
Abstract
Background
Goals-of-care (GOC) discussions align medical treatment with older adults’ preferences, yet are hindered by communication barriers, provider discomfort, and misinformation. Video-based decision aids improve understanding and reduce decision conflict, though data on their use in older populations remain limited. This review aimed to determine the effectiveness of video-based decision aids in improving GOC discussions and decision-making outcomes among older adults.
Methods
For this systematic review, a medical librarian conducted a literature search of Medline, Embase, Web of Science, CINAHL, PsychINFO, and Cochrane from database inception through April 2025. Eligible studies evaluated a video-based aid in US adults aged ≥65 years to facilitate GOC or code status decisions. The Cochrane Risk of Bias tool was used to assess quality of randomized, interventional studies.
Results
Of 4438 identified studies, 7 underwent full review, and 5 met inclusion criteria. Among inpatient settings, 2 studies found video interventions significantly increased patient preference for comfort-based care, while another using a shorter video, found no effect. In outpatient settings, one study found increased preference for comfort-based care with video intervention, while another reported no preference differences. Two studies assessed knowledge; one inpatient study found no change, while an outpatient study reported greater end-of-life knowledge in the intervention group. Video variability and differences in measured outcomes limited comparisons and generalizability.
Conclusions
Video-based decision aids show promise for improving knowledge and aligning treatment preferences. Further studies are needed to investigate the impact of video-based decision aids on GOC conversations in older adults in acute care settings.
Keywords
Introduction
Goals-of-care (GOC) discussions are important in older adult care (aged 65+) and align with the “what matters most” pillar of the 4 Ms (what matters, medication, mentation, and mobility) framework of Age-Friendly Health systems. These best practice guidelines emphasize prioritizing older adults’ health care preferences and goals to better align care plans with values, improve clinical outcomes, and reduce treatment burden.1,2 Additionally, shared decision-making, which occurs during GOC discussions is associated with less aggressive care at the end-of-life, 3 improved quality of life, 4 reduced ICU length of stay, 5 and delivery of values congruent treatments. 6
Despite these many benefits, there are multiple barriers to effective GOC discussions. Physicians report struggling with GOC discussions, especially when caring for critically ill patients, due to a lack of preparedness, concern for causing emotional distress, and language or health literacy constraints.7-12 When GOC discussions do occur, they are often brief and ineffective at increasing knowledge about cardio-pulmonary resuscitation (CPR), intubation, and other life-sustaining medical interventions and often fail to follow a shared-decision-making framework.13,14 GOC conversations can be especially difficult for older adults as they tend to have increased complexity of illness due to frailty and multimorbidity,15-17 emotional responses to reflecting on death, 18 and patient or family denial of prognosis.19,20 Additionally, older adults are highly susceptible to framing effects—cognitive biases that occur when the language used to present information influences individuals’ decision-making. Therefore, this population may require a more systematic, unbiased approach during medical decision-making. 21
Video based interventions have been described as a promising technique to improve knowledge, reduce decisional conflict, and support values-congruent decision making.22,23 In cancer patients, the use of video-based decision aids to discuss GOC have previously been shown to decrease patient anxiety, increase adherence to treatment, and improve knowledge about treatment.24,25 A meta-analysis of video decisions for GOC conversations found they increased advance care planning (ACP) related knowledge and decreased preferences for aggressive end of life care. 26 Studies focused on various surgical populations found video-based decision aids for GOC conversations reduced decisional conflict and uncertainty, increased patient knowledge, and improved patient decision-making but found no impact on decisions to pursue surgical vs noninvasive treatment.27-29
Video aids have also been found to beneficial when utilized for code status discussions — one component of GOC which addresses the use of life-sustaining treatments such as CPR and intubation. Multiple studies have found that video-based interventions have been found acceptable to patients and family members, reduce decisional conflict, and improve knowledge about code status among advanced cancer patients, 30 ICU patients, 31 and medical ward patients. 32 One systematic review and meta-analysis of communication interventions discussing code status found video interventions resulted in a greater decrease in patients’ preference for CPR, but few studies noted decreased trust and perceptions of reduced physician compassion with the use of a video aid. 33
Although studies have investigated various decision aids for GOC and code status discussions and ACP across multiple medical populations and age ranges,26,33-39 there is limited data regarding the utility of video-based decision aids specifically in older adult populations. This systematic review aims to examine the healthcare settings in which video aids have been used for GOC or code status conversations and to investigate their impact on these discussions among older adults.
Methods
Search Methodology and Study Selection
The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines were followed. 40 The protocol was registered with the international prospective register of systematic reviews (PROSPERO CRD420251021664). In January 2025, a trained Medical Librarian (LO), conducted a systematic search of literature on Older Adult GOC/Care Planning Visual Discussion Aids. Using Medline (OVID Platform) as the primary database, the topic was explored using both controlled (in database) and natural languages and determined to have three distinct concepts: Geriatric Patients/Geriatrics 1), Medical Visual Discussion Aids 2), and GOC/Care Planning 3).
MeSH terms were identified, and keywords were gathered and searched using the title, abstract, and keyword fields within the Medline OVID database with the English Language filter. Six databases were used: Medline OVID (primary), Embase, Web of Science, CINAHL, PsychINFO, and Cochrane. Final search results were de-duplicated in EndNote 21, manually refined, and delivered to the PI as an RIS text file along with the corresponding database search strategies on April 1st 2025. All identified citations were uploaded into Rayyan and screened independently by study title and abstract and then full text using inclusion criteria by two reviewers (AK, MF) and a third (SM) providing consensus for any disagreements.
Inclusion Criteria
We included studies which used a video-based aid to impact decision making about GOC or code status in primarily older adult populations (≥65) or their surrogate decision makers in either inpatient or outpatient healthcare settings in the US. We excluded studies conducted in a nursing home or community setting or if they were conducted outside of the US. We also excluded studies in which video conversation aids were not the primary intervention (such as being solely used to supplement palliative care educator-led GOC conversation). We excluded videos which did not have video content related to end-of-life care, GOC, or code status. We considered both experimental and quasi-experimental study designs including randomized controlled trials, non-randomized controlled trials, and before and after studies.
Variable Collection
Study Characteristics
Quality Assessment
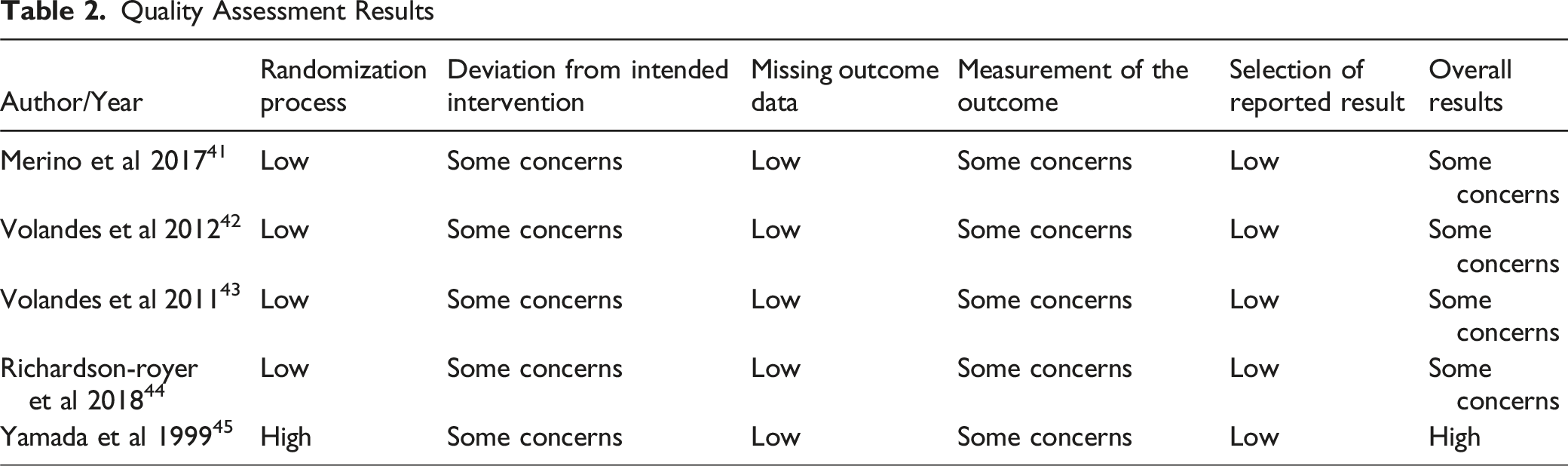
Quality assessment was performed on all included publications using the Cochrane Risk of Bias tool 45 for assessing the quality of randomized, interventional studies. This tool consists of the following domains through which bias may be introduced: (1) randomization process; (2) deviations from intended interventions; (3) missing outcome data; (4) measurement of the outcome; (5) selection of reported result. There are three possible risk-of-bias judgements: low risk, some concerns, or high risk of bias. Study quality assessment was completed independently by two reviewers (AK and MF) and disagreements were adjudicated by a third reviewer (SM). Heterogeneity could not be assessed due to limited number of studies.
Results
Study Characteristics
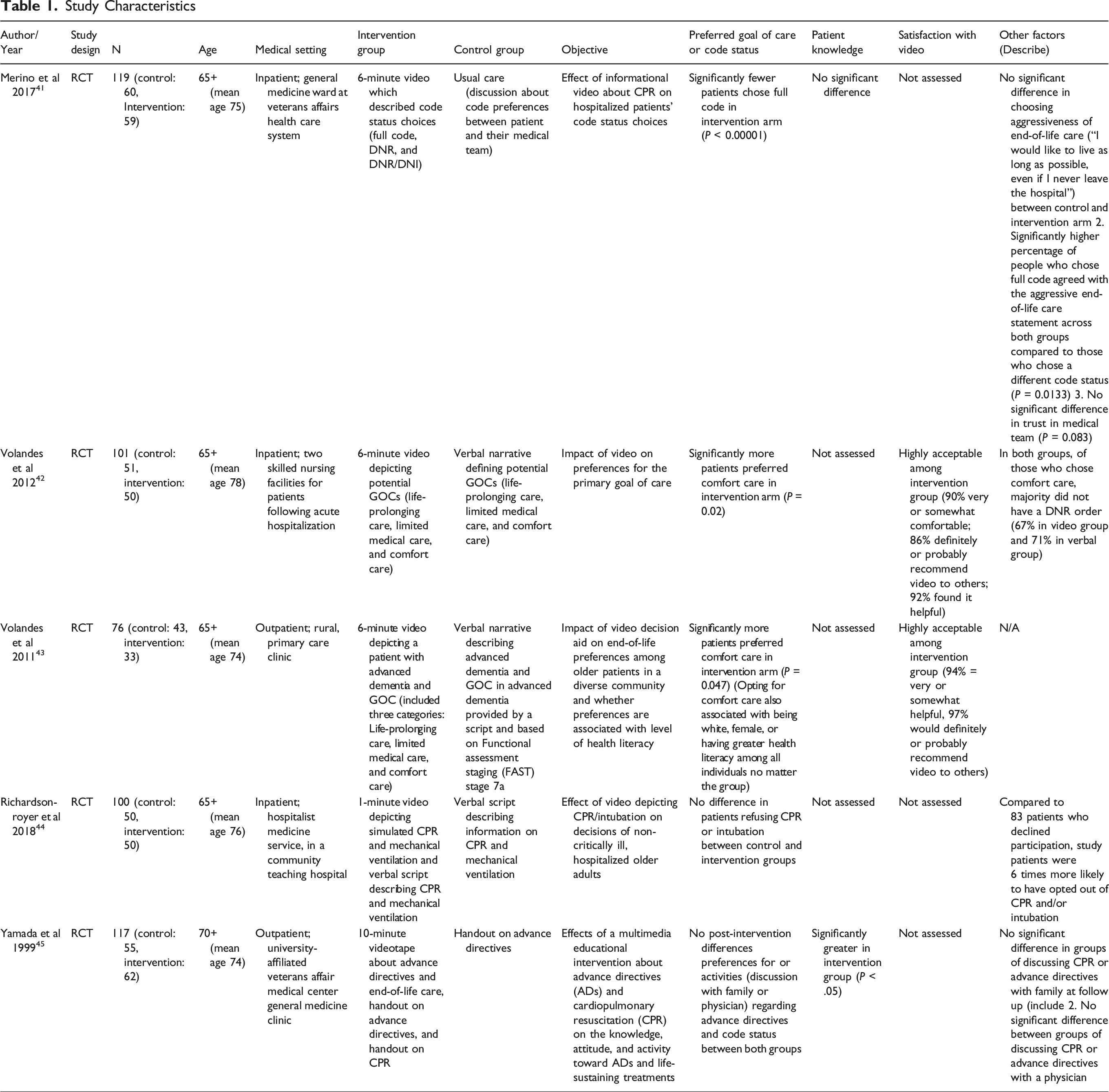
After deduplication, our search revealed 4438 studies. After reviewing abstracts, we excluded 4431 articles. Seven studies underwent full review, and we further excluded two studies. Five studies were included in the final analysis (Figure 1). Among them, 2 studies41,43 were conducted in outpatient settings and 3 studies42,44,46 in inpatient settings (Table 1). All studies were randomized controlled trials and study sample sizes ranged from 76 to 119 patients per trial. Two studies42,43 were conducted with Veteran Affairs hospital patients, one study
41
focused on patients in a rural setting, and the remaining two studies44,46 did not focus on a specific older adult patient population. All studies included patients on general medicine or medical hospitalist services. Most studies41-44 did not have exclusion criteria based on illness. One study
46
excluded patients receiving critical care on admission and two studies41,44 assessed for and excluded patients based on cognitive impairment. Study selection and screening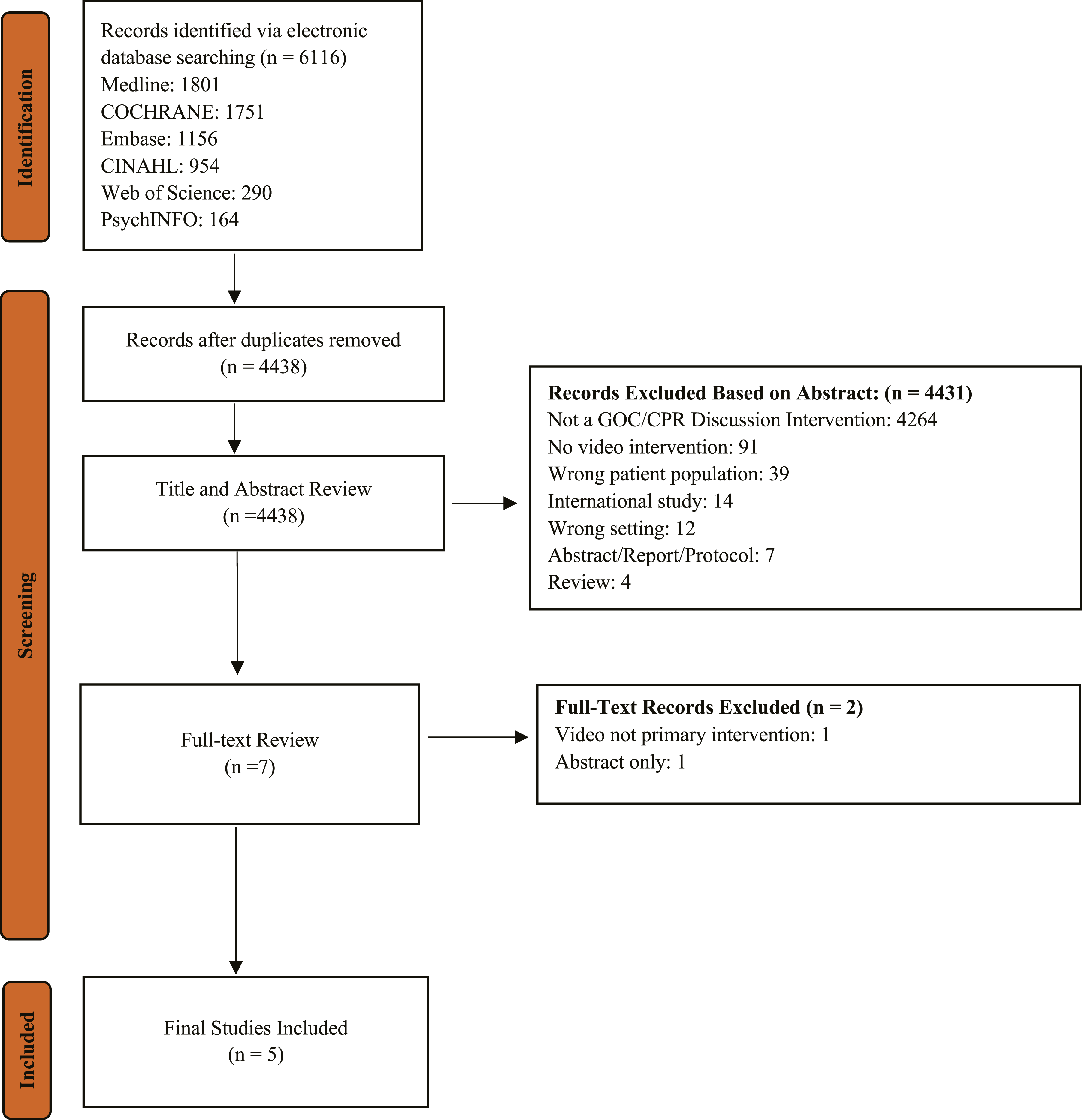
Among the included studies, video length, content, and format varied (Table 1), consistent with other video-based decision aids in the literature. Video content largely described code status choices,42,46 levels of medical care (life-prolonging, limited, and comfort care),41,44 or advance directives. 43 The shortest video used was 1 minute and showed simulated CPR and mechanical intervention while the longest was 10 minutes and explained advance directives and end-of-life care.43,46 Only one study, conducted in an outpatient setting, used a video depicting a hypothetical scenario rather than one tailored to the patient’s specific clinical condition. 41 Three studies41,42,44 described a multidisciplinary approach to the creation of their videos, and none discussed adherence to a specific patient decision aid standard.
All studies used questionnaires or interviews for data collection and evaluated patient preference for GOC or code status (Table 1). Additionally, 2 studies42,43 determined post-intervention knowledge and 2 studies41,44 investigated satisfaction with the intervention video. Individual studies also investigated outcomes of preference alignment with current GOC, 44 perceived trust in medical team, 42 and discussion with a physician regarding GOC preferences. 43 Only one study 41 investigated whether end-of-life care preferences were associated with level of health literacy.
Quality Assessment
Quality Assessment Results
Goals of Care or Code Status Preference
Among inpatient settings, two studies42,44 utilized ∼6-minute video interventions and found significant differences in code status and GOC choices between control and intervention groups. Patients in the intervention arm were significantly more likely to prefer comfort care than those in the control arm (80% for intervention vs 57% for control, P = 0.02) 44 or significantly less likely to choose full code (37% for intervention vs 71% for control, P < 0.0001). 42 One study correlated stated preference with code status documentation in patient charts. Preferences did not always align with documented GOC — only 33% of patients who chose comfort care in the intervention group and 29% of patients who chose comfort care in the verbal group had a documented Do Not Resuscitate (DNR). 44
In contrast, another inpatient study 46 utilized a shorter video (1-minute) with non-terminally ill patients not receiving critical care. They compared the video intervention describing CPR to a control group which received a standardized verbal script describing CPR and found no significant difference in CPR or intubation refusal between the two groups (22% for intervention vs 22% for control). Study participants were 6 times more likely to have opted out of CPR or intubation in comparison to 83 patients who declined participation after meeting eligibility criteria and received no standardized information. Those who declined participation may have been less willing to engage in discussions about code status and may have been less likely to accept an advance directive. 46
In one outpatient study, patients were shown a video describing advanced dementia and three levels of medical treatment. Then, they were asked to choose their GOC in the hypothetical situation they developed advanced dementia and became critically ill. A greater proportion of patients opted for comfort care if they were in the intervention group (91% for intervention vs 72% for control, P = 0.047). 41 However, another outpatient study found no postintervention differences between groups in their preferences for undergoing CPR (75.6% for intervention vs 80.5% for control; OR = 0.75, 95% CI: 0.27, 2.10). 43 Additionally, there were no significant differences in whether patients discussed CPR or advance directives with family members at follow-up (40.0% for intervention vs 27.5% for control; OR = 1.76, 95% CI: 0.70, 4.39) or informed their physician of code status preference immediately postintervention (12.5% for intervention vs 12.8% for control; OR = 0.97, 95% CI: 0.26, 3.66). 43
Patient Knowledge
Only one inpatient study investigated patient knowledge of GOC postintervention. The authors found no significant difference in the percentage of patients who agreed with the statement: “If I choose to avoid resuscitation efforts, I will not receive care” (28% control vs 22% intervention group). 42 In contrast, one outpatient study reported those in the intervention group, compared to the control group, were more likely to correctly estimate their likelihood of being resuscitated and discharged home (62.9% for intervention vs 32% for control, P ≤ 0.05), to know what an advance directive is (87.2% for intervention vs 52.5% for control, P ≤ 0.05), and to correctly identify different procedural aspects of CPR (P ≤ 0.05). Most differences in knowledge were reduced at a 2-to-4-week follow-up postintervention, except for knowledge about advance directives (72.3% for intervention vs 40.0% for control, P ≤ 0.05). 43
Patient Satisfaction and Trust
Two studies in different medical settings investigated patient satisfaction.41,44 The majority of inpatient patients found the video to be highly acceptable with minimal discomfort (10%) from watching and had a substantial likelihood (86%) of recommending the video to other patients. 44 When shown a similar video describing GOC, with the addition of describing advanced dementia, 94% of rural patients in an outpatient setting (95% CI, 80-99) found the video to be helpful and 97% (95% CI, 84-100) had a substantial likelihood of recommending the video to others. 41
Only one study investigated trust in the medical team and found no significant difference between the intervention group (76%) and control group (93%) agreeing with the statement “My doctors and healthcare team want what is best for me” (P = 0.083). 42 In another study, there was no significant postintervention difference between groups in wishing to discuss CPR preference with their physician (68.9% for intervention vs 54.0% for control; OR = 1.88, 95% CI: 0.76, 4.65). 43
Discussion
Based on 5 randomized trials of heterogeneous patients, our review suggests that video-based decision aids may meaningfully enhance GOC discussions in older adults, demonstrating benefit in non-acute inpatient and outpatient medical settings.41,42,44 Video-based decision aids were well received by patients, with studies41,44 reporting high levels of acceptability, comfort with video content, and a strong likelihood of recommending the video to others. However, the degree to which these aids influenced decision making varied and these benefits did not always translate to clinical changes in care preferences or increased discussions with physicians. Additionally, the overall confidence in these results may also be limited due to risk of bias arising from methodological concerns. Therefore, current data should be interpreted as promising but preliminary, supporting the potential value of video-based decision aids. Other systematic reviews investigating video-based decision aids for ACP and GOC discussions among younger adult patient populations similarly found that the videos decreased patient preference for life-sustaining treatment, improved patient knowledge regarding ACP, and increased patient satisfaction with the decision aids.26,33,47
Two studies in our review found that video-based decision aids did not consistently translate into changes in care preferences or increased discussions with physicians regarding code status.43,46 There was also conflicting evidence on the impact of video-based decision aids on improving patient knowledge of end-of-life care.42,43 Although the different findings may be attributable to the variations in video intervention, future studies should explore the impact of video-based decision aids on patient knowledge among older adults. There is a limited body of research on video-based decision aids regarding GOC or CPR for older adult patient populations, as demonstrated by only five studies meeting inclusion criteria. Additionally, no studies have examined the effectiveness of such interventions in the setting of an acute decline in health, such as in injured patients, leaving the impact of video aids in this context unclear.
Video-based decision aids are being increasingly evaluated in clinical studies and have the potential to address multiple gaps in patient education and shared decision-making. They can increase accessibility across literacy levels and deliver standardized, less biased information, enhancing patient agency and engagement in complex decisions.13,22,25 However, the lack of standardization across tools and limited availability of video aids outside of research studies are barriers to incorporating high quality video-based decision aids in clinical care. Deviations from standard protocol and inconsistent quality can make it difficult for physicians and patients to identify reliable decision aids. Standards for patient decision aids, such as the International Patient Decision Aid Standards (IPDAS), 48 exist, though they may not always be applied. Although no standards exist specifically for video-based decision aids, they should align with IPDAS or a comparable framework that outlines criteria to ensure quality and accessibility.
Variations among video conversation aids included the length of the video, the breadth of the alternatives for code status discussed, and the use of real-life vs hypothetical scenarios. Educational videos should ideally be 6 minutes or shorter to optimize engagement and retention, although no data currently defines a minimum length. 49 Additionally, IPDAS criteria recommend that decision aids present all available options, including the choice to forgo treatment. 48 One inpatient study 46 used a short 1-minute video, which may have been engaging due to length, but did not provide an explanation of other code status options (DNR or DNI). This may have limited its effectiveness as a decision aid and possibly contributed to the lack of significant difference in code status preference between intervention and control groups.
Another outpatient study, which found a significant preference for comfort care within the intervention group, used a video with a hypothetical scenario rather than presenting decisions immediately relevant to the patients’ medical context. 41 This approach may be helpful in outpatient settings, where patients have more time and autonomy to make GOC decisions, but may be less applicable in inpatient contexts where patients are often acutely ill and face immediate, complex medical decisions. Hypothetical scenarios may be more tolerable, as they are less likely to provoke emotional distress which may affect decision making. 50 A study of Chinese older adults found that hypothetical scenarios improved understanding of life-sustaining treatment decisions, suggesting potential educational value of these scenarios. 51 However, hypothetical scenarios may not elicit real-world behavior, as individuals overestimate their willingness to seek treatment in a hypothetical situation and have difficulty envisioning hypothetical health states.52,53 Further research is needed to determine whether hypothetical scenarios or real-life formats better support informed GOC decisions. Ultimately, video aids should be brief, include essential decision-making information, and be tailored to specific clinical contexts.
None of the studies in this review offered guidance for implementing the video aid into a clinical workflow, a gap also noted in a previous systematic review of video-based decision aids for ACP.26,41-44,46 Of the included studies, two42,46 provided access to the video aids evaluated, allowing for potential use in practice. Studies conducted by Volandes et al41,44 did not include specific video aids, although the research team maintains a publicly available ACP library with videos 54 for purchase and use in patient care. Future studies should incorporate the video into clinical care, follow patients longitudinally to assess its impact on ACP or clinical outcomes, and document decisions in the medical record to better inform the use of a video-based decision aid in practice. Other, recommended strategies for implementing patient decision aids include involving system-level support such as team training, leadership buy-in, and standardized delivery processes. 55
Limitations
This review is limited by the small number of included studies, reflecting the lack of research on video decision aids for GOC and CPR discussions in older adults. Additionally, all studies were at some concern for or a high risk of bias, limiting the strength of conclusions due to lack of high-quality evidence. Variability in type, length, and content of video conversations and differences in measured outcomes made direct comparisons difficult across all studies and limited generalizability. Given the heterogeneity of studies, a meta-analysis was unable to be performed. Most studies focused on stable older adults with varying prognoses, making it difficult to investigate effectiveness of video decision aids in acute care settings.
Conclusion
GOC discussions are important in older adults and video-based decision aids show promise as a method to improve alignment of patient preferences and increase patient knowledge. However, current evidence is limited to a small number of heterogenous studies with interventions having thus far only been applied to outpatient settings, non-acute inpatient settings, and nursing homes in community settings. While findings are encouraging, investigations of video-based decision aids for GOC conversations in older adults after an acute decline in health (eg, in older adult trauma populations) are needed.
Supplemental Material
Supplemental material - Video Conversation Aids to Assist in Goals-of-Care Discussions with Older Adults in a Medical Setting: A Systematic Review
Supplemental material for Video Conversation Aids to Assist in Goals-of-Care Discussions with Older Adults in a Medical Setting: A Systematic Review by Ashna S. Karpe, BA, Mokunfayo O. Fajemisin, MD, Stephanie Martinez Ugarte, MD, Lara Ouellette MLS, Martin L. Blakely, MD, MS, Gina H. Khraish, MD, Shreyans V. Sanghvi, DO, Min J. Kwak, MD, MS, Jessica L. Lee, MD, MS, Lillian S. Kao, MD, MS, Thaddeus J. Puzio, MD, MS in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental material - Video Conversation Aids to Assist in Goals-of-Care Discussions with Older Adults in a Medical Setting: A Systematic Review
Supplemental material for Video Conversation Aids to Assist in Goals-of-Care Discussions with Older Adults in a Medical Setting: A Systematic Review by Ashna S. Karpe, BA, Mokunfayo O. Fajemisin, MD, Stephanie Martinez Ugarte, MD, Lara Ouellette MLS, Martin L. Blakely, MD, MS, Gina H. Khraish, MD, Shreyans V. Sanghvi, DO, Min J. Kwak, MD, MS, Jessica L. Lee, MD, MS, Lillian S. Kao, MD, MS, Thaddeus J. Puzio, MD, MS in American Journal of Hospice and Palliative Medicine®
Footnotes
Ethical Considerations
Ethical approval was not required due to nature of systematic review.
Author Contributions
Conception and Study Design: TJP, ASK
Literature Review: ASK, LO, TJP, MOF
Data Acquisition: ASK, LO, MOF, SMU
Data Analysis and Interpretation: ASK, TJP
Drafting of the manuscript: ASK, TJP, MOF
Critical Revision: ASK, MOF, SMU, LO, MLB, GK, SS, MJK, JLL, LSK, TJP
The corresponding author affirms they have listed everyone who contributed significantly to this work.
The authors have no other contributions to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.