
Abstract
Context
Health inequities in Hispanic populations require community-engaged solutions. Engaging Hispanic communities in research related to advance care planning (ACP) is critical to inform the development and evaluation of culturally appropriate interventions.
Objectives
To understand how to best adapt and implement Spanish-language ACP interventions in Hispanic communities across the US.
Methods
We apply the Framework for Reporting Adaptations and Modifications to Evidence-based Interventions (FRAME) to detail experiences during implementation of the national Project Talk Trial (PTT) that delivers two ACP interventions using a community-based delivery model. Semi-structured interviews with Hispanic community event hosts and research assistants (RAs) were conducted to explore challenges and solutions to implementation. Thematic analysis was applied to transcripts.
Results
Three themes from the community hosts (n = 9) were: (1) certified translation professional services were inadequate to successfully adapt interventions for diverse Hispanic communities; (2) a lack of Spanish-speaking RAs undermined the intention to address health inequities in the research; and (3) cultural norms, such as RSVP systems, differ in Hispanic populations. Themes from the RA interviews (n = 7) include: (1) discomfort with being unable to communicate appropriately with the research participants; and (2) improved connection and event flow when bilingual RAs attended events.
Conclusion
Our work highlights the value of a strong community-based delivery model, attention to local dialects and cultural nuances, the need for Spanish-speaking workforce and for balancing fidelity across national sites with adaptability when conducting rigorous research.
Trial registered
The trial titled “Engaging underserved communities in end-of-life conversations: a cluster, randomized controlled trial” is registered at clinicaltrials.gov [NCT04612738].
Keywords
We describe experiences during implementation of a national advance care planning trial conducted in diverse Hispanic communities. Interviews with community hosts and research assistants demonstrate the value of a strong community-based delivery model, challenges regarding dialects, the need for Spanish-speaking workforce, and balancing fidelity with adaptability when conducting rigorous research.Key Message
Introduction
It is well-established that Hispanic individuals in the U.S. face health disparities regarding advance care planning (ACP).1-5 ACP involves discussing one’s wishes with loved ones and clinicians, and then documenting them in an advance directive. 6 Hispanic individuals are less likely to have engaged in ACP or have named a surrogate decision maker or had end-of-life (EOL) conversations than white individuals.2,4 Community-engaged research can help overcome many of the barriers that contribute to these disparities, such as distrust in the health care system, language barriers, and cultural differences regarding discussion of EOL issues.7,8 Engaging Hispanic communities in ACP research is critical to inform development and evaluation of culturally appropriate interventions.
Tailoring research tools for use with Spanish-speaking participants must involve cultural and linguistic translations that retain meaning and relevance. 9 Although Nagy et al define translation as the process of “transmitting content from one language to another,” cultural and linguistic adaptation is more broadly understood as “transmitting the meaning of words while accommodating both content and context”. 9 Relatedly, heterogeneities in Hispanic culture and dialects must be considered when conducting national studies. Though crucial for generalizability of research, national implementation may be particularly challenging across multiple dialects/languages and is often not feasible for a single project.
Here we report on insights gained by our team after working in 9 distinct Hispanic communities as part of a cluster randomized controlled trial (RCT) among 75 underrepresented communities across the US. The trial uses community-engaged practices to implement two different ACP interventions using a community-based delivery model.10,11 Although all study materials were translated into Spanish by certified translation professional services, the need for additional adaptations arose during the trial because of our national scope and regional differences in dialect. We faced the challenge of balancing the need for reactive adaptations with the need for consistency and fidelity across sites and used the Framework for Reporting Adaptations and Modifications to Evidence-based Interventions (FRAME) or FRAME-Implementation Strategies (FRAME-IS)12,13 to document our experiences and lessons learned during our trial’s implementation to date. The Framework for Reporting Adaptations and Modifications to Evidence-based Interventions (FRAME) is a comprehensive approach with eight domains that systematically document intervention changes. These domains cover intervention components, implementation strategies, context, rationale, adaptation hypotheses, pilot testing, fidelity considerations, and measurement and evaluation. The framework aims to promote transparency and facilitate understanding of how evidence-based interventions are modified for specific settings and populations.12,13 Below results are reported from qualitative interviews with host participants and research assistants (RAs) to understand how to best adapt and implement Spanish-language interventions for Hispanic communities across the US.
Methods
The Project Talk Trial (PTT) is an NIH-funded RCT that seeks to determine underserved individuals’ responsiveness to two conversation-based ACP interventions (the Hello game and The Conversation Project Starter Guide). Communities agree to host events with a goal of 25-50 attendees, and the trial’s main outcome is completing an Advance Directive (AD). Additional outcomes include engagement in other ACP behaviors. The trial is registered at clinicaltrials.gov [NCT04612738] and is IRB-approved through Penn State (STUDY00014689).
PTT employs a community-based delivery model (CBDM),
10
which engages underserved populations by leveraging existing sociocultural networks to partner with trusted community partners. Hosts are recruited by the Hospice Foundation of America via its extensive national list-serv, social media, and other networks that includes a range of community-based organizations. Selected hosts complete three hours of research/event training and then utilize existing community connections and partners to arrange a PTT event. Hosts are required to use an RSVP system to confirm an acceptable number of anticipated attendees. As of 5/10/24 the study team had completed 45 of 75 events (Figure 1), with >1123 participants. Details of the trial protocol and CBDM have been published previously.10,11 Completed and pending events for project talk trial.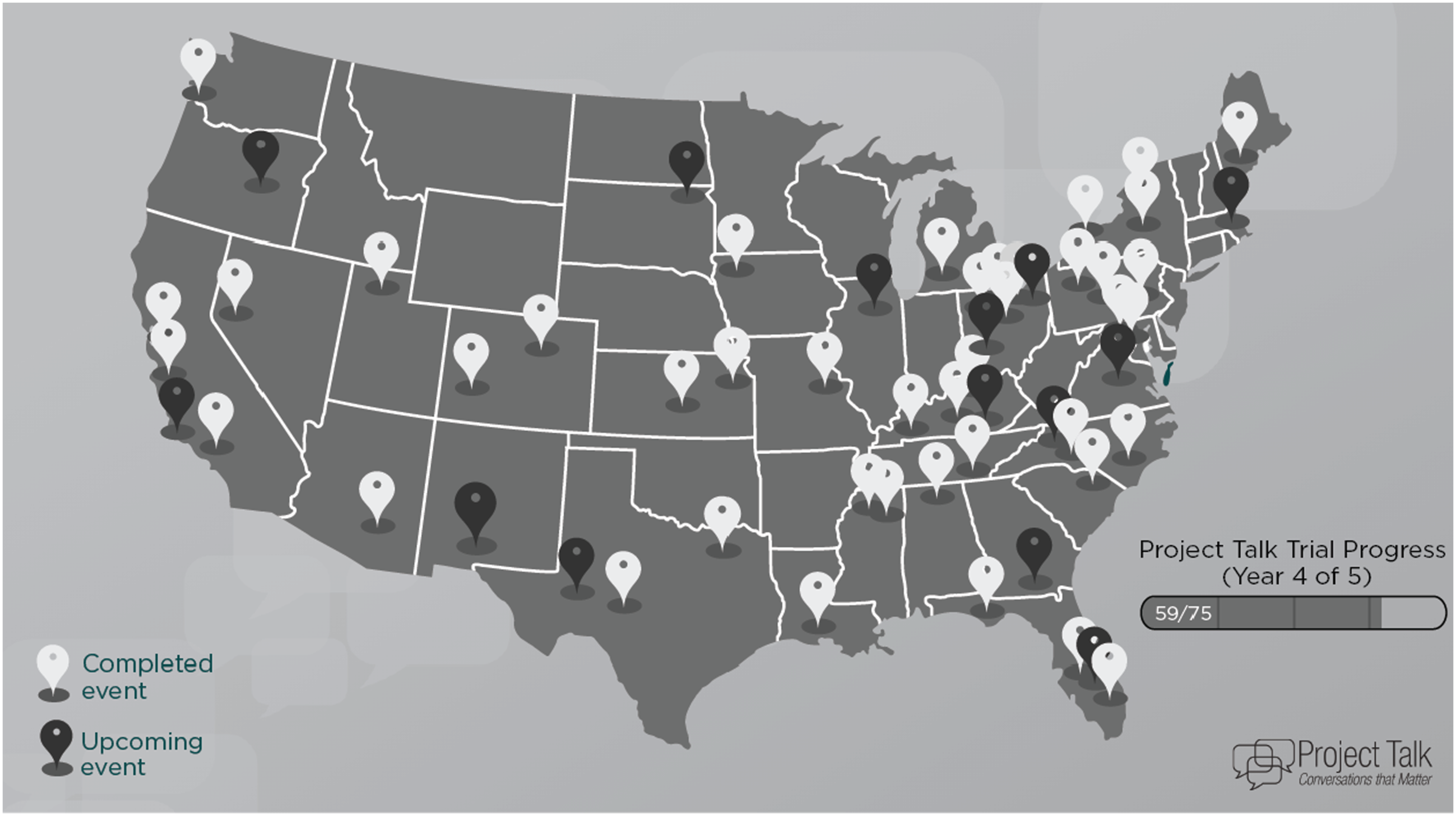
Qualitative Interviews
Summarized FRAME/FRAME-IS Reporting for Study Modifications.
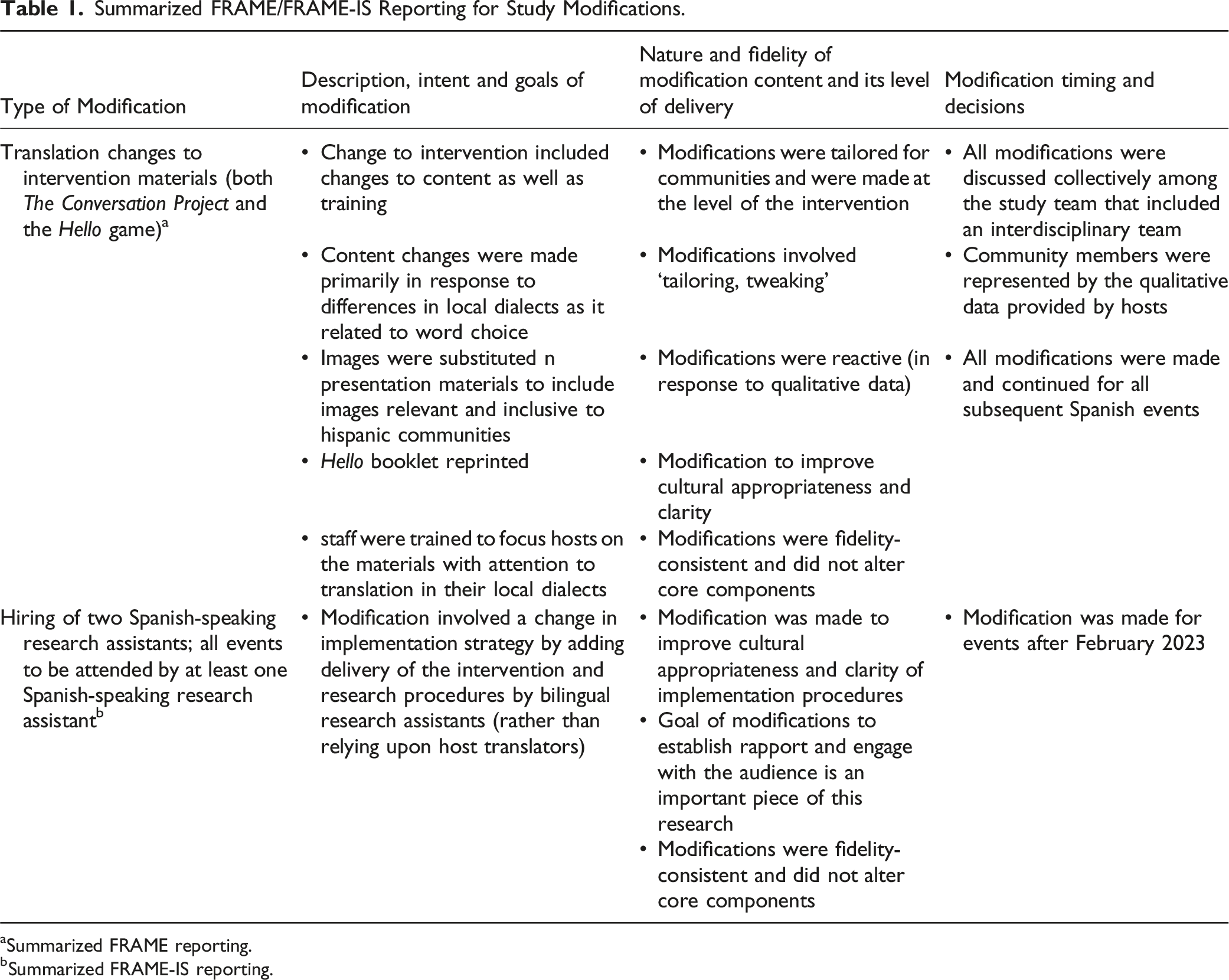
aSummarized FRAME reporting.
bSummarized FRAME-IS reporting.
Qualitative Analyses
Formal thematic qualitative analysis was conducted on transcribed Spanish-event host interviews and RA interviews conducted between 4/7/22 and 9/22/23. 14 Two analysts coded host interviews (HC, SA) and two analyzed RA interviews (EV, KF). Analysts reviewed transcripts to create an inductive codebook organized by categories, codes, definitions and examples. MAXQDA (v. 22) was used to organize and code the data. 15 All nine host transcripts were reviewed during codebook development; two analysts (HC, SA) independently coded 3 transcripts using the preliminary codebook, discussed discrepancies, and adjusted the codebook before analyzing the 6 remaining transcripts. Cohen’s kappa coefficient was 0.83, demonstrating high inter-rater reliability. Similar process was used by two analysts (EV & KF) code RA transcripts. Cohen’s kappa statistic was 0.81. For both datasets, themes related to the research question are included in these analyses.
Results
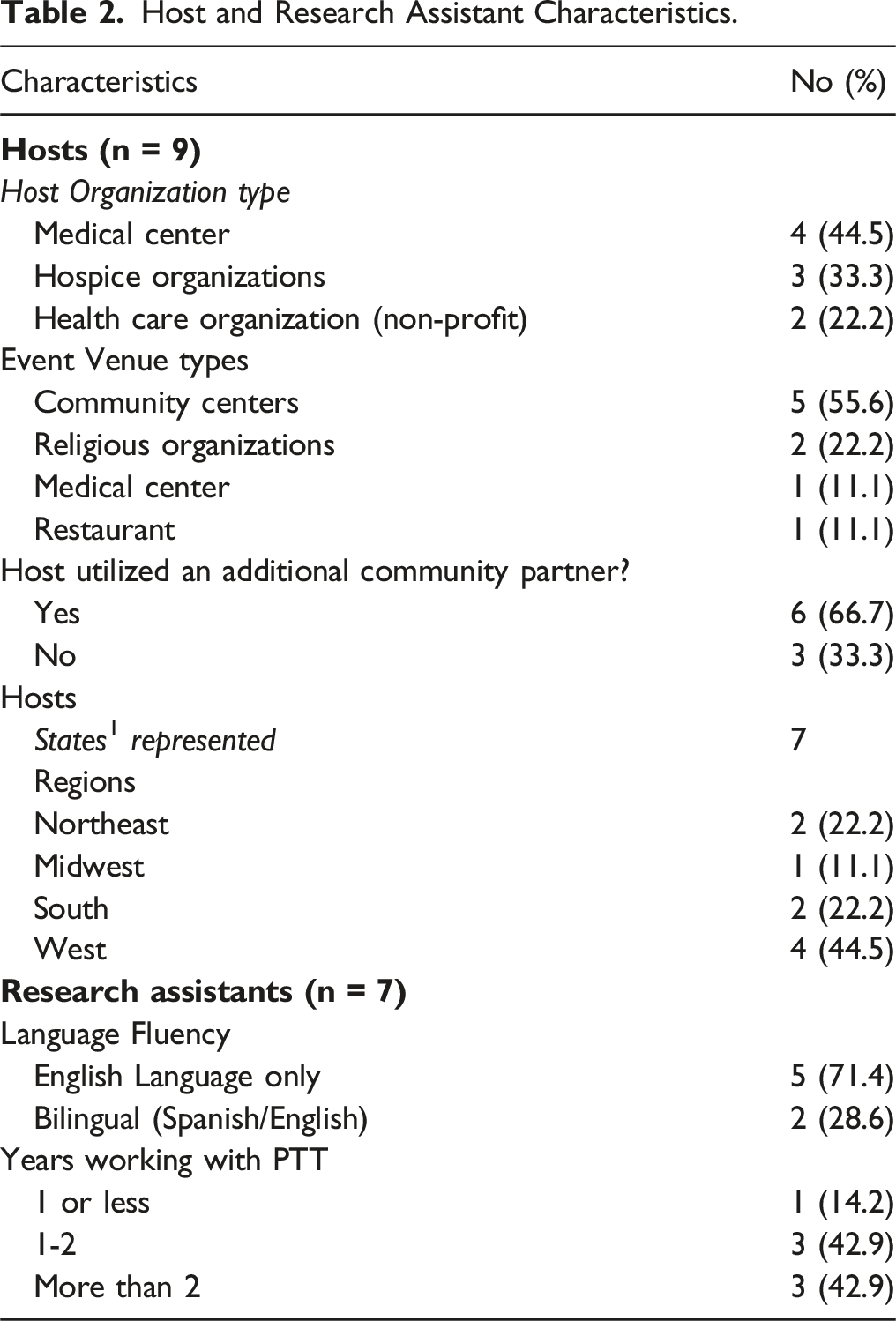
Host and Research Assistant Characteristics.
Themes From Host Interviews and Modification Decisions.
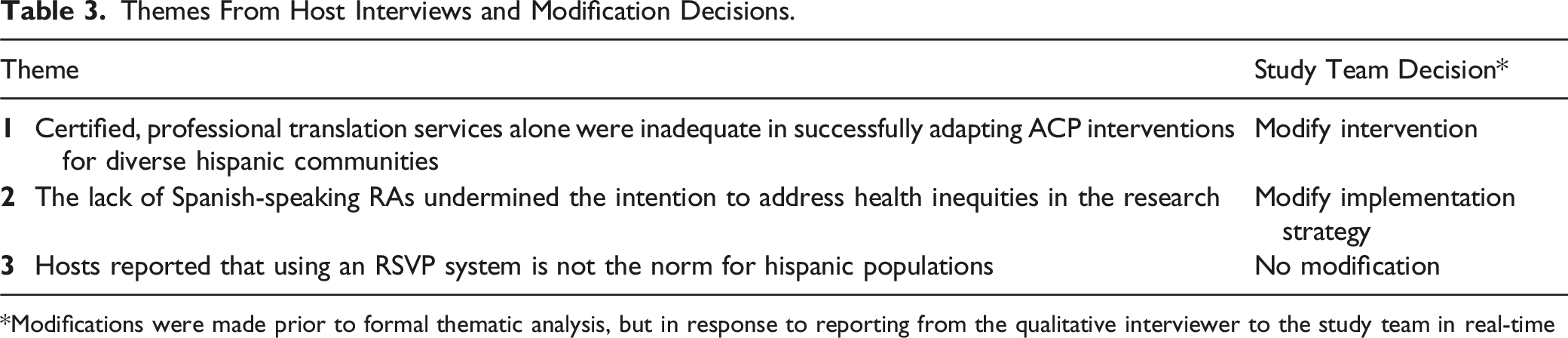
*Modifications were made prior to formal thematic analysis, but in response to reporting from the qualitative interviewer to the study team in real-time
Theme 1. Certified, Professional Translation Services Alone Were Inadequate to Successfully Adapt ACP Interventions for Diverse Hispanic Communities
Hosts noted some of the materials for both interventions were either confusing or inappropriate for their local communities. Several hosts noted that the Spanish translation of The Conversation Project material had confusing terminology or inappropriate grammar or ambiguous dialect. “On the PowerPoint, there was something, when he said “tips from the field”, when translated literally, it sounds like …fields of corn, fields of sunflowers. So the way it was translated, it sounded very much like tips from [a] rural town. Tips from the countryside. And [we] were constantly going to the English version to see exactly what the meaning was, and we're like, “No, this is field like expertise or people who experience this all the time, not [tips] from [a] rural town.” (Western Host)
Similar confusions were noted with the Hello game intervention. “We had played the Hello game ahead of time, probably about four weeks ahead of time, and that's when it was discovered by our Spanish interpreters that, Hey, I don't even know what this means. This doesn't mean what the English means. So [PTT] had to translate the entire Hello game booklet over.” (Western Host)
These findings were unexpected since both tools had been professionally translated during the design phase and implemented nationally. In response, the research team met with Spanish-speaking researchers and community members to seek guidance. During this process, we identified that the words in question were often dialect-specific and reflected geographical linguistic differences. The team applied the FRAME model to determine appropriate modifications that did not affect the core elements of the intervention (hence were “fidelity-consistent”; Table 1). Only minor edits related to language, changing images and adding Spanish-speaking videos were made. To address nuances of dialectical variations for future events, we began providing English-versions of the book to aid interpretation at events in response to feedback from a PTT host: [Something that was helpful]… a comment by the interpreters, was having the Hello game in English, as well as having it in Spanish….There was a few terms or a few differences in language that they wanted to see what does it say in English so I can make sure that I'm saying the right thing in Spanish, because there was a little bit of difference. (Northeast Host)
After modifications were made to the materials, no additional concerns were raised about translations in subsequent interviews.
Theme 2. A Lack of Spanish-Speaking RAs Undermined the Intention to Address Health Inequities in the Research
Nearly all hosts were motivated to participate in the research by individual and organizational missions to help reduce health inequities in Hispanic-speaking communities, particularly around ACP. “[We participated because of] the big picture goal of really wanting to know what best practices are in doing advance care planning, education and assistance for underserved or marginalized communities is a value that we share...” (Western Host)
However, hosts noted that because our team did not include a Spanish-speaking representative, there was substantial burden on the host to aid in translating the research instructions, despite all materials being available in Spanish. The inability for our research team to communicate directly with the participants served as a barrier to successful community engagement. “It's really important to have a Spanish speaker there representing [the research team]. First of all, it's a respect thing to have a person of the team be able to communicate with the people that they're trying to get information from. The other thing, just for your convenience, Hispanics and well, we have a tendency to be distrusting of agencies, government, things like that so when you have a person that just speaks English and there's no other way that audience is going to be able to identify with whoever's doing that presentation, it's not going to do that well. (Western Host)
Another host said, “We're trying to break that [communication barrier], but at the same time, we're not willing to go not even the extra mile but the extra couple of inches for it, just for something that small.” (Midwestern Host)
In addition to the lack of personal connections, several hosts noted the back and forth of interpretation added time, because information was relayed in English and then Spanish, which was burdensome. “To provide translation [for research instructions] …you to have one person talk and then another person to translate that, take the time to think about it and translate that. You're now doubling what's said and so doubling the amount of time.” (Western Host)
In response, we added two part-time Spanish speaking RAs to lead the Spanish-speaking events. All subsequent Spanish events were attended by at least one Spanish-speaking RA. After this modification, subsequent hosts stated how they can’t have imagined doing the event as originally planned (ie, without the support of the RA who spoke Spanish): “Having the bilingual staff helped. It made a big difference because I know at the beginning when they were training me, they said that I needed to provide the translations. So, a person was gonna be given instructions in English and then I needed to provide the interpretation. That would have been insane.” (Western Host)
Theme 3. Hosts Reported that Using an RSVP System is not the Norm for Hispanic Culture
Our protocol included a process whereby the research team required hosts to collect RSVPs prior to the PTT team committing to air travel and hotel fees, but several hosts were resistant to this request. While hosts understood the need for this, they also shared concerns that RSVP systems are not typically utilized in Hispanic populations around group events. “The Latino community, as I know it, are not used to RSVP. They're not used to [that], not even for weddings. So I [used] any chance or conversation that I had, to write down [their] name and phone number and do check-ins with them. So, I [would] not give all the information on the first contact. I will say, “I'm doing this event. What do you think? You want me to call you later to give you more information?” “Yes.” Okay, phone number. And I will call again and dedicate [time] to a one-on-one …and create that bond.” (Southern Host)
Another host explained how multiple contacts with participants were needed to try to secure a definitive RSVP. “The Latino community has a hard time when it comes to doing online registrations and also, you know, RSVPs. So, just keep that in mind that you're not gonna get people to RSVP, but they do show up,” (Western Host)
Others explained that punctuality is not a major concern for individuals when they attend events in the Hispanic community. “Culturally, timeliness is not embraced in many of the communities represented there. 11 o'clock might mean 11:30 or so, and that is really a cultural phenomena. So in order to get people there on time, it took a lot of effort...” (Southern Host)
RA Interviews
English-speaking research assistants noted discomfort with being unable to communicate with the research participants and needing to rely on the host. The RAs noted substantial improvements in both the flow of the events and the relationships between the event staff and the participants once Spanish-speaking RAs were hired, incorporated into the study team, and attending events. But you can definitely tell a difference in getting community buy-in and getting everyone to feel comfortable is like if someone can actually speak the language. And I think that’s one thing that I’ve heard from pretty much [all the RAs] after they’ve gone with someone that speaks Spanish to an event.” –English speaking RA
Interviews with the bilingual RAs demonstrated that they felt welcomed by the community and that their presence was appreciated. “Most people there didn’t speak English. So, once they learned that I spoke Spanish, then everyone felt a lot more comfortable. I think everyone was really happy to have us there and they all seemed really excited about the event. Yeah, it was a very welcoming community thankfully that I went to and I’m sure other people have different experiences, but I felt very included.”” – Bilingual RA
Additionally, English-speaking RAs noted feeling disconnected and uncomfortable when visiting Spanish-speaking communities without a Spanish-speaking team representative. I didn’t feel, to be able to really engage and to have to go through a host or their team members to communicate. I think it just showed, I don’t really know that I want to say lack of respect, but it wasn’t a good feeling [not having a Spanish-speaking team member present].” –English speaking RA
Discussion
Conducting effective community-engaged research requires a careful balance between respecting local, cultural-specific contexts, and maintaining interventional consistency across sites. While failing to respect community practices risks losing participants, having too much protocol variation across study sites risks loss of generalizability of the research findings. Our data provides important lessons for community-engaged researchers seeking to expand reach into Spanish-speaking populations.
First, our findings showed that despite the use of certified translation professional services to translate research materials from English to Spanish, additional considerations related to local dialects and cultural implications were necessary. In fact, even among our Spanish-speaking consultants was debated. We struggled to find a solution that ensured that the chosen use of language was appropriate for the participants’ local context without a need to continuously revise and re-tailor the tools and instruments for each unique site. We considered printing specific materials for each local dialect, but this was deemed infeasible due to the need to track and distribute unique materials across three arms for 15 different Hispanic communities. A more feasible resolution was to invite the local community hosts to review the materials, with special attention to the words that tend to vary across dialects so that they could point these out verbally during the event.
Second, our qualitative data reiterated the importance of personal connections between the research team and participants, particularly for a topic such as ACP that is deeply grounded in communication, trust, and relationships. Our community hosts pointed out that the absence of in-person Spanish-speaking research assistants felt inauthentic for a community-engaged project, with one host suggesting that this practice perpetuated the marginalization of Hispanic culture. Even though our preliminary analysis of qualitative data from the Hispanic participants themselves did not reveal these perceptions, our team took seriously the opportunity to diversify our team. We hired several part-time Spanish-speaking RAs to work on the project but acknowledge that it can be challenging to find bilingual assistants to support research. This highlights the need to increase the diversity of the research workforce to include bilingual individuals who can be part of community-engaged research. After adding in-person, bilingual RAs, both hosts and RAs reported a smoother flow of events, events that were more efficient, and improved experiences on the part of our English-only speaking RAs.
The FRAME reporting system allowed systematic reporting that will be useful for interpreting the final results of our trial. All modifications made to the interventions and to the implementation strategy were ‘reactive’ in nature (ie, made in response to a finding rather than pre-emptively). Even so, the changes remained fidelity-consistent and did not involve modifications of any core interventional elements, such as delivery method, intervention methods, etc. Our findings show that adaptation of non-core elements are equally important to the success of the interventions as the core elements, and thus to the integrity of the research itself. Identifying non-core elements is essential for, research conducted in real-world settings to maintain a careful balance of rigor and flexibility. Non-core elements refer to elements that are more flexible in nature, such as dialectical translations and adding bilingual Research assistants.
Finally, in response to challenges that we could not feasibly address in our research design (eg, concerns about using an RSVP system), it was important for our team to look critically at these challenges to determine what we could (and could not) accommodate. For example, while the RSVP system was difficult for hosts to implement because of cultural norms, eliminating the RSVP system altogether risked incurring substantial unnecessary expenditures should team members travel (often cross-country) to attend an event that may not have attendees. For this reason, we opted not to implement this modification, but noted that the RSVP system may not be reliable and made final travel arrangements accordingly.
Limitations include the small sample size and that the qualitative nature of the analysis does not allow for a systematic pre- and post-assessment of modifications from the same host (since hosts can only participate in a single event to avoid cross-arm contamination). Thus, we relied on research assistant perspectives and experiences to determine whether modifications resulted in improvements.
Despite these limitations, our experiences help to demonstrate some of the challenges of implementing research in Spanish-speaking communities on a national scale. Our work highlights the importance of having a strong community-based delivery model, attention to local dialects and cultural nuances, the value of a Spanish-speaking workforce, and the need to balance fidelity across national sites with adaptability in the conduct of rigorous research.
Disclosures
The Principal Investigator (LJV) is an unpaid scientific advisor for Common Practice, LLC, which is the company that designed the Hello game. The remaining authors declare that they have no competing interests.
The Project Talk Trial Collaborative Working Group Members
Lauren J. Van Scoy, MD, Samaa Ahmed, BS, Morgan Bucher, BS, Cindy Bramble, William Calo, PhD, JD, Vernon M. Chinchilli, PhD, Heather Costigan, BS, Lindsey Currin, MSc, Zuiry Ghatan, BS, Denise Grant, MA, Michael J. Green, MD, Christopher Hollenbeak, PhD, Kylee Kimbel, BS, Benjamin H. Levi, MD, PhD, Charu Maheshwari, MPH, Sara Marlin, MS, Terrence E. Murphy, PhD, Angela Novas, MSN, RN, CRNP, Allison M. Scott, PhD, Erika VanDyke, MPH, Emily Wasserman, MAS, and Amy Tucci, BS.
Footnotes
Acknowledgments
The study authors thank the Nick Jehlen at Common Practice, LLC (creator of the Hello game), Kate DeBartolo and Patty Webster, MPH and the team at The Conversation Project (an initiative of the Institute for Healthcare Improvement) and the team at TableTopics for their support of this project. We thank our safety monitoring committee members Jennifer McCormick, PhD, MPP and David Mauger, PhD and the John and Wauna Foundation for their support of the pilot work that led to this trial. We would also like to thank Dr William Calo’s team for aiding with discussion and subsequent translation modification. A thank you to Candace Bordner who was our outside qualitative interviewer for the RA interviews, Kate Ferguson who assisted with coding of the RA interviews, and Anna Costello who served as a bilingual research assistant for the project. Finally, we sincerely thank our hosts and research participants for their engagement and participation in this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the National Institutes of Minority and Health Disparities (5R01MD014141).