
Abstract
Background
Moral distress (MD), the notion of not being permitted to act in a morally and ethically correct manner, is evident amongst oncologists caring for terminally ill patients. Oncologists often contend with complex decisions, such as withholding treatment and managing family distress. Sociocultural and individual considerations also influence an oncologist’s perception of MD, which can vary in severity due to changing ethical, practical, clinical, moral and professional considerations and shifting contextual circumstances. Their impact compromises an oncologist’s wellbeing, patient outcomes and care of their family. Recent data suggests long-term consequences to MD and alludes to a broader cost of caring that encompasses compassion fatigue, vicarious trauma, secondary traumatic stress and burnout.
Methods
This study aims to determine how oncologists in Singapore experience MD and the costs of caring through secondary analysis of interviews with 12 oncologists.
Results
Analysis of the interview transcripts revealed the following domains: 1) sources of MD; 2) sources of the costs of caring; and 3) protective factors.
Conclusion
This secondary analysis of Singaporean oncologists suggests that MD is not frequently an isolated experience; rather, it leads to growing distress amongst oncologists—contributing to a wider cost of caring. This then impacts oncologists’ decisioning, actions, practice and career trajectories. Longitudinal structured training, establishing personalised support for all oncologists and creating a safe working environment supported by the host organisation are thus critical to ensure sustainable practice.
Keywords
Introduction
Experiences during the COVID-19 pandemic have had significant ramifications upon the careers, mental health and general wellbeing of physicians. 1 These reports have refocused attention to the impact of moral distress (MD) on physicians. 2 However, effective study of this phenomenon is compromised by the lack of a clear understanding of MD.
MD has been variously attributed to “a serious threat to an individual’s moral integrity, inability to act on core values and obligations” 3 ; “distress resulting from one’s actions not achieving the desired outcome” 4 ; and deciding on a course of action without effectively balancing the issues or a clear determination of what is ethically right.5,6 In truth, concepts of MD have been shown to be shaped by the physician’s prevailing values, beliefs and principles (henceforth belief systems), as well as the ethical, practical, clinical, moral and professional considerations in the wider sociocultural setting.3,5-10 It is also affected by resource availability, manpower shortages, high workloads and poor continuity of care.3,6,7,10,11
Recent studies have revealed that physicians not only experience MD, but also a wider cost of caring that encompasses compassion fatigue, vicarious trauma and secondary traumatic stress.12-15 If left unattended, this may predispose to burnout and limit physicians’ practice and ability to find meaning and satisfaction in their roles. This is especially felt by medical oncologists (henceforth oncologists) due to their involvement in end-of-life care; recruitment of terminally-ill patients in clinical trials; use of therapies based on extrapolated data and questionable evidence; and acquiescence to unwise patient choices and family demands.16-21
Contributing to the above phenomenon in Singapore are ‘Asian values’ transmitted by local governmental policies rooted in regnant family-centric thinking.22,23 These evolved Confucian-based concepts have been absorbed by a multi-cultural, multi-ethnic and multi-religious population 24 that considers the interests of the family unit as part of, or more important than, the individual. This is partly due to the belief that the fate of the individual impacts the family as a whole,25,26 leading to familial participation in any decision-making processes.27-29 However, taken to the extreme, familial determination may usurp the patient’s autonomy and right to self-determination.27-30 It also reduces personal privacy as family members become privy to any and all aspects of care determinations. In some cases, this dynamic dispenses with the involvement of the patient as a whole.27,28,31,32 Moreover, the patient’s best interests might be trumped in favour of those determined by the family,27,28,33,34 leading to practices such as collusion. These scenarios can significantly impact care approaches and end-of-life practices locally and regionally, such as in Malaysia, Taiwan, Hong Kong, China, Korea and Japan.28,30,35,36
One such example illustrating the complex interplay of cultural factors and oncological treatment principles is the act of providing treatments, such as total parenteral nutrition (TPN), to conform with familial beliefs and societal norms on feeding at the end-of-life. This is despite regnant clinical evidence 37 suggesting the limited impact of such interventions on the prognosis of patients at the end-of-life. Rather, such interventions may even diminish the quality of life, prolong the dying process and impede the patient’s wishes to pass at home. Contextually, however, feeding at the end-of-life is a key sociocultural belief in Singapore. These beliefs purport feeding as a sign of ‘love’, non-abandonment and enduring filial piety.18,38,39 Continuing to feed loved ones via artificial means, including TPN, intravenous hydration or nasogastric tubes, presents a sign of ‘maintaining hope’—another key facet in local interpretations of filial piety underpinning Asian values.
Individual and contextual factors thus influence MD and its links with the wider costs of caring, burnout, 10 job dissatisfaction, increased intention to quit5,10,11,40,41 and compromises to physicians’ physical and mental health. 42 Considering the downstream effects on patient care, outcomes, experiences and safety, there is a pressing need to better appreciate MD, the costs of caring and the precise mechanisms by which individual, contextual and sociocultural factors exert their influence.
Methods
To answer the primary research question, “What is known about moral distress and the costs of caring on medical oncologists in Singapore?”, and secondary questions including, “What are the factors contributing to moral distress and the costs of caring on medical oncologists in Singapore?”; “What is the impact of moral distress and the costs of caring on medical oncologists in Singapore?” and “How do medical oncologists in Singapore cope with moral distress and the costs of caring?”, we carried out a secondary analysis of previously conducted semi-structured interviews with oncologists with MD at a tertiary cancer centre in Singapore. 43
Ethics Approval and Consent to Participate
Ethics approval (2021/2176) was obtained from the SingHealth Combined Institutional Review Board. Informed written and verbal consent was obtained from all participants.
Semi-Structured Interviews
A systematic approach was adopted by the expert and research teams to review current accounts of oncologists’ encounters with MD. Insights from these reviews contributed to the design of the semi-structured interview guide (Supplemental File 1).
The interview questions were designed to explore and evoke notions of how the personal beliefs, values, principles and practices of oncologists were influenced by their lived experiences in the field. Local oncology physicians and qualitative researchers then reviewed and refined the interview guide44-46 through a modified Delphi process. 47
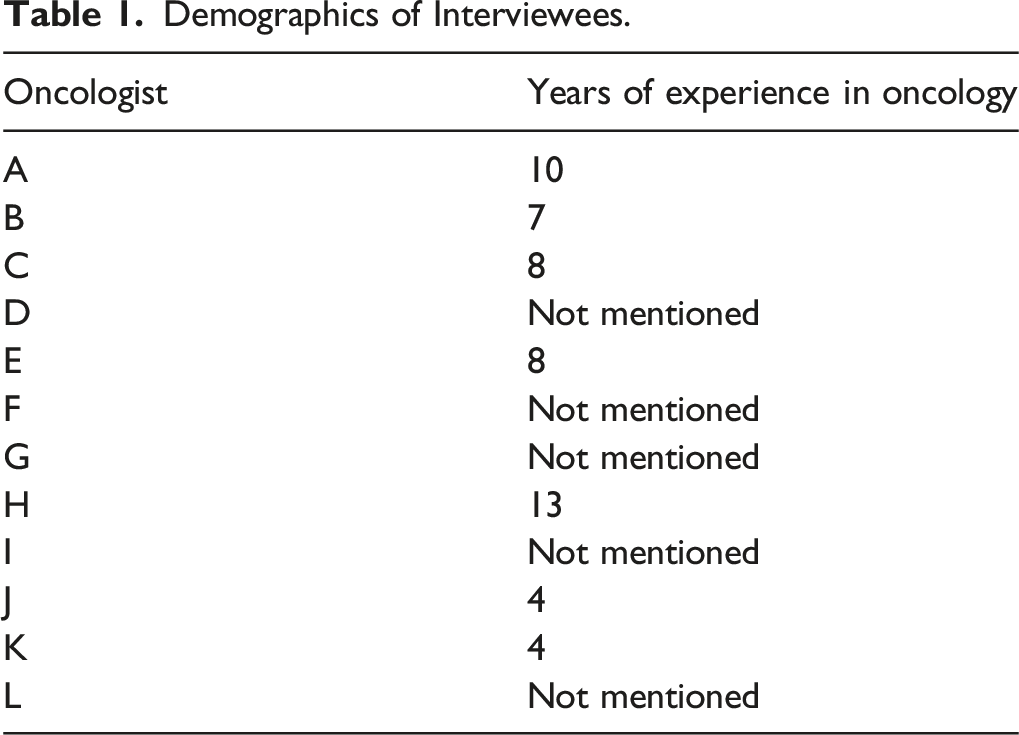
In 2023, 12 oncologists were recruited through email invitations sent to all medical oncologists in the National Cancer Centre Singapore, a tertiary cancer institute. Enclosed in the emails were the participant information sheets, including details on the study’s context, aims and duration. Participants were informed of their rights to anonymity and withdrawal from the study at any point without prejudice. Participation was also voluntary, with no incentives provided. Verbal and written consents were obtained from all participants before the commencement of the interviews. On an institutionally secured Zoom video-conferencing platform, two trained research team members conducted one-on-one interviews between 12th September 2023 and 17th December 2023. Each interview, conducted in English and audio-recorded with consent, lasted around an hour each. Data collection and analysis were conducted simultaneously. Three reviewers experienced in the use of Braun and Clarke’s 48 approach to thematic analysis carried out independent analyses of the anonymised transcripts.
Participant recruitment and interviews were concluded when no new themes or insights emerged in two consecutive interviews. Audio recordings were anonymised and underwent transcription before member-checking for confirmation that the transcripts accurately conveyed the perceptions of the participants.
Validity and Reliability of Analysis
For the purposes of triangulation, the secondary analysis was carried out by three independent reviewers (YTO, YY, VR). The codes and themes identified by each reviewer were then discussed with one another in online and face-to-face meetings. In addition, the findings of each reviewer and the subsequent combined analysis were reviewed by an experienced external reviewer well-versed in the topic at hand. To further ensure theoretical validation, the results of the analysis were compared with prevailing data. An iterative process was employed wherein the identification of any new codes prompted a review of all transcripts to verify classifications and ensure complete data extraction.
Results
Demographics of Interviewees.
The following domains of key themes were found: 1) sources of MD; 2) sources of the costs of caring; 3) protective factors.
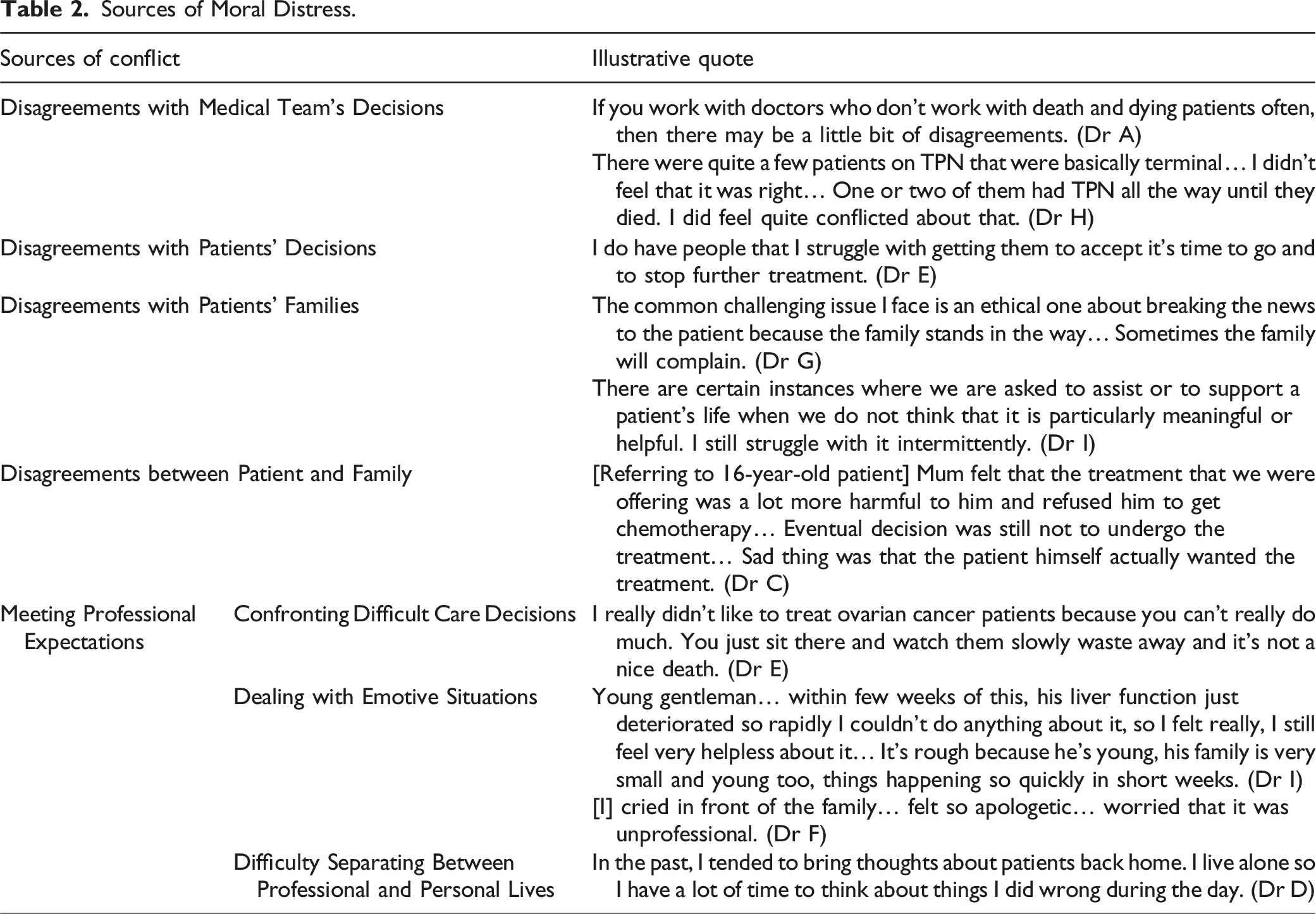
Domain 1: Sources of Moral Distress
Sources of Moral Distress.
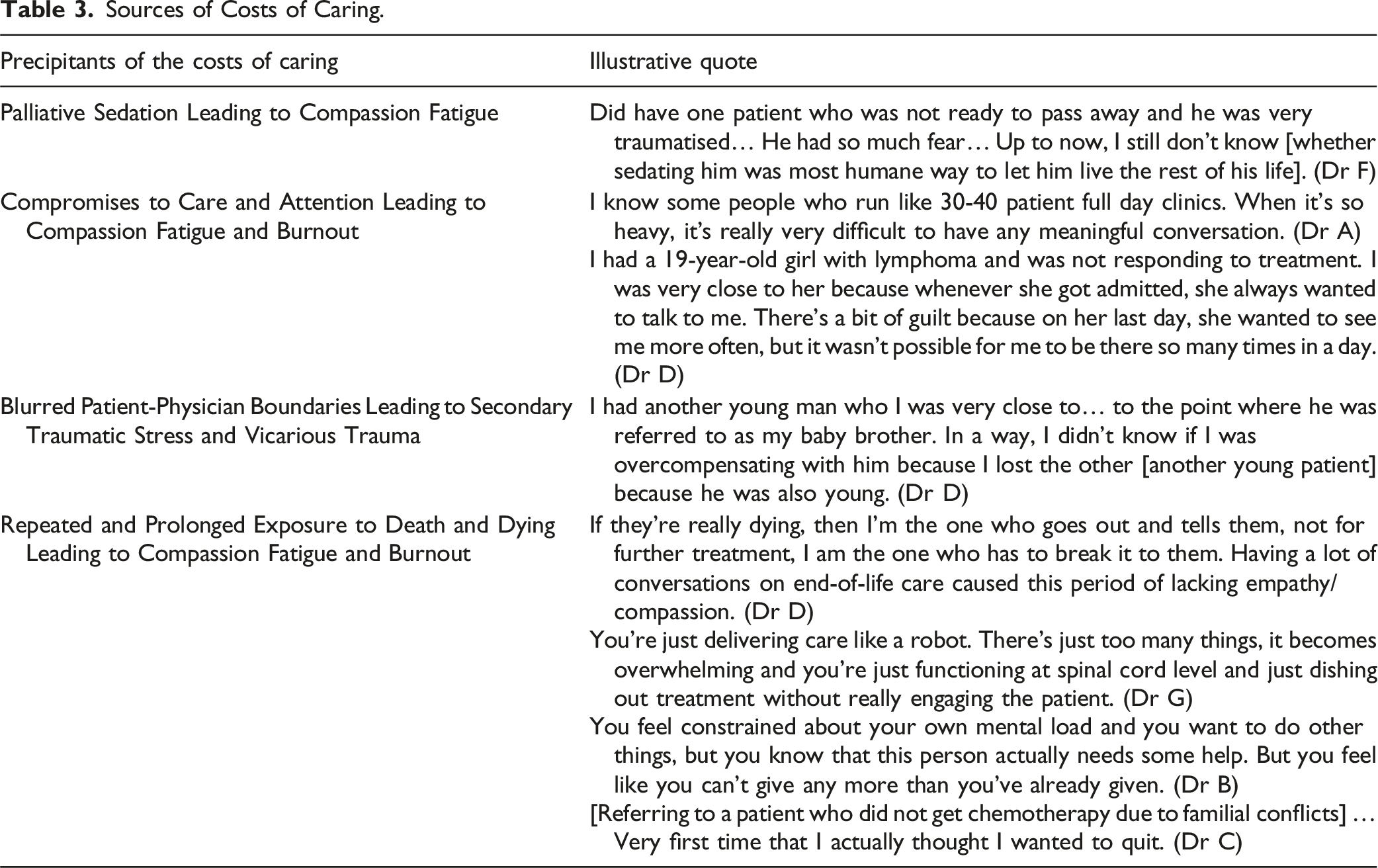
Domain 2: Sources of Costs of Caring
Sources of Costs of Caring.
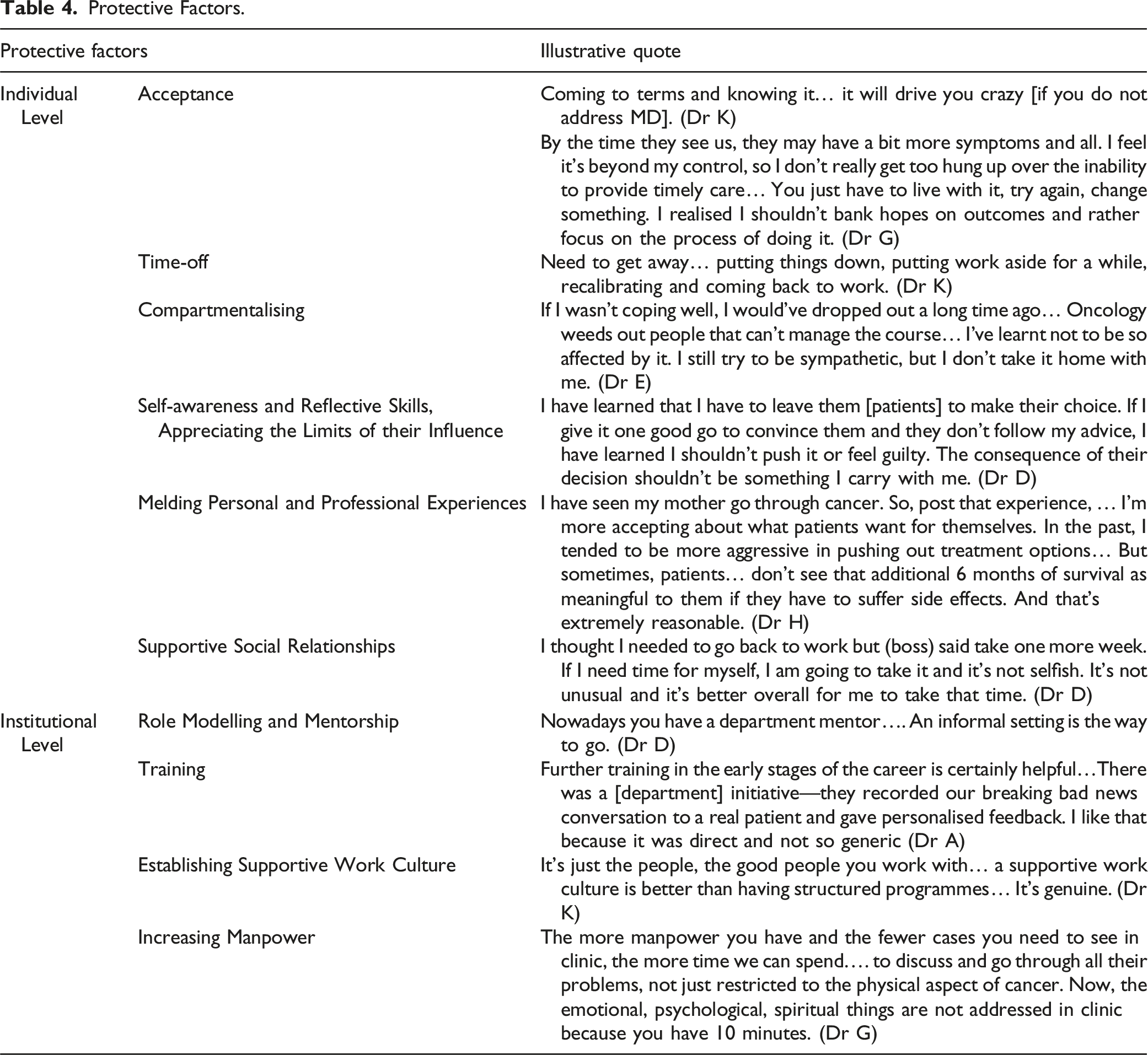
Domain 3: Protective Factors
Protective Factors.
Discussion
This secondary analysis of semi-structured interviews with Singaporean oncologists carried out in light of widespread accounts of MD and the costs of caring has yielded several noteworthy insights.
To begin, MD as a “negative emotional response that occurs when physicians know the morally correct action but are prevented from taking it because of internal or external constraints”
49
is a layered and evolving sociocultural construct with deep ramifications upon oncologists. MD appears to be a highly personalised notion that extends beyond sociocultural considerations.
50
Rather, it shows evolving individualised, relational, societal and psycho-emotional features linked to self-concepts of self and identity over time. If left unattended, it may lead to a wider cost of caring that encompasses CF, STS, VT culminating in burnout (Figure 1).43,51 Factors influencing moral distress, fatigue and the cost of caring.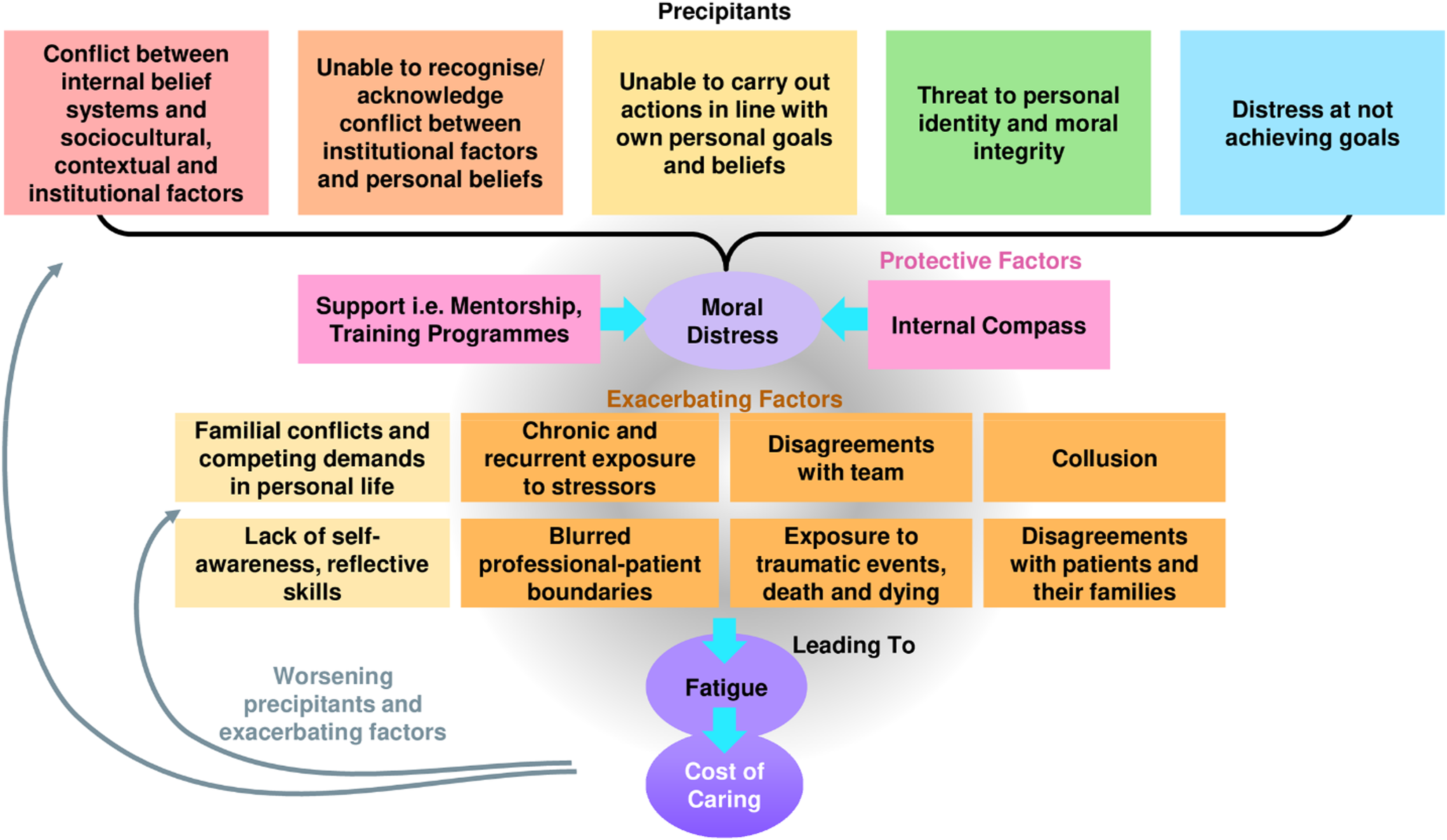
First, it is proposed that MD may be triggered by multiple factors either on their own or, more likely, in combination with one another. This includes internal conflicts between professional roles and personal beliefs; conflicts between regnant belief systems and contextual considerations; inability to act in a manner that is consistent with the oncologist’s belief systems and ethical and moral perspectives; threats to the oncologist’s identity; and failure to achieve desired treatment objectives.
Acknowledgement that one or more sources may provoke MD raises the possibility of persistent or repeated episodes of MD, given that these triggers persist within the working environment.
Predisposing to MD are individual and contextual considerations. Individual considerations include compromises to familial and social support; lack of self-awareness and reflectivity; blurring of professional and personal boundaries through development of personal ties with patients and their families; and identification with patients and their circumstances. This may be further exacerbated by contextual considerations, such as the lack of effective support at work; high workloads; manpower and resource shortages; and a poor practice environment. Constant exposure to death and dying in an emotionally laden setting where there may be little mentoring, guided immersion, regular debriefs and reflective support amplifies the contextual considerations at play. These contextual factors also raise the possibility that they may co-exist with and even exacerbate individual considerations.
Conversely, attenuating the risk of MD and its sequalae are growing levels of resilience, developing experience, maturing competencies, deeper and more consistent reflectiveness, greater self-awareness and better coping and support mechanisms. These oncologist-specific factors are also complemented by better sensing of conflicts or situations that could raise MD. The ability to assess, adapt and re-evaluate situations further builds the oncologist’s internal compass, described as an overall moral code that guides decisioning and actions. A maturing internal compass and institutional support factors (denoted by the pink boxes in Figure 1) attenuate MD.
It is also through the secondary analysis that we find links between MD and physical and emotional exhaustion traditionally associated with compassion fatigue. The near constant exposure to traumatic events, associated with feelings of powerlessness in witnessing complicated clinical, psychosocial and existential needs of patients and their families, and contending with familial demands amidst high workloads and resource and manpower shortages perpetuate distress and give rise to secondary traumatic stress. Additionally, a blurring of the physician’s personal and professional boundaries derived from journeying and building personal ties with patients and their families predisposes to emotional distress or vicarious trauma. We refer to this unique blend of compassion fatigue, vicarious trauma, secondary traumatic stress and burnout as the costs of caring (denoted by dark purple oval in Figure 1). Such links between MD and these costs of caring are novel and reveal a feedback loop that sees the costs of caring reducing resilience, hampering the internal compass and accentuating the exacerbating factors featured in the yellow boxes in Figure 1.
The complexities brought to the fore by evaluating individual and contextual considerations underline the need for longitudinal support and mentored immersion into oncology where coping and effective decision-making can be taught and cultivated over the course of training and beyond. It also reveals the need for careful consideration of the practice environment and its hidden curriculum and culture. Furthermore, this theory of MD and its relationship with the broader costs of caring may be applied to other specialties and practice settings. As shown by recent studies, physicians do not have separate professional and personal selves, thus a holistic whole-physician approach is necessary to effectively support physicians.12-14
Limitations
Interviewees who responded to our email invitations may have encountered more instances of MD or have been more impacted by MD. Interviewees who were more willing to share might also have more robust coping mechanisms that might not be representative of the oncologist population in Singapore. This generalisability of this study is further limited due to the exclusion of oncology trainees and other junior doctors caring for dying patients. Recall bias might pose a concern due to the one-off nature of the interviews.
Conclusion
This study represents a call to action for host organisations. Evidence of MD and indeed its propensity to incur the costs of caring emphasises the need for better appreciation of this phenomenon. To facilitate efforts to enhance support of oncologists, further studies on MD through the lens of personhood are proposed as the effects of caring for terminally-ill patients extend beyond the professional sphere. The design of a personhood-based assessment tool of MD could complement longitudinal appraisals of the effects of MD to evaluate the complex interplay of individual and environmental considerations that precipitate the costs of caring. This then will be our focus of our coming research as we look forward to continuing our discussion on this critical intersection of staff wellbeing, patient safety and organisational reputation.
Supplemental Material
Supplemental Material - Moral Distress and the Cost of Caring Amongst Medical Oncologists in Singapore
Supplemental Material for Moral Distress and the Cost of Caring Amongst Medical Oncologists in Singapore by Varsha Rajalingam, Yutian Yu, Yun Ting Ong, Annushkha Sinnathamby, Nila Ravindran, Nagavalli Somasundaram, Simon Yew Kuang Ong, and Lalit Kumar Radha Krishna in American Journal of Hospice and Palliative Medicine.
Footnotes
Acknowledgments
The authors would like to dedicate this paper to the late Dr S Radha Krishna, whose advice and ideas were integral to the success of this study, the late A/Prof Cynthia Goh, whose mentoring and insights guided the analysis of this data, and Thondi, Maia Akhlil and Raja Kamarul Ariffin whose short lives continue to inspire us to better support and care for others.
Author Contributions
All authors V.R., Y.T.Y., Y.T.O., A.S., N.R., N.S., S.Y.K.O. and L.K.R.K. were involved in data curation, formal analysis, investigation and preparation of the original draft of the manuscript, as well as the review and editing of the manuscript. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The MPS Foundation Grant Programme under Grant number TMPSFG2023008. The MPS Foundation was established to undertake research, analysis, education, and training to enable healthcare professionals to provide better care for their patients and improve their well-being. To achieve it supports and funds research worldwide that will make a difference and can be applied in the workplace.
Ethical Statement
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials. To request data from this study, please contact Prof Lalit Kumar Radha Krishna (
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.