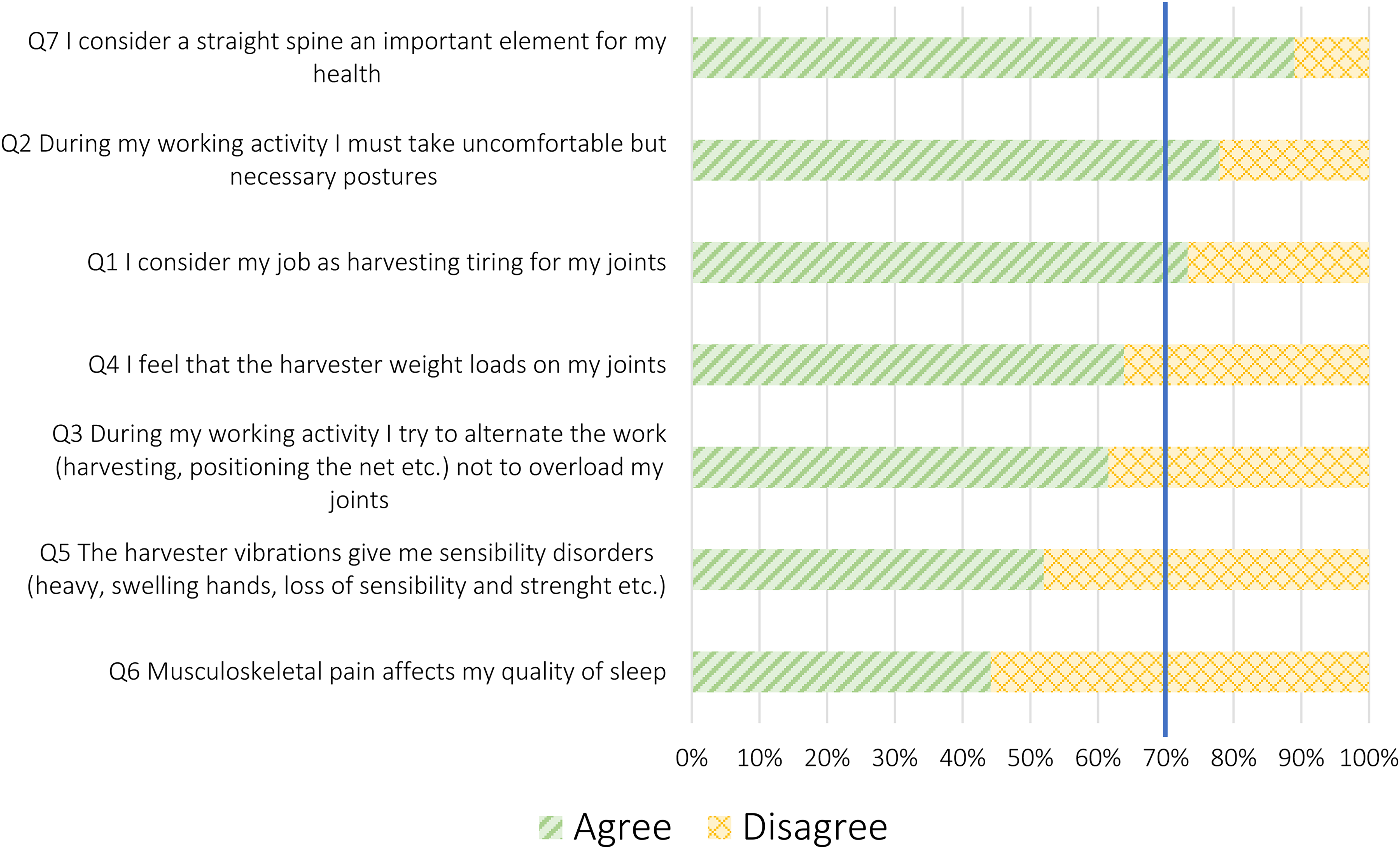
Beliefs towards olive pickers’ work.
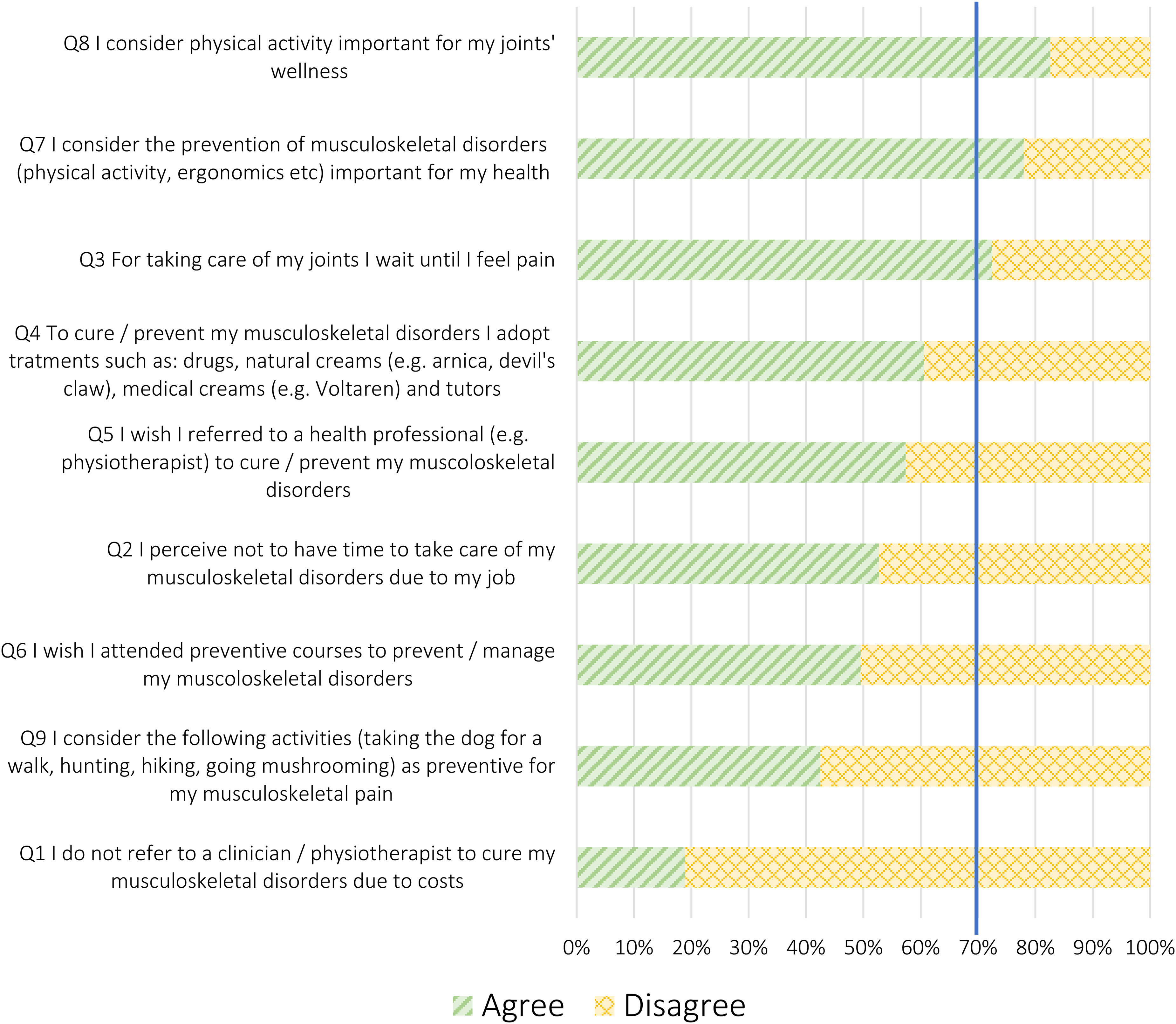
Beliefs about the cure of MSK pain.
Discussion
This quantitative web-based cross-sectional survey study explored the prevalence of MSK pain in a sample of Ligurian (Italy) olive pickers and their attitudes, expectations, and beliefs about MSK pain care.
Regarding prevalence, half of Ligurian olive pickers experienced moderate MSK pain over a year. Specifically, over one year, almost 85% of olive pickers experience MSK pain, which is much greater than the percentage that affects the general population (between 13.5% and 47%). 30 While the MSK pain localisation was predominant in the shoulders, cervical and lumbar spine, with an increased frequency during the harvest time. These findings align with the existing literature highlighting similar patterns in MSK pain joint locations in the shoulders and upper and lower back in olive pickers.7,8
For 63% of the participants, MSK pain posed a significant obstacle, leading to fear-avoidance behaviour. Such avoidance can negatively impact the healing process, fostering catastrophic thinking, pain-intensity amplification, anticipation of pain, and prolonged avoidance of physical activity, which can cause deconditioning of the musculoskeletal and cardiovascular systems, 31 facilitating the onset of chronic MSK pain.31,32 Moreover, fear-avoidance behaviour might also affect the work quality and performance of olive pickers, leading to sickness absence. 33 It is noteworthy that our study did not measure the level of fear avoidance in the sample. Therefore, future studies might investigate these beliefs by adopting specific tools such as the Fear Avoidance Beliefs Questionnaire. 34
Surprisingly, nearly half of the participants reported taking no preventive measures against MSK pain onset, emphasising a lack of instruction on prevention or management strategies. This underscored the need to fill this gap through educative campaigns or interventions focused on ergonomic training and health education. These elements are fundamental for reducing the prevalence of MSK pain and their impact on the quality of life of agricultural workers. 35 Currently, the participants tend to self-manage their pain, mainly relying on the use of painkillers or anti-inflammatory drugs. Even though these drugs can help manage acute pain, important risks are associated with their chronic use, especially when abused. 36 Most likely participants had poor awareness of the non-pharmacological management strategies of MSK pain, such as lifestyle changes, education on weight loss, and individualised exercise regimen, which are considered first-line interventions for many rheumatic and musculoskeletal diseases.37–39
Among these beliefs, olive pickers trusted that posture played a significant role in their joints’ health and that their job was physically tiring, especially due to the forced posture they needed to take and maintain. Moreover, when consulting with a health professional, participants were mostly expecting manual treatment and to be educated on the right movements to perform while working. These findings suggest that participants relied on a postural-structural-biomechanical model to understand their joints’ health and that passive treatments are sufficient to recover. However, posture has been proven unreliable in assessing and understanding musculoskeletal pain as the current evidence does not support the ideas of ‘good’ and ‘bad’ postures linked to pain.40,41 Moreover, participants reported not alternating the work tasks so as not to overload their joints, even though this has been proven to be an effective strategy for preventing MSK pain. 41 Eventually, pain onset was the main trigger to consult a physician or physiotherapist, as also reported in the literature.42,43 Finally, participants acknowledged the importance of prevention and physical activity for wellness but did not engage in preventive programs.
Several limitations in this work and on the outcomes need to be addressed, including the cross-sectional design preventing causal relationships, potential recall biases, gender imbalances and the low response rate. Therefore, we could not establish causal relationships between olive picking and the onset of MSK pain. While we can report a certain prevalence of pain among participants, we cannot conclude that it is solely attributable to their profession, as we did not collect data on prior injuries or other potential contributing factors. This limitation emphasises the need for caution when interpreting the results and highlights the importance of longitudinal studies to explore causal links further. In addition, there is a possibility of selection bias, as those experiencing MSK pain may have been more inclined to participate. Future cohort studies with specific outcome measures could further explore the impact of MSK pain on life and work. On the other hand, this study is the first one that thoroughly explored the prevalence and characteristics of MSK pain, as well as the attitudes, expectations, and beliefs about MSK pain care in a specific population of olive pickers. It should be noted that we were unable to differentiate between acute and chronic pain and that we only evaluated MSK pain. Therefore, we did not examine specific rheumatic and musculoskeletal diseases. For future research, we recommend adopting specific standardised tools to measure and differentiate pain types. Moreover, it is noteworthy how, in our study, there was a robust integration of patient and public involvement throughout all phases, enriching every aspect of our research and making it relevant for olive pickers.
Conclusion
MSK pain significantly impacts Ligurian olive pickers, since three out of four experienced them during the last six months. Education is crucial to provide effective strategies for MSK pain prevention and management. Olive pickers emphasised the need for ergonomic education and recognised the importance of physical activity. Future research should further validate these findings in a broader sample and assess the efficacy of educational programs on ergonomics and physical activity for preventing and managing MSK pain among olive pickers.
Supplemental Material
sj-docx-1-wor-10.1177_10519815241304999 - Supplemental material for Exploring musculoskeletal pain among Italian olive pickers: A cross-sectional investigation into prevalence, attitudes, expectations, and beliefs
Supplemental material, sj-docx-1-wor-10.1177_10519815241304999 for Exploring musculoskeletal pain among Italian olive pickers: A cross-sectional investigation into prevalence, attitudes, expectations, and beliefs by Benedetto Giardulli, Simone Battista, Lucia Grazia Sansone, Gaia Leuzzi, Riccardo Giordano and Marco Testa in WORK
Footnotes
Acknowledgements
This work was supported by the Italian regional activity: “Measure 16.1 of the Rural Development Programme 2016–2020 of the Liguria Region IEP”. This work was developed within the DINOGMI Department of Excellence framework of MIUR 2018–2022 (Legge 232 del 2016).
Ethics approval
This observational study was conducted according to the Declaration of Helsinki and its reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations. Ethical approval was obtained from the Ethics Committee of the University of Genova (approval date: 17/02/2022; CERA2022.14). The participants have given their digital informed consent before partaking in the study.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
The authors affirm that human research participants provided informed consent for publication, however, in our study, we did not take any images or videos.
Author contributions
All authors made substantial contributions to the conception, design of the work, acquisition, analysis, or interpretation of the data. All authors drafted the manuscript or revised it critically for important intellectual content. All authors approved the publication of the final version of the manuscript. All authors agreed to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.