
Abstract
Background
Family members experience decision-making conflicts regarding changes in patient care. If the medical team does not attempt to understand the family members’ awareness of palliative care, family members may experience medical decision-making stress and dilemmas. This study examined the decision-making conflicts of the family members of patients dependent on prolonged mechanical ventilator regarding palliative care in Taiwan.
Methods
A cross-sectional design was used in this study. Family members of such patients in the subacute respiratory care ward and the respiratory intensive care unit of a medical center in Taiwan were recruited. A structured questionnaire was used to collect data.
Results
Among the family members of the 127 patients included, 57.5% hesitated to make palliative medical decisions and 61.4% experienced palliative medical decision conflicts. The absence of other chronic diseases, family members’ inability to accept the movement of patients to palliative care, and family members’ hesitation in palliative care medical decision-making resulted in decision-making conflicts. In this study, 127 prolonged mechanical ventilation-dependent patients (PMVDP) and their family members were examined. The results revealed that family members experienced palliative care medical decision-making difficulties (61.40% = <2.5). Predictors of palliative care decision-making conflict for PMVDP and their family members included the following: absence of other comorbid chronic diseases, the inability of family to accept palliative care on behalf of patients, and hesitation in palliative care medical decision-making by family members.
Conclusion
The study results are able to help Taiwanese medical staff in evaluating such conflicts and palliative care medical decisions of PMVDP.
Keywords
Introduction
Health care has identified 20 million patients with chronic diseases and related comorbidities requiring intensive care and respiratory care each year, ventilators consume medical service manpower and resources and lead to prolonged ventilator dependence. 1 Prolonged ventilator dependence cannot prevent death and decreased quality of life. 2 Many countries have actively promoted palliative care medical decision-making, and people have started to understand the concrete benefits of palliative care and provides a different medical decision-making and way of thinking.3,4
In 2000, the Taiwanese government launched the ventilator care integration plan for effective medical resource allocation in patients who require respiratory care. Care is provided on the basis of the stage of the medical tasks required for the patient; the four stages can be categorized as follows: intensive care unit (duration of ventilator usage: 0-21 days), subacute respiratory care unit (duration of ventilator usage: >21-42 days), chronic respiratory care unit (duration of ventilator usage >42 days), and home ventilator care (includes non-invasive positive pressure ventilators). 5 Although prolonged ventilation extends patients’ life expectancy, their self-care ability decreases with the progression of their disease, and their disease becomes irreversible. 6 Understanding patient and family–centered palliative care and providing decision support is essential. 7 In family members who are responsible for caring for the patient, the physical and mental stress and the costs of care will affect their decision toward the subsequent mode of health care for the patient.8,9 Stress may occur when taking life-or-death health care decisions. This results in an emotional burden. Furthermore, decision-making conflict showed a tendency to occur when family experience complex and uncertain medical decision-making and they are unable to make a decision. 10 Taiwan’s policy regarding palliative care for patients with mechanical ventilation, such as Hospice Palliative Care Regulation Amendment (2000) and Patient Right to Autonomy Act (2019) that allow patients to refuse treatments including mechanical ventilation. By having clear criteria for Do Not Resuscitate, thus avoiding medical conflicts between doctors and patients.11,12
Moreover, when families had a good relationship with the patient, the subsequent medical decision conflict was considerably less (P = 0.03). 13 The primary decision maker was more often male than female (P = 0.00). This may be because men are perceived by society as individuals as making major decisions and being primary supporters. The younger the family member and the poorer their financial status, the higher their “uncertainty” decision conflict score (P = 0.00). 14 Furthermore, the attitudes of medical proxies in medical decision-making reported that among Asian families, decision-making conflicts dramatically reduced if the family member was the eldest son. 15 Furthermore, the relationship between siblings may become strained when facing palliative decisions for their parents. However, even if the decision-making proxy has a close relationship with the patient (eg, spouse), both parties were reported to have different viewpoints and values. 15
In Chinese culture, affection and relationships between family members are expressed with subtlety. Family may typically experience medical decision-making stress and dilemmas when the patient is unconscious, and has not discussed subsequent medical care with their relatives. 16 In Taiwan, medical decisions are usually made by family members together rather than by the patient alone (eg, mechanical ventilation). This decision-making process is influenced by Confucious culture; however, it might create emotional burdens and moral tensions.17,18
A study on Chinese people who migrated from countries, such as China and Australia found that Chinese families often have similar health care decision-related issues (eg, not wanting to burden others) and the culture of filial piety affects discussion contents and conflict in medical decision-making. 15 Uncertainty regarding the prognosis that may occur after the decision is made persists. 19 Studies in Western countries have also reported that important family (eg, spouses) are worried that the treatment decisions of the patient will be affected by their decision-making. Hence, family evidently show doubts when making medical decisions for patients in both Chinese and Western cultures.20-22 One study on dementia patients revealed that the decision-making conflict was decreased after the intervention of advanced palliative care planning, and family expressed a clear understanding of the main components of end-of-life care, the risks, and the difficulties in making their own decisions. 23 Therefore, early palliative care intervention could improve the care quality of patients. It can also alleviate stress and conflict in family members, increase support in decision-making, and allow both patients and family to achieve a consensus in future medical decisions.24,25
A review of the literature revealed that studies have examined the issue of palliative care acceptance in ventilator-dependent patients6,26-28; however, few have examined the decision-making conflict in family regarding the movement of the patient to palliative care. Hence, the following variables were considered in decision-making conflict related to this study are derived from Behavioral Decision Theory developed by O’Connor (1995) 29 : uncertainty, feeling uninformed, uncertainty regarding personal values, feeling unsupported, and decision satisfaction.
Therefore, this study was to examine medical decision-making conflict and the associated factors that influence the family members of prolonged mechanical ventilation-dependent patients (PMVDP). The study framework is based on the above literature review and can be seen as follows (Figure 1). Study framework.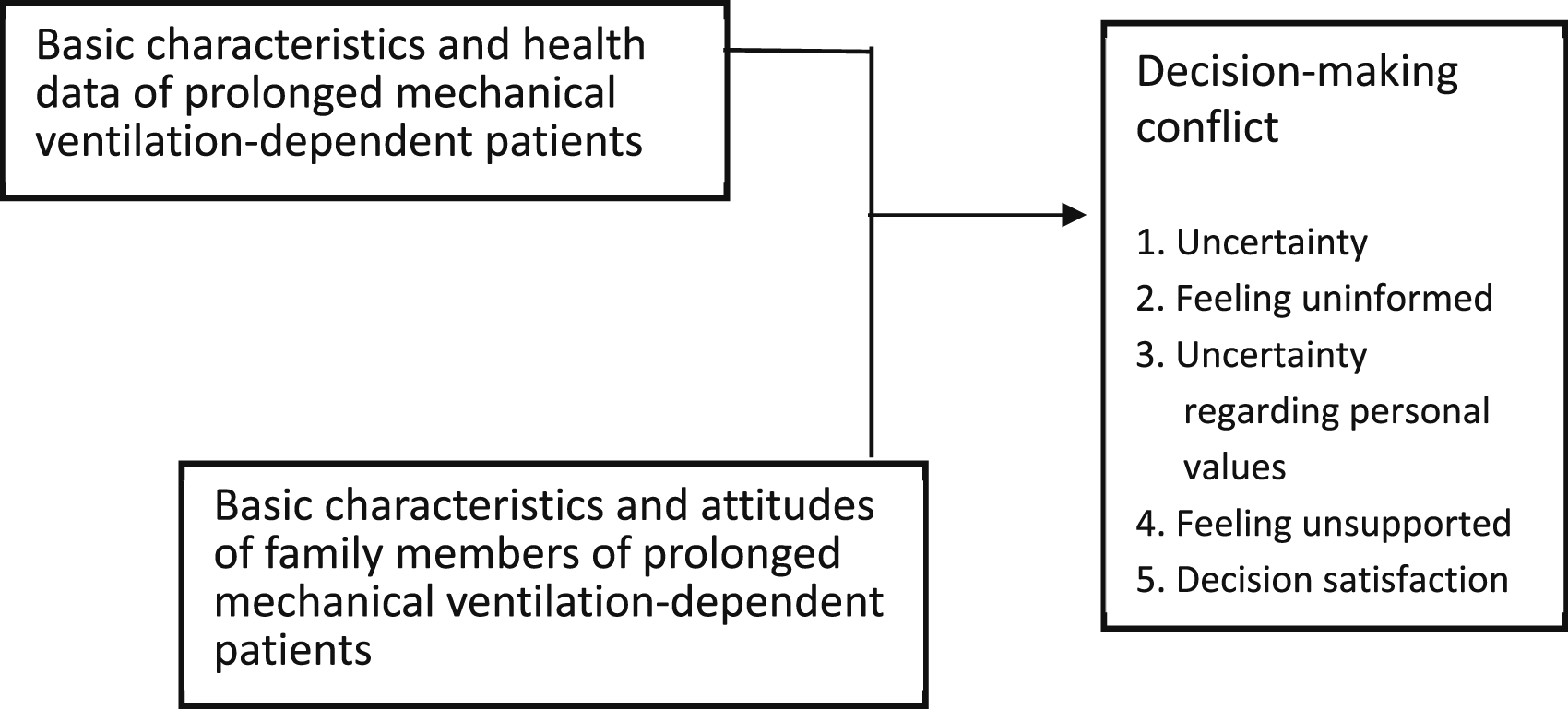
Study Objectives
To examine the decision-making conflicts of the family members’ attitudes of family members of PMVDP regarding palliative care in Taiwan.
Methods
A cross-sectional study design was used, and convenience sampling was employed to examine palliative medical decision-making conflict in the family members of PMVDP. The study participants were the family members of patients who had been using ventilators for >21 days in a subacute respiratory care ward in a medical center in Taiwan. A structured questionnaire was used for data collection. The participants were recruited from March 2019 to October 2020 in the subacute respiratory care center of a metropolitan hospital in Taiwan.
Study Participants
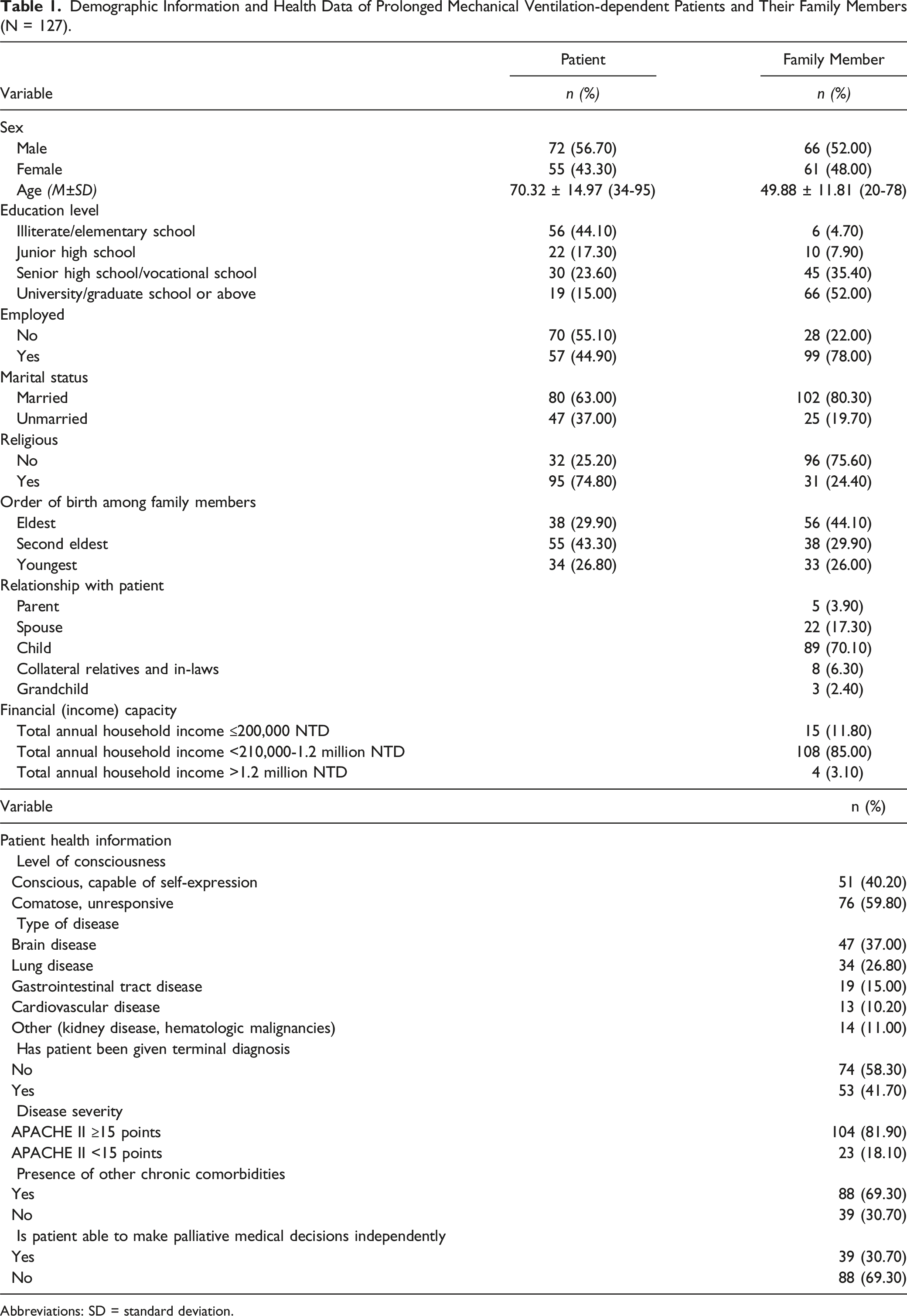
Demographic Information and Health Data of Prolonged Mechanical Ventilation-dependent Patients and Their Family Members (N = 127).
Abbreviations: SD = standard deviation.
Study Tools
The study tools were developed by O'Connor (1995) 29 and de Su (2013) 31 except general characteristic data (developed by the author following relevant literature40).
General Characteristic Data of PMVDP
Sex, age, education level, employment status, marital status, religious beliefs, and order of birth in family members.
Health Information of PMVDP
Level of consciousness, disease category, terminal diagnosis, disease severity (APACHE II), other chronic comorbidities, and whether the patient could participate in palliative care decision-making independently.
Attitudes of Family Members of PMVDP toward Palliative Care
Attitudes toward palliative care (DNR [do not resuscitate] signing), hesitation toward palliative care, and their perceived level of support in their willingness to participate in decision-making.
Decision Conflict Scale (DCS)
A decision conflict scale with good validity and reliability was used.14,32 This includes uncertainty of the contents of palliative care, feeling uninformed, uncertainty regarding personal values, feeling unsupported, and decision satisfaction (16 questions in total). The scale uses a Likert-type scale for scoring, and the total score ranged from 16-80 points. The total score was divided by the number of questions and a final score of ≥2.5 indicated the presence of decision-making conflict whereas a score of <2 indicated the absence of decision-making conflict. The Cronbach’s α for this scale was 0.94.
Data Collection
This study protocol was reviewed by the Institutional Review Board (IRB) (no. CF19058A-1) prior to conducting research, and the ward supervisor assisted in initiating palliative care consultation meetings to invite the family of patients who met the recruitment criteria. A researcher verbally informed the study participants regarding the objectives and methods and also informed them that they could terminate the interview and questionnaire completion at any time. All information was anonymized and collected questionnaires were coded to protect the privacy of the participants.
Statistical Analysis
IBM SPSS for Windows 26.0 statistical software was used for database construction and analysis. 33 Descriptive statistics, an independent sample t test, one-way analysis of variance (ANOVA), and binary logistic regression analysis were all used for statistical analyses. Statistical significance was set at P < 0.05.
Ethical Consideration
All procedures were performed in compliance with the hospital’s guidelines and ethical committee requirements after the IRB approval.
Results
Analysis of the Basic Characteristics and Health Data of PMVDP and Their Family
There are 127 family members who participated survey in this study and relevant patient information for this study was collected from the medical record. The basic characteristics and health data of PMVDP and their family members were presented in Table 1.
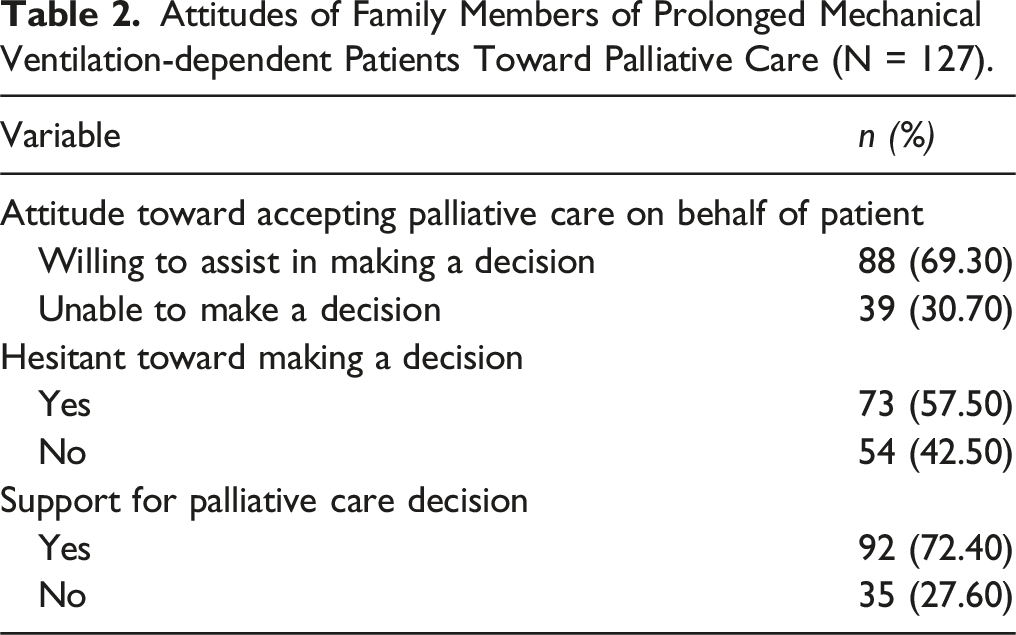
Attitudes of Family Members of PMVDP toward Palliative Care
Attitudes of Family Members of Prolonged Mechanical Ventilation-dependent Patients Toward Palliative Care (N = 127).
Palliative Care Decision Conflict in Family Members of PMVDP
Palliative Care Decision-Making Conflict in Family Members of Prolonged Mechanical Ventilation-dependent Patients (N = 127).
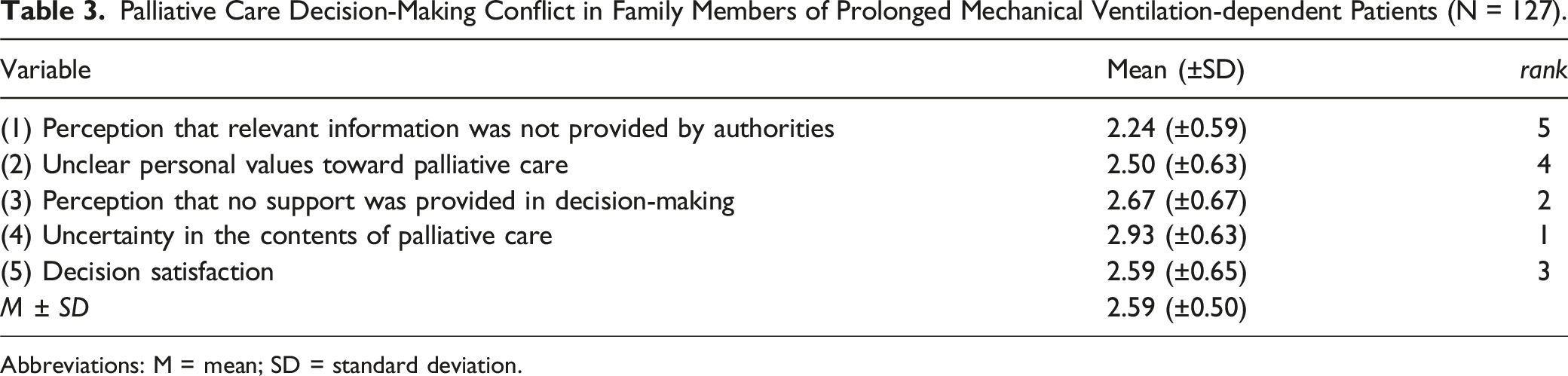
Abbreviations: M = mean; SD = standard deviation.
Comparison of the Differences in PMDVP
Differences in the Basic Information, Family Attitudes Toward Palliative Care, and Palliative Medical Decision Conflict in Prolonged Mechanical Ventilation-dependent Patients (N = 127).
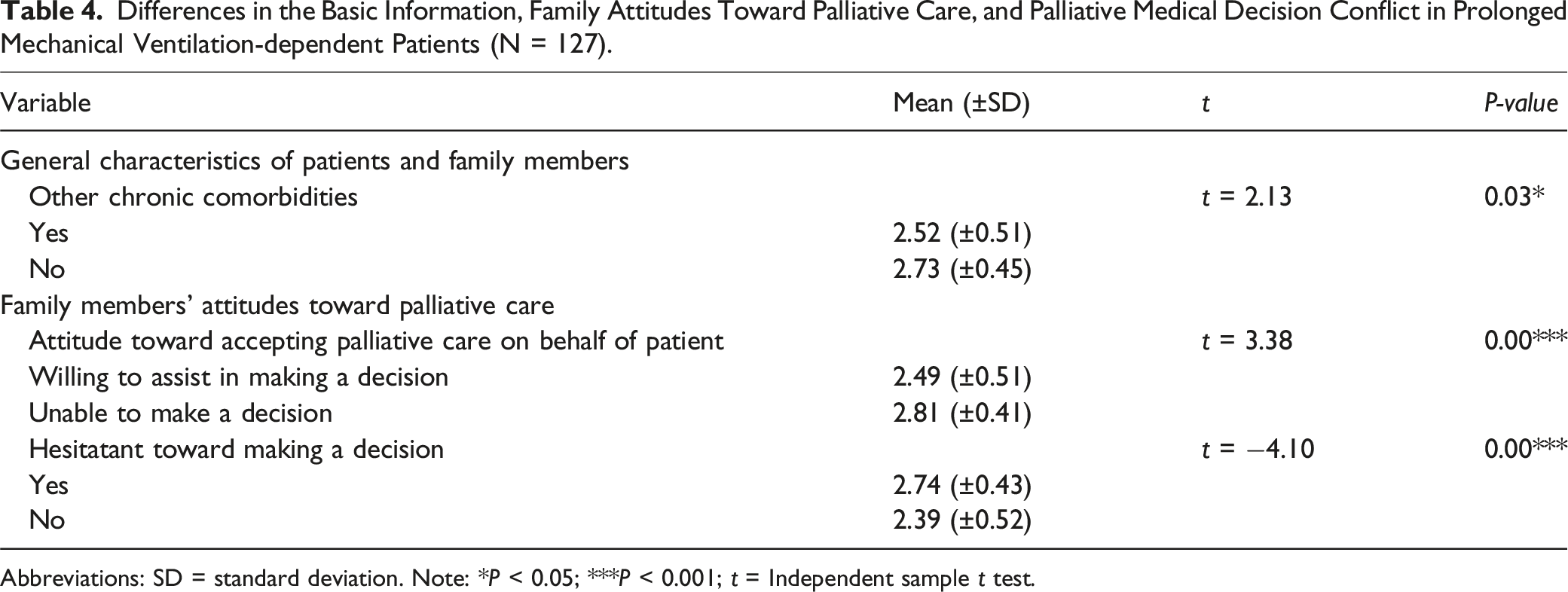
Abbreviations: SD = standard deviation. Note: *P < 0.05; ***P < 0.001; t = Independent sample t test.
Family who were unable to make the decision of moving patients into palliative care (2.81 ± 0.41) had greater medical decision-making conflict than those who could take the decision (2.49 ± 0.51) (t = 3.38; P = 0.00). Family who hesitated in making palliative care decisions (2.74 ± 0.43) had greater medical decision-making conflict than those who did not hesitate (2.39 ± 0.52) (t = −4.10; P = 0.00) (Table 4).
Predictors of Palliative Medical Decision Conflict in PMVDP and Their Family
The presence of significant differences between the family of PMVDP who did and did not have other chronic comorbidities (Δ odds [odds ratio (OR) value] = 5.11; 95% confidence interval [95%CI] = 1.71-15.24). Therefore, the probability of decision-making conflict arising in family of the patients without other chronic comorbidities was 5.11 times that of those with other chronic comorbidities. A significant difference was observed in the attitude of family members toward accepting palliative care on behalf of the patient for those in the “unable to accept palliative care on behalf of the patient” category (Δ odds = 4.77; 95%CI = 1.54-14.71). This shows that the probability of decision-making conflict in family who were “unable to accept palliative care on behalf of the patient” was 4.77 times that of those who “were able to accept palliative care on behalf of the patient.”
Binary Logistic Regression Analysis of Predictors of Palliative Medical Decision Conflict in Prolonged Mechanical Ventilation-dependent Patients and Their Family Members (N = 127).
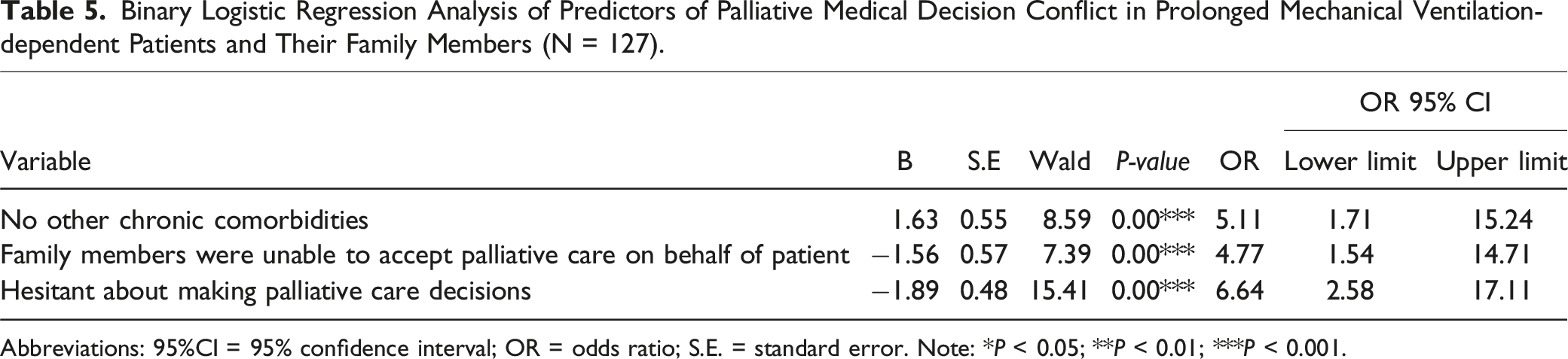
Abbreviations: 95%CI = 95% confidence interval; OR = odds ratio; S.E. = standard error. Note: *P < 0.05; **P < 0.01; ***P < 0.001.
Discussion
Among the 127 study participants (family) and patients, the patients were older adults (>70 years) whereas their family members were in their middle-ages and employed. The main decision-making family were predominantly men rather than women. Men are perceived as individuals who fulfill the role of making major decisions and being primary supporters for their families. However, with changing times, the role of females in shared medical decision-making should not be overlooked. Typically, in Asian family, more responsibilities and expectations are on women as caregivers. They feel guilt if they can not perform this duty. In Chinese society, “filial piety” is usually interpreted as “trying one’s best to save the patient to the end”. Choosing palliative care is sometimes seen as giving up or being unfilial. Therefore, families avoid talking about death when patients’ condition worsens which increases stress and guilt. 15 The medical decision-making process is influenced by Confucious culture, but can create emotional burdens and moral tensions, as women are expected to play the primary caregiver role in the family. This gender role stereotype makes women the default caregivers.17,34 Furthermore, it is almost common belief that females are the caregivers of society. However, physical care tasks are delegated to female caregivers, and decision making to male caregivers. 34
We found most family were unable to make palliative care decisions independently (69.3%). If the patient did not independently express their preference for palliative care and the clinician provided the decision-making family with PMVDP care outcomes without fully understanding the treatment preferences of the patient, the family may make alternative decisions owing to the arising conflict. This form of ineffective communication may lead to the default provision of active life support, which may conflict with the patient’s preferences. 9 Hence, when patients in the intensive care units who experience a major trauma or illness leading to loss of consciousness, the family members will experience hesitation or decision-paralysis as all possible decisions will affect the medical outcomes of the patient. This will extend to the next stage of subacute respiratory care. 20 Therefore, delays in the decision-making process may lead to worsening of the patient’s condition. Hence, the patient and their family should ensure that discussion of the decision-making process as soon as possible, as it is vital to achieve a consensus in the decision-making process. 25
Overall, the family members of PMVDP experienced difficulties in making palliative care decisions (mean score ± SD: 2.59 ± 0.50). This is predominantly due to the fact that family do not have the experience in making medical decisions on behalf of the patient. The family members also had likely never discussed future medical preferences with the patient in the past. This resulted in unease and uncertainty during the entire process, and family expressed regrets toward their decisions owing to doubts and lack of support from other family members. 34 Having an understanding of the values of family, appropriately dispelling doubts, asking other joint decision-making family to help participate in decision-making, and increasing family support could decrease regrets associated with the decision-making process.9,14,19 Therefore, when family have no choice but to make medical decisions on behalf of the patient, medical staff should also remind family to respect the patient’s stance and views, and objectively choose the decision that will maximally benefit the patient based on their past beliefs and values. This will reduce decision-making conflicts in family members. Conflicts may also be minimized by providing psychosocial support to family members with tense relationships and not increasing the stress experienced by the family tasked with the decision-making process when they face the patient.17,22,35
The general characteristic predictors of palliative care decision-making conflict in family members of PMVDP were as follows: “absence of other comorbid chronic diseases,” “family were unable to accept palliative care on behalf of patients,” and “family hesitated in palliative care decision-making.” Sudden changes in a patient’s outlook and the absence of other pre-existing chronic comorbidities may leave the family unprepared. Furthermore, family are typically concerned that palliative care intervention is equivalent to abandoning treatment altogether. Furthermore, most patients are dependent on prolonged ventilation and unable to communicate, resulting in family members facing a dilemma on whether to move the patient into palliative care.17,34
Indicated that improving communication and decision-making for patients and families are high priorities in the last days to weeks of life. 36 Moreover, study on understanding responses of family members psychological symptoms after patients’ critical illness, they found when family members are not able to discuss with patients regarding the treatment preferences of the end of life, it usually leads difficulties in decision making. 37 This is similar to our study’s predictors on “unable to accept palliative care on behalf of the patient” and “family members hesitated in palliative care decision-making”. Few studies also indicated that patients’ disease severities (eg, brain injury) may have multiple clinical factors, including age, prognosis and multiple complications. These are factors that may affect decision-making for patients.38,39 These are also aligned with our study on predictors of palliative care decision-making.
However, if the patient has been bedridden for a long time due to a stroke or has cancer which has progressed, their family will have a better understanding of the future condition of the patient and the difficulties they may face in arranging future care. These factors, combined with explanations from the medical team, allow the family to gradually understand the changes in the patient’s quality-of-life and reduce conflict in decision-making.4,22 Patients without other chronic comorbidities may also have better general life functions than those with other chronic comorbidities. Once patients are no longer able to independently make a decision, the impact on their family members will be extremely significant. The family will consider whether the patient will experience the worsening effects of their condition for an extended period of time and whether their future quality-of-life will be worsened. This may lead to decision-making conflict arising from potential differences between their decisions and the patient’s original intentions. This finding is identical to those reported previously8,14 and the results reported by another study indicated that impractical and optimistic views among family members and a lack of consensus on medical intervention resulted in the unwillingness of family to discuss subsequent medical care for the patient. 21
Regarding Taiwanese patients with chronic comorbidities, one study found that ventilators are still used even though 80% of patients before death. 28 Hence, even if the patient does not have any chronic comorbidities, the impact of decision-making on the family could be reduced at all stages if the family understand the meaning of palliative care sooner, or if the patient has signed a medical order for pre-emptive treatment.27,28 Hesitation in making medical decisions can be reduced by allowing family to consider the best health care interests of the patient; listening to, and arranging for the intervention of interdisciplinary team (eg, psychologists); providing holistic health care that meets physical, mental, social, and spiritual needs; assisting family in understanding legal, emotional matters, decisions must be made; and increasing support between family members.22,39
Study Limitations
This study was performed in the subacute respiratory care unit of a medical center in Taiwan. Due to the geographic location and the turnover rate for access to beds, it required more than 1.5 years to recruit participants for this study. During this period, researchers attempt to recruit participants in other regional hospitals. However, regional hospitals’ staff were unwilling to participate in the study. Therefore, the recruitment process of our study population was limited to one single hospital. Furthermore, because of the COVID-19 pandemic, the time for visiting patients in person was limited. The pandemic led to the restriction of visitors in medical settings, which made it difficult to recruit participants. Furthermore, this study is a cross-sectional study that focuses on family caregivers. Other populations, such as health professionals or patients (when they are still conscious) views may be limited. Moreover, using qualitative interviews of family caregivers are not included.
Conclusion
In this study, we examined the perspectives of families in decision-making conflicts related to palliative care for PMVDP in Taiwan. A cross-sectional design was used in this study. Among the family members of the 127 patients included, more than half of participants (57.5%) hesitated to make palliative medical decisions and more than sixty percent of participants (61.4%) experienced palliative medical decision conflicts. The results revealed that family do experience palliative care decision-making difficulties. We also found that the absence of other comorbid chronic diseases, the inability of family members to accept palliative care on behalf of patients, and hesitation in palliative medical decision-making by family members are predictors of palliative care decision-making conflict for PMVDP and their family. This study is able to help Taiwanese medical staff evaluate such conflicts and palliative medical decisions when they take care of PMVDP.
For future research, our study is focused on a quantitative approach to perspectives of families in decision-making conflicts related to palliative care for PMVDP. The health professionals’ views on this topic can be investigated further. Furthermore, qualitative research design can be considered to obtain an in-depth understanding of the decision-making process of family members of PMVDP in facing palliative care. Moreover, further understanding of the general public’s views of the palliative care process can also be explored.
Relevance to Clinical Nursing Practice
Our study found that family members of PMVDP may face conflicts when they realize patients encounter various life-support and long-term ventilator dependence. Furthermore, family face whether to decide to use palliative care or not is a complicated in decision-making process. The main predictors of family palliative care decision-making conflicts may include whether patients have other chronic illness comorbidities or not, the family’s ability to make palliative care decisions for patients, and the family’s uncertainty about palliative care decisions. In clinical practice, these can be included as key points in the meetings with family. Furthermore, it is recommended to strengthen the interaction between the health care team (including nurses) and family members, such as, holding family conferences regularly and flexible visiting hours. In doing so, family and the health care team can frequently communicate and discuss regarding palliative care for PMVDP.
Footnotes
Acknowledgments
The authors thank all participants who participated in this study.
Author Contributions
Made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; CJC, LWL, SYW. Involved in drafting the manuscript or revising it critically for important intellectual content; LWL, CJC, SYW. Given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content; SYW, LWL, CJC, JLW. Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; SYW, LWL, CJC, JLW
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.