
Abstract
Background
Palliative care training in neurology residency is commonly limited, despite the fact that neurologists care for patients with complex palliative needs, such as high symptom burden, unique illness trajectories and prognoses (including prognostic uncertainty), and issues of decisional capacity.
Objective
The objective is to expand on neuropalliative curricula for neurology residents to improve delivery of palliative care to patients with neurological illness.
Methods
We developed an educational needs assessment to gather insight into the perceptions of palliative care topics, and confidence in providing palliative care, among adult neurology residents in 2020. The needs assessment guided the construction of a neuropalliative curriculum, including lecture materials and a simulation workshop focusing on provider communication skills, which was implemented in neurology training programs at two major academic medical centers between 2020 and 2024. Pre- and post-intervention surveys of self-reported comfort in different palliative care topics on a five-point Likert scale were analyzed with statistical testing to determine the effectiveness of the neuropalliative simulation curriculum.
Results
15 neurology trainees completed the needs assessment. For all palliative care topics, perceived importance was significantly higher than perceived confidence among trainees. After development and implementation of a novel neuropalliative curriculum, trainees reported improved comfort by an average of 0.6 points in all 6 domains between pre- (n = 58) and post- (n = 41) surveys.
Conclusions
Formal, simulation-based neuropalliative curriculum is effective at improving self-reported comfort in providing primary palliative care among neurology trainees.
Keywords
Introduction
While the importance of palliative care for patients with serious neurological illness is widely recognized, there remains a shortage of palliative and neuropalliative specialists, which is why it is crucial that all neurologists receive quality training in this area.1–3 According to the Accreditation Council for Graduate Medical Education (ACGME) Program Requirements for Graduate Medical Education in Neurology for at least two decades, resident physicians must demonstrate competence in their knowledge of “palliative care, including adequate pain relief as well as psychosocial support and counseling for patients and families. Residents must learn to advocate for patients within the health care system to achieve the patient’s and patient’s family’s care goals, including, when appropriate, end-of-life goals. 4 ” However, multiple studies have identified gaps in neurology training and subsequent unmet needs in adequate delivery of neuropalliative care.5–8
According to a 2009 survey of US neurology residency program directors less than 52% of programs had formal lectures in palliative care topics. 6 A 2017 survey found that 20% of all U.S. adult neurology residency programs had no palliative care education whatsoever. 7 Based on other nationwide surveys, neurology residents tend to demonstrate low knowledge in core palliative care topics. 8 This highlights the need for not only access to expert faculty and dedicated time for teaching, but also the development and standardization of educational content to enhance neuropalliative training.5,7,9,10
Quality education in palliative care is didactic as well as experiential in nature, which represents another challenge in designing training initiatives. 11 Outside of lived clinical experience, educational modalities have been developed to foster experiential palliative care training, particularly simulation-based medical education (SBME). 12 In the world of palliative care, this most often takes the form of simulated patient encounters and has been described in palliative care training since at least 1994. 13 Simulated patient encounters have the benefit of allowing trainees to practice difficult communication skills in a safe space, with the opportunity for debrief, discussion, and feedback that can benefit future practice. There is ample data to support the use of SBME in palliative care to improve provider confidence, communication skills, and even improve patient outcomes.14,15
However, there is room to expand research and implementation of SBME, particularly in the world of neuropalliative care training. Data has been inconsistent on the effectiveness of SBME in non-cancer palliative care overall, owing mainly to the small number of studies in this field. 16 One systematic review of SBME in palliative care found that across 78 different studies, only 1 study focused on learners in neurology. 14 Distress in approaching end-of-life neuropalliative care has been described in both neurology and palliative care trainees, with a significant factor being lack of experience and practice. 17 A recent pilot study of a learning activity that included an interactive simulation session for 26 neurology residents showed that this was a feasible, well-received learning model that was effective at improving comfort with addressing prognosis and navigating goals of care conversations. 18 This study also found that high confidence in palliative skills did not correlate with competency, as evaluated by faculty advisors in observed standardized patient encounters. 18 This is a commonly found tendency and represents a limitation to reliance on self-assessments to evaluate resident learners.19,20 These findings highlight the need for further research in SBME and neuropalliative care to define training gaps and inform the development of relevant curricula.
We developed a needs assessment to gather insight into the educational needs of adult neurology residents at the University of California, Los Angeles (UCLA). The assessment asked about their perceptions of the most important palliative care topics and their confidence in providing such care. The results of this needs assessment were utilized to help guide the development of neuropalliative lecture materials and a simulation workshop focusing on provider communication skills in serious neurological illness, executed at UCLA and Cedars-Sinai Medical Center (CSMC). Change in self-reported comfort in different palliative care topics before and after the simulation was used to assess the effectiveness of the educational intervention. The education modules are included here, for use at other institutions who may wish to increase neuropalliative care training in their residency programs.
Methods
Needs Assessment Development
We developed an anonymous survey addressing 11 general palliative care topics and six neurological diseases that have specific palliative care needs. It was electronically disseminated to UCLA neurology residents in Fall 2020. The topics included in the survey were based on the domains that were consistently found across multiple resources including ACGME guidelines for neurology residency as well as hospice and palliative care fellowships, previous studies on palliative care education in residency, major literature reviews aimed at establishing an evidenced-based consensus of core principles in palliative care for patients with serious and progressive neurological disorders, and input from domain experts on the research team (D.K., C.S.).4,7,8,21-25
The survey used a 5-point Likert scale for each question (not at all, slightly, moderately, very, extremely). Respondents were first asked to rate how important they believed it was to receive education on each palliative care topic. Next, they rated their comfort/confidence in providing palliative care in each area. The third section asked about confidence addressing disease-specific palliative care needs of patients with Parkinson’s Disease, Amyotrophic Lateral Sclerosis (ALS), dementia, stroke, Multiple Sclerosis (MS), and malignant brain tumor(s). Lastly, there was an open-ended feedback section asking about any other palliative care skills that residents would like to be included in their neuropalliative curriculum not mentioned elsewhere in the survey. All questions were optional, and completion was not required to end the survey.
Needs Assessment Analysis
Likert scale responses were converted to a numerical scale (1-5). Quantitative data was then analyzed using two-tailed t-tests for normally distributed data (ethical and legal aspects of care, shared decision-making regarding initiating or withdrawing life-prolonging therapies, empathetic responses, delivering bad news, managing imminent death and end-of-life symptoms, managing hospice patients, prognostication) while the remaining data were analyzed using the Wilcoxon Signed-Rank Test for Paired Samples, which uses medians, given evidence against the null/normality assumption according to Shapiro-Wilk Test. A significance level of P < .0045 was used to account for the multiple comparisons performed (ie, Bonferroni correction). This allowed for identification of statistically significant differences between perceived importance of receiving education in palliative care topics and confidence in providing different types of palliative care. The average scores on each question were then used to rank palliative care topics from first to 11th to examine whether there was concordance or discordance between importance and confidence rankings, with relative discordance demonstrating a “need for improvement.” After looking at the data in aggregate, it was then stratified by post-graduate year. The same approach was taken for the analysis of section three, addressing comfort with providing disease-specific palliative care.
Educational Materials (Lecture & Simulation)
Needs assessment results helped to inform the development of the educational materials, including both the lecture and simulation case content, in addition to the recognized need for more integrated palliative education in neurology residency training as described in the introduction. At UCLA, a 2-hour lecture was given by content expert, C.S., introducing important topics in serious illness communication to residents approximately 1 month prior to simulation. At CSMC, a series of similar lectures mostly focused on communication topics were given by content expert, J.B., throughout the year totaling at least 10 hours. Lecture content related to the palliative simulation was highly similar between the two institutions. The case-based simulation was carried out at both institutions with a 30-minute lecture to review key palliative care concepts and skills discussed in prior session(s) including shared decision making, empathic responses, breaking bad news, prognostication, and utilizing time limited trials. The simulation case was identical at both sites. The intervention was done once per academic year between 2020 to 2024 at UCLA and between 2022-2024 at CSMC.
Analysis of Intervention
A survey asking for the respondent’s level of training and the same six questions was distributed before and after conducting the simulation workshop. Each question used a 5-point Likert scale (not at all, slightly, moderately, very, extremely) and asked respondents to describe how comfortable they felt employing certain palliative care skills. Data was then analyzed using two-tailed Welch’s T-test with significance levels of P < .05.
IRB Statement
The UCLA Institutional Review Board (IRB) exempted this minimal risk study from further review (IRB #23-000807). The Cedars-Sinai IRB exempted this minimal risk study from further review (IRB #00002169). There were no financial incentives offered for completion or participation in this study and participation was voluntary.
Results
Needs Assessment
Full needs assessment results and analysis are published elsewhere.
26
15 residents completed our electronically disseminated needs assessment in October of 2020. 9 (60%) respondents were female. 5 (33%) were first year residents (PGY2), 3 (20%) were second year residents, and 7 (47%) were third year residents. The cohort of residents surveyed believed, on average, it was “very important” or “extremely important” to receive education in all palliative care topics included. They also felt, on average, “slightly comfortable” or “moderately comfortable” providing all aspects of palliative care. For each palliative care topic, residents rated the importance of palliative care topics significantly higher than their comfort/confidence level (P < .0045). Figure 1 and Table 1 highlight some of the most important findings. Three out of four communication skills (bad news, empathic responses, communicating uncertain prognoses) were generally perceived to be among the most important topics, and areas in which respondents reported a high degree of confidence. One exception to this was the communication skill of shared decision-making, which was tied with prognostication for most important, but was an area that residents felt relatively uncomfortable practicing. On the other hand, non-pain symptom assessment and management was least important (11th), but it ranked as the area of 5th most confidence (delta 6). Hospice patient management was rated of intermediate importance (7th) and an area of intermediate confidence (7th). Psychological, existential, and religious/spiritual distress was identified as the area of 9th most important and 9th most confidence, while imminent death management was relatively unimportant (10th) and the area of least confidence (11th). Relative Perceived Importance of Palliative Care Topic Evaluation Vs. Confidence in Providing Different Aspects of Palliative Care Overall Ratings of Residents’ Comfort in Addressing Disease-Specific Palliative Care Needs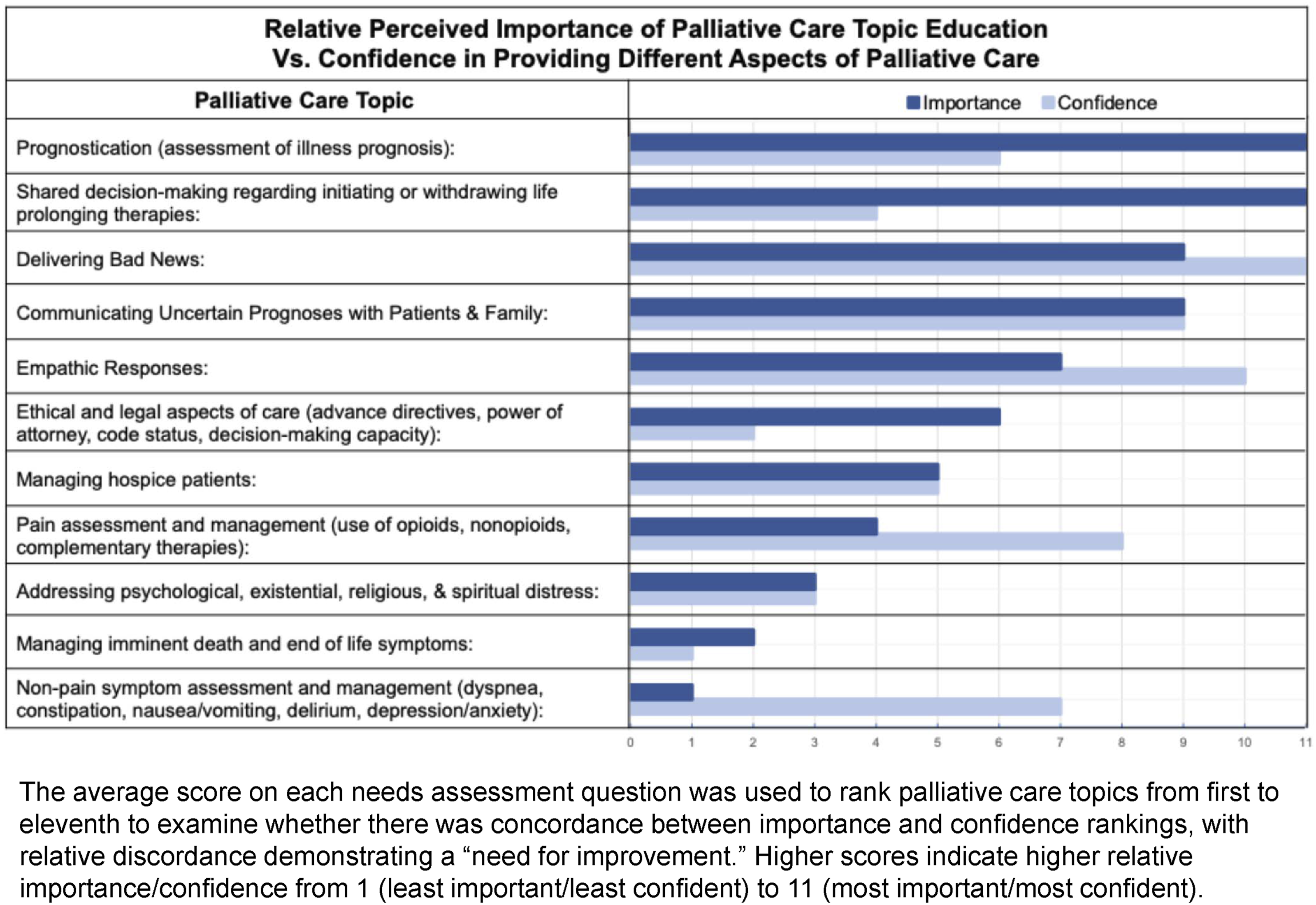
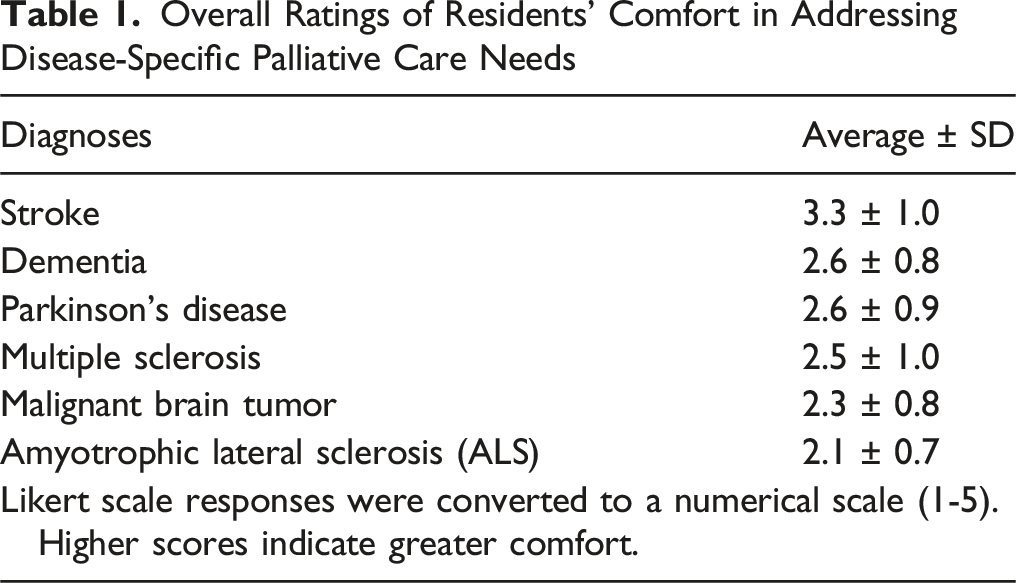
Overall, and when stratifying by training levels, residents felt most confident in dealing with stroke (Table 1). Residents overall, and across all training levels, felt least confident in addressing malignant brain tumors and ALS (stratified data not shown). The following are free-text responses for other areas of perceived need or interest to be emphasized in the neuropalliative curriculum that were not in the survey: “moral injury & processing our own reflections/feelings,” (n = 1) “outlining goals with families,” (n = 1) and “using appropriate/easy to understand patient-level terminology for specific diagnoses/symptoms” (n = 1).
Educational Materials
Supplemental show(s) the lecture material from each site and the simulation case information. In creating these educational materials and activities, we addressed the five topics rated as highest importance to residents with some expert discretion (C.S. and J.B.).
Analysis of Intervention
In total, there were 58 responses to the pre-simulation survey (“pre-survey”) and 41 responses on post-simulation survey (“post-survey”). There were 39 PGY2s, 14 PGY3s, 4 PGY4s, and 1 PGY6 that completed the pre-survey while 29 PGY2, 8 PGY3, 3 PGY4, and 1 PGY6 completed the post-survey. 39 pre-survey respondents and 22 post-survey respondents were from UCLA. 19 pre- and post-survey respondents were from Cedars Sinai Medical Center (CSMC).
Figure 2 summarizes the average numerical response for each survey question and results of statistical testing. The average comfort across all questions significantly increased after the intervention (P = .0018). The average score on pre-survey questions was 3.2 corresponding most closely to “moderately comfortable.” The average score on post-survey questions was 3.9 corresponding most closely to “very comfortable.” All 6 questions had statistically significant increases. Change in Comfort with Palliative Care Topics Before & After Simulation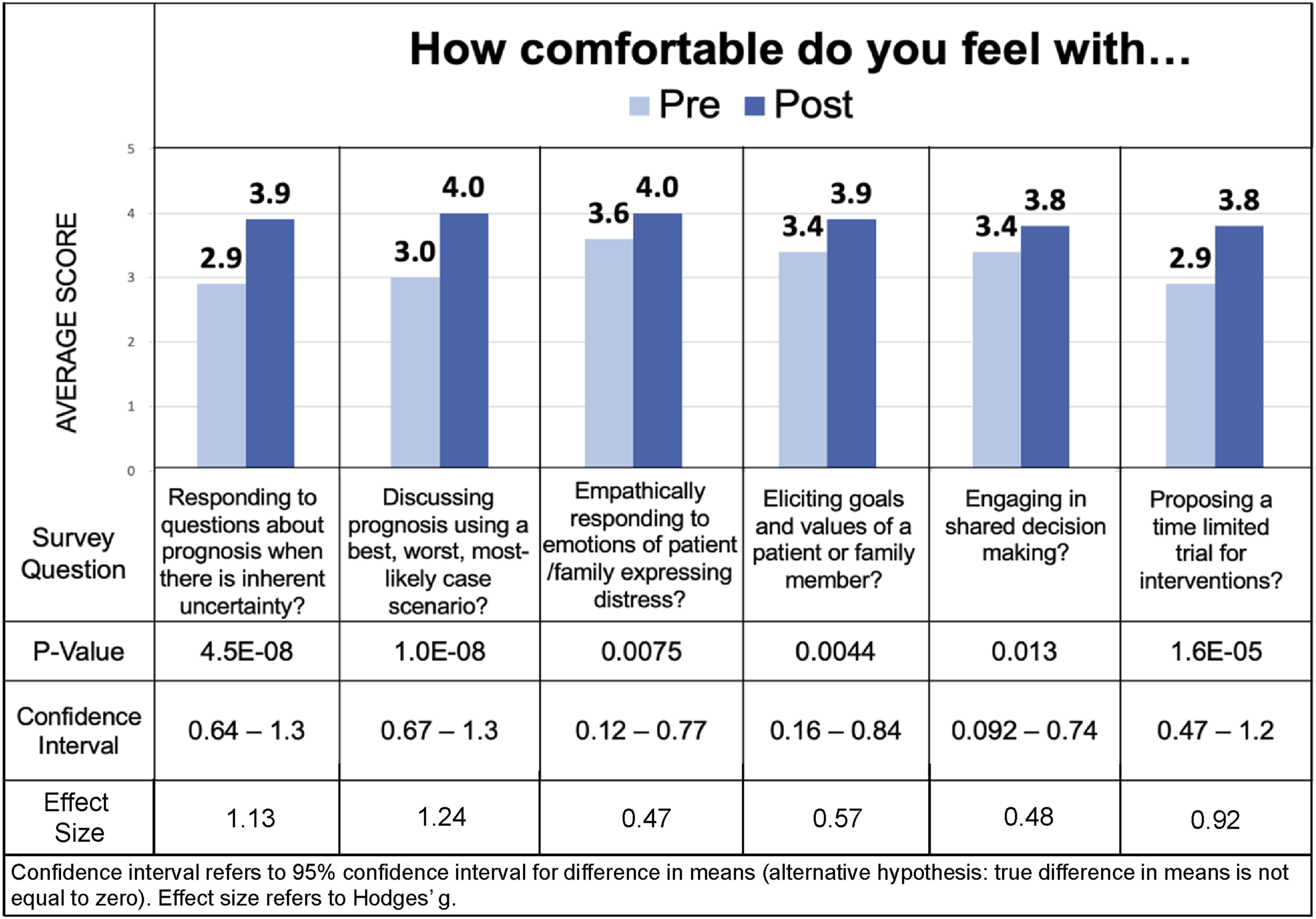
Discussion
Overall, our study aimed to not only highlight potential gaps in palliative care education among neurology residents but also begin to develop and receive feedback on a more structured neuropalliative curriculum. One recent pilot study 18 established the feasibility and efficacy of a simulation-based session for neurology learners using a neuro-specific patient case, however, the authors focused on only a few broad aspects of serious illness communication (conducting goals of care discussions, sharing prognosis, and recommending hospice) identified by the authors as important. We sought to identify and teach communication skills that our neurology residents expressed in their needs-assessment to be highest yield and most challenging, including prognostication, prognostic uncertainty, and shared decision-making.
Communication skills and prognostication were considered among the most important topics on the needs assessment. However, assessing illness prognosis and specifically engaging in shared-decision making were areas of low confidence, demonstrating a need to improve education. These are highly relevant to a neurologist’s day-to-day work as they are commonly asked to discuss goals of care with patients or loved ones, especially in the inpatient setting after an acute neurological injury. Psychological, existential, and religious/spiritual distress and hospice management were areas of relatively low perceived importance and confidence, which may indicate that residents feel these palliative care needs are better addressed by ancillary services such as psychiatry, chaplain/spiritual services, or primary palliative/hospice specialists. Overall, our findings that communication and prognostication were considered most important while psychological/spiritual distress were least important are consistent with previous research from 2017 investigating residency training in neuropalliative care. 7 Analysis of aggregate and stratified data by training level did not demonstrate striking differences in relative importance and confidence rankings, which underscores the need for a more structured neuropalliative curriculum that builds on itself as residents progress through training. Our results also suggest there is adequate or strongest training in stroke management amongst all levels of residents while there is a need to improve training in malignant brain tumor and ALS. This is likely because stroke and dementia are two of the most commonly encountered neurological disorders.27,28
Our lecture material and case simulation focused on formulating and disclosing prognosis, shared decision making, and other communication skills based on needs assessment findings and expert consensus. We addressed the five topics rated as highest importance to residents. While some communication topic areas such as delivering bad news, empathic responses, and communicating uncertain prognosis were identified as relatively high confidence areas on the needs assessment, they were still included in the educational intervention. Given the risk of falsely elevated confidence,18–20 and the critical importance of these communication skills, content experts agreed to include these in the intervention. Subjects deemed important but with lower confidence areas, such as shared decision making and prognostication, were also prioritized in our educational materials and intervention. Ethical and legal aspects of care were considered because this was of moderate relative importance but one of the areas of lowest confidence; this is a broad topic and felt it may require its own lecture and case sessions. This could be explored with future research or interventions.
Pre and post simulation survey results demonstrate that comfort increased across every palliative care topic area. The topics with the largest improvements were on questions 1, 2, and 6, which focus on communicating prognostic information and proposing time-limited trials. Interestingly, prognostic communication skills had a high degree of confidence on needs assessment. This emphasizes the power of simulation as a teaching tool to highlight growth opportunities and improve trainee confidence even in high-confidence areas. Similarly, a previous randomized control trial with simulation-based multisession workshops on palliative care communication skills delivered over an academic year was associated with improved self-assessed competency among healthcare trainees. 15
Strengths include that our development and assessment of our intervention was learner centered. Additionally, our case simulation fulfilled the commonly highlighted need for interactive learning with directly observed practice, debriefing, and feedback.9,10,25 Our feedback also suggests it was well-received and generally achieved the intended goal. There were some differences in the lecture materials and preparation between the two sites, but the pre-simulation comfort levels were not significantly different (except for question 1). The post-simulation levels were significantly different between the two sites for questions 1 and 5. Overall, the inclusion of data from multiple-centers suggests that the case-based simulation was easily replicable and can serve as a model for others. We demonstrated it is also feasible to deliver remotely, which was especially important during the COVID-19 pandemic. Social distancing and reliance on telehealth services pose unique challenges to providing optimal care for patients with neurological conditions that were directly or indirectly exacerbated by complications of COVID-19. 29
Our study has limitations. First, our sample sizes limit interpretation and generalizability of our results. Further, while the survey was anonymous, optional, and had no repercussions on academic standing, respondents may have rated their confidence higher than it actually was to avoid feeling embarrassed or out of fear of feeling incompetent. Those that responded may have perceived palliative care as being of higher importance than those who did not respond. Additionally, our needs assessment and simulation surveys evaluated subjective importance and confidence levels rather than objective knowledge of neuropalliative care topics. More robust evaluation methods with, for example, qualitative or open-ended feedback could have helped make an even stronger evaluation of the intervention.
Consistent with previous literature, the results of our study suggest room to improve education across many aspects of palliative care in neurology resident training that translates into better palliative care given the growing patient population living with complex neurological disease.5–10 The emergence of more fellowship training opportunities for neuropalliative specialists will hopefully begin to correlate with better education for neurology residents. 5 Next steps include repeating this course for additional residents. Future research can help understand the benefits and limitations of similar educational interventions, add to palliative curriculum for neurology residents, and subsequent study of outcomes that would signify better delivery of neuropalliative care to patients in need.
Supplemental Material
Supplemental Material - Needs-Driven Simulation Education: Advancing Neuropalliative Communication for Neurology Residents
Supplemental Material for Needs-Driven Simulation Education: Advancing Neuropalliative Communication for Neurology Residents by Katherine E. Makaroff, Alice Hawkins, Nathan Chu, Alex Aw, Jessica Besbris, Dan Karlin, Cara Siegel in American Journal of Hospice and Palliative Medicine®.
Supplemental Material
Supplemental Material - Needs-Driven Simulation Education: Advancing Neuropalliative Communication for Neurology Residents
Supplemental Material for Needs-Driven Simulation Education: Advancing Neuropalliative Communication for Neurology Residents by Katherine E. Makaroff, Alice Hawkins, Nathan Chu, Alex Aw, Jessica Besbris, Dan Karlin, Cara Siegel in American Journal of Hospice and Palliative Medicine®.
Footnotes
Ethical Considerations
The UCLA Institutional Review Board (IRB) exempted this minimal risk study from further review (IRB #23-000807). The Cedars-Sinai IRB exempted this minimal risk study from further review (IRB #00002169). There were no financial incentives offered for completion or participation in this study and participation was voluntary. All participant information was deidentified and data will not be shared with third parties.
Consent to Participate
Participant consent was obtained verbally.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.