
Abstract
Purpose
Communities in Canada have created targeted hospice palliative care strategies such as facility-based hospices for the homeless (H4H) to promote equitable access to care. To ensure the sustainability of H4H programs, there is a need to prevent and mitigate burnout and enhance workplace wellbeing. The objectives for this study were to, (1) develop a better understanding of H4H staff and volunteers’ experiences of stress and wellbeing; and (2) explore opportunities for additional resources to support workplace wellbeing.
Methods
We developed and administered an anonymous 26-item survey to 104 providers including both staff (eg, nurses, administrators) and volunteers at a facility-based H4H in Ontario. The survey gathered open and closed-ended data on sociodemographic information, compassion satisfaction, and H4H stories of workplace experiences.
Findings
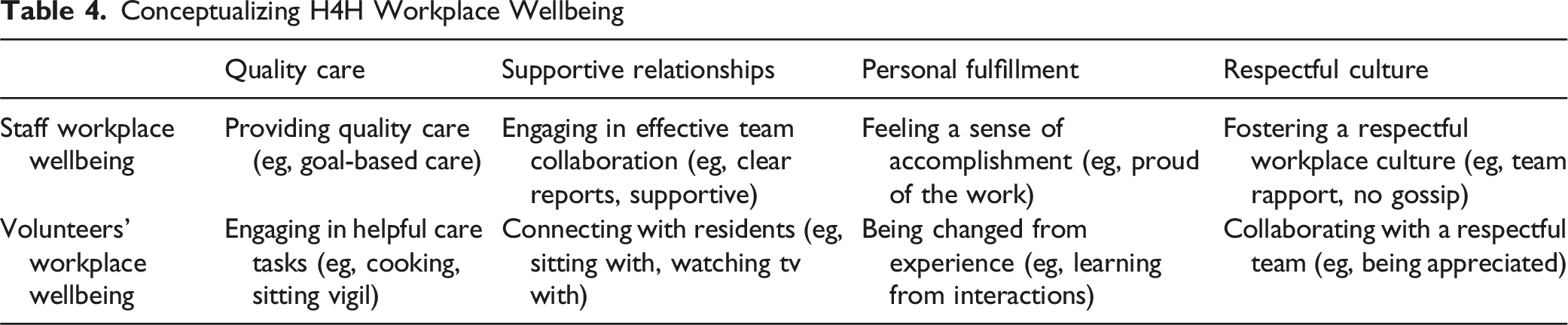
The response rate was 56% (n = 58). Most respondents had high compassion satisfaction. However, multiple factors causing stress at work across the socio-ecological model were discussed. Requests for additional resources to foster workplace wellbeing included educational, process-related, spiritual/psychological, and social supports. Respondents storied that positive workplace wellbeing includes being able to provide quality care, and having supportive relationships, personal fulfillment, and a respectful culture within the workplace.
Conclusion
Provider participants were satisfied with their ability to be effective carers, yet chronic multi-level work-related stressors can erode a sense of meaning in H4H work. A multi-faceted evidence-based approach to supporting workplace wellbeing is needed in H4H settings. Research has shown that mindfulness could be an effective strategy, as it can decrease burnout and promote coping, team connection, and anti-oppressive care.
Keywords
Introduction
Several communities in Canada have created targeted hospice palliative care strategies, such as facility-based specialized hospices for the homeless (H4H), to promote equitable access to care for the 235 000 people experiencing homelessness in any given year.1-5 H4H organizations provide services within home-like facilities where clients receive palliative care often for the last 30 days of their life. This differs from other specialized hospice services that deliver care in the community. H4H organizations aim to improve quality of life by attending to symptoms of illness and psychosocial suffering 6 and use trauma-informed and anti-oppression approaches to care. 5
Sustaining and growing equitable access to H4H care hinges on staff and volunteers having work conditions that support their wellbeing and protects their capacity to deliver care.7,8 However, multiple compounding work-related stressors are thought to put providers working at the intersection of death and homelessness at high risk for burnout. 9 Burnout results from “extreme occupational stress” (9, p. 1365) and presents as as emotional exhaustion, cynicism, and/or feeling inefficient in job-related roles.7,10 It is estimated that the prevalence of burnout in palliative care nurses is between 24%-39%9,11 and largely associated with factors 10 such as heavy workloads; workplace harassment; tense relationships with colleagues; and contact with death.7,10,12 To account for the H4H context of caring for structurally vulnerable people, we also examined literature on burnout in homeless shelter workers, which has a similar estimated prevalence of 30%-40% 13 due to exposure to violent deaths, vicarious trauma, and witnessing the realities of structural oppression.4,13
Furthermore, experiences of burnout are often stratified across diverse identities. Men are more likely than women to exhibit cynicism.11,14 Women tend to have higher levels of exhaustion than men.14,15 Additionally, younger people are at a higher risk for cynicism,11,16 and non-white individuals and members of 2SLGBTQ + communities are more likely to experience exhaustion and feelings of job inefficiency than white and heterosexual individuals. 14 When left unaddressed, burnout often leads to poorer provider wellbeing, compromised care, provider attrition, and decreased organizational and system capacity.8,9,17,18
A factor that protects against burnout and supports providers’ wellbeing at work and at home is compassion satisfaction (ie, the feeling that one is an effective carer).8,19,20 Wellbeing is a multidimensional concept that utilizes a holistic understanding of the relationship between physical, mental, social and spiritual functioning that results in a sense of flourishing. However, this strengths-based conceptualization has received little attention in burnout literature to date. 21 It is known that compassion satisfaction is positively correlated with job satisfaction and employee retention and negatively correlated with burnout. 10 Compassion satisfaction is often increased by leaning on support systems and resources, effective coping strategies (eg, self-compassion), displaying compassion, and seeing the positive impact of one’s work.8,19,20
At this time, little is known about the experience of burnout, compassion satisfaction, or wellbeing in H4H settings, or the factors shaping these phenomena. To sustain H4H programs and enhance workplace wellbeing, there is a need to better understand provider experiences in this context.
Methodology
Research Objectives
Study objectives were to: (1) develop an understanding of H4H staff and volunteers’ experiences of stress and wellbeing; and (2) explore opportunities for additional resources to support workplace wellbeing. Research questions to meet these objectives included: 1. To what extent are H4H staff and volunteers experiencing compassion satisfaction; 2. How do H4H staff and volunteers experience work-related stressors; 3. In what ways can resources support their workplace wellbeing; and 4. How do H4H staff and volunteers envision workplace wellbeing?
Study Design
We developed a cross-sectional, multi-method survey informed by a pragmatic paradigm that incorporated both post-positivist and interpretive knowledge.
22
The Sex- and Gender-based Analysis (SGBA+) framework
23
and socio-ecological model
24
guided our exploration of factors that are thought to influence burnout such as racism, sexism, and workplace harassment (see Image 1).4,7,11,12,14,15 Image 1: Socio-Ecological Model With SGBA + Factors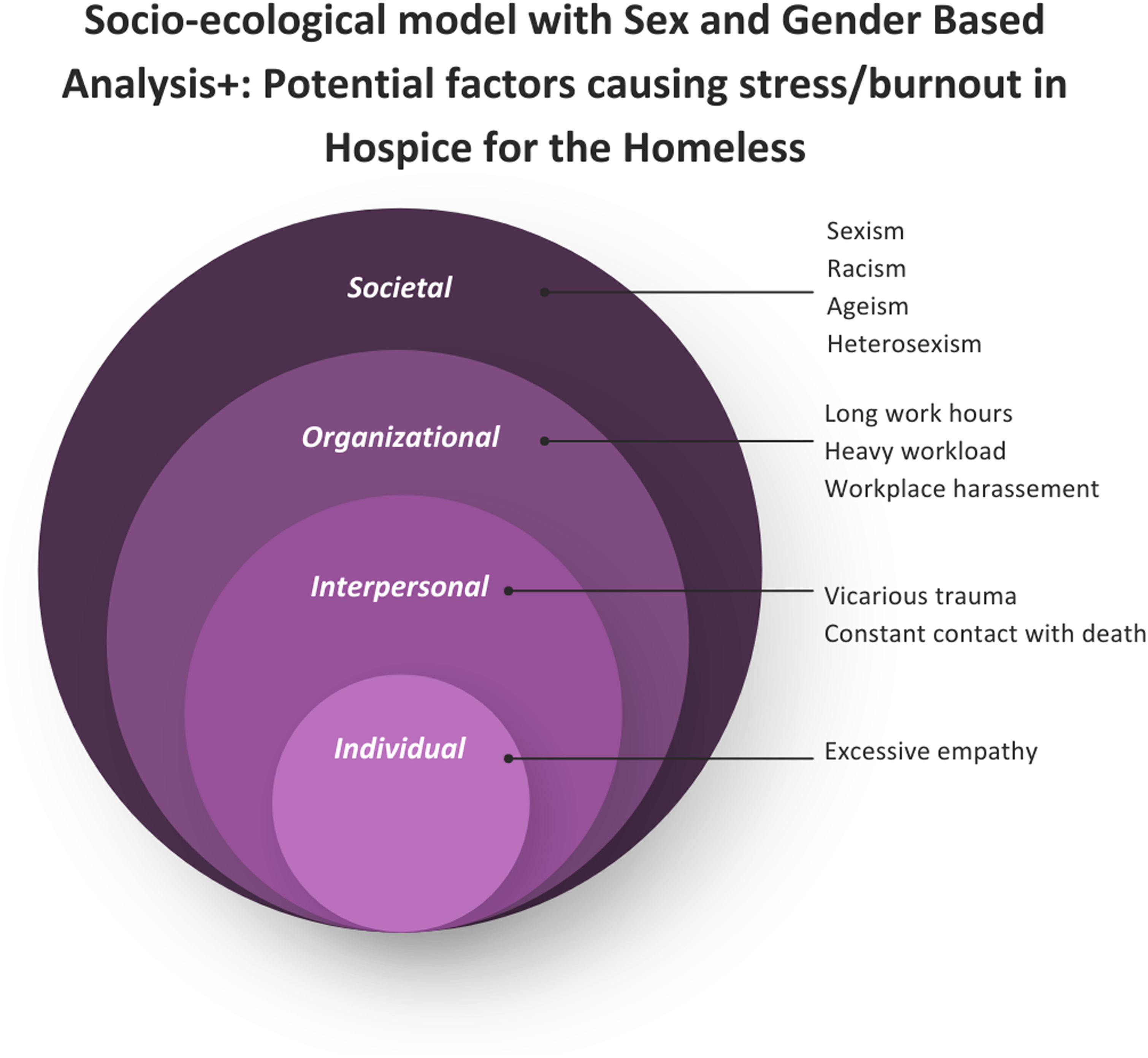
Sampling and Recruitment
The site for this study was a facility-based H4H in Ontario, Canada located in an urban environment with 16 beds and 104 providers, half of which were volunteers. In this hospice, there are several managers and coordinators, several supportive care providers, and one physician, with the largest proportion of staff being nurses and personal support workers (PSWs). There is an approximate provider-to-patient ratio on days and nights of 3:16 with one registered nurse, one registered practical nurse and one PSW. Data on the age, race, and gender of providers was unavailable.
H4H leadership provided the email contacts of current staff and volunteers to support sharing of the voluntary survey participation opportunity. Our research team emailed potential survey respondents a recruitment letter containing a study summary, consent information, and a link to the secure online survey that included radio button consent. Up to two follow-up reminder messages were sent. Participants were offered a $10 CAD gift card for completing the survey.
Data Collection
The online survey, hosted via Qualtrics, contained 26 items (see Supplemental File (1)) and took approximately 20 minutes to complete. Anonymous responses were collected over 2 weeks in May 2024. Duplicate detection, bot detection, and preventing indexing were used. The survey included: (1) closed-ended questions collecting sociodemographic information; (2) self-rating via the compassion satisfaction (CS) subscale from the Professional Quality of Life scale (PROQOL-5) 25 ; and (3) open-ended questions on H4H workplace experiences with one dichotomous question about accessing resources.
The PROQOL-5 CS subscale is a 10-item measure that uses a 5-point frequency scale (1 = never to 5 = very often) to determine the degree to which individuals feel satisfied in being able to do their work well. Items are added for a total score25,26 with a ‘high CS’ cut-off ≥42, ‘moderate CS’ cut-off ≥23, and ‘low CS’ cut-off ≤22. The CS subscale is publicly available and is a valid and reliable tool for use in hospice palliative care settings; the burnout and secondary trauma subscales from PROQOL were excluded due to concerns with their validity and reliability.27,28
Open-ended questions were informed by narrative inquiry and asked people to reflect on their H4H experiences. 29 Respondents were invited to engage in metaphoric reflection and storytelling.29,30 This included asking respondents to create a metaphor that represents their experience of work-related stressors. 30
Data Analysis
Survey responses were analyzed both descriptively and interpretively while considering levels of the socio-ecological model. Quantitative data were analyzed using descriptive statistics (eg, frequency, mean, standard deviation, t-tests) in SPSS. As is common practice in the use of the CS frequency scale, data were treated as continuous variables.10,20 There was no missing CS subscale data. Open-ended questions were analyzed by looking for narrative threads (ie, patterns) within and across responses. 31 Lead researcher (CC) treated the respondents’ metaphors, metaphor stories, and descriptions of work-related stress as a whole; grouping similar threads together across and between responses. Data about requested resources and stories of wellbeing were analyzed by creating common threads across responses. Thread groupings and names of threads were refined iteratively through discussion with the research team until they felt credible and resonant. 32 While not initially planned, differences between staff and volunteers become apparent in the qualitative threads; sub-group analysis was then applied to survey data. 33
Results
A total of 58 surveys (response rate = 56%) were received with 50 respondents providing responses to the open-ended questions.
Summary of Respondent Socio-Demographic Characteristics
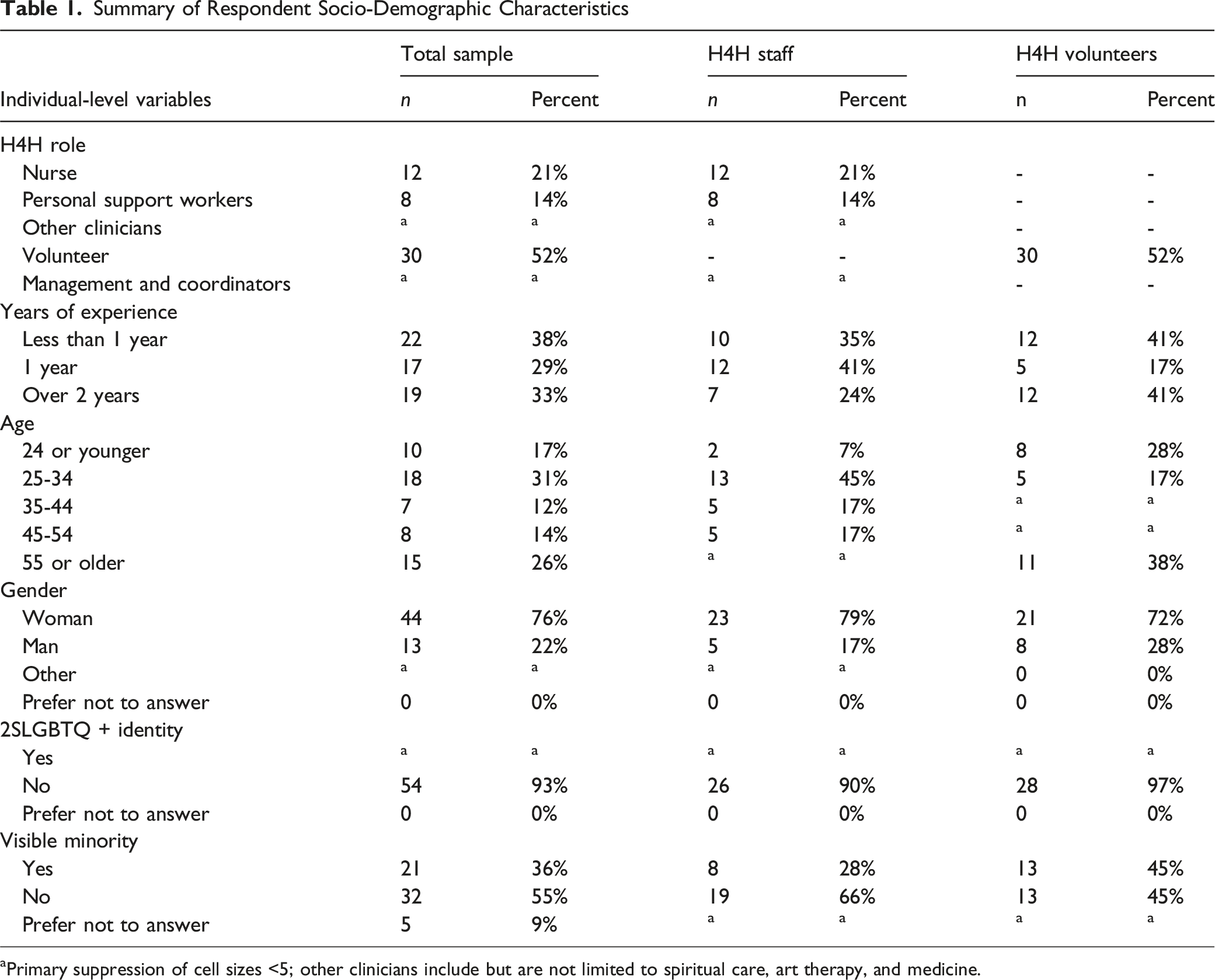
aPrimary suppression of cell sizes <5; other clinicians include but are not limited to spiritual care, art therapy, and medicine.
Compassion Satisfaction
H4H providers (n = 58) had an average PROQOL-5 compassion satisfaction (CS) subscale score of 45.1 (SD 5.0). No statistically significant differences were noted between staff and volunteer responses (P = .535). Volunteers on average scored 44.3 (SD 4.9), while staff scored 45.8 (SD 5.1). The majority of respondents (74%) scored above the ‘high compassion satisfaction’ cutoff (PROQOL-5 CS subscale >42). No respondents scored within the ‘low compassion satisfaction’ cutoff (PROQOL-5 CS subscale ≤22).
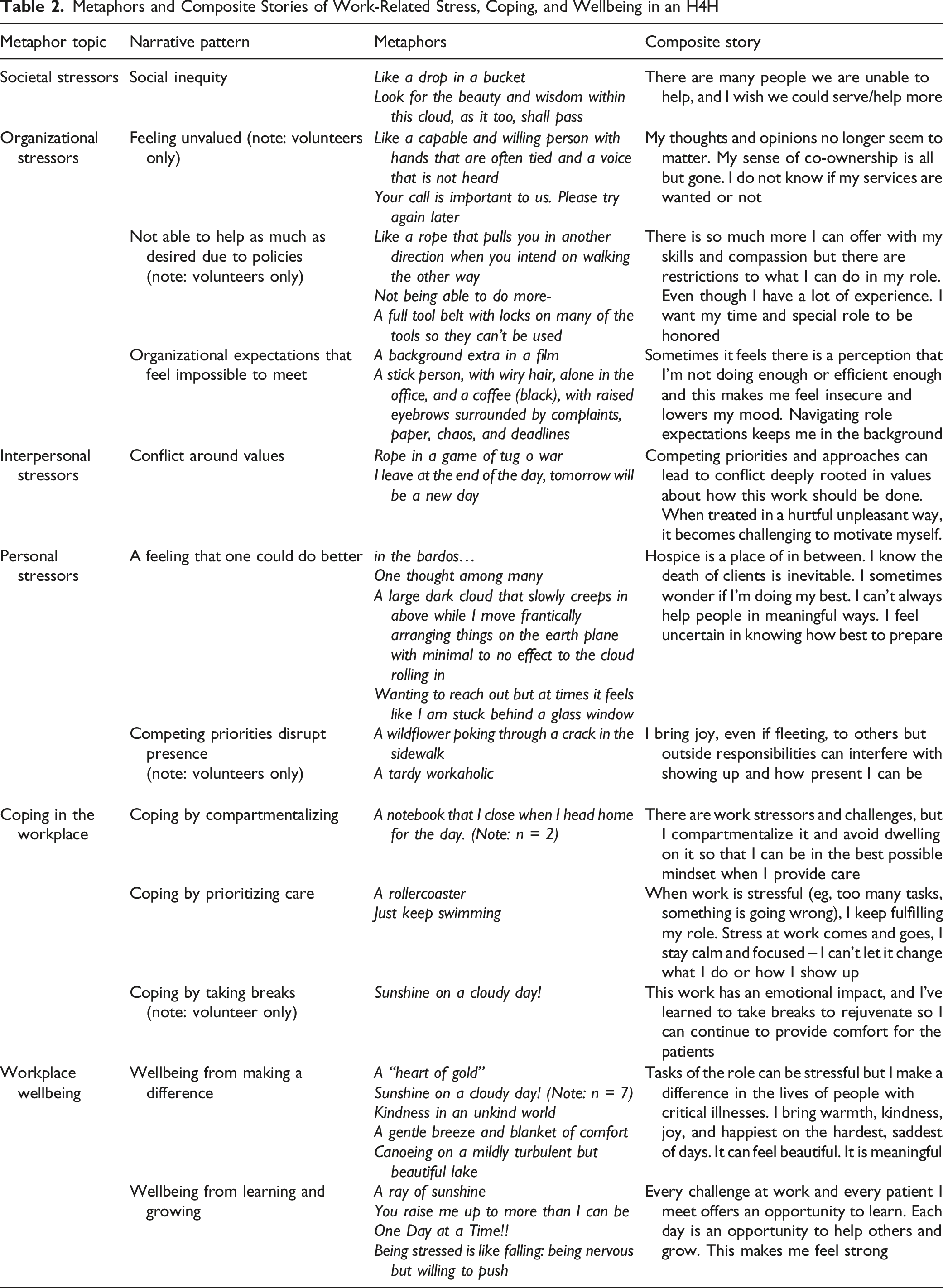
Metaphors of Stress at Work
Metaphors and Composite Stories of Work-Related Stress, Coping, and Wellbeing in an H4H
Resources to Support Workplace Wellbeing
When asked if they accessed any formal or informal resources to support workplace wellbeing, 30 respondents answered “no”, explaining that they were “not interested” or “unaware of resources”. However, of these 30 respondents, five respondents (2 staff; 3 volunteers) said that they drew on personal resources (eg, exercise, prayer, meditation, music). Of the remaining respondents, four (3 staff; 1 volunteer) said they use formal resources (eg, virtual meditation sessions, spiritual counselling). Twelve respondents (6 staff; 6 volunteers) said they use informal resources (eg, peer support) and one preferred not to answer.
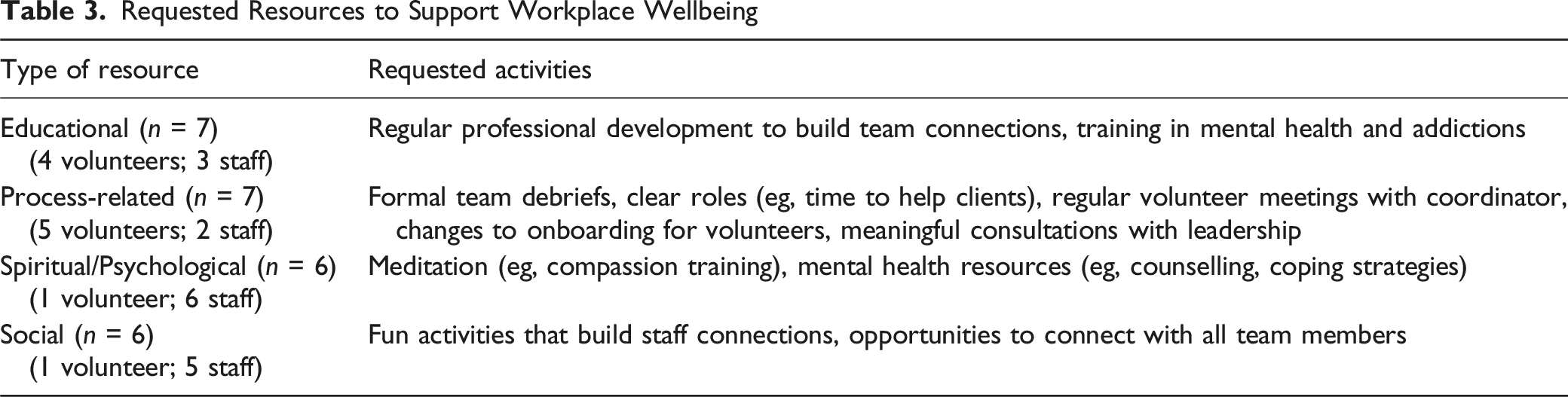
Requested Resources to Support Workplace Wellbeing
Conceptualizing H4H Workplace Wellbeing
Conceptualizing H4H Workplace Wellbeing
Discussion
Summary of Findings
Most respondents had high CS and, notably, two-fifths had started H4H work within the last year. Respondents’ storied metaphors span the socio-ecological model, depicting seven factors causing them stress. Volunteers shared unique stressors (eg, feeling undervalued) which may require specific support. While most respondents indicated they do not access resources to support workplace wellbeing, requests for additional resources were made. Respondents conceptualized workplace wellbeing as involving quality care, supportive relationships, personal fulfillment, and respectful culture.
Key Interpretations
Responses on the PROQOL-5 CS subscale were positively skewed and indicated high CS in this population. In other research, hospice care workers in the USA had lower mean CS scores of 40.5 20 and 41.07. 10 Previous research demonstrates that CS scores are positively correlated with mindful meditation, self-reflection, play, and rest.10,20 Some survey respondents reported using meditation, prayer, exercise, music, and spiritual counselling to support their workplace wellbeing. This offers a potential explanation. However, the highly skewed data may also indicate a ceiling effect or a social desirability bias. Future research can examine other scales that measure protective factors against burnout.
The metaphors of work-related stress are similar to other hospice research that attributes provider burnout to organizational factors, such as high workload and prolonged work hours10,34; interpersonal factors such as disagreement with colleagues over treatment plans; and individual factors such as feeling ineffective in treating patients’ symptoms. 34 Likewise, other hospice volunteers also experience stress from not feeling appreciated, conflict with colleagues, and feeling limited by role restrictions.35,36 Unique to this group of H4H providers, societal inequity was identified as a factor causing stress, which reflects the complex H4H context. While not reflected in hospice literature, our findings share similarities with research on social workers’ and shelter providers’ burnout which is shaped by societal inequities such as reduced resources and clients’ oppression.13,37 Societal inequities will need to be considered within solutions to mitigate burnout in future work.
Two-fifths of respondents started providing H4H care within the last year. CS is positively correlated with job satisfaction and employee retention 10 and negatively correlated with burnout. 10 Having a workforce that is new to the work and feels effective in their abilities offers an opportunity to develop innovative ways to sustain this feeling of effectiveness. However, over half of the survey respondents said that they do not access any formal or informal resources to support workplace wellbeing. Of the respondents who do, about equal numbers of volunteers and staff use informal resources (eg, peer support) with more staff than volunteers accessing formal resources (eg, virtual meditation sessions, spiritual counselling), which may be related to more time spent at the hospice. To address low engagement with resources yet a desire by many for more, future work could plan for ways to integrate tailored resources into the work flow to increase access and uptake. 38 Knowing that burnout develops over time, supporting orienting H4H providers may be especially crucial. This echoes the respondents’ suggestions for enhancing orientation, role clarity, training, and volunteering processes.
Potential indicators that may help sustain workforce capacity are found in respondents’ conceptualization of workplace wellbeing. Most of the concepts align with psychological health and safety in the workplace. 39 Both staff and volunteers discussed wellbeing as tied to providing quality care, personal fulfillment, and a respectful culture. Having supportive relationships was also important; staff focused on supporting colleagues, whereas volunteers focused on supporting clients. Other research has found that the wellbeing of hospice providers is linked to the intrinsic emotional rewards of the work10,36 and having a sense of accomplishment.5,36 Integrating and enhancing these aspects of wellbeing into future strategies will be important.
The requested workplace resources differ slightly by role, with volunteers requesting more process-related support and staff requesting more spiritual/psychological and social support. Overall, the requests align with research on protective measures against burnout. Process-related resources,10,18,34 team education, 34 and supportive relationships10,34 can mitigate burnout. Spiritual and psychological resources such as meditation can help manage stress,7,12 are negatively correlated with burnout, 20 and are already being accessed for support by some providers indicating some acceptability.
In developing resources to mitigate occupational stress, personal coping strategies and developing supportive relationships have been found to be particularly important. 10 Given the identified stressors, requested resources, and the conceptualizations of wellbeing, mindfulness-based interventions appear promising as a protective measure in the hospice context. Mindfulness-based interventions have been effective for enhancing personal coping, and addressing personal-level factors such as feeling inadequate and juggling multiple priorities in hospice palliative care providers. 8 There is also evidence to suggest these practices can address organizational factors by strengthening respectful team relationships, and improving team communication in hospice settings.7,8 Furthermore, critical for this context, mindfulness training has lowered levels of secondary traumatic stress 10 and helped providers develop anti-oppressive practice to target systemic level stressors. 40 We recommend future work take a multifaceted approach to providing and integrating resources that support wellbeing in the H4H context, which can include mindfulness-based interventions in addition to education, team building, recognition, and other organizational processes.
Strengths and Limitations
Our survey is among the few hospice studies to include volunteers, who are often excluded despite playing a critical role in care delivery. 36 Methodologically, eliciting metaphors 31 within a survey was, to our knowledge, novel. Over half of respondents created a metaphor, indicating that metaphors are a feasible way to engage experts-by-experience within surveys.
This survey was conducted in a single organization, limiting the sample pool and potential for representation of the perspectives of men, gender diverse people, and people who identify as 2SLGBTQ+. Future work will involve multiple H4H organizations to boost diversity and total sample size which would support more complex analytics to explore the impact of intersectionality on CS.
Conclusion
The wellbeing of these H4H providers appears to be tied to their ability to be of service to clients, develop supportive relationships, experience personal fulfillment, and belong to a respectful culture. Chronic multi-level work-related stressors that erode the sense of meaning about why one is engaged in the work they do is linked to burnout. 17 We recommend future work take a multifaceted approach to supporting workplace wellbeing. One approach could include enhancing orientation with a focus on role clarity, training, and volunteering processes. Another approach could implement group-focused interventions, such as recognition of work and mindfulness-based practices to increase personal coping, strengthen team connections, and promote anti-oppressive practices to address systemic stressors. To our knowledge no mindfulness-based interventions have been tailored to the unique H4H context, creating an opportunity for future research in this area.
Supplemental Material
Supplemental Material - Examining Compassion Satisfaction and Work-Related Stress Within a Hospice for the Homeless (H4H) Organization: Results From a Multi-Method Survey
Supplemental Material for Examining Compassion Satisfaction and Work-Related Stress Within a Hospice for the Homeless (H4H) Organization: Results From a Multi-Method Survey by Celina Carter, Mary Anne Olalia, and Justine Giosa in American Journal of Hospice and Palliative Medicine®
Footnotes
Author Note
All authors have read and agreed to the published version of the manuscript.
Ethical Considerations
Ethics was approved and obtained through the Research Ethics Board at Southlake Health (SRHC # S-004-2425).
Consent to Participate
Our research team emailed potential survey respondents a recruitment letter containing a study summary, consent information, and a link to the secure online survey that included radio button consent.
Author Contributions
Authors (CC and JG) made substantial contributions to the concept, design, analysis, interpretation, and writing of the work. (MAO) made substantial contributions to the data collection, analysis, and interpretation. All authors critically reviewed the work, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by SE Health and the Saint Elizabeth Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.