
Abstract
Background
Palliative care in community settings can support seriously ill individuals to reduce symptoms and maintain quality of life. However, many individuals decline palliative care, even when they have health concerns. Differences in understanding how palliative care can help manage serious illness may contribute to declining.
Objective
This study explores the relationship between individuals’ understanding of palliative care, their health concerns, and education levels (a proxy for health literacy).
Methods
We use survey responses from a validated instrument assessing palliative care knowledge and information from semi-structured interviews for 21 seriously ill individuals (n = 3) and family caregivers (n = 18) who were eligible for community-based palliative care services and declined. We explore the relationship between respondents’ education, understanding of palliative care, and their concerns about their or their loved one’s health.
Results
Among participants, twelve had a bachelor’s degree or more; nine had some college or less. Six participants with some college or less expressed concerned about stress from serious illness. Of these, half (n = 3) did not understand palliative care could help. Conversely, five participants with a bachelor’s degree concerned about stress understood palliative care could help. Seven participants with some college or less expressed concerned about medication side effects; four did not understand palliative care could help. Conversely, three participants with a bachelor’s degree concerned about medication knew that palliative care could help.
Conclusion
Assessing health concerns and explaining how palliative care can address those concerns may reduce barriers to accepting palliative care, particularly among individuals with lower levels of education.
Keywords
Introduction
Sixty four percent (64%) of the over 55 million adults aged 65 and older in the United States (US) have two or more chronic medical conditions. 1 Individuals with poorly managed chronic conditions are often seriously ill and experience heavy symptom burden,2,3 psychological distress,4,5 and difficulty managing medications,6,7 all of which negatively impact quality of life.8-10 Poorly managed chronic conditions also place considerable burden on the healthcare system. 11
Palliative care provides support to relieve physical, psychological, and spiritual burden associated with disease to improve quality of life for seriously ill individuals and their families, regardless of disease stage.12,13 Palliative care’s team-based approach includes physicians, nurses, social workers, pharmacists, and therapists. 12 Alongside routine care and treatment, it provides pain and symptom management, advance care planning discussions, and referrals to other supportive services. 14 Community-based palliative care (CBPC) is provided in outpatient settings including doctor’s offices and in-home care. CBPC provides medical, spiritual, and social support,15-20 and benefits family caregivers 21 by reducing stress and improving quality of life.20,22
However, 64% of US adults know very little or not much about palliative care. 23 Palliative care is often confused with hospice care or end-of-life care, even though it is provided at any stage of serious illness.24-31 Distrust in the healthcare system due to exposure to racial discrimination and systemic racism, particularly for Black or African American individuals and for members of other racially and ethnically minoritized groups, may influence understanding of palliative care.32,33 As such, patients and families may decline palliative care, even when it could address their health concerns and challenges.
Lack of knowledge about palliative care and the services provided by CBPC may be partially attributable to lower levels of health literacy. Health literacy includes knowledge of health and healthcare, processing and using health information, and the ability to maintain health through self-maintenance and working with health providers. 34 Low health literacy is significantly associated with social determinants of health, 35 defined by the World Health Organization as the “conditions in which people are born, grow, live, work, and age” and include factors such as income and poverty, structural racism, access to housing, neighborhood conditions, and food accessibility. 36 Approximately 90% of adults in the US have health literacy insufficient to successfully navigate the healthcare system, and those aged 65 and older tend to have the lowest levels of health literacy. 37 Low health literacy, which disproportionately affects those with lower incomes and education levels, 38 is associated with poorer health outcomes and poorer use of healthcare services.39-42 Socioeconomic status, positively associated with educational attainment, 43 is the strongest determinant of health literacy 44 and significantly contributes to disparities in healthcare use. 45
Research on the role of health literacy in palliative care decision-making and enrollment is limited. However, prior research found health literacy is associated with hospice knowledge, attitudes, and decisions among community-dwelling older adults. 46 Other studies found that low levels of health literacy are a significant barrier to patient and family knowledge and planning surrounding end-of-life goals of care47,48 and is associated with higher odds of no hospice use, repeated hospitalization, and in-hospital death. 49 When faced with decisions surrounding care options for themselves or family members experiencing serious illness, individuals with low health literacy levels may be reluctant to engage clinicians in discussions and accept services if they do not understand what is being offered to them.
This study uses a novel approach of combining a validated palliative care knowledge scale paired with corresponding semi-structured interview data to gain a better understanding of why eligible individuals decline to enroll in CBPC services. Using the Palliative Care Knowledge Scale (PaCKS), a validated palliative care knowledge questionnaire, 50 and semi-structured interview responses, we examine how patient and family caregiver knowledge of palliative care, health concerns, and education level compare in decisions to decline CBPC services. Identifying barriers to accepting palliative care may help clinicians develop targeted strategies for explaining the potential benefits of palliative care to eligible individuals and their family members.
Methods
Participants. This analysis is part of a larger study examining decisions to decline CBPC services at a Medicare Advantage (MA) health insurance plan provided by a non-profit healthcare provider in the Northeastern US that serves a racially and ethnically diverse population. Individuals were eligible for the study if they were an MA plan member who had been offered palliative care services in the previous year and declined, or if they were a caregiver of an MA plan member who declined palliative care. Seventy-five (75) individuals had declined palliative care in the previous year. Of these, we contacted 70 before reaching thematic saturation in study interviews. Of the 70, 15 were not interested, 20 were unreachable, 5 were deceased, and 7 were ineligible to participate (eg, did not speak English). The remaining 23—4 MA plan members and 19 family caregivers—enrolled in the study. One family caregiver dropped out after informed consent was obtained and before study activities occurred. One plan member was excluded from the results because they completed the interview but not the Palliative Care Knowledge Survey (PaCKS). We analyzed responses for 21 participants. Each participant provided informed consent and was compensated $75. All study activities were approved by the appropriate institutional review boards.
Data. We used two data sources in this analysis. First, prior to the interview, participants completed a demographic questionnaire and the PaCKS. Participants were given the option of completing these questions through an online survey (n = 14) or over the phone with trained research staff (n = 7). The PaCKS is a validated survey that assesses general palliative care knowledge. 50 It is comprised of 13 true/false questions about the scope of palliative care with respect to psychological and symptom relief, disease management, and hospice care, with higher scores indicating greater knowledge of palliative care (possible range: 0 = 13). Second, participants completed a semi-structured interview that included questions about their experience with and knowledge of palliative care and their concerns regarding their or their family member’s health. Interviews were conducted by telephone or videoconference according to the participant’s preference, audio recorded and transcribed, and lasted an average of 27 min (range: 6-50 min). Research staff took detailed notes during interviews which were summarized in a memo.
Data analysis. Study team members met weekly while interviews were conducted to identify common themes found during the interviews. A preliminary set of codes was created based on interview questions and themes identified during weekly meetings. A small number of additional codes were generated during the transcript coding process. Codes included palliative care knowledge, palliative care experience, and healthcare concerns. Each transcript was independently coded by two individuals on the study team, which consisted of four individuals who were trained and supervised by the Principal Investigator, who is experienced in descriptive analysis, qualitative methods, and palliative care research. After coding was completed, team members met to discuss coding decisions and reach agreement on discrepancies. Interview data analysis was conducted using NVivo 14.
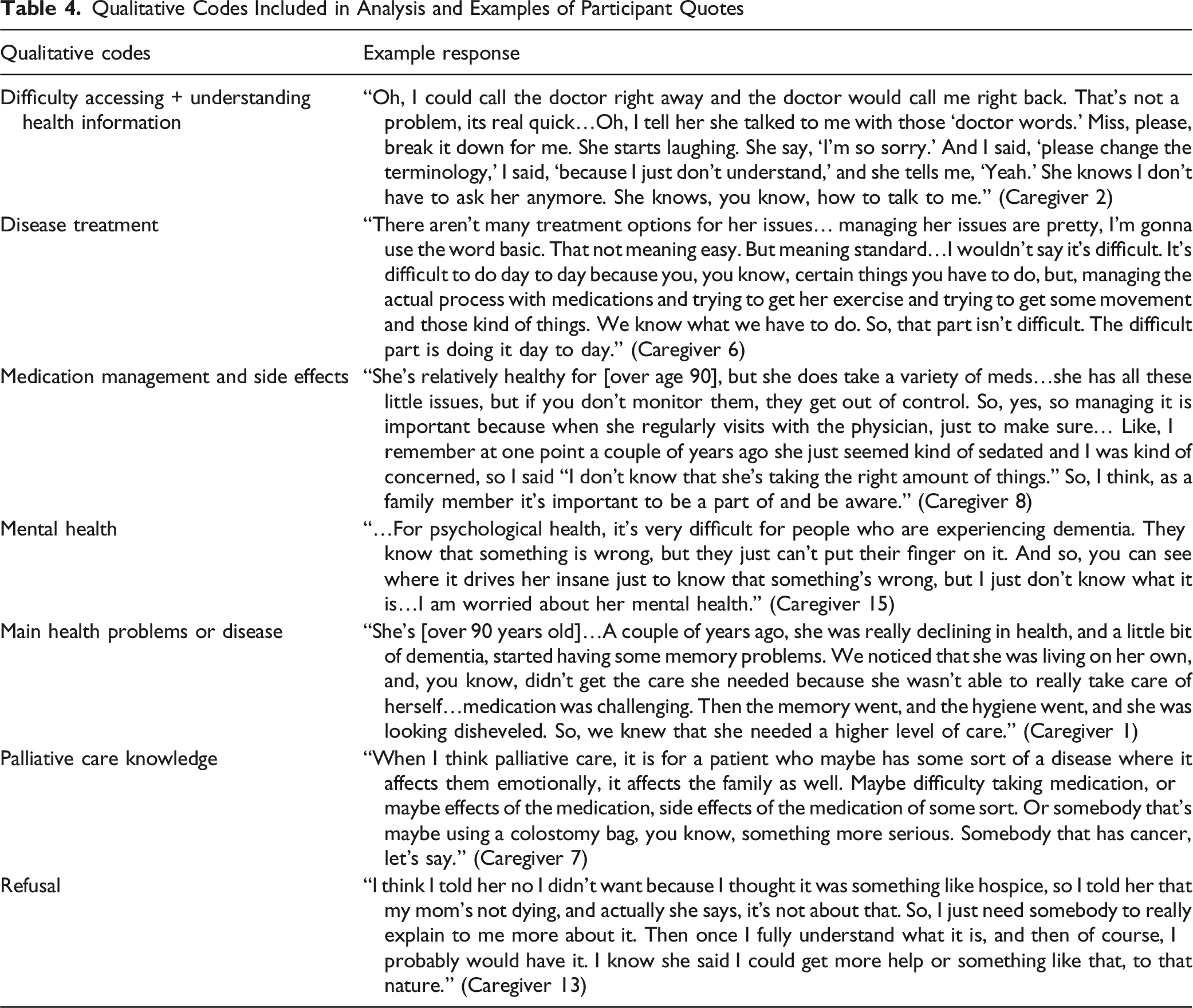
We selected codes for analysis corresponding to interview questions related to two PaCKS items: (1) “Stress from serious illness can be addressed by palliative care,” and (2) “Palliative care can help people manage the side effects of their medical treatments.” We then compared responses to PaCKS items to information provided in interviews. We examined participant responses to four questions asked as part of a longer interview about their experiences managing their/their loved one’s health and with palliative care. The first two were asked in a series of questions related to challenges the participant (for MA plan members) or their family member (for caregivers) face in managing their health: “How worried are you about you/your loved one’s psychological health or feelings of stress?” and “How worried are you about managing side effects from medicine you/they take?.” The remaining questions were asked in a series of questions asking why the participant declined palliative care services: “Can you please talk about why you said no to palliative care?” “Were you worried about your/their psychological issues or stress?” and “Were you worried that you/they would have to stop taking medication for their illness(es)?” To capture additional references to concerns about stress and treatment side effects that participants mentioned elsewhere in the interviews, we analyzed responses that were coded by the research team as related to “difficulty accessing and understanding health information,” “disease treatment,” “medication management and side effects,” “mental health,” “main health problem or disease,” “palliative care knowledge” and “refusal.”
Results
Sample Description for 21 Medicare Advantage Plan Members and Their Family Caregivers
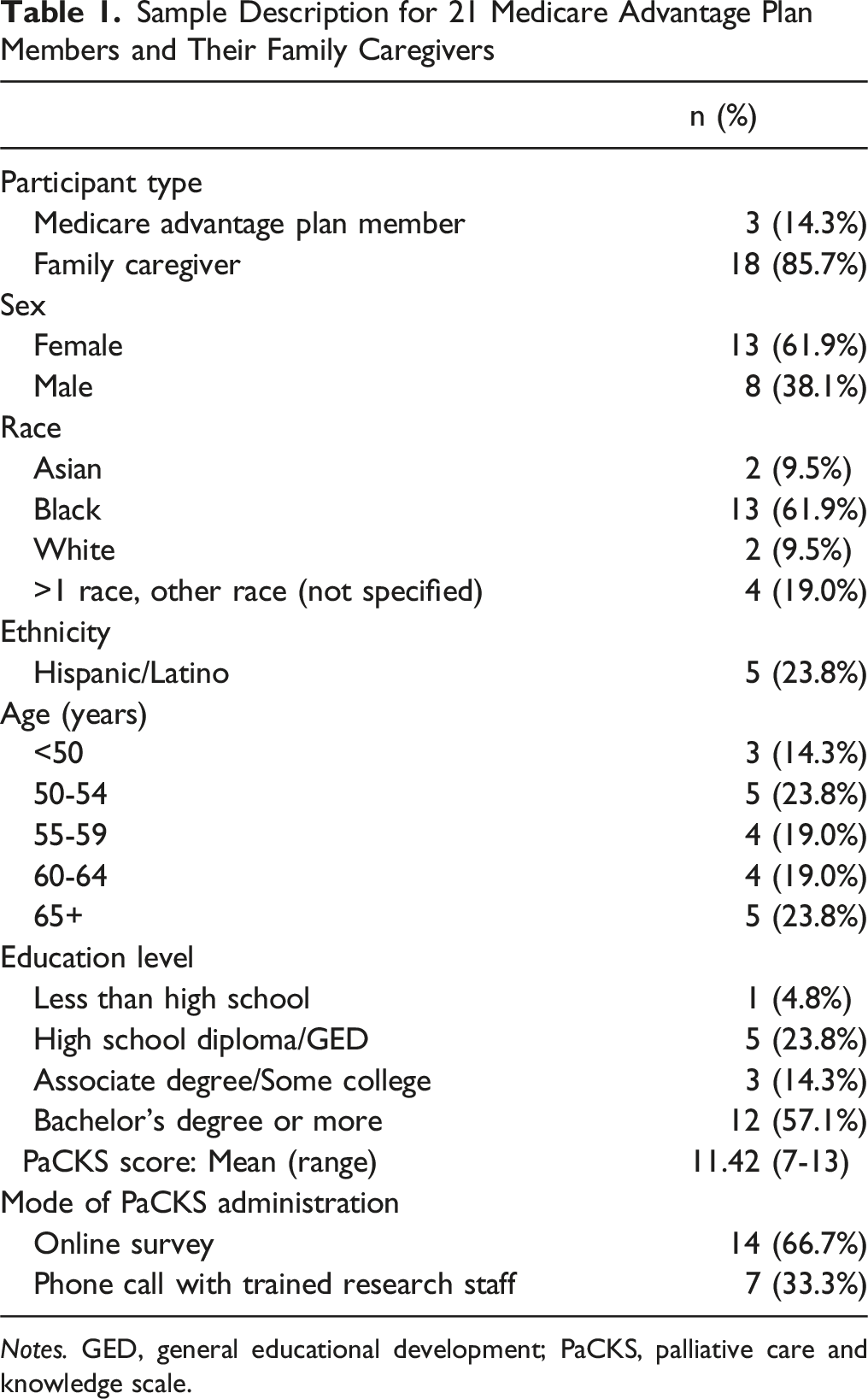
Notes. GED, general educational development; PaCKS, palliative care and knowledge scale.
PaCKS Scores. Participants averaged 11 on the PaCKS (sample range: 7-13). Those with the highest scores had some college or higher education. Of the six participants that scored perfectly, five had a bachelor’s degree or more and one had some college. In contrast, education levels differed among the two participants with the lowest PaCKS scores. One had high school/GED equivalent, the other a bachelor’s degree or more.
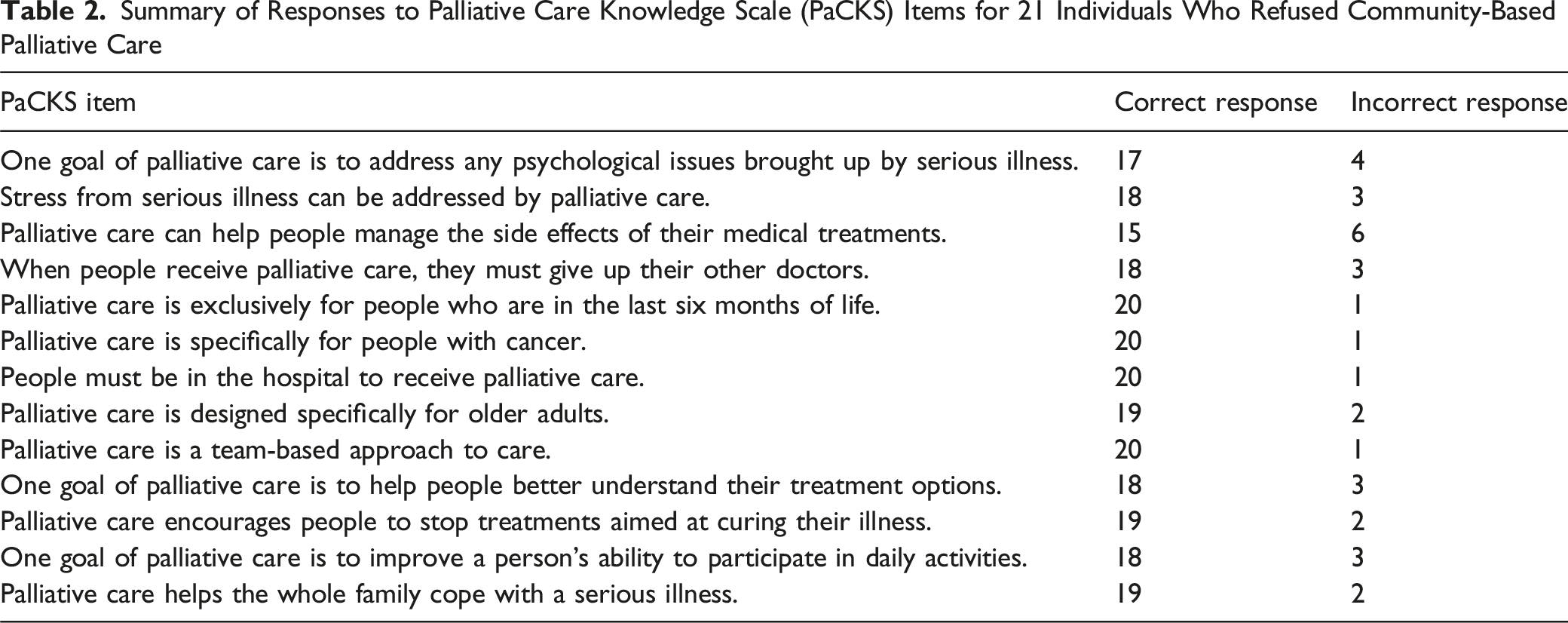
Summary of Responses to Palliative Care Knowledge Scale (PaCKS) Items for 21 Individuals Who Refused Community-Based Palliative Care
Comparison of PaCKS Responses and Participant Concern by Education Level
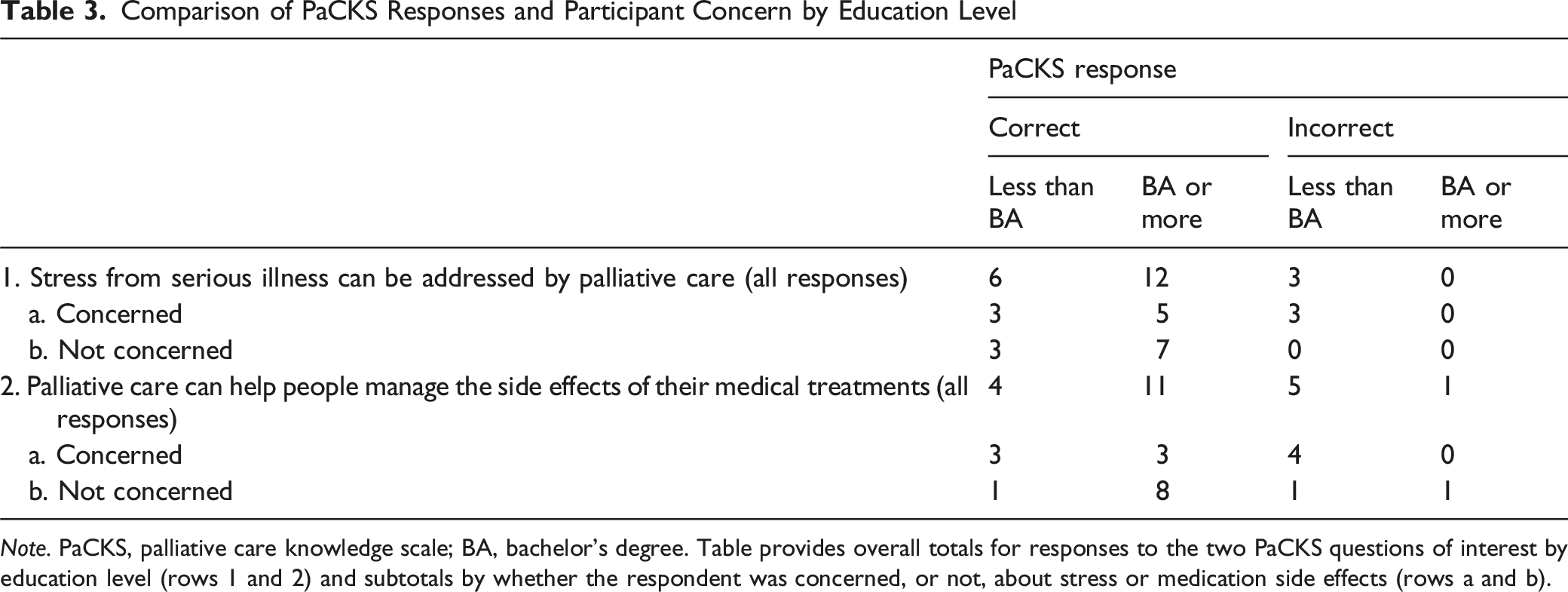
Note. PaCKS, palliative care knowledge scale; BA, bachelor’s degree. Table provides overall totals for responses to the two PaCKS questions of interest by education level (rows 1 and 2) and subtotals by whether the respondent was concerned, or not, about stress or medication side effects (rows a and b).
Eighteen individuals correctly responded that palliative care could help address stress. Eight (44%) of these individuals were concerned about their or their love one’s stress levels in the interviews. Caregiver 6 stated “We would like to see my mother live as comfortably as possible for as long as she can. This is obviously her end of life. So, we would just want her to be as comfortable as possible at home and not having these stresses.” The other ten (56%) participants stated that they weren’t worried or had other issues to worry about. One member said “I’m fine. Stress is gonna come and go, that’s life… I worry about a lot of things, but I’m not worried about being depressed and anything. Things happen.” (Member 4).
Of the eight individuals who answered correctly and were concerned three (37.5%) had less than a bachelor’s degree and five (62.5%) had a bachelor’s degree or more. Of the ten individuals who answered correctly and were not concerned three (30%) had less than a bachelor’s degree and seven (70%) had a bachelor’s degree or more.
Of the three participants who did not understand that palliative care can help with stress, all (100%) were concerned about their or their loved one’s stress levels. Caregiver 16 mentioned “Well, I mean, I think I be kinda worried sometimes, but what can I do about that? I mean, it’s part of life.” All had less than a bachelor’s degree.
A more mixed picture emerged with respect to knowledge of palliative care’s role and their concern for managing treatment side effects. Fifteen individuals correctly responded that palliative care could help people manage side effects of their medical treatments. Six (40%) of these individuals were worried about managing side effects and nine (60%) were not. Caregiver 17 expressed difficulty with keeping track of medications: “It can be hard. She uses eye drops multiple times throughout the day for her eye, for her vision. And she does take her blood pressure medication. So, we have to be on top of that.”
The nine participants who understood palliative care could help with treatment side effects but were not concerned about them were in a situation where either the patient did not take medication or the family had someone they could contact with questions. One caregiver shared: “She don’t take that much medication. She’s okay.” (Caregiver 18). Another reflected, Well, the good thing about it is that my sister-in-law, her daughter, is a registered nurse… I rely on her daughter to decipher the medical piece of it. And so, she's able to watch it, you know, watch the medication with conversations from me. Yeah, I... So, I'm not as worried because I have somebody to lean on for that. (Caregiver 15).
Of the six participants who understood palliative care could help with side effects and were concerned about managing them, three (50%) had less than a bachelor’s degree; the other three (50%) had a bachelor’s degree or more. Of the nine individuals who were not concerned, one (11%) had less than a bachelor’s degree and eight (89%) had a bachelor’s degree or more.
Of the six individuals that did not know palliative care could help manage treatment side effects, four (67%) were worried about managing side effects. All of these indivdiuals had less than a bachelor’s degree. Caregiver 13 recounted an experience her mother had using medication: Oh, I was worried. One time, my mom, I had to go over to her house because she-- I don't know if she has fell out and she hurt whole face, her whole mouth was swollen up and puffed up and I thought something happened… We went to the ER, and I was devastated. I was there, I said, ‘Does this look like some type of abuse or her lips are puffed up or anything?’ They said, ‘No it was an allergy reaction from the Lisinopril.’ … So, yeah, of course, I get worried and get upset and scared, and she have any type of reactions from any type of medication.
Qualitative Codes Included in Analysis and Examples of Participant Quotes
Discussion
This study takes a novel methodological approach in comparing individuals’ knowledge of palliative care using a validated scale with responses to questions in semi-structured interviews about their health concerns. We found that participants with a bachelor’s degree or more tend to be less concerned about stress and managing treatment side effects. They also had a more accurate understanding of how palliative care can help with both of these concerns. To the extent education is associated with health literacy,44,45 our findings could be an indication that, regardless of their knowledge of palliative care, individuals with more education feel more confident navigating healthcare systems or obtaining needed support for themselves or their loved ones. To the extent education is associated with broader socioeconomic status, 43 they may have access to additional resources such as stable healthcare providers or paid caregivers that reduce their concerns.
For individuals who are worried about specific health issues and understand that palliative care can help, but still decline it, additional information is needed to understand why they forego a service that might help address their concerns. Participants with less than a college degree more often expressed concern regarding managing stress and treatment side effects. They also tended to have a more mixed understanding of how palliative care might help with these concerns. For individuals who are worried about health issues but do not understand if or how palliative care can help, structured conversations that ask about specific health concerns, followed by education about how palliative care might help, may encourage them to accept palliative care services. Mistrust in the medical system and providers may be a deterrent to engagement with palliative care, particularly among Black or African American individuals, who represented a majority of our sample. 33 Asking patients about past experiences with hospice or palliative care, religious preferences, and goals with respect to managing their health may help providers frame discussions about palliative care in a way that resonates with patient values and encourages palliative care uptake.51,52 The “Ask-Tell-Ask” approach to communication, which starts with a patient’s understanding of their health, followed by a straightforward explanation of palliative care and how it can help, and checking the patient’s understanding, may provide a guide for conversations about the role of palliative care in addressing health concerns. 53
The terminology healthcare personnel use also creates confusion and stigma regarding palliative care, creating a need to redefine and destigmatize the language surrounding palliative care. 26 Palliative care should be explained to seriously ill older adults and their caregivers in a way that is tailored to how the service can address their health statuses and concerns.(31) It should also be emphasized that palliative care is not end of life care.
Limitations. This study has limitations. The sample size is too small to perform formal statistical analyses, precluding assessment of statistically significant relationships and limiting generalizability of results. However, observed patterns warrant further investigation, such as how to inform individuals with lower education levels that palliative care can help with their health concerns. Among all individuals eligible for the study, a higher percentage of Black and Asian individuals participated and lower percentage of White individuals participated compared to those who did not participate, indicating potential recruitment bias. Additionally, the sample was highly educated, potentially yielding different patterns than in a sample with more diverse education levels. We may observe different patterns of health literacy and palliative care knowledge among non-English-speaking individuals. As the study was designed to understand why individuals refuse palliative care, we are unable to compare education levels between our sample and individuals who accepted palliative care. We were not able to evaluate other factors that may influence health literacy or healthcare decision-making such as experiences with racial discrimination, trust in healthcare providers, or religious preferences. Finally, results reflect the experiences of individuals at one MA plan and may not be generalizable to other MA plans.
Conclusion. Palliative care is a resource for seriously ill individuals and their caregivers. However, many seriously ill individuals that could benefit from palliative care do not accept it, even when it could address their health concerns such as managing stress. This pattern was observed among individuals with lower levels of education. In contrast, in the case of concern and palliative care knowledge regarding treatment side effects, there was no relationship with education level. Regardless of education level, increasing understanding of palliative care or providing additional education about palliative care may encourage uptake of services, particularly among individuals who are worried about their or their loved one’s well-being and illness management. Identifying specific health concerns and tailoring responses about how palliative care might address their concerns may improve uptake of palliative care among seriously ill individuals concerned about managing stress and medication.
Footnotes
Ethical Considerations
All study procedures were approved by VNS Health and Rutgers University’s Institutional Review Boards.
Consent to Participate
All participants provided informed consent.
Author Contributions
AA and EL were responsible for study design. AA, KS, and EL conducted and transcribed participant interviews and analysed data. AA, KS and EL drafted the manuscript. AA, KS, and EL contributed to manuscript revisions. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by a pilot grant from the University of Pennsylvania Roybal Center on Palliative Care in Dementia and the National Institute on Aging (NIA), a department under the National Institute of Health (NIH) under award number P30AG064105. The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.