
Abstract
Background
Systematic reviews show palliative care improves outcomes in patients with heart failure (HF), but prior meta-analyses were not HF-specific, or explored how intervention and patient characteristics influence effectiveness, whilst new randomized controlled trials(RCTs) have been published.
Methods
We conducted a systematic review and meta-analysis of RCTs exploring PC in HF. PubMed, EMBASE, CENTRAL and CINAHL were searched until January 24th 2025(PROSPERO ID:CRD42024607104). The primary outcome was hospitalisations. Secondary outcomes included change in quality of life(QoL), assessed by Kansas-City-Cardiomyopathy Questionnaire (KCCQ) and Functional Assessment of Chronic Illness Therapy-Palliative Care(FACIT-Pal) and mental health, assessed by Hospital-Anxiety-Depression-Scale(HADS). Subgroup analyses were conducted based on intervention characteristics (mode and duration), and patient characteristics (gender distribution and HF symptom severity, measured by NYHA class).
Results
Twenty-one RCTs were identified; thirteen were included in meta-analyses(n = 1919). PC was associated with reduced hospitalisation [log OR -0.6 (95% CI -1.14, −0.07); I2 = 69%], and improvement in QoL [mean difference(MD) in KCCQ: 3.09 [95% CI 1.43, 4.75], I2 = 35%] and depression [MD HADS-D: −0.44 (95% CI -0.75 to −0.13)]. No clear differences were observed between intervention modes. Longer interventions (>12 weeks) and interventions targeting patients with advanced HF symptoms (NYHA III/IV ≥70%) were associated with greater improvement in KCCQ and reduction in hospitalisation respectively. No differences in outcomes were observed by gender distribution.
Conclusions
Palliative care reduces hospitalisations, improves QoL and mental health in HF. Longer interventions and those targeting patients with advanced symptoms were linked to differences in outcomes, whereas mode of intervention and gender did not appear to impact outcomes.
Introduction
The treatment of heart failure (HF) has advanced greatly over recent years. 1 However, HF is still a progressive illness with poor prognosis.2,3 Patients with advanced HF are often highly symptomatic4–6 with breathlessness, pain and poor mental health, the prevalence of which may be even greater than in patients with malignancy. 7
Palliative care is a specialty which is focussed on optimizing quality of life (QoL) and reducing suffering of patients and families affected by serious illnesses. 8 Palliative care may include but is not limited to, pain and symptom management; assistance with treatment decision-making; psychological, spiritual and social support and complex care coordination. 9 Multiple systematic reviews and meta analyses of randomised controlled trials have highlighted the role of palliative care in HF management10–14: improving symptoms and QoL as well as reducing hospital re-admissions. This has led to the recommendation within guidelines of early palliative care integration in the management of HF.15,16
However, existing systematic reviews10,13,14,17 included studies recruiting patients with a range of advanced non-cardiac 18 as well as cardiac conditions, 19 which limits the applicability of results to HF patients specifically. There have also been several newly published RCTs studying the efficacy of palliative care interventions in HF populations eg, Bekelman et al., 20 Balata et al., 21 and Piamjarikul et al., 22 which have not been included in previous systematic reviews and meta-analyses. Moreover, previous systematic reviews did not explore how intervention or patient characteristics may influence clinical outcomes.
These gaps highlight the need for an updated and targeted systematic review and meta-analysis into palliative care interventions in HF. In this systematic review, we aim to provide an updated assessment of the impact of palliative care interventions on hospitalisations, QoL and mental health in patients with HF and to explore the impact of intervention and patient characteristics on effectiveness of palliative care in this population.
Methods
This systematic review was conducted by adhering to the rigorous criteria defined in the Cochrane Handbook for Systematic Reviews of Interventions 23 and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 statement. 24 The protocol was registered with PROSPERO under the ID: CRD42024607104.
Search Strategy
A systematic search was conducted from inception to January 24th 2025, using the following databases: PubMed via Medline, EMBASE, CENTRAL and CINAHL. The full details of the search strategy and MeSH terms are included as Supplemental material 1. Reference lists of other systematic reviews and randomised controlled trials were also screened.
Eligibility Criteria
We included randomised controlled trials which compared the efficacy of palliative care interventions vs usual care in adults ≥18 years old with HF. We included studies that exclusively enrolled patients with HF, or studies with mixed populations where results were reported separately for the HF subgroup. Palliative care interventions were defined as specific interventions delivered by any members of the multi-disciplinary team with training in palliative care, aiming to improve QoL for individuals with HF by addressing their physical, psychological, social and spiritual needs. Only trials that reported the primary and/or secondary outcomes of interest were included in the review. For a detailed description of outcomes, please refer to the section on primary and secondary outcomes below. We excluded all non-randomized studies such as retrospective and prospective cohort studies, as well as case-control studies. Editorials, systematic reviews and conference abstracts were also excluded, as were articles not written in English.
Study Selection
Following deduplication by title/abstract, six independent reviewers (RC, AA, HM, SS, EB, RA) screened studies in pairs, with each article assessed by at least two reviewers. Any conflicts were resolved by discussion with a third (independent) reviewer.
Data Extraction
Data were extracted from selected studies by two independent reviewers (RC and AA). Data including study characteristics (author, year, country), patient characteristics (sample size, demographic data, HF severity), type of palliative care intervention (mode and length of intervention, length of follow up) and reported outcome measures (hospitalisation rates, changes in QoL and mental health) were collected.
Primary Outcome
The primary outcome was the proportion of patients with at least one hospital admission for any cause, compared between the palliative care and usual care cohorts and expressed as a log odds ratio. This was selected as a primary outcome due to its clinical objectivity and reduced susceptibility to performance bias compared with patient-reported outcomes, which may be influenced in unblinded trials by differences in follow-up intensity and clinician contact. 25
Secondary Outcomes
Key secondary outcomes included change in QoL, reported as the unadjusted mean difference in change from baseline scores of validated tools such as Kansas City Cardiomyopathy Questionnaire(KCCQ), the Functional Assessment of Chronic Illness Therapy-Palliative Care (FACIT-Pal) Scale, 26 the Minnesota Living with Heart Failure Questionnaire, 27 or the Edmonton Symptom Assessment Scale 28 ; and change in mental health scores, reported as the unadjusted mean difference in change from baseline scores of validated tools such as the Hospital Anxiety and Depression Scale, 29 the Personal Health Questionnaire 9-item score 30 or Generalised Anxiety Disorder-7-item questionnaire. 31 Unadjusted mean differences were used to ensure comparability across studies, as adjustment methods varied or were not clearly reported. Studies that reported final scores without baseline scores were also not included in the meta-analysis to ensure a consistent measure of the treatment effect.
Risk of Bias Assessment
The risk of bias assessment was conducted independently by two reviewers, using the Cochrane risk of bias 2 tool. 32 Any conflicts were resolved by discussion with a third reviewer who was not involved in the initial assessment. The risk of bias plots were generated using the robvis tool. 33
Data Synthesis
Meta-analyses were performed for each outcome of interest using the random-effects model. A random effects model was used as clinical and methodological heterogeneity was anticipated due to variability in populations and interventions within studies. For hospitalisation, the pooled effect size was presented as log-odds ratios of the number of patients with at-least one hospitalisation with 95% confidence intervals (CIs). For changes in QoL and mental health, we calculated the mean difference of each score with 95% CIs.
Where sufficient data were available, subgroup meta-analyses were planned to explore differences in clinical outcomes such as hospitalisations and QoL, according to intervention and patient characteristics. Intervention characteristics planned for subgroup analysis included mode of delivery (in-person vs virtual), length of delivery (≤12 weeks vs >12 weeks). Key patient characteristics planned for analyses included age, gender distribution (proportion male ≤70% vs >70%) and HF symptom severity (proportion New York Heart Association (NYHA) class III/IV ≤70% vs >70%). All subgroup analyses were considered exploratory.
Statistical heterogeneity was assessed using the I2 statistic. Meta-regression could not be performed due to the small number of studies within the meta-analysis. Publication bias was evaluated using funnel plots and statistically with Egger’s test if at least 10 studies were included in a meta-analysis. All analyses were performed using Stata18 (StataCorp, College Station, TX).
Results
Literature Search
After removing duplicate articles (n = 482) and following title and abstract review, a total of 112 records were identified for full-text review (Figure 1). Of these records, 91 were excluded for the reasons listed in Figure 1. The remaining 21 studies were included in the systematic review,20–22,34–51 involving 2851 HF participants. Thirteen studies, encompassing a total of 1919 patients, were included in the meta-analyses. PRISMA Flowchart of the study selection process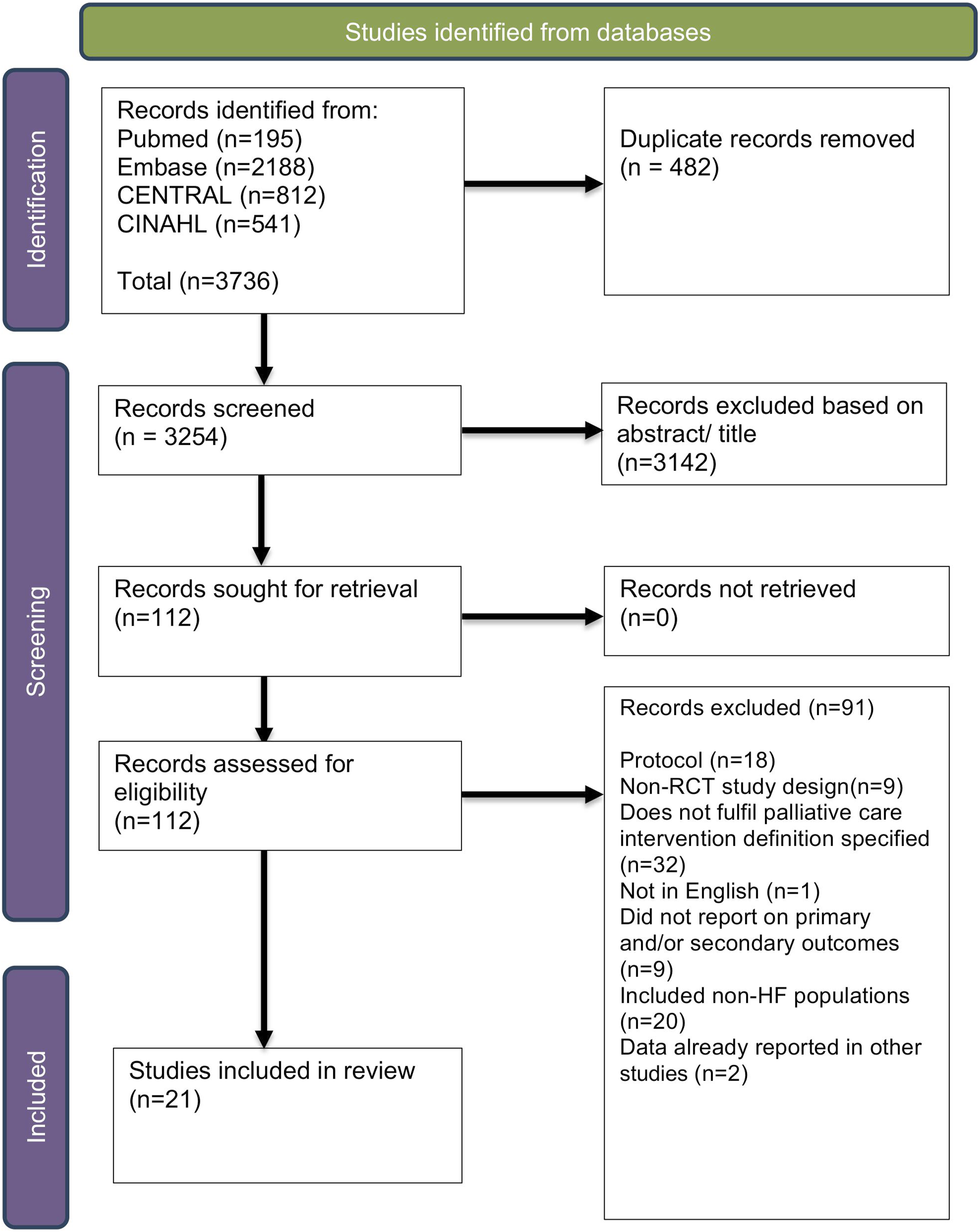
Characteristics of Included Studies
Summary of study characteristics
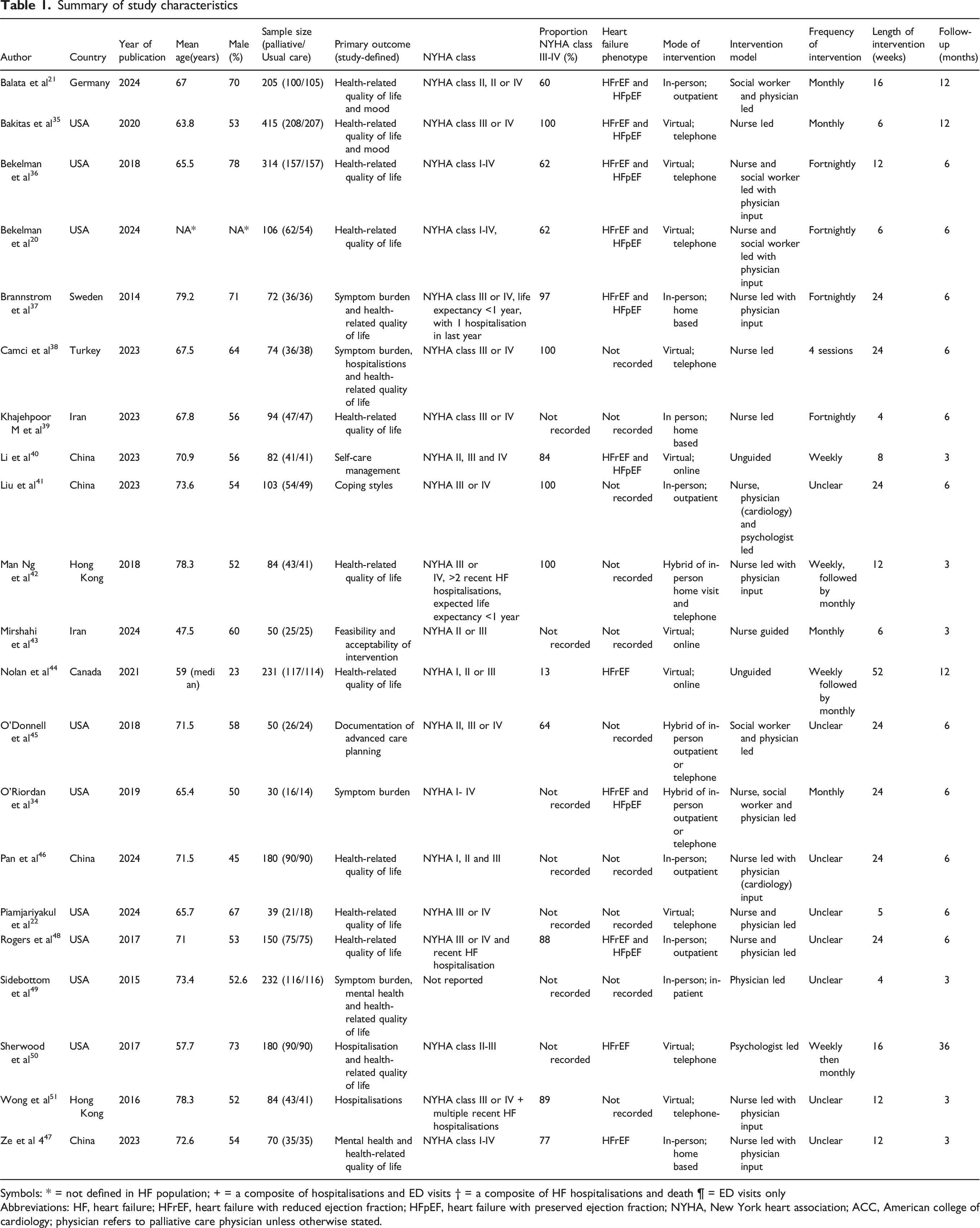
Symbols: * = not defined in HF population; + = a composite of hospitalisations and ED visits † = a composite of HF hospitalisations and death ¶ = ED visits only
Abbreviations: HF, heart failure; HFrEF, heart failure with reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; NYHA, New York heart association; ACC, American college of cardiology; physician refers to palliative care physician unless otherwise stated.
Details of Palliative Care Interventions
All studies examined palliative care interventions vs usual care in patients with HF. Palliative care interventions were typically multicomponent and incorporated a combination of symptom assessment and management, psychosocial support, advance care planning and coordination of care. Interventions were most commonly delivered by specialist palliative care nurses, either independently, or alongside physicians or a multidisciplinary team, including psychologists and social workers (Table 1). Some interventions were led by psychologists and social workers, either independently or with physician input. Two interventions did not involve a healthcare professional and patients worked through palliative care themed educational modules independently. Interventions typically involved structured follow-up with regular scheduled contacts, although the frequency and duration of intervention varied considerably and were not consistently reported across studies. Ten studies evaluated virtual interventions, either via telephone consultations20,22,35,36,38,50,51 (n = 7) or online platforms40,43,44 (n = 3). Eight studies evaluated in-person interventions, including outpatient clinic-based21,41,46,48 (n = 4), home-based37,39,47 (n = 3) or in-patient based 49 (n = 1). There were 3 additional hybrid interventions,34,42,45 delivered via a combination of in-person and virtual strategies.
Usual care was predominantly defined as the usual follow up the patient would have received in their respective healthcare systems, other than in Nolan et al 44 and Sherwood et al 50 which used an educational HF program as control.
Regarding outcome measures, ten studies reported on hospitalisation data,21,35–38,44,48–51 all twenty-one studies reported on changes in QoL and eleven studies reported on changes in mental health.20–22,35–37,41,47–50 A summary of outcomes of each study is reported within supplemental Table 1.
Effect on Hospitalisations
Six studies (n = 899) reported the effect of palliative care interventions compared to usual care on the proportion of patients with at least one hospitalisation during follow up period. A random effects meta-analysis of these studies showed that palliative care intervention was associated with a significant reduction in hospitalisations compared to usual care in HF patients (overall log odds ratio −0.6; 95% CI = −1.14, −0.07) (Figure 2). Substantial heterogeneity was observed (I2 = 69%). Forest plot illustrating the effect of palliative care interventions compared to usual care on the proportion of patients with at least one hospitalisation for any cause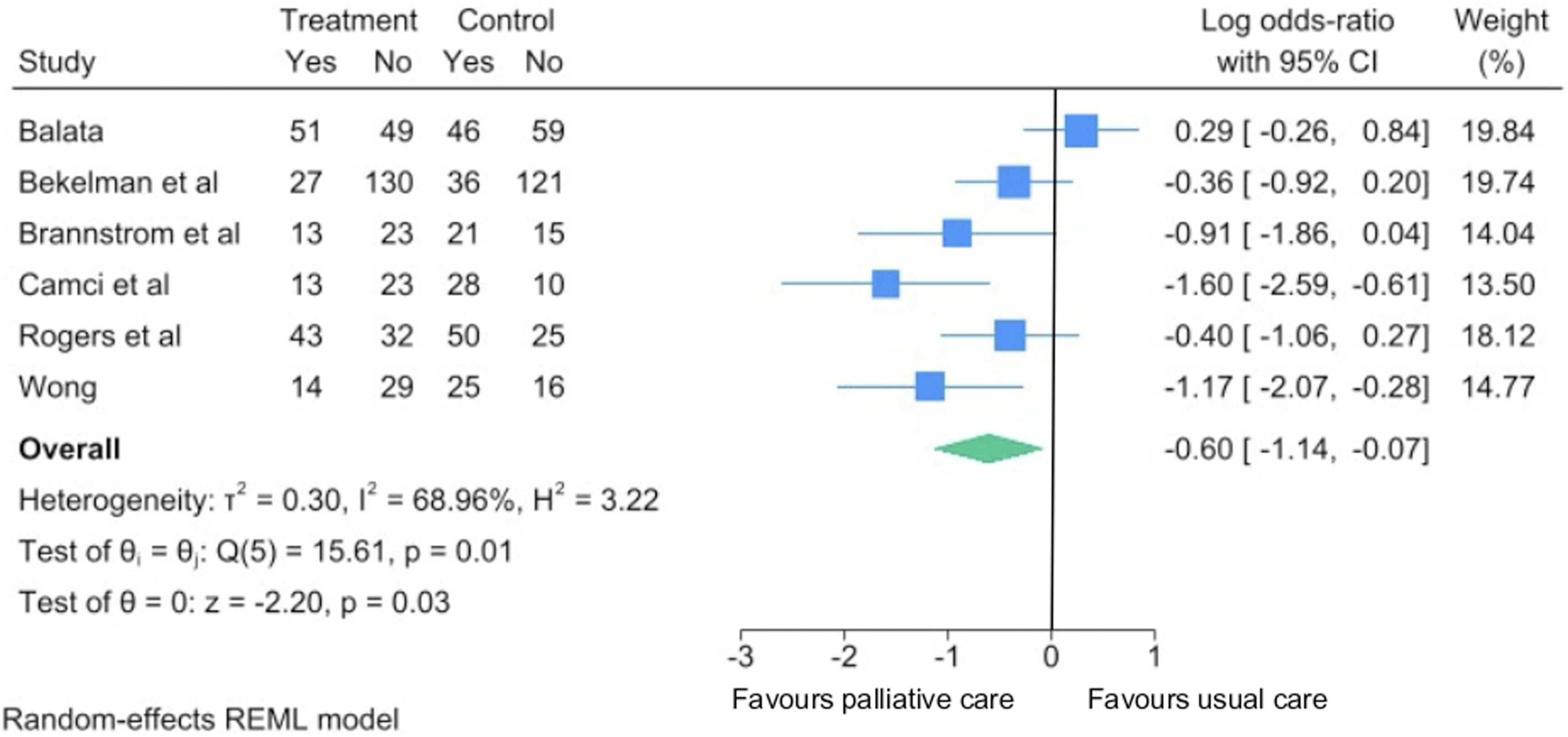
Subgroup analyses comparing intervention and patient characteristics were conducted to explore potential sources of heterogeneity. There was no significant difference in hospitalisations comparing virtual care interventions vs in person interventions [−0.96 (95% CI −1.71, −0.2) vs −0.26 (95% CI −0.93, 0.41), P = .18] (Supplemental Figure 1) and comparing interventions >12 weeks vs ≤12 weeks [−0.58 (95% CI −1.36, 0.21) vs -0.69 (95% CI −1.47, 0.10), P = .84] (Supplemental Figure 2). There was no significant difference in hospitalisations in studies where the proportion of male patients were <70% vs ≥70% [−0.98 (95% CI −1.71, −0.26] vs −0.25 (95% CI −0.88, 0.39), P = .13] (Supplemental Figure 3). Palliative care interventions were associated with a significantly greater reduction in hospitalisations in studies where the proportion of patients in NYHA class III/IV were ≥70% vs <70% [−0.94 (95% CI −1.48, −0.41) vs −0.03 (95% CI −0.67, 0.60), P = .03] (Figure 3). Forest plots illustrating the effect of palliative care interventions compared to usual care on the proportion of patients with at least one hospitalisation, stratified by proportion of patients with advanced heart failure symptoms (proportion New York Heart Association class III/IV >= 70% vs <70%)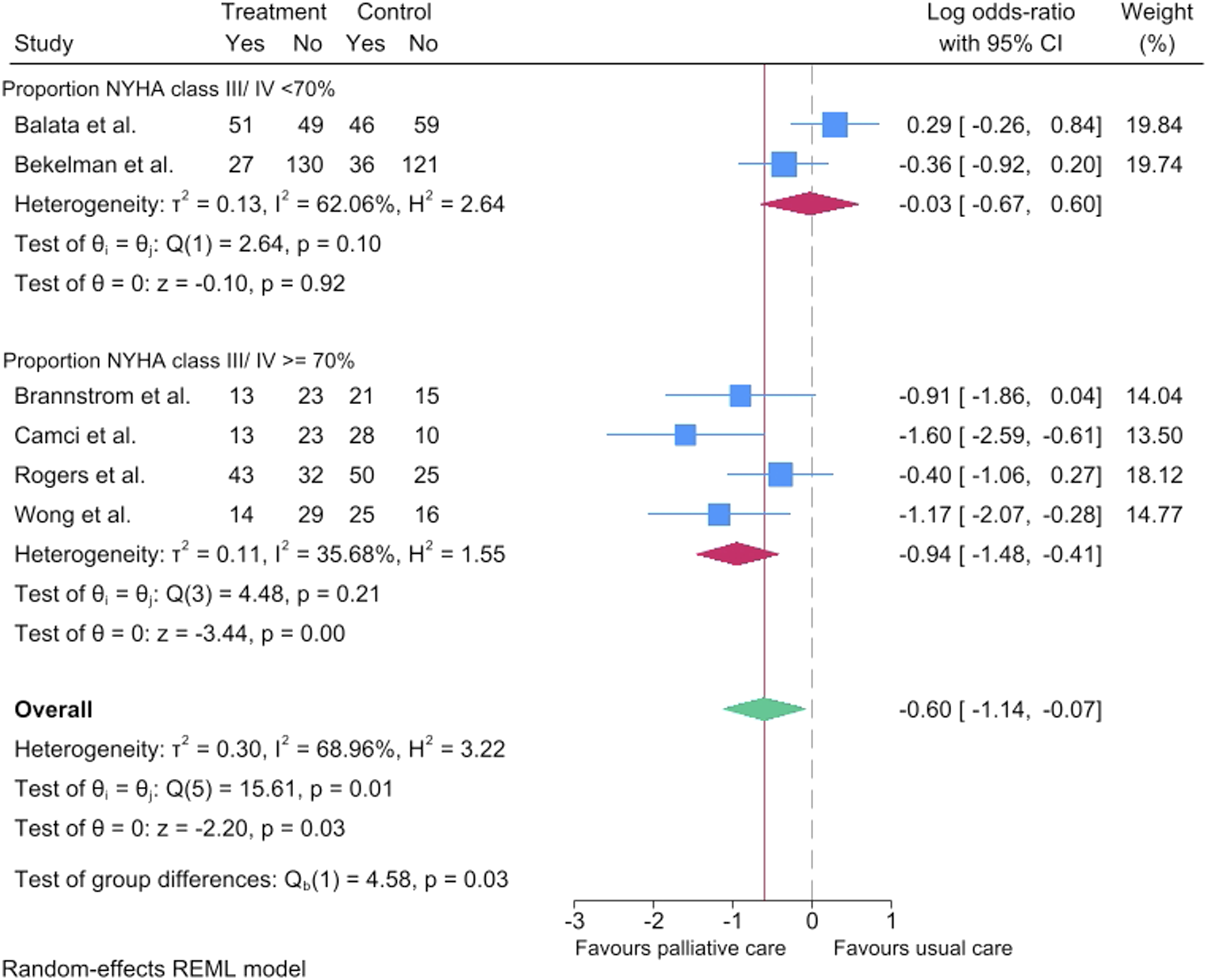
Effect on QoL
All studies reported the effect of palliative care interventions compared to usual care on changes in QoL.
KCCQ
Ten studies (n = 1689) assessed changes in QoL via mean change from baseline in KCCQ. A random effects meta-analysis of these studies showed that palliative care intervention was associated with a small but significant improvement in KCCQ scores compared to usual care in HF patients (mean difference 3.09; 95% CI 1.43, 4.75) (Figure 4). There was moderate heterogeneity observed (I2 = 35%). Forest plot illustrating the effect of palliative care interventions compared to usual care on change in health-related quality of life, as assessed by Kansas City Cardiomyopathy Questionnaire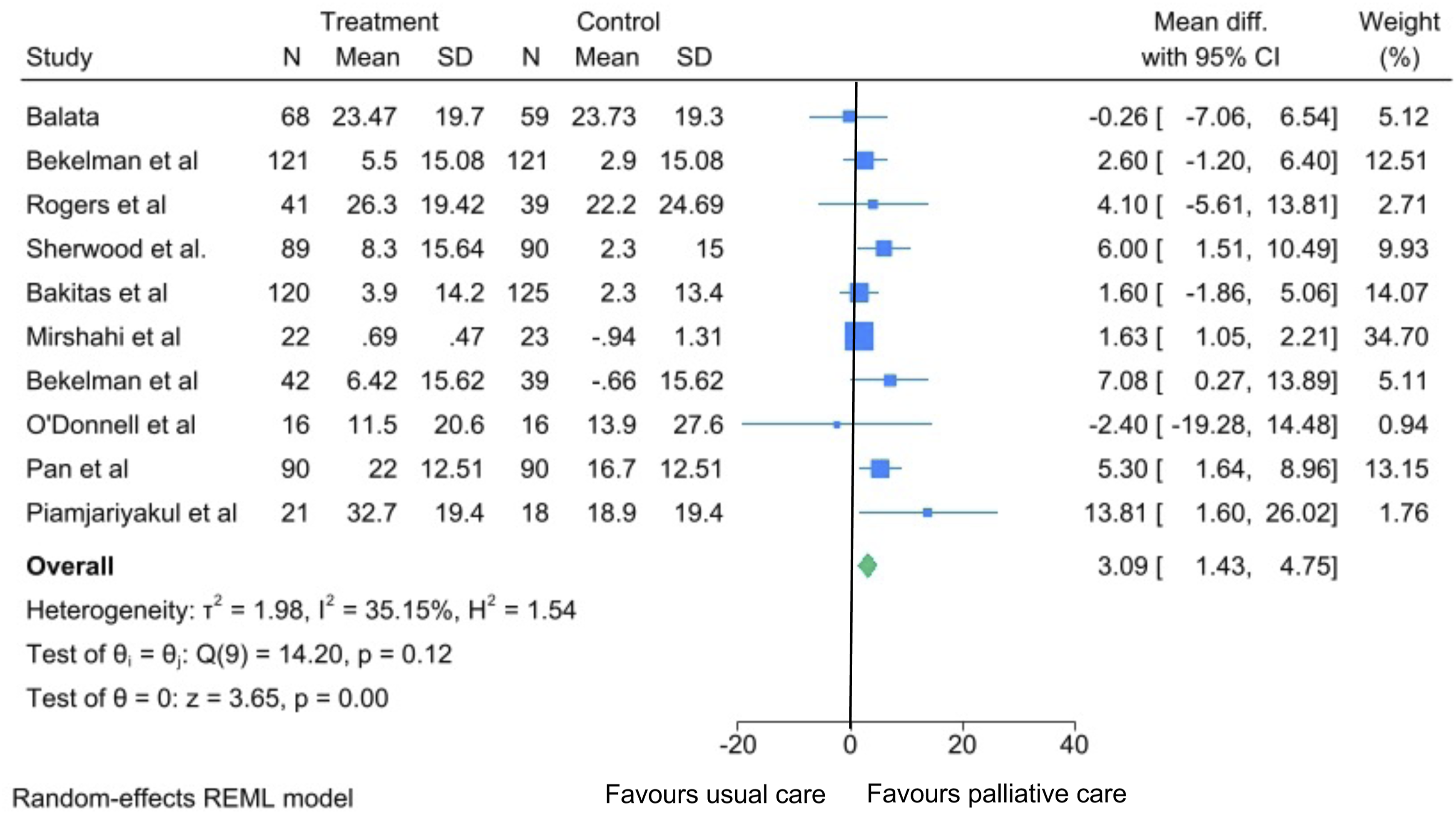
Subgroup analysis found that interventions >12 weeks were associated with a greater improvement in KCCQ scores compared to those Forest plots illustrating the effect of palliative care interventions compared to usual care on change in health-related quality of life, as assessed by Kansas City Cardiomyopathy Questionnaire, stratified by intervention duration (>12 weeks versus </= 12 weeks)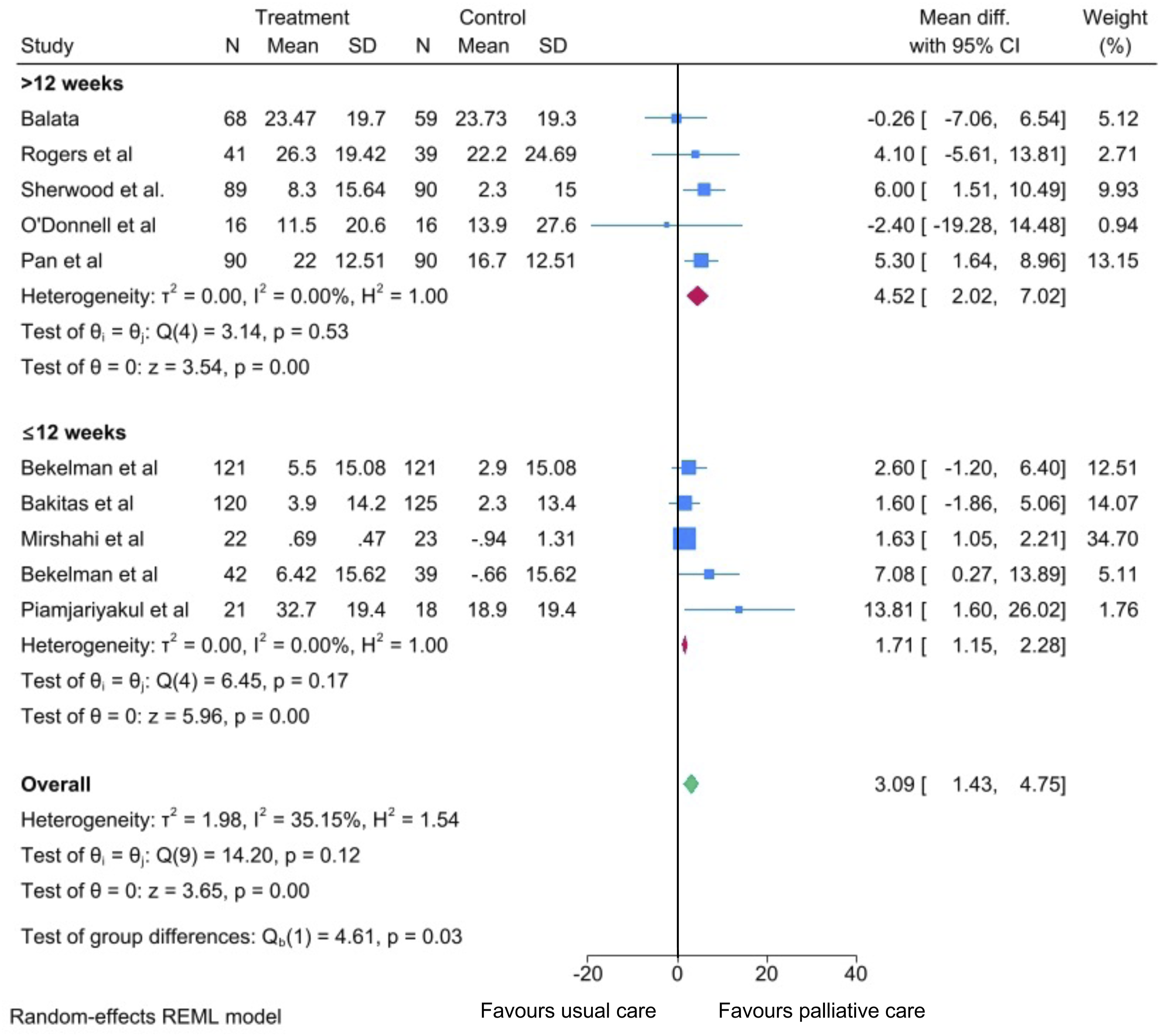
FACIT-Pal
Five studies (n = 462) assessed changes in QoL via mean change in FACITPal. One study was excluded as they did not report baseline scores. A random effects meta-analysis of four studies which assessed mean change from baseline scores (n = 432) showed that palliative care interventions was associated with a small but significant improvement in FACITPAL score [mean difference 2.52 (95% CI 0.56, 4.49]. There was moderate heterogeneity observed (I2 = 36%) (Supplemental Figure 6).
Effect on Mental Health
Thirteen studies (n = 1920) reported the effect of palliative care interventions compared to usual care on changes in mental health.21,22,34–36,40,41,43,45,47–50 Five studies (n = 870) assessed changes in mental health using HADS21,34,35,47,48; four studies (n = 496) used GAD-736,40,43,45; four studies (n = 678) used PHQ-936,40,43,49; two studies (n = 283) used beck inventory scores41,50; one study(n = 50) used PHQ-8 45 and one study (n = 39) used PHQ-4. 22
A random effects meta-analysis of 3 studies which reported mean change from baseline in HADS scores was performed. 2 studies were not included in the meta-analysis: Balata et al 21 only reported the adjusted mean difference in HADS scores and O’Riordan et al 34 did not report baseline HADS scores. The meta-analysis showed that palliative care intervention was associated with a trend towards reduced anxiety assessed using HADS anxiety score, compared to usual care, although it did not reach statistical significance [mean difference −0.31 (95% CI -0.76, 0.13) (Supplemental Figure 7).
A random effects meta-analysis of 3 studies showed that palliative care intervention was associated with a significant improvement in HADS depression score, compared to usual care [mean difference −0.44 (95% CI -0.75, −0.13)] (Supplemental Figure 7). A meta-analysis was not conducted for GAD-7 or PHQ-9 as there were not enough eligible studies which reported baseline and final scores.
Quality Assessment
The overall bias assessment across included studies primarily suggested a high risk of bias. Bias was frequently observed in domains 3 (bias induced by missing outcome) and 4 (bias in outcome measure). Nine out of 21 studies had high risk for bias in domain 4,20,22,34,39–42,45,46 as it was impossible to blind participants to the intervention and hence, any self-reported QoL or mental health assessment may be affected by knowledge of their treatment allocation. Figure 6 illustrates a detailed risk of bias assessment. Risk of bias assessment in randomised controlled trials using Rob 2.0 tool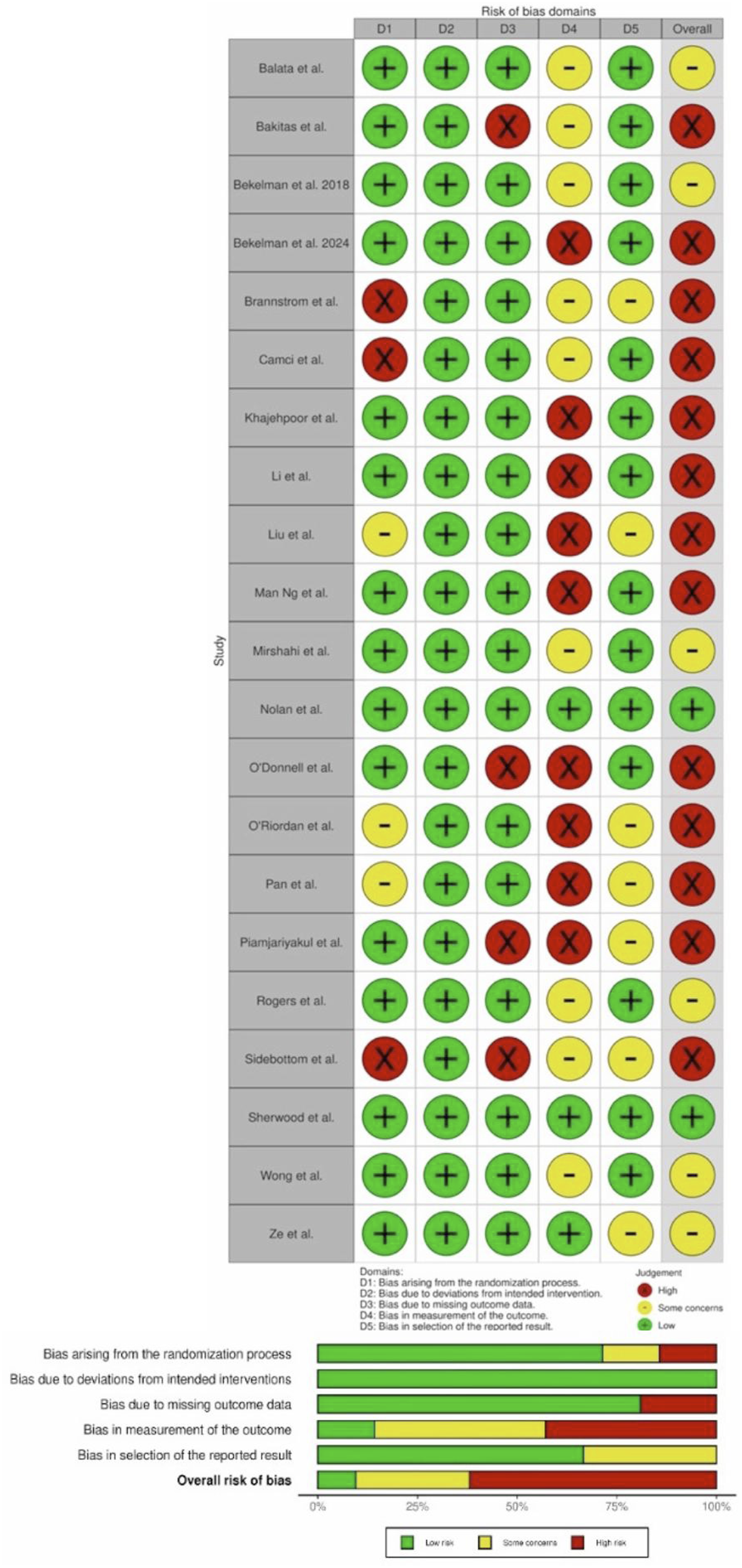
Publication Bias
Publication bias was assessed for KCCQ meta-analysis. The generated funnel plot appeared asymmetrical, and egger’s test indicated significant asymmetry (intercept = 0.89, standard error = 0.39, z = 2.3 P = .022), suggesting publication bias or small-study effect (supplemental Figure 8).
The trim and fill analysis imputed 14 potentially missing studies, increasing the total to 24. However, the adjusted mean pooled difference remained identical at 1.85, suggesting that publication bias would not have affected the overall effect size.
Discussion
In this systematic review, we examined the impact of palliative care interventions on hospitalisations, QoL and mental health in patients with HF. To the best of our knowledge, this is the first systematic review to also explore potential differences in the effect of palliative care interventions in patients with HF according to intervention and patient characteristics.
Overall, palliative care interventions were associated with a significant reduction in all-cause hospitalisations and improvements in QoL. There was also a significant reduction in depression scores, and a non-significant decrease in anxiety scores. However, populations studied and hospitalisation outcomes are heterogenous with varying definitions across trials, therefore, our findings should be interpreted with caution.
Subgroup analyses suggested that interventions lasting more than 12 weeks were associated with greater improvements in QoL than shorter interventions, although intervention duration did not result in significant differences in hospitalisation. Mode of intervention delivery, whether in-person, virtual or hybrid, appeared to have little effect on hospitalisation or QoL. Studies including a greater proportion of patients with advanced HF symptoms (≥70% NYHA class III/IV) showed greater reduction in hospitalisations that those with lower proportion of such patients. Gender distribution did not appear to influence the effect of palliative care interventions on hospitalisation or QoL. Subgroup analyses were based on relatively few studies in each individual subgroup and did not use individual patient data. These analyses should therefore be considered exploratory and hypothesis generating.
Our results are broadly consistent with results from previous systematic reviews of palliative care in HF. However, earlier reviews may have been limited by the inclusion of heterogenous patient populations, reducing the applicability of the results to patients with HF specifically. Several reviews10,13,14 included data from Denvir et al, 52 which examined palliative care interventions in patients with “various advanced cardiovascular diseases”. While 68% of the study’s cohort had HF, 22% had acute coronary syndrome, and 10% had aortic stenosis. Furthermore, another meta-analysis 17 included data from Brumley et al, 18 which examined palliative care interventions in patients with a range of cardiac and non-cardiac conditions, with only 33% of patients in their cohort having HF.
Previous reviews may also have been limited by inconsistencies in outcome definition in previous systematic reviews. Sebestian et al 10 examined telehealth palliative care interventions in HF and included data from Bakitas et al 35 within their meta-analysis for hospitalisations. Unlike the other studies within their meta-analysis that report hospitalisations as the “number of patients with at least one hospitalisation”, Bakitas et al 35 measured hospitalisations by the number of days in hospital, the results of which contributed to 23.1% of the weight of the meta-analysis for hospitalisation data. Combining different outcome measures in a meta-analysis without further sensitivity analysis introduces significant heterogeneity and leads to misleading conclusions. These limitations in the existing literature along with publication of more recent RCTs, highlighted the need for an updated and targeted systematic review and meta-analysis into palliative care interventions in HF.
Strengths
A key strength of this review is the use of stricter inclusion criteria and more standardised outcome measures than in previous reviews, improving the relevance of the findings to HF populations. We have conducted a comprehensive assessment of palliative care interventions across clinically meaningful outcomes including recurrent hospitalisations, QoL and mental health. We also explored whether intervention and patient characteristics were associated with differences in effectiveness of palliative care interventions, identifying potential factors to optimise palliative care delivery in HF patients.
Limitations
There are several limitations to our review. Firstly, there was substantial heterogeneity in the meta-analysis of hospitalisations (I2 = 68%), and hence our results should be interpreted with caution. Subgroup analyses indicated that intervention mode and length did not explain this heterogeneity; however, baseline symptom burden or disease severity may partly account for difference in hospitalisation outcomes.
Secondly, only a small number of studies were included in meta-analyses of mental health outcomes, limiting the certainty and generalisability of these findings.
Third, analysis of funnel plot suggested there may be publication bias within the meta-analysis of KCCQ scores. However, further trim-and-fill analysis suggests this potential publication bias may not have affected the overall effect size.
Fourth, data regarding the cause of hospitalisation (eg, heart failure-related vs non-cardiac admissions) were inconsistently reported across included studies, limiting more granular analysis of intervention effects.
Finally, many studies within the meta-analysis were deemed to be at high risk of bias, mainly due to the reliance on patient-reported outcome measures for key outcomes, increased follow up and clinician contact within intervention groups and the fact that patients and personnel could not be blinded. 25 . These factors may introduce performance and detection bias, potentially affecting subjective outcome reporting. 25 Two studies were able to account for this by including a sham control group, using HF education44,50. Future studies should consider similar designs where feasible to reduce bias related to knowledge of treatment allocation.
Clinical and Research Implications
Our findings support current guideline recommendations for the use of palliative care in patients with HF,15,16 as these interventions were associated with reductions in hospitalisations and modest improvements in QoL and mental health. Exploratory subgroup analyses suggested that patients with more advanced HF symptoms may derive greater benefit from palliative care interventions in terms of reduced hospitalisations and longer interventions may be associated with greater improvement in QoL. However, these findings are hypothesis-generating, and should not be interpreted as evidence of causality, particularly given the limited number of studies contributing to each subgroup and the absence of individual patient data.
We did not find any association between outcomes of virtual care interventions and in-person interventions; however, this should ideally be examined within a comparison study. Virtual palliative care may provide a distinct benefit to patients with advanced HF, as they may have difficulty attending outpatient healthcare appointments. 53 Studies have also demonstrated it may be cost and resource saving when compared to in-person care.54,55 However, certain groups of patients, particularly older adults or those with suboptimal digital literacy, may struggle to engage with virtual care. 56
It is important to note that the positive effect of palliative care on outcomes was not consistent across all RCTs: several studies found no impact of palliative care on hospitalisations, QoL or mental health.21,34,35,44,45 This variability may reflect differences in intervention content, duration, timing of delivery within the disease trajectory, the characteristics of study population, and the nature of usual care provided to control groups. Whilst our exploratory subgroup analyses identified some potential factors to explain variability in outcomes, further well-designed studies are needed to determine which patients are most likely to benefit and how palliative care should best be delivered in HF. Ultimately, palliative care interventions should be tailored to the individual. Patients differ in their preferences, values, symptom burden and disease trajectory, and these factors should inform the content, timing, duration and mode of delivery of care. A personalised approach may help maximise the benefit of palliative care and ensure support remains responsive to patients’ changing needs over time.
Conclusion
The findings of this systematic review and meta-analysis suggest that palliative care is effective in reducing hospitalisation, improving QoL and mental health in patients with HF. The mode of intervention, either virtual or in-person does not seem to affect these outcomes. Interventions with a longer duration and those targeting patients with advanced symptoms may lead to greater improvements in QoL and reduction in hospitalisation. Further high-quality studies are needed to confirm these results and examine the optimal delivery of palliative care in HF.
Supplemental Material
Suppplemental Material - Palliative Care in Heart Failure: An Updated Systematic Review and Meta Analysis of Randomised Controlled Trials and Associations With Intervention and Patient Characteristics
Suppplemental Material for Palliative Care in Heart Failure: An Updated Systematic Review and Meta Analysis of Randomised Controlled Trials and Associations With Intervention and Patient Characteristics by Ravi Chotalia, Hasan Mohiaddin, Alisha Aggarwal, Edward Bouchardt, Robert Ambrogetti, Minesh Chotalia, Iain Squire, Shirley Sze in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Suppplemental Material - Palliative Care in Heart Failure: An Updated Systematic Review and Meta Analysis of Randomised Controlled Trials and Associations With Intervention and Patient Characteristics
Suppplemental Material for Palliative Care in Heart Failure: An Updated Systematic Review and Meta Analysis of Randomised Controlled Trials and Associations With Intervention and Patient Characteristics by Ravi Chotalia, Hasan Mohiaddin, Alisha Aggarwal, Edward Bouchardt, Robert Ambrogetti, Minesh Chotalia, Iain Squire, Shirley Sze in American Journal of Hospice and Palliative Medicine®
Footnotes
Ethical Considerations
This research required no specific ethical approval.
Author Contributions
RC was involved in conceptualisation of the review, design of the search strategy, screening of articles, risk of bias assessment, writing the initial manuscript, and reviewing and editing the final manuscript. AA was involved in design of the search strategy, screening of articles, risk of bias assessment and reviewing and editing the final manuscript. RA, EB, HM were involved in screening of articles and reviewing and editing the final manuscript. IS and MC were involved in reviewing and editing the final manuscript. SS was involved in conceptualisation of the review, screening of articles, writing the initial manuscript and reviewing and editing the final manuscript. All authors have reviewed this manuscript and have given consent for this submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Details of search strategy are provided in supplementary materials. The dataset supporting the conclusions of this article is available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.