
Abstract
Keywords
Introduction
Approximately 1.4 million individuals in the United States suffer from hematological malignancies, a cancer of the bone marrow or immune system’s lymphatic cells. 1 Due to the complex and unpredictable nature of hematological malignancies, patients often require intensive therapies such as hematopoietic stem cell transplants (HSCTs), which, despite their curative potential, negatively impact morbidity, mortality, and overall prognosis. 2 Depending on the malignancy, patients may receive their own genetically altered (autologous) cells or those from a donor (allogeneic) through a marrow donation program. Hematopoietic stem cell transplants require myeloablative chemotherapy and radiation conditioning, with subsequent depletion and regeneration of bone marrow cells and then chronic immunosuppressive therapy. Allogeneic HSCTs are also often more unpredictable, with an increased risk for graft vs host disease (GVHD), infections and sepsis, high symptom burden, malignancy relapse, and lower quality of life (QOL). 3 Despite these potential consequences, evidence suggests that about 30% of hematologists report never referring patients to palliative care (PC) services for symptom and comorbidity management, goals of care, advance care planning, and treating psychological distress. 4
Palliative care is a relatively new medical specialty that grew from the 1960s hospice movement to incorporate aspects of end-of-life care into the standard treatment plan. 5 In 2006, the American Board of Medical Specialists and ten constituent specialty boards successfully approved the Hospice and Palliative Medicine board certification, which started in 2008. 6 Palliative care provides psychosocial, spiritual, and caregiver support for patients and their families, as well as pain and symptom management. Furthermore, evidence suggests that implementing PC may reduce costs per admission by 26%, reduce overall lengths of stay by at least two days, and lead to better QOL and higher quality care. 7 Early implementation has an evidence-based benefit for the patient; however, the combination of professional workforce demands and changes in cancer care delivery has made this evidence-based translation into practice complex. 8 Additionally, the unpredictable nature of hematological malignancies and HSCT complicates integrating a standardized referral program for PC and oncology collaborative care. 1 Unfortunately, patients undergoing HSCTs often experience acute and chronic physical and psychosocial complications, such as pain syndromes, increased frailty, and decreased physical performance, which impact QOL long after hospital discharge from an HSCT. 9
In current clinical practice, comprehensive PC referral systems are uncommon in the HSCT patient population despite the chronic comorbidities and side effects of HSCT that both patients and caregivers often experience. To our knowledge, there has yet to be an integrative literature review that evaluates and synthesizes the current literature on PC integration in the allogeneic adult HSCT populations. This review aims to address that gap by assessing the impact of PC on the adult HSCT standard of care; we have also examined the effect on patients’ QOL during the acute phase of allogeneic HSCT. This review defines the acute HSCT phase as inpatient hospital admission for conditioning, transplantation, engraftment, and symptom management.
Methods
This review utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 10 The search was conducted in March 2024 and did not limit articles by year parameters; however, if the articles were older than five years, they were assessed for relevance and pertinence to the review goals. The PubMed and CINAHL databases were searched for articles using MeSH terms “palliative care,” “stem cell transplant,” OR “stem cell transplantation,” “hematopoietic stem cell transplant,” and “early palliative care.” Inclusion criteria were adults >18 years old, available in English, PC-focused, and acute phase allogeneic HSCT-focused. Studies were excluded if they were case studies, protocols, or animal studies.
Results
Two blinded reviewers initially independently reviewed the results of the 488 titles, applying the eligibility criteria; any lack of consensus was resolved with a third reviewer. PubMed results initially yielded 411 articles from the MeSH search, and CINAHL yielded an additional 77 articles. Exclusion criteria were applied, yielding 95 total relevant abstracts for review. Thirty-eight articles were selected for full-text analysis, yielding 19 relevant articles for this review (see Figure 1). Prisma flow diagram.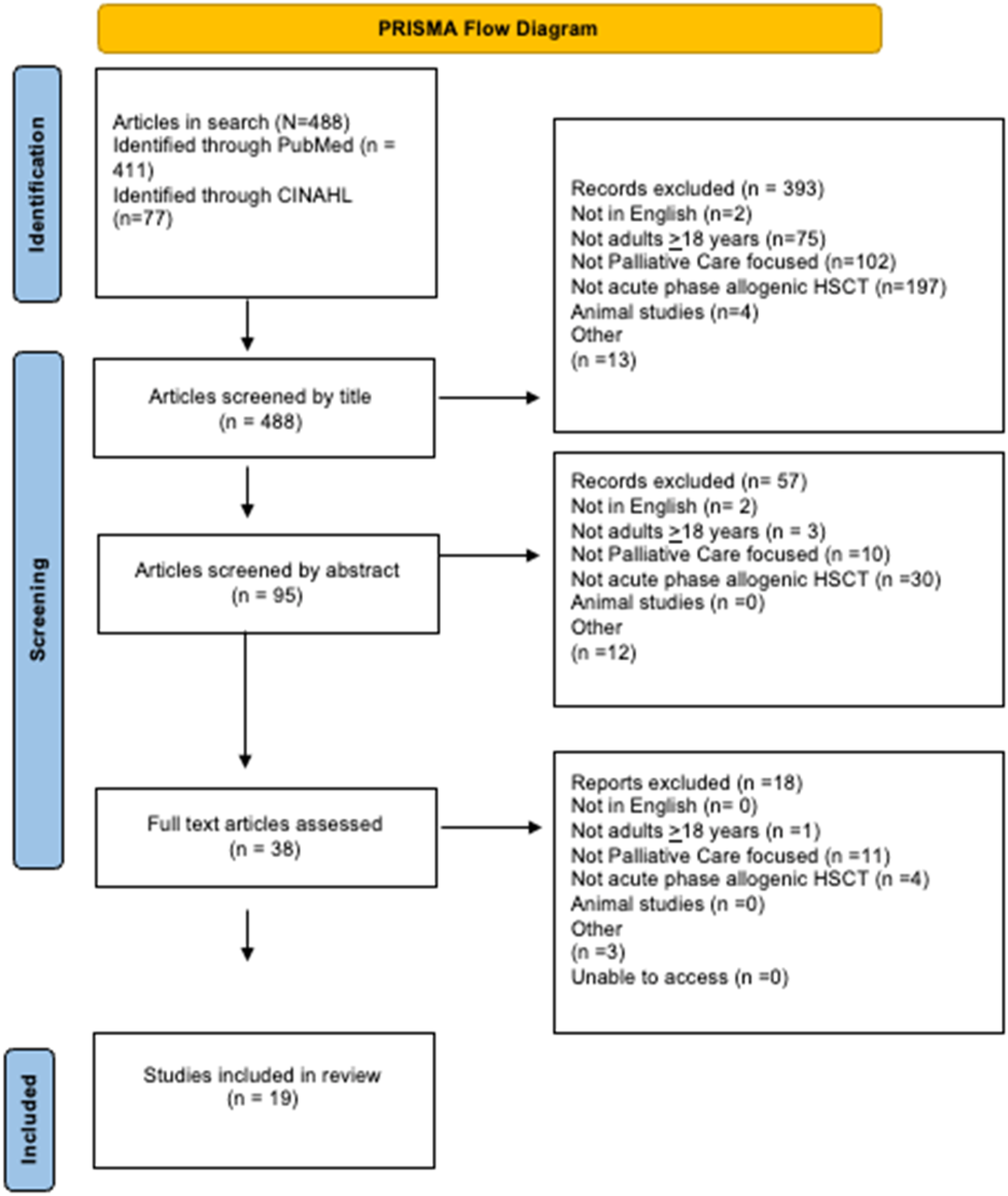
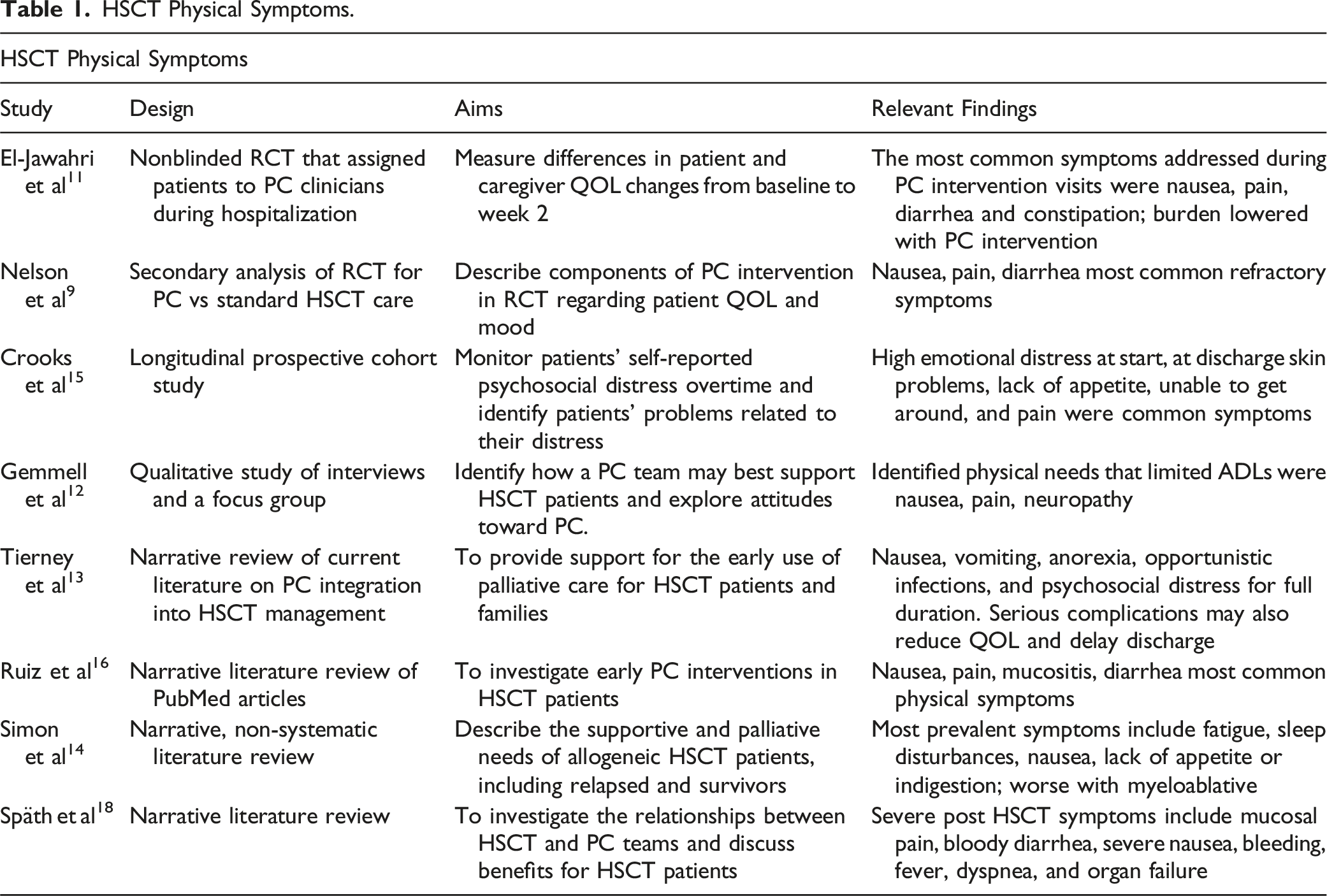
HSCT Physical Symptoms.
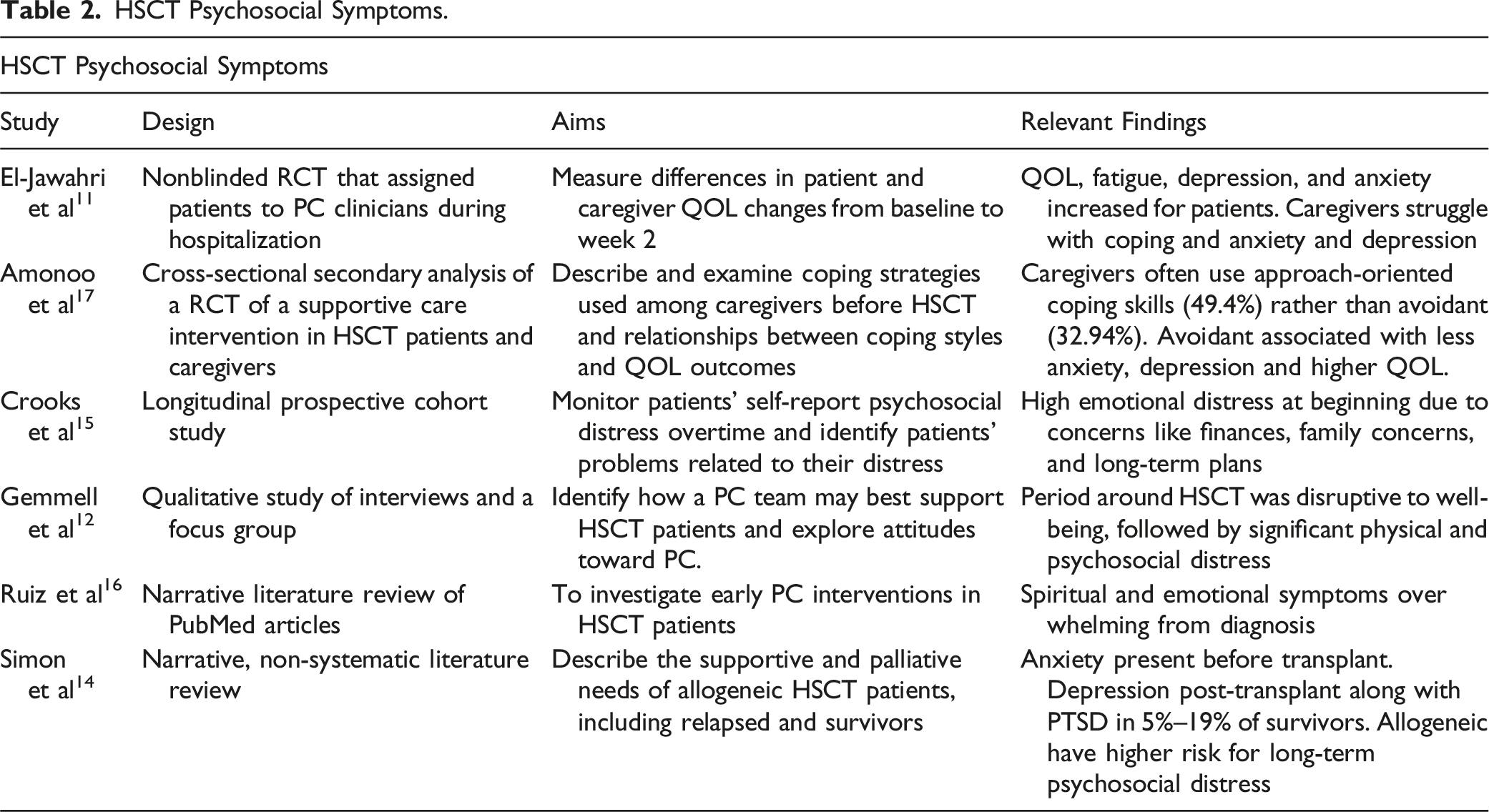
HSCT Psychosocial Symptoms.
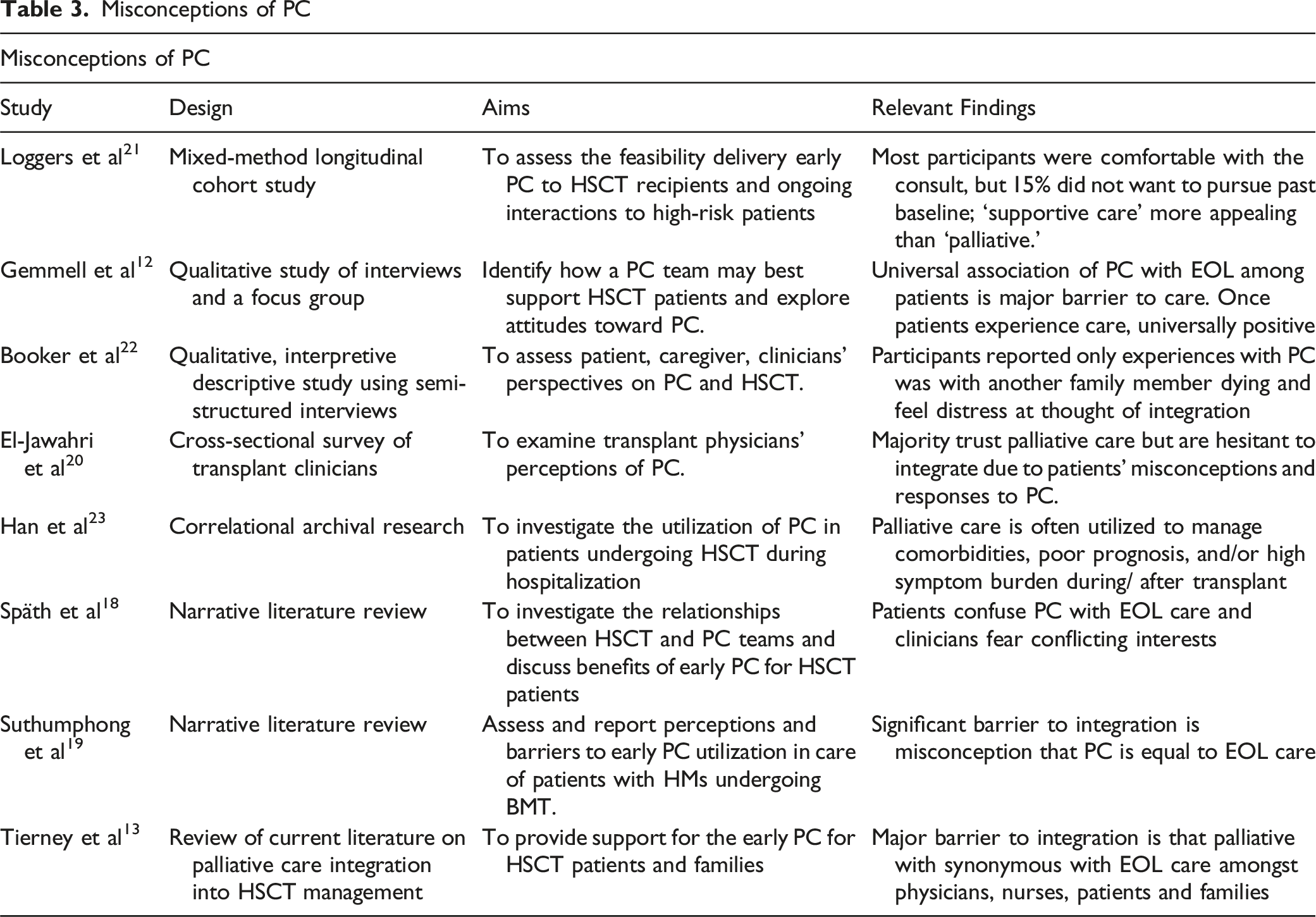
Misconceptions of PC
Palliative Care Integration and Quality of Life.
Early PC Integration and HSCT
Physical and Psychosocial Needs
The first theme deduced from this literature review indicates that HSCT recipients undergo significant changes in both physical and psychosocial needs (Tables 1 and 2). In the RCT conducted by El-Jawahri et al, 11 the most common symptoms that were addressed during PC intervention visits were nausea (initial PC visit 69.9%, subsequent visits 69.8%), pain (initial PC visit 65.4%, subsequent PC visits 53%), diarrhea (initial PC visit 53.1%, subsequent PC visits 38.1%) and constipation (initial PC visit 55.6%, subsequent PC visits 12.7%). The impact of these burdensome symptoms is further described in the qualitative interview study by Gemmell et al 12 in which the responses of HSCT patients indicated that refractory physical symptoms such as pain and nausea became debilitating and contributed to worsening mental health during HSCT. Additionally, Nelson et al 9 investigated the topics and management of HSCT supportive care measures through a secondary analysis of a previous RCT conducted by El-Jawahri et al. 11 Nelson et al 9 concluded that nausea, pain, and diarrhea were the most common symptoms during HSCT and required various treatment approaches by HSCT providers. For example, 50% of PC management of nausea during HSCT was managed by medication, 39% by counseling, and 0.3% by referral to other services. 9 Fatigue and insomnia were often addressed at PC consults and continued throughout HSCT. 9 In contrast, constipation was addressed during consults (53%) and week 1 (29%) but often needed to be discussed at weeks 3 or 4 (4% and 9%, respectively) post-transplant. 9
However, the severity and combination of physical symptoms may vary amongst patients. Additionally, Tierney et al 13 diagramed the progression of side effects of HSCT, starting from the conditioning regimen to recovery, in which symptoms such as nausea, vomiting, anorexia, opportunistic infections, and psychosocial distress may last the duration of treatment and well into recovery. In the acute phase, serious complications such as sinusoidal obstructive syndrome (SOS), diarrhea, kidney injury, integumentary toxicities, and mucositis may also delay recovery and reduce overall QOL at discharge. 13 The severity of symptoms may depend on the intensity of the treatment (ie, myeloablative vs reduced-intensity conditioning), which not only further complicates anticipatory therapy but increases the symptom burden and coping strategies for both patients and caregivers during the long HSCT process. 14
Psychosocial
According to Crooks et al, 15 patients experience significant psychosocial symptoms throughout the transplant experience. In fact, 71% of patients self-reported emotional problems before transplant, and psychosocial distress surrounding care, such as finances and long-term care plans, were significantly debilitating to well-being. 15 Ruiz et al 16 corroborated these findings through a literature review and deduced that spiritual and emotional well-being concerns are overwhelming from diagnosis for patients. The authors found that up to 18% of patients experienced a religious/spiritual struggle during HSCT. 16 The systematic review conducted by Simon et al 14 on allogeneic HSCT and PC integration indicated that anxiety, depression, and PTSD are highly prevalent during the HSCT acute phase. Psychological distress was among the most prevalent symptoms in patients undergoing allogeneic HSCT, with PTSD regarded as a primary concern in about 5% to 19% of HSCT survivors. 16 Ultimately, patients experience significant psychosocial distress that impacts their overall well-being before HSCT and progresses over time.
The psychosocial consequences of HSCT also concern caregivers, as they are essential participants in patient care after discharge from the hospital. Simon et al 14 found that caregivers experienced symptoms of depression, such as fatigue, insomnia, weight loss, and changes in social life. Additionally, Amonoo et al 17 conducted a cross-sectional analysis of data from 170 caregivers of HSCT recipients to assess coping strategies and mental health. The authors concluded that caregiver psychosocial distress may highly depend on the type of coping strategy utilized during HSCT. For example, avoidant coping was associated with more anxiety and depression symptoms, while approach-oriented coping often yielded higher QOL outcomes. 17 Overall, the authors suggested that caregivers and patients may benefit from coping strategy education during HSCT to prevent negative coping habits that would further decrease QOL. 17
Misconceptions of PC
Another theme identified through this review is that gross misconceptions of PC by patients, caregivers, and providers are significant barriers to integrative care (Table 3). Unfortunately, patients, clinicians, and family members often equate PC with end-of-life care and are frequently hesitant and distressed at the thought of integrating into HSCT care.12,13,18,19 In a cross-sectional study to examine transplant physicians’ PC perceptions, El-Jawahri et al 20 found that while most clinicians trust PC, they are often hesitant to integrate into their care due to concern for causing distress due to these misconceptions. There is also a concern for conflicting interests between oncologists and PC providers, and patients are also often unwilling to transition to palliative topics in the context of the curative HSCT treatment plan.18,19 The term ‘palliative care’ may be a barrier for PC integration, whereas ‘supportive care’ is more appealing when presented to patients.20,21 However, once education was provided on the benefits of PC integration, patients and families were often open to counseling and almost universally reported positive experiences.12,22
While PC rates have increased, Han et al 23 found that PC is more commonly considered for allogeneic HSCT recipients with higher comorbidities burden, acute changes in patient status, and poor prognosis rather than for QOL management before HSCT. Patients with higher odds of post-transplantation complications such as GVHD are more likely to receive PC to manage complex care planning. 23 This may lead to a further misconception of the impact PC has on QOL, as patients receiving PC are statistically more susceptible to poorer prognosis and outcomes when, in fact, the significant decline in QOL is what prompts providers to refer. 23 Overall, these findings further suggest how ongoing educational efforts by clinicians on the benefits and goals of PC may reduce a significant barrier to PC integration in the HSCT patient population.
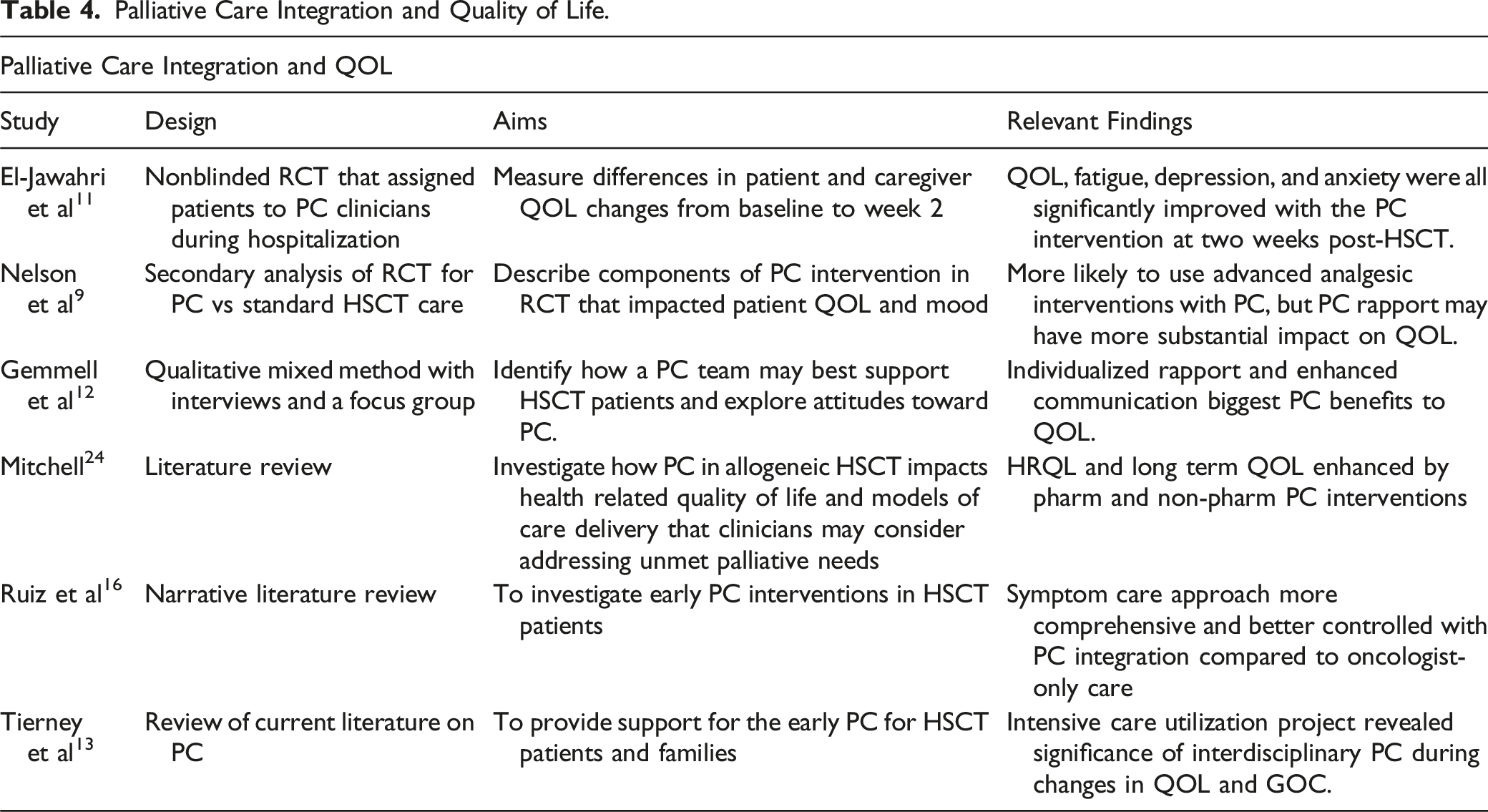
PC Integrations and QOL
The literature further revealed that pharmacologic components of PC integration into HSCT correlate with improved QOL over time (Table 4). El-Jawahri et al 11 demonstrated that QOL, fatigue, depression, and anxiety were all significantly improved with the PC intervention at two weeks post-HSCT. Intervention participants also reported lower symptom burden increases during HSCT (P = 0.03). They were less likely to develop anxiety and depression symptoms (P < 0.001 and P < 0.001, respectively). They reported decreased anxiety symptoms from baseline at week 2 of the intervention (mean change 1.12, P = 0.03). 11 Nelson et al 9 identified that patients were more likely to receive more comprehensive physical symptom management, such as patient-controlled analgesia or standing orders for supportive care. Additionally, Ruiz et al 16 found that the pharmacologic symptom care approach is more comprehensive and better controlled with the addition of PC providers, suggesting a need for interdisciplinary pharmacologic care.
However, nonpharmacologic PC approaches correlate with long-term impactful outcomes for HSCT recipients. According to Nelson et al 9 and Gemmell et al, 12 HSCT patients’ QOL significantly benefits from rapport and enhanced communication with PC clinicians. These PC components provide support and community and aim to empower patients to participate in PC-specific lifestyle interventions. 12 Nelson et al 9 concluded that the pharmacological interventions from PC did not significantly impact QOL, so the authors suggested that the rapport between PC clinicians and patients and caregivers may substantially impact QOL. 9 Tierney et al 13 also concluded that patients with complex symptoms and psychosocial concerns will benefit from interdisciplinary palliative care to help facilitate ongoing ACP and GOC conversations, especially if patients require intensive care to provide families with more counseling and support. In the literature review by Mitchell, 24 the author suggested that PC interventions that promote exercise and rehabilitation, yoga, meditation, and nonpharmacologic management of fatigue, nutrition, and mood enhance health-related quality of life. Combining PC-guided effective symptom management and coping strategies may improve physical functioning, emotional well-being, mood, and spiritual well-being, ultimately contributing to enhanced QOL. 24
Early PC and HSCT
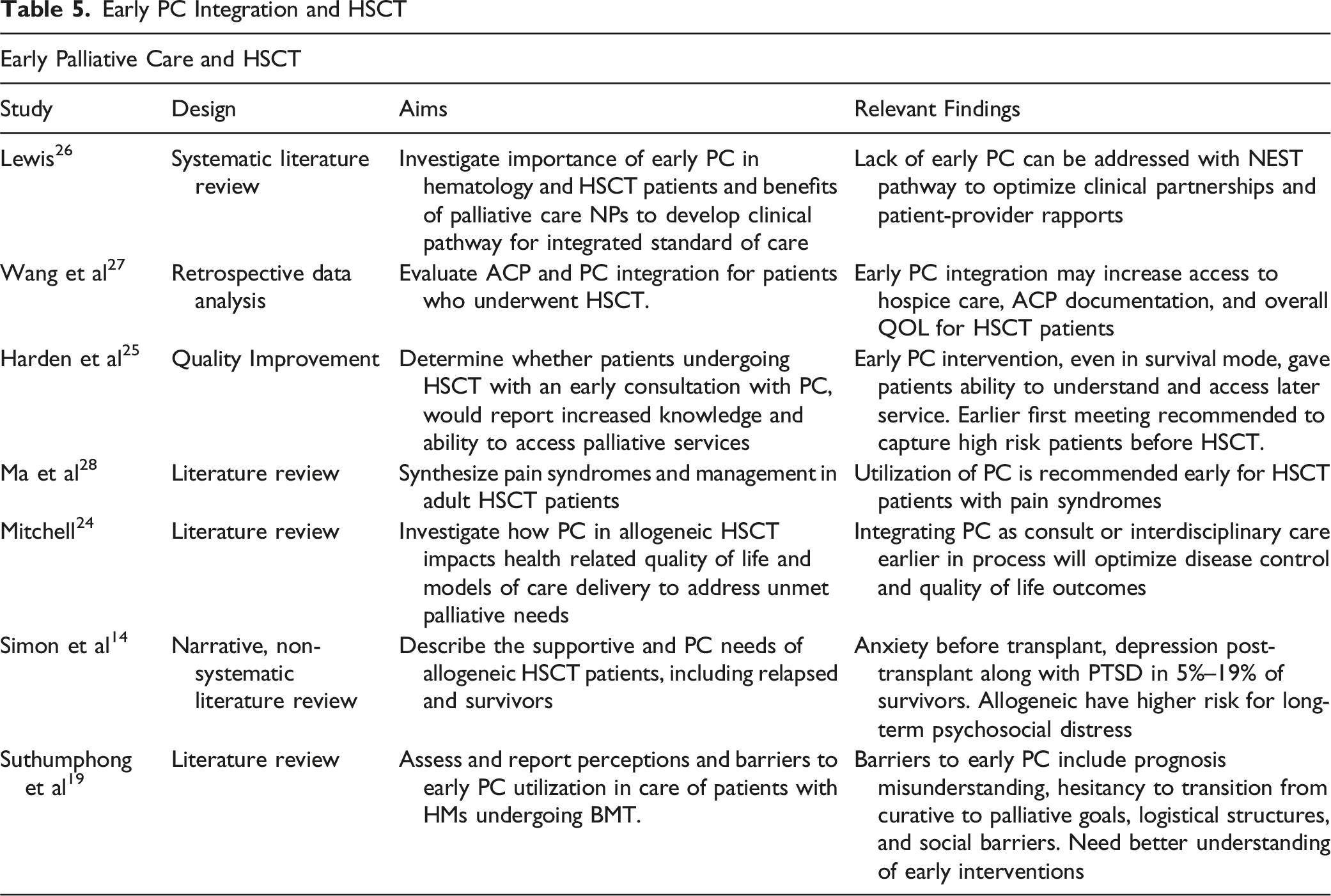
The final theme identified in this review regards the timely integration of PC into HSCT care (Table 5). Overall, implementation of early PC is infrequent in HSCT, with only about 1.95% of HSCT recipients receiving early PC. 14 The optimization of early PC integration has been investigated throughout the literature. Harden et al 25 implemented a PC Early Access Project Team to promote PC integration throughout the HSCT experience. The PC team reported that patients were often overwhelmed in the initial consultations and had difficulty retaining the information due to the stress of impending HSCT. The providers suggested that patients were likely in survival mode, so the timing of the first meeting for PC is delicate. The conclusion was that earlier introduction to PC for high-risk patients may reduce HSCT barriers that hinder well-being and QOL discussions during admission. 25
Additionally, Lewis 26 proposed the Nurse Practitioner-Delivered Early Palliative Care for Stem Cell Transplants (NEST) pathway to optimize early PC implementation to enhance care delivery by utilizing PC Nurse Practitioners. While this model may ideally foster clinical partnership and decrease provider stress and burnout, it automatically uses more resources than a trigger-based model. However, it may be challenging to implement depending on the transplant center size, patient acuity, and the number of providers required. 26
While Lewis 26 proposed that optimization would be achieved through systemic clinical partnership, Mitchell 24 concluded that the workforce demand is a barrier to early PC and favored a trigger system for referral. Triggers may include patients with significant or refractory symptom burden, multiple comorbidities, and significant psychological distress or limited coping. 24 While problematic in that there is a need for further education on triggers for PC, the trigger system may lead to improved QOL through PC integration without burdening the workforce and ultimately preserve the quality of care and provider well-being over time. 24
In addition to contrasting implementation models, there are barriers to early PC that are unfortunate characteristics of the HSCT process. Simon et al 14 characterized the objective (disease-related unpredictability) and subjective (perception of PC, reducing patients’ hope, unrealistic expectations, and collaborations) factors of hematologic malignancy that discourage providers from referring before HSCT and hurt the efficacy of the trigger system. 14 Ultimately, to optimize a trigger system, there is a need for an objective, ongoing assessment that may flag potential triggers for referral and integrate early PC without burdening or disrupting the workforce while still providing HSCT recipients with proper and timely PC care.
In addition to structural barriers to early PC integration, physicians and patients hesitate. In the review by Suthumphong et al, 19 the authors found that providers often hesitate to refer to PC due to their relationships with patients and caregivers. Although referral is often intended to complement curative therapies, patients and caregivers may not be willing to discuss palliative goals during curative therapy. 19 Ultimately, PC is an essential adjunctive service for oncological care in the complex management of difficult cases, so providers must consider the benefits of encouraging PC supplement therapy to encourage comfort, well-being, and prognosis understanding along with the curative goals of treatment.19,27 This is especially important when patients begin to experience HSCT complications. For example, the review by Ma et al 28 endorsed early PC in managing peri-transplantation pain complications such as oral mucositis and pain to appropriately titrate the best regimen for QOL and well-being while these syndromes persist. 28 Furthermore, Tierney et al 13 explained that the HSCT might often consult PC for high-risk patients with a complex history (ie poor coping, pain syndromes, substance misuse, etc.), which may not be as effective if consulted later in the HSCT process. The evidence endorsing early PC integration into the HSCT standard of care suggests that there is a need for an objective understanding of the timing of triggers during HSCT to optimize patient benefits without jeopardizing the structure of hematologic malignancy or HSCT care algorithms.
Discussion
Overall, the consensus from this evidence suggests that interdisciplinary PC during HSCT enhances the quality of care.9,11-13,23,24 This review was limited in that the eligibility of studies was restricted to English only, and pediatric patient populations were not involved. Additionally, only the acute phase of HSCT was considered for review, so the long-term impact of integrative PC was not investigated. While these may have narrowed the results, the themes that were generated from this review provide implications for guiding future practice in both PC and HSCT specialties. HSCT’s physical and psychological consequences are significant life-altering for the healthiest HSCT candidate and indicate the need for extra supportive care that PC integration may provide.9,11,14,24 The historic misconceptions of PC by patients, providers, and the community highlight the need for ongoing education on the goals and benefits of early PC integration, especially for patients with chronic, advanced illnesses, such as HSCT recipients.19-22 The debate of a trigger-based model versu a standardized referral system is an ongoing hurdle to the proper PC integration into the HSCT. However, the discussion of this evidence further exemplifies the need to identify unmet palliative needs earlier so that PC may be integrated before the severe consequences of HSCT.24,26 Unfortunately, patient, provider, and institutional barriers have hindered universal early PC integration into HSCT care; therefore, ongoing education and palliative care needs assessments to demonstrate the breadth of unmet PC needs within this patient population are needed in future work.14,25
Conclusion
The results from this literature review suggest a need for a better understanding of unmet palliative needs in HSCT recipients. Because earlier PC may mitigate the acute and chronic consequences of HSCT, it would be beneficial to utilize palliative care needs assessments to identify unmet needs sooner. Therefore, future work is needed to use palliative care needs assessments during the acute phase of transplant to objectively determine the unmet palliative needs and initiate a referral so patients may benefit from the comprehensive, collaborative care that a PC integration may provide.
Footnotes
Acknowledgments
We acknowledge Jamie Conklin, MLIS for her advice and assistance with the literature search.
Author Contributions
Abigail C. Short. Conceptualization, Investigation, Formal Analysis, Methodology, Writing- original draft and review and editing. Mika Kuroki. Formal Analysis, Writing Review and Editing. Lorinda Coombs., Analysis, Methodology, Writing Review and Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.