
Abstract
Background
Although previous research has highlighted the protective effect of social support in caregiving contexts, further investigation is needed to understand its complex roles in modifying and explaining the impact of caregiver stressors. This cross-sectional study assessed family caregivers’ social support, digital literacy, and caregiving-related stressors, examining their relationships and impact on mental health outcomes (anxiety and depressive symptoms). Specifically, we investigated (1) whether digital literacy interacted with stressors to influence caregivers’ perceived social support and (2) whether social support mediates the relationship between caregiver stressors and mental health.
Methods
Data were collected from 308 caregivers of people living with dementia receiving hospice care using structured assessments, including validated measures of social support, digital literacy, anxiety, depressive symptoms, and key sociodemographic characteristics.
Results
The direct and total effects of caregiver stressors on mental health outcomes were statistically significant, whereas the indirect effects mediated by social support were not. Although tangible support was individually associated with both outcomes, the overall mediating effect of social support was not accounted for by either emotional/informational or tangible support alone. The moderating effect of digital literacy was also not statistically significant.
Conclusions
The association between caregiver stressors and mental health appears to be more directly driven than mediated by social support. The absence of significant indirect or moderating effects highlights the complexity of these relationships and underscores the need for future research to explore additional pathways, contextual influences, and conditions under which aspects of social support or digital literacy may exert greater impact.
Introduction
Over 55 million people live with dementia, and approximately 10 million new cases are diagnosed annually. 1 As dementia progresses, many caregivers in the community—typically family members and friends—become involved in assisting the person living with dementia in completing activities of daily living, such as eating, dressing, and maintaining hygiene. Increasingly, many people living with dementia (PLWD) receive hospice care at the end of life, 2 reflecting growing awareness of the benefits of hospice care for PLWD, such as managing complex symptoms in the terminal stage of the illness. 3 In the United States, community-based hospice care relies heavily on caregivers, who face greater risks of psychological distress and mental health decline than the general population.4,5
Caregiving can be rewarding yet stressful for some caregivers, especially when they lack adequate social support. Social support is widely recognized as a crucial factor in easing caregiver burden and reducing the risk of adverse mental health outcomes.6,7 In this study, social support is conceptualized as the interpersonal and structural engagements that offer emotional, informational, and tangible assistance to caregivers of PLWD receiving hospice care. 8 Emotional/informational support involves having people with whom caregivers can share their problems and obtain information to manage challenges, whereas tangible support refers to perceived physical assistance from others.9,10 Despite its importance, many caregivers often struggle to access consistent social support because of barriers such as limited time, financial constraints, and social isolation, especially when they cannot leave their care responsibilities unattended.11,12
Technology, including computers and mobile devices, can help reduce barriers to social support. This is particularly likely to be the case for caregivers of PLWD receiving hospice care, because they often encounter time constraints, transportation difficulties, and limited external assistance in accessing social support through more traditional in-person or local community-based channels. 12 Although technology-based interventions for caregivers are becoming more common, a digital divide persists, especially among older caregivers of PLWD. 13 To better understand this issue, researchers consider the sociocultural contexts of technology users, including their existing experience with technology and their digital health literacy, as well as environmental infrastructure such as broadband access and public technology resources. 14
Digital literacy, defined as the effective use and evaluation of technology, has emerged as an important factor influencing how people engage with technology in health and caregiving contexts.15-17 As caregiving increasingly relies on digital platforms for communication, care coordination, and information seeking, digital literacy may shape how caregivers access and benefit from social support resources.11,18 Yet, a comprehensive understanding of how digital literacy, mental health, and social support are interrelated is lacking. Therefore, further research is needed to examine these complex relationships across varied caregiving contexts and different disease types. 19
This study aimed to address this gap by examining the relationships among caregiving stressors, social support, digital literacy, and mental health among caregivers of PLWD receiving hospice services. We posited that caregiving stressors may influence caregivers’ mental outcomes both directly and indirectly through social support. 20 Social support functions as a key coping resource that may also moderate these associations by shaping caregivers’ ability to seek and utilize support. Accordingly, we hypothesized that (a) greater caregiving stressors would be associated with poorer caregiver mental health outcomes, (b) digital literacy would moderate the association between caregiving stressors and social support, and (c) social support would mediate the relationship between caregiving stressors and caregivers’ mental health outcomes, including anxiety and depressive symptoms. Specifically, significant interaction terms would indicate that the relationship between caregiving stressors and social support varies depending on levels of digital literacy.
Methods
Settings and Participants
For this cross-sectional study, 308 participants were recruited between September 2022 and November 2024. The parent study was a 5-year randomized clinical trial, Supporting Family Caregivers of Persons with Dementia (ClinicalTrial.gov ID NCT05336344; PI: Demiris), in which participants were caregivers of PLWD receiving hospice care. Study participants were randomly assigned to a group receiving standard hospice care with the addition of ‘friendly video-calls’ providing active listening sessions or a group receiving standard hospice care with the addition of a cognitive behavioral intervention. The data utilized in this study were derived from baseline assessments before exposure to any interventions. Potential participants were identified through referrals from local hospice agencies. Eligible individuals were 18 years of age or older and identified as caregivers of PLWD receiving hospice care. After electronic written consent was provided, participants provided demographic data and completed baseline surveys via REDCap (Research Electronic Data Capture). All study procedures were approved by the University of Pennsylvania Institutional Review Board (IRB Protocol #856882).
Measurements
Demographic Characteristics and Stressors
We collected information on participants’ age, biological gender, education level, race/ethnicity, and marital status. In addition, each caregiver’s stressors were captured individually based on the criteria provided below, and these stressors were summed to provide a total stressor count. By examining each stressor independently, we could assess its unique impact, while the total count of stressors provided insight into the overall burden experienced by caregivers. These individual stressors were determined using the following criteria: (1) Duration of Care: Caregivers had provided care for more than 1 month; (2) Time Commitment: They spent more than 20 h per week caring for their PLWD; (3) Financial Burden: They incurred out-of-pocket expenses for services or material in the past 12 months; (4) Employment Status: They were currently employed; and (5) Geographical Distance: They lived remotely from the care recipient. Additionally, we included as a potential stressor (6) Work-life Impact: They had taken sick leave or vacation time for caregiving responsibilities.
Caregiver Mental Health Outcomes
Anxiety
Symptoms of anxiety were measured by the Generalized Anxiety Disorder 7-item scale (GAD-7; α = 0.92).21,22 This self-report questionnaire consists of 7 items that measure the frequency of general anxiety symptoms experienced over the past 2 weeks. Each item is rated on a 4-point Likert-type scale that ranges from 0 (“not at all”) to 3 (“nearly every day”). The possible range of score is 0 to 21, with a score of 10 or higher indicating clinically significant levels of anxiety.
Depressive Symptoms
Depressive symptoms were assessed using the Patient Health Questionnaire– 9 (PHQ – 9), a widely tool designed for screening depression (α = 0.84). 23 This self-report questionnaire consists of 9 items that measure the frequency of depressive symptoms experienced over the past 2 weeks. ” Each item is rated on a 4-point Likert-type scale, ranging from 0 (“not at all”) to 3 (“nearly every day”). The possible score ranges from 0 to 27, with a score of 10 or higher indicating clinically significant levels of depressive symptoms.
Social Support
Social support was measured by the Medical Outcomes Study Social Support Survey (MOS-SSS). 8 This well-validated measurement tool (α = 0.81) was utilized to evaluate perceived support across four domains, including emotional/informational, tangible, affection, and positive interaction. 8 Two key subscales of the MOS-SSS, emotional/informational support and tangible support, which are essential in the context of mental health and digital literacy, were used in this study. Participants rated each item on a 5-point Likert-type scale that ranged from 1 (“never”) to 5 (“always”). Higher scores indicate greater levels of social support, and the total score for each dimension is calculated by averaging the scores for the items in that dimension.
Digital Literacy
Digital literacy was measured by an established scale called the Functional Assessment of Comfort Employing Technology Scale (FACETS). 24 With the developer’s permission, we modified the scale to evaluate an individual’s comfort and proficiency with technology across various aspects of daily life. Our modifications included removing 2 questions from the original 10-item FACETS questionnaire, resulting in a more focused 8-item assessment. The original FACETS contained response options ranging from 0 (“never”) to 5 (“daily”), with higher scores indicating a greater frequency of technology use (α = 0.90). 24 The survey responses were combined for an overall score ranging from 0 to 40. Our modified version maintained the same response format and questionnaire structure while streamlining the assessment to better address the specific technological interactions relevant to our target population. The digital literacy survey was introduced to the baseline survey in July 2024; therefore, only participants who enrolled in the study after that date had their digital literacy level assessed. Analyses involving this variable were conducted on this subsample.
Statistical Analysis
We first computed descriptive statistics for the demographic characteristics of 308 caregivers of PLWD who enrolled in the ongoing clinical trial. Along with demographic characteristics, the mean, frequency, and standard deviation of the GAD-7, 21 the PHQ-9, 23 the MOS-SSS, 8 and the FACET 24 were analyzed. The total stressors count is a continuous variable, allowing for the analysis of both individual stressors and their cumulative impact. The mean, minimum, and maximum stressor counts were calculated to provide an overview of the distribution of stressors among caregivers.
Descriptive analyses were conducted to summarize participant characteristics, including age, gender, education, marital status, race, and scores of the PHQ-9, GAD-7, and FACETS. An a priori power analysis was not conducted for the original data collection, as this study involved secondary analysis of an existing dataset. We used R statistical software (version 4.2.0; R Core Team, 2024) for all analyses. The following packages were used for data management, statistical modelling, and visualization: tidyverse* 25 for data wrangling and plotting, laavan 26 for mediation and moderation analysis.
We examined moderation and mediation using a regression-based approach (hypotheses and rationale are detailed in the introduction; see also Figure 1). For the moderation model, we tested whether digital literacy modified the association between caregiving stressors and social support. Social support was regressed on stressors, digital literacy, and the interaction of stressors and digital literacy, while controlling for demographic characteristics, including age, gender, race, education, and marital status. The significance level for all analyses was set at α = 0.05. The moderation and mediation analysis of digital literacy and social support Note. The dash line suggests the moderation analysis sought to determine if digital literacy moderates the relationship between stressors and social support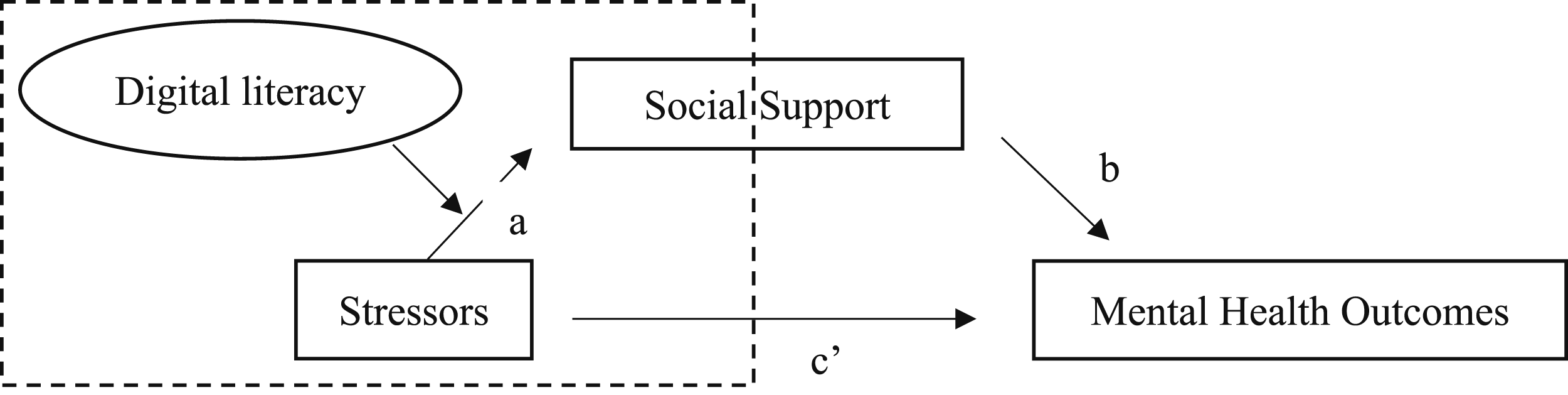
For the mediation model, we evaluated whether social support explained the association between the number of stressors and mental health outcomes. We estimated separate linear regression models for the mediator (social support) and for each outcome (depressive and anxiety symptoms), adjusting for the same covariates. To interpret the results of our mediation analysis, we reported the direct effect of stressors on each outcome (the effect not mediated by social support) and the indirect effect (the portion of the effect explained by social support). By estimating both effects, we can better understand the mechanisms linking caregiving stressors, social support, and mental health outcomes. The total effect (c’) represents the direct relationship between stressors and each outcome without considering social support. Bootstrapping methods were applied to estimate the confidence interval for the indirect effects.
Results
Descriptive Statistics
Characteristics of Participants
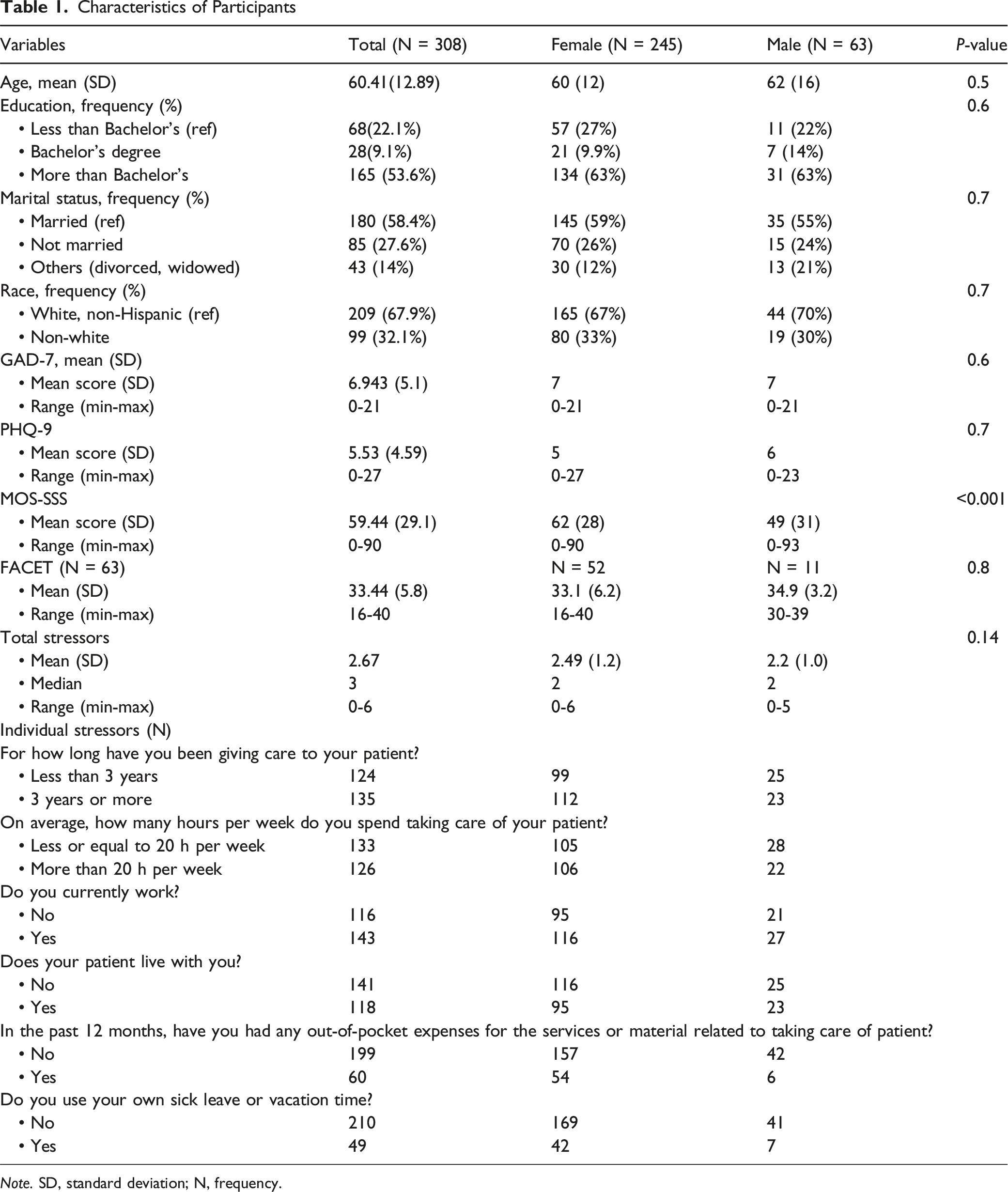
Note. SD, standard deviation; N, frequency.
Pearson Correlation Coefficients Among Study Variables
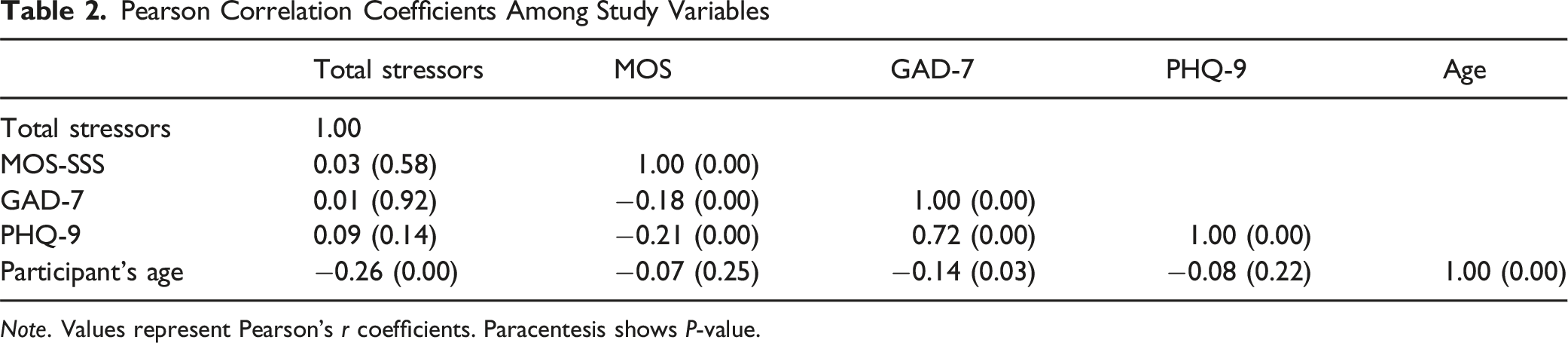
Note. Values represent Pearson’s r coefficients. Paracentesis shows P-value.
Moderation Analysis
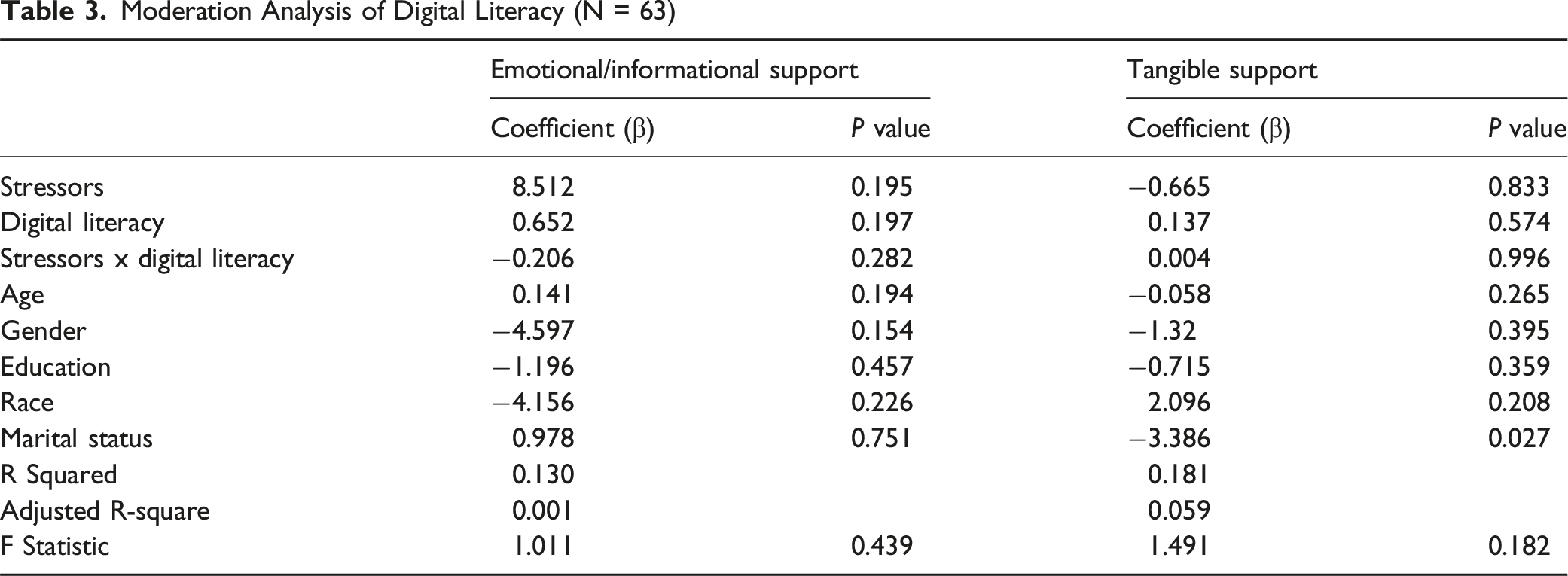
Moderation Analysis of Digital Literacy (N = 63)
Mediation Analysis
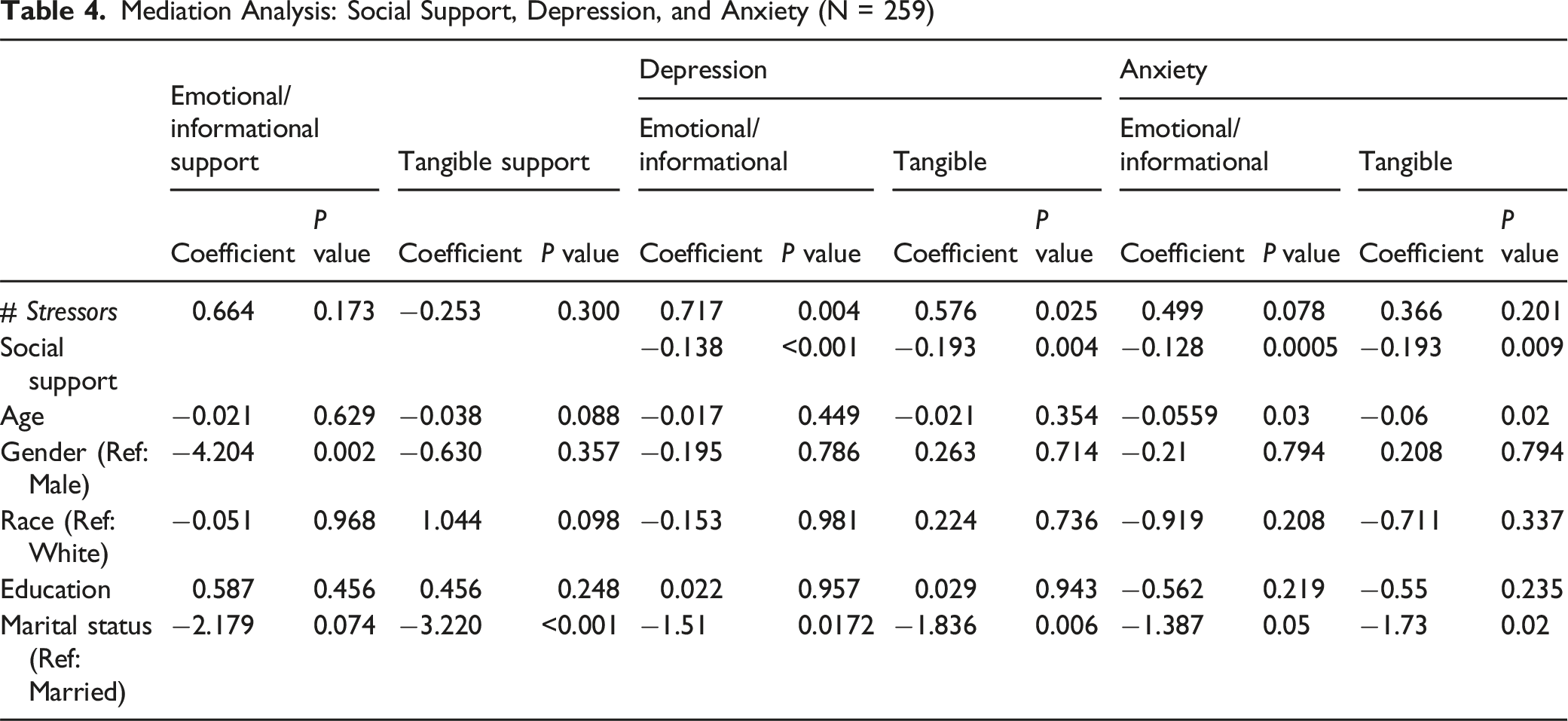
Mediation Analysis: Social Support, Depression, and Anxiety (N = 259)
Effects of Stressors: Depression and Anxiety (N = 259)
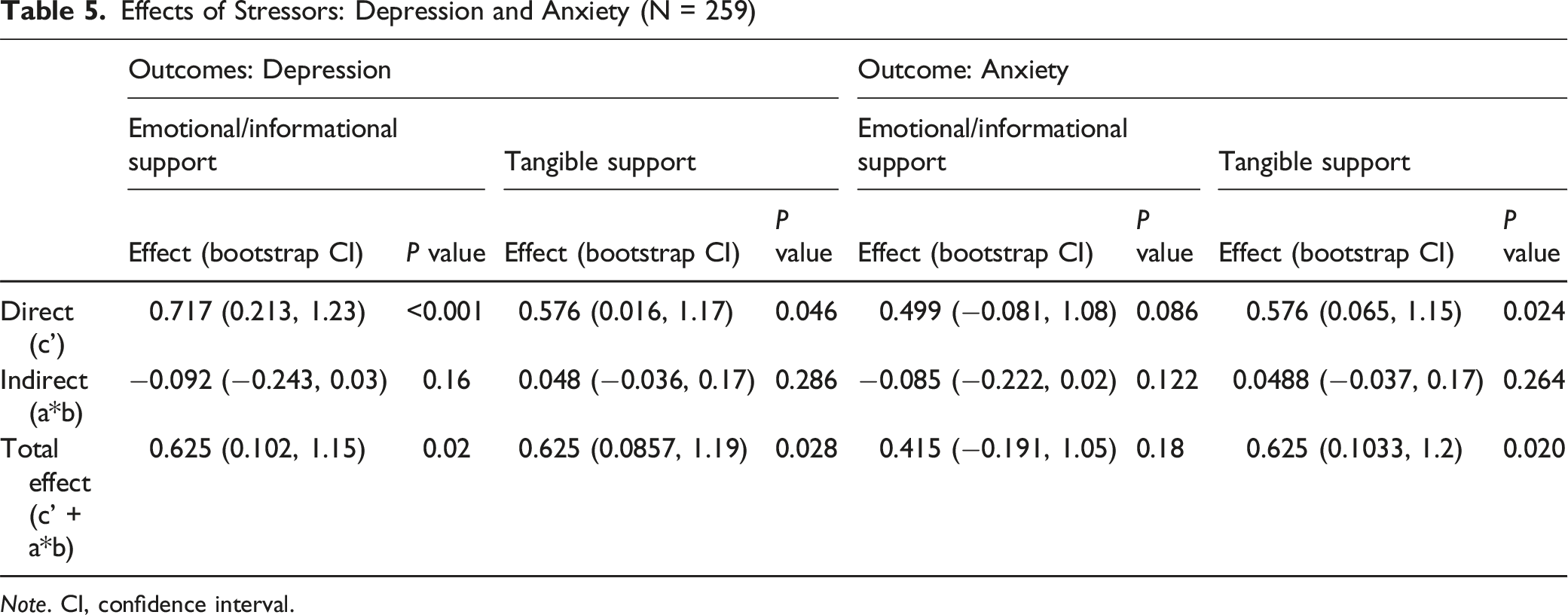
Note. CI, confidence interval.
Depressive Symptoms
A mediation model showed the relationship between stressors and emotional/informational and tangible social support. The total effect (c’ + a*b) showed the overall relationship between stressors and depression, which was statistically significant (P < 0.05). Both emotional/informational and tangible support showed statistical significance (β = 0.625, P = <0.02, β = 0.625, P = 0.028, respectively).
The direct effects of emotional/informational and tangible support were statistically significant (β = 0.717, P = <0.001, β = 0.576, P = 0.046, respectively). The indirect effect (path a*b) showed the potential mediating effect of social support on the relationship between stressors and depression. However, the indirect effect of emotional/informational and tangible support was not statistically significant (β = −0.092, P = <0.16, β = 0.048, P = 0.286, respectively), indicating that social support does not significantly mediate the relationship in this model. Interestingly, within the indirect path (a*b path), both ‘a’ paths for informational/emotional and tangible supports were both statistically insignificant (β = 0.664, P = 0.17; β = −0.253, P = 0.3, respectively), while both ‘b’ paths of informational/emotional and tangible support were statistically significant (β = −0.138, P = 0.001; β = −0.193, P = 0.004, respectively).
Anxiety
We found that the tangible support was significantly associated with anxiety in both direct and total effect (β = 0.576, P = 0.024; β = 0.625, P = 0.02, respectively). Although the ‘a’ path —representing the relationship between the stressors and informational/emotional and tangible support— was not statistical significance, indicating the relationship between social support and anxiety (‘b’ path) demonstrated a significant negative influence on both informational/emotional and tangible support (β = −0.128, P = 0.0005; β = −0.193, P = 0.009, respectively).
Discussion
This study examined the relationships among caregiver stressors, social support, digital literacy, and mental health in the context of hospice care for PLWD. Our findings indicate that both direct and total effects of caregivers’ stressors on anxiety and depressive symptoms were statistically significant, whereas the indirect effects through social support were not. This suggests that the association between stressors and mental health outcomes may be driven more by a direct pathway rather than through the mediating role of social support. While the direct path coefficient (path b) for tangible support was significantly associated with both depressive symptoms and anxiety, the overall indirect effects of both emotional/informational and tangible support were insignificant. These results underscore the complexity of these relationships and suggest that other contextual factors may also contribute to caregivers’ mental health.
Although the moderating effect of digital literacy was not statistically significant, its broader social relevance remains important. Caregivers of PLWD receiving hospice services often face time and resource constraints that limit their ability to engage with traditional support networks. In this context, digital literacy may still influence caregivers’ ability to access and effectively use supportive resources, especially when care involves digital tools or online platforms. 26 Given that this study used cross-sectional secondary data, longitudinal research is needed to establish causal relationships and, if indicated, inform the design of programs that improve caregivers’ digital literacy skills. Further research also needs to explore additional pathways or conditions under which aspects of social support, such as informational support, may play a more significant role.
To our knowledge, this is the first study to examine both social support and digital literacy level among caregivers in a hospice context. By highlighting the nuanced ways social support relates to anxiety and depression, the study offers valuable insights that can inform the development of more tailored and accessible interventions to support caregiver well-being.
This study has several limitations. First, it used cross-sectional data, which limits our ability to assess the long-term effects of caregiving. Longitudinal studies are needed to better understand how caregiving responsibilities impact social support and mental health over time. Second, the FACET instrument may not fully capture the digital literacy level within our specific population. This instrument was originally designed for use in the general population, where the context and requirements for digital literacy may differ significantly. Additionally, the relatively small sample size and low population diversity of the study may limit the generalizability of the findings.
Conclusions
This study found that social support did not significantly mediate the impact of caregiver stressors on mental health outcomes, nor did digital literacy moderate this relationship. These results suggest that interventions focusing solely on strengthening social support or digital literacy may be insufficient to protect caregivers. Given the strong direct effect of stressors, future studies are needed to clarify whether targeting these stressors directly could complement or enhance the impact of existing support-focused interventions.
Footnotes
Acknowledgments
The authors gratefully acknowledge Dr Lepkowsky for granting permission to use the FACETS instrument.
Author Contributions
Conceptualization: H.C., G.D.,; Methodology: H.C., L.H., G.D.; Formal Analysis: H.C., L.H.; Writing – original draft: H.C.; Writing-reviewing & editing: H.C., L.H., K.H., J.S.S., N.A.H., K.W., G.D.; Supervision: J.S.S., N.A.H., G.D.; Funding acquisition: K.W., D.B.O., G.D. All authors approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author has received the Carol Ware Scholarship. Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R01AG069936 (PI Demiris). Research reported in this publication was supported by the National Institute Of Nursing Research of the National Institutes of Health under Award Number T32NR009356. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.