
Abstract
Background
Chemotherapy at the end of life may not extend survival and can diminish quality of life. Understanding patterns of use is critical to ensuring equitable, patient-centered care.
Objective
To examine racial and ethnic disparities in chemotherapy receipt within 30 days of death among patients with colon cancer, and whether these disparities changed over time.
Design
We conducted a retrospective cohort study using the National Cancer Database, identifying patients with colon cancer who died within 30 days between 2004 and 2021. The final sample included 43 490 patients. The primary outcome was chemotherapy receipt within 30 days of death. Multivariable logistic regression adjusted for demographics, insurance, comorbidities, facility characteristics, and socioeconomic factors. A difference-in-differences approach compared 2 periods: 2004-2012 and 2013-2021.
Results
Among 43 490 patients (mean age, 75.6 years; 51.1% female), 1275 (2.9%) received chemotherapy near death. Adjusted analyses found no statistically significant racial or ethnic differences in use. However, Asian American patients had a marginally increased likelihood of receiving chemotherapy over time compared with non-Hispanic White patients (interaction OR, 2.25; 95% CI, 0.95-5.32; P = .065). Older age (≥80 years: OR, 0.12), higher comorbidity burden (Charlson-Deyo score ≥2: OR, 0.61), and uninsured status were associated with lower odds of treatment. Private insurance (OR, 1.67) and treatment at comprehensive cancer centers were associated with higher odds.
Conclusion
While overt racial disparities were not observed, disparities by insurance and facility type point to structural inequities that should be addressed in future quality improvement efforts.
Introduction
Chemotherapy administered within 30 days of death has become an important quality metric in oncology, 1 as it often provides limited clinical benefit while potentially diminishing quality of life and increasing healthcare costs during patients’ final weeks of life.2-4 The American Society of Clinical Oncology and other professional organizations have identified aggressive end-of-life care, including chemotherapy use within 30 days of death, as a marker of poor-quality cancer care. 5 Despite growing emphasis on palliative care and advance care planning,6,7 substantial variation persists in end-of-life chemotherapy use across different healthcare settings and patient populations. 8
Racial and ethnic disparities in cancer care have been extensively documented across the continuum from screening and diagnosis through treatment and survivorship. Black and Hispanic patients often experience delayed diagnosis, receive less guideline-concordant treatment, and have worse survival outcomes compared with White patients.9-11 However, the relationship between race, ethnicity, and end-of-life cancer care is more complex, as disparities in this context may paradoxically represent both underuse of beneficial palliative interventions and overuse of aggressive treatments that provide little benefit. 12 In fact, 1 study conducted in over 84 countries revealed that 20% of ICU patients endured some form of futile care, with only a small fraction of them surviving the hospital period. 13 With the significant limitations and risks of futile care, the disparities in the prevalence of futile care administered to different subpopulations becomes a major public health focus area. Some studies have suggested that minority patients may be more likely to receive aggressive end-of-life care, 14 potentially reflecting differences in cultural attitudes toward death and dying, 15 communication patterns with healthcare providers, 16 or differential access to palliative care services.
Colon cancer represents an ideal model for studying end-of-life care disparities, as it is the third most common cancer diagnosis in the United States and has well-established treatment guidelines. 17 While systemic chemotherapy can provide meaningful symptom relief and quality-of-life benefits in the palliative setting, 18 its use very close to death is generally considered inappropriate. 19 Previous research has shown that patients who receive chemotherapy within 30 days of death are less likely to die at home, more likely to be admitted to intensive care units, and less likely to receive hospice care, suggesting cascade effects on overall end-of-life care quality. 20
Despite the clinical importance of this issue, limited research has specifically examined racial and ethnic disparities in end-of-life chemotherapy use among colon cancer patients, and whether such disparities have changed over time as awareness of end-of-life care quality has increased. Understanding these patterns is crucial for developing targeted interventions to improve equity in end-of-life cancer care. 21 Therefore, we conducted this study to examine racial and ethnic disparities in chemotherapy receipt within 30 days of death among patients with colon cancer using a large, national cancer registry, and to assess whether these disparities changed between 2004-2012 and 2013-2021.
Methods
Study Design and Data Source
We conducted a retrospective cohort study using data from the National Cancer Database (NCDB), a joint program of the American College of Surgeons and the American Cancer Society that captures approximately 70% of newly diagnosed cancers in the United States.22,23 The NCDB collects comprehensive information on patient demographics, tumor characteristics, treatment details, and outcomes from Commission on Cancer-accredited facilities. We included patients diagnosed with colon cancer between 2004 and 2021 who died within 30 days of diagnosis, had complete data on key covariates including median income quartile, facility type, and chemotherapy receipt, and excluded those with unknown or refused race/ethnicity information. The final analytic cohort comprised 43 490 patients. This study was deemed exempt from institutional review board approval as it used de-identified registry data.
Patient and Public Involvement
Patients and members of the public were not involved in the design, conduct, reporting, or dissemination of this study. The analysis was based on retrospective, deidentified data from the National Cancer Database. As such, there was no direct contact with participants, and no mechanisms for patient or public involvement were incorporated into the study protocol.
Variable Definitions and Statistical Analysis
The primary outcome was receipt of chemotherapy within 30 days of death, defined as any systemic chemotherapy administration. Race and ethnicity were categorized using NCDB coding into 6 mutually exclusive groups: Non-Hispanic White, Non-Hispanic Black, Hispanic (any race), Non-Hispanic American Indian/Alaska Native, Non-Hispanic Asian American, and Non-Hispanic Native Hawaiian/Pacific Islander. Covariates included age (categorized as 18-64, 65-74, 75-79, and ≥80 years), sex, insurance status, median household income quartile, facility type, percentage of adults without high school education quartile, and Charlson-Deyo comorbidity score. To assess temporal trends, we divided the study period into 2 cohorts: 2004-2012 and 2013-2021. We used multivariable logistic regression to examine associations between race/ethnicity and chemotherapy receipt, adjusting for all covariates and calculating odds ratios (ORs) and 95% confidence intervals (CIs). A difference-in-differences approach with interaction terms between time period and race/ethnicity assessed whether disparities changed over time. Statistical significance was set at P < .05, and analyses were performed using Stata version 17.0 (StataCorp LLC).
Results
Study Population
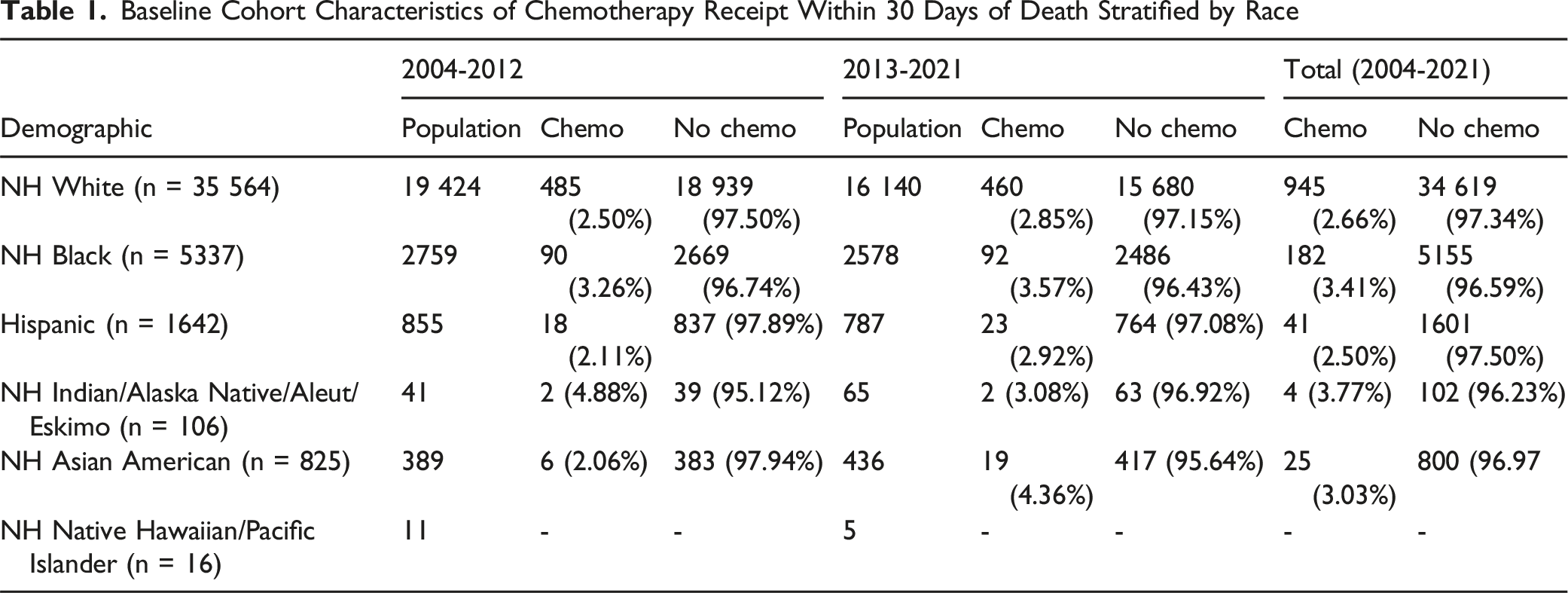
The final analytic cohort included 43 490 patients with colon cancer who died within 30 days of diagnosis and met all inclusion criteria. The majority of patients were Non-Hispanic White (81.8%), followed by Non-Hispanic Black (12.3%), and Hispanic (3.8%) individuals. Most patients were aged 80 years or older (50.8%), with Medicare as the primary insurance (77.5%). The study period was divided into 2 cohorts: 23 479 patients (54.0%) diagnosed between 2004-2012 and 20 011 patients (46.0%) diagnosed between 2013-2021.
Chemotherapy Use Patterns
Baseline Cohort Characteristics of Chemotherapy Receipt Within 30 Days of Death Stratified by Race
Multivariable Analysis
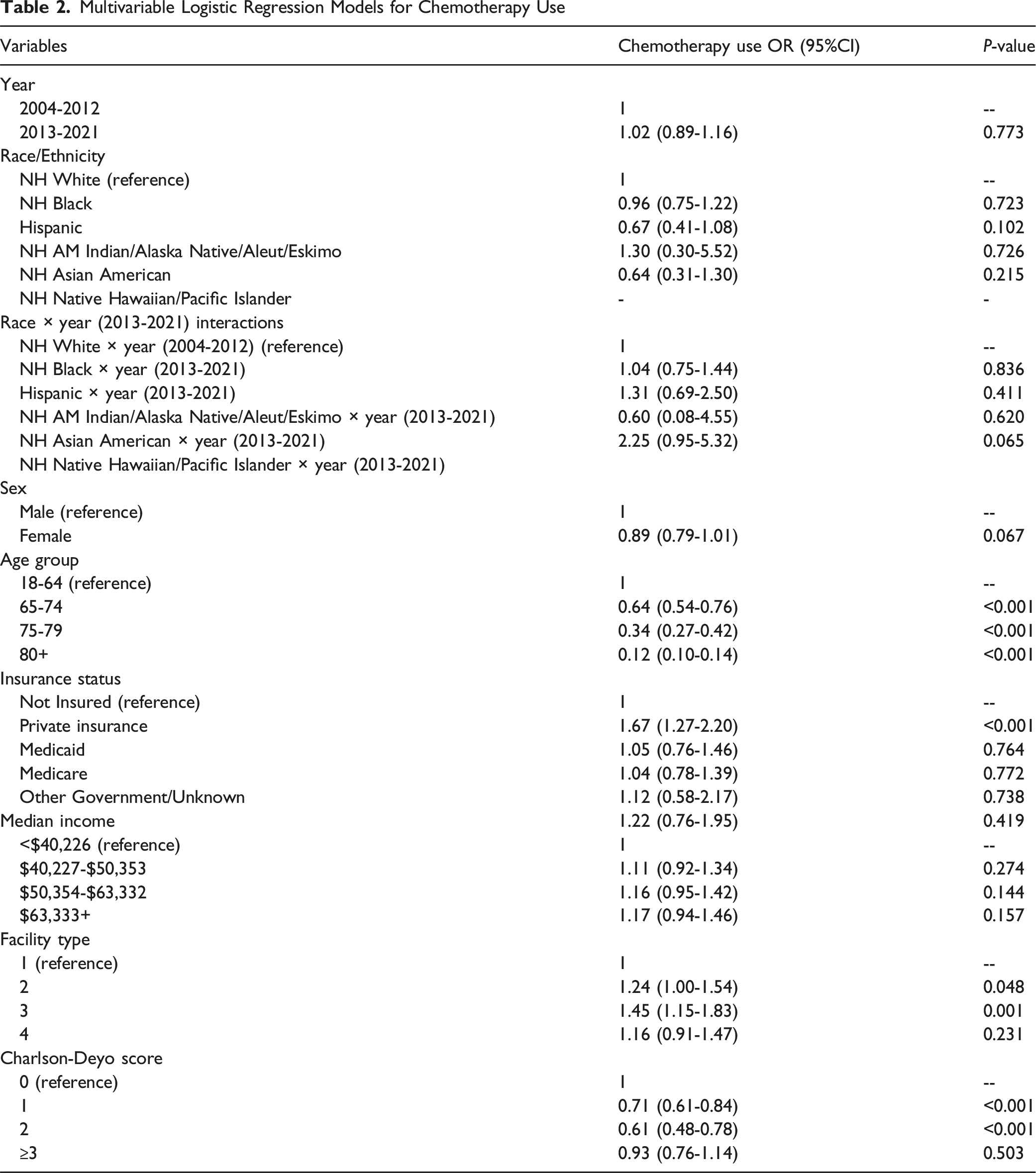
In the difference-in-differences logistic regression model adjusting for patient demographics, insurance status, socioeconomic factors, facility characteristics, and comorbidities, there was no statistically significant overall change in chemotherapy use between time periods (OR, 1.02; 95% CI, 0.89-1.16; P = .77). Compared with Non-Hispanic White patients, there were no statistically significant differences in chemotherapy receipt for any racial or ethnic minority group in the main effects model.
However, the interaction between time period and race revealed potentially important trends. Non-Hispanic Asian American patients showed a marginally significant increase in chemotherapy use in the later time period compared with Non-Hispanic White patients (interaction OR, 2.25; 95% CI, 0.95-5.32; P = .065). No other racial or ethnic groups demonstrated significant changes in chemotherapy use patterns over time (Figure 1 and Table 2). 30-day chemotherapy by race and time period. Note. Some categories have small sample sizes Multivariable Logistic Regression Models for Chemotherapy Use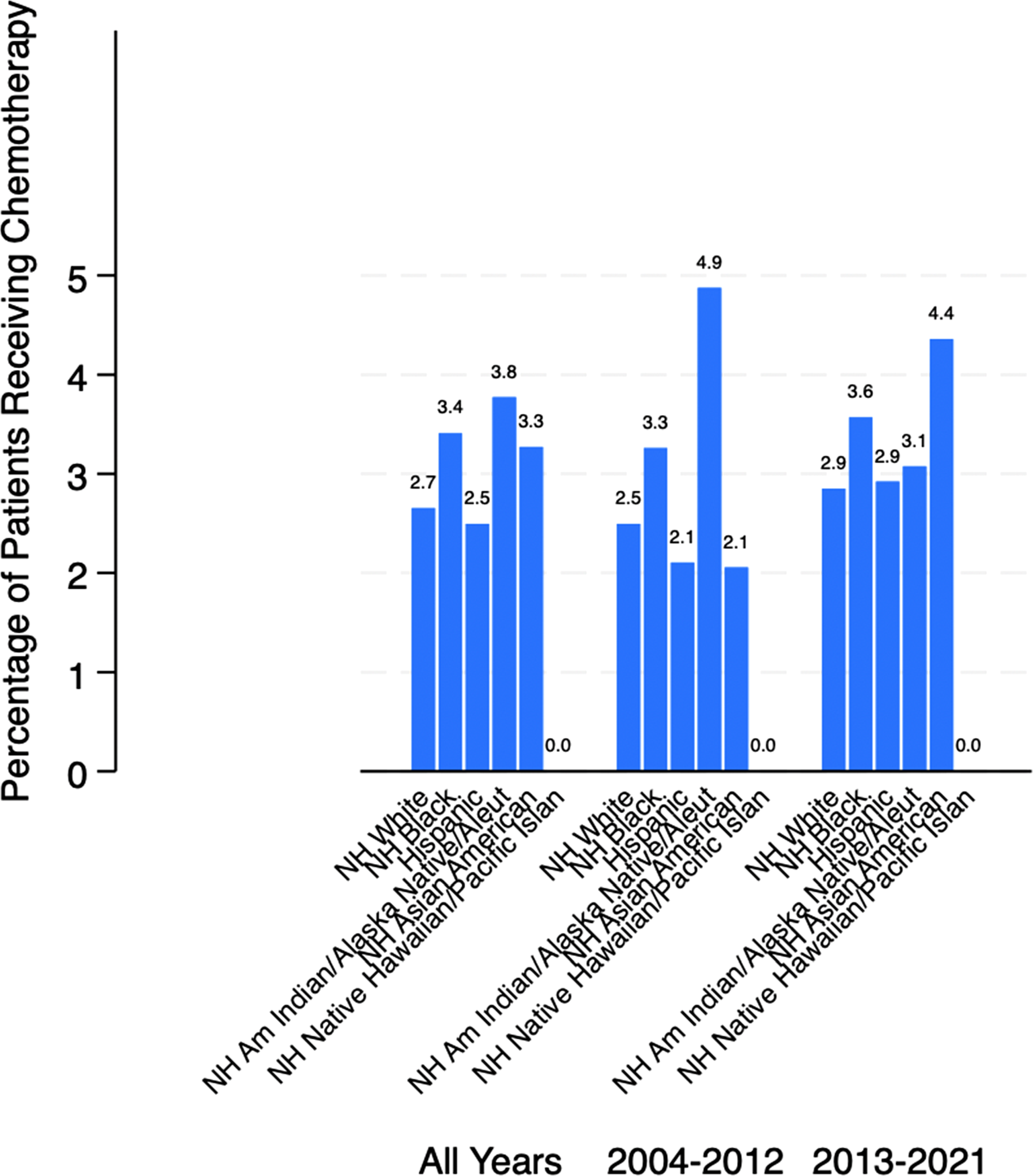
Other Associated Factors
Several patient and system factors were significantly associated with chemotherapy receipt. Advanced age was strongly associated with lower odds of receiving chemotherapy, with patients aged 75-79 years (OR, 0.34; 95% CI, 0.27-0.42) and those 80 years or older (OR, 0.12; 95% CI, 0.10-0.14) substantially less likely to receive treatment compared with younger patients. Private insurance coverage was associated with higher odds of chemotherapy use (OR, 1.67; 95% CI, 1.27-2.20) compared with uninsured patients. Treatment at comprehensive community cancer programs (OR, 1.45; 95% CI, 1.15-1.83) and academic/research programs showed higher odds of chemotherapy use. Higher comorbidity burden was associated with lower chemotherapy use, with patients having Charlson-Deyo scores of 1 (OR, 0.71; 95% CI, 0.61-0.84) or 2 (OR, 0.61; 95% CI, 0.48-0.78) less likely to receive treatment.
Discussion
This nationally representative, population-based study reveals that chemotherapy use within 30 days of death among colon cancer patients remains relatively low at 2.7%, though there are several variations by race and ethnicity. Our findings reflect a lack of statistically significant disparities in chemotherapy use, which suggests that overt differences in end-of-life chemotherapy prescription are less pronounced than other forms of cancer care.9-11 However, there was a distinct rise in chemotherapy use between 2004 and 2021 for Non-Hispanic Asian American patients, warranting further investigation into evolving cultural attitudes toward aggressive end-of-life care, 15 changes in clinical decision-making patterns, or equity concerns influenced by the COVID-19 pandemic. 14
The strong inverse relationship between patient age and chemotherapy receipt aligns with existing clinical standards, as older adults typically derive fewer benefits and face greater risks from aggressive treatment.2,3,6 Similarly, the association between higher Charlson-Deyo comorbidity scores and lower chemotherapy use suggests that clinicians are appropriately weighing treatment burden against competing mortality risks. 7
Patients with private insurance were significantly more likely to receive chemotherapy near the end of life. This pattern raises equity concerns and suggests that insurance status may influence not just access to care but also treatment decisions.9,10,21 Disparities may stem from differences in access to timely diagnosis, continuity of care, 11 or communication and shared decision-making across insurance types. The higher odds of chemotherapy use at academic centers may reflect institutional variation in practice patterns, referral systems, or specialist involvement. 8
Future research should examine the mechanisms behind these disparities, particularly the roles of cultural norms, provider communication, 16 and individual preferences. Qualitative studies could offer deeper insight into how end-of-life decisions are made and help guide interventions to promote equitable, patient-centered care across diverse populations.14,21
In parallel, prior literature highlights the importance of early palliative care and informed decision-making about end-of-life systemic therapy. Randomized controlled trials have shown that introducing palliative care at the time of metastatic cancer diagnosis improves quality of life, reduces depressive symptoms and aggressive end-of-life care, and can even lengthen median survival. 24 More recently, a stepped palliative care model, with visits triggered by declining quality of life, achieved comparable quality-of-life benefits with substantially fewer visits, demonstrating a scalable approach to delivering early palliative services. 25 Observational studies further highlight that systemic treatment near the end of life is generally low-value, being strongly associated with increased emergency department visits, hospitalizations, late hospice enrollment, and higher costs.26,27 Although overall rates of end-of-life treatment have not declined in the immunotherapy era, there has been a shift from cytotoxic chemotherapy to checkpoint inhibitors and other targeted agents, 28 and continued administration of these therapies beyond the point of futility is linked to increased acute-care utilization. 29 Prognostic tools such as the Palliative Prognostic Index (PPI) can more accurately estimate short-term survival for patients with advanced cancer. Incorporating such indices into practice may help clinicians recognize when to de-escalate or stop chemotherapy, potentially preventing overuse of treatment and reducing hospitalizations for treatment-related complications.30-32 Past findings show that early palliative interventions and use of prognostic guidance are associated with fewer chemotherapy administrations in the last weeks of life and higher hospice utilization. 33 Collectively, these findings reinforce the need for early, structured palliative care consultation and the development of evidence-based guidelines to avoid systemic therapy when the likelihood of benefit is minimal.
Equitable decision-making at the end of life also demands cultural humility and attention to communication barriers. Cultural beliefs and values profoundly shape how patients and families understand death, pain management, and the meaning of palliative and hospice care. 34 Limited English proficiency and linguistic differences can further impede shared decision-making; qualitative research indicates that patients with limited English proficiency have lower hospice utilization and poorer advance care planning, and that medical interpreters often struggle to navigate complex terminology and emotional nuances.35,36 Palliative care experts have therefore called for culturally tailored information and interpreter training to ensure that prognostic information and goals-of-care discussions are accessible across diverse populations.36,37 This need is particularly urgent in resource-constrained settings, where systemic factors often limit patients’ ability to participate in end-of-life decisions. For example, Shahjalal et al found that in Bangladesh, patients with advanced cancer rarely engaged in shared decision-making due to physician time constraints, inadequate healthy literacy rates, and cultural norms around deference to clinicians. 38 Respectful, culturally sensitive communication, supported by interpreters when needed, is essential to aligning treatment with patients’ goals of care and to encouraging timely transitions to hospice or comfort-focused care.
Conclusion
While racial disparities in end-of-life chemotherapy use among colon cancer patients appear limited, structural factors such as insurance status and treatment setting continue to shape care. Promoting equity in end-of-life decision-making will require more consistent communication, greater access to palliative care, and targeted efforts to ensure treatment aligns with patient values across all demographic groups.
Footnotes
Ethical Considerations
Ethical approval was not required for this study as it involves utilizing a publicly available national database.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data supporting the findings of this study are included within the manuscript. Additional details are available from the authors upon reasonable request.