
Abstract
Aims
Akathisia is a disturbing, reversible but under-diagnosed extrapyramidal side effect of medications used in palliative medicine. We assessed patients’ subjective experience of akathisia and response to procyclidine, an anticholinergic used to treat extrapyramidal effects. We also aimed to discuss future areas of research and alternatives to akathisia-causing medications.
Methods
Suitable patients were retrospectively identified by palliative medicine physicians in a tertiary hospital and a chart review was undertaken. Information gathered included the account of their experience of akathisia, use of inciting medications, treatment, and outcome.
Results
20 patients were identified, 12 females, 8 males. Mean number of days on the inciting drug(s) to onset of akathisia symptoms was 18.1. Mean number of days from commencing inciting drug(s) to diagnosis was 20.9. Patients’ descriptions revealed similarities including feeling “locked in” and a need to constantly move. One patient described a “glass coffin” enclosing her. 16 patients had full response to treatment with procyclidine, 3 had partial response requiring up-titration of dosing, response was not documented in 1.
Conclusions
Akathisia is an elusive symptom that can have dramatic reversibility when treated. Lack of recognition causes unnecessary patient suffering. Procyclidine appears to aid diagnosis and be an effective treatment. Protocols to reduce incidence and guide diagnosis and management are proposed. Further studies are required, in which subjective outcome measures are used and medications to treat akathisia are studied. Recognition remains challenging, causing significant distress for palliative patients, for whom quality of life is paramount.
Introduction
Medication-induced akathisia is an extrapyramidal (EP) movement disorder defined by the American Psychiatric Association 1 as “subjective complaints of restlessness, often accompanied by observed excessive movements”. It is felt that the inner sensation of restlessness is the primary feature, and the motor features are an attempt to manage this. 2 Akathisia has been shown to cause dysphoric symptoms such as depression, irritability, and panic. 3
Akathisia is believed to be mediated primarily through an imbalance between dopaminergic and serotonergic/noradrenergic neurotransmitter systems. 4 It is most closely linked with the neurotransmitters gamma-aminobutyric acid (GABA), which influences dopamine-dependent signalling, and serotonin. 4 Therefore, it is associated with medications which affect these, most notably D2 dopamine receptor antagonists. 4 Classically, akathisia has been primarily associated with antipsychotics, but it also occurs with antiemetics and antidepressants. 5
It is a common side effect of antiemetics which act on the D2 dopamine receptors, with one study stating its incidence in patients receiving antiemetics during chemotherapy as 50%. 6 Despite this, it is under-diagnosed. Hirose 7 has put forward several reasons for this. Patient factors included: lack of apparent motor restlessness, no voluntary expression or clear communication of inner restlessness, restlessness in body parts other than the legs, confounding psychiatric signs, or the absence of other EP signs. For example, in the study mentioned above, 75% of the patients with akathisia stated they would not have self-reported the inner symptoms of akathisia. 6 Clinician attitudes that may contribute to under-diagnosis were: emphasis on objective restlessness, failure to consider akathisia during therapy with akathisia-causing drugs, failure to fully implement anti-akathisia measures in ambiguous cases, and strict adherence to research diagnostic criteria.
There is limited evidence on the overall incidence of akathisia in the palliative care population. In a palliative care setting, restlessness is often attributed to a myriad of other causes such as terminal agitation or anxiety, therefore akathisia may not be considered. 8 Strict adherence to diagnostic criteria is also particularly noteworthy in relation to palliative care. The Barnes 9 Akathisia Rating Scale (BARS) for diagnosing drug-induced akathisia consists of both subjective and objective criteria and requires the patient to stand for a period of time. In a palliative care setting, or at end of life (EoL), patients are often unable to perform the objective portion and therefore would not meet diagnostic criteria. In one cross sectional study examining the incidence of EP side effects in a specialist palliative care inpatient unit, only 12.5% of participants were able to stand for sufficient time to complete the BARS. 10 Clinicians working in palliative care may therefore need to be flexible with their assessments and wary of more unusual presentations. A case has been reported of a bed bound man approaching EoL who developed abnormal rubbing and twisting motions of his limbs, which settled after stopping haloperidol. 11
When reviewing the literature in preparation for this article, we found no reports including the patients’ own words or description of their subjective experience. By listening closely to patients’ histories and asking specifically about restlessness, some of the issues described above can be addressed. Giving the patient a voice is vital, especially in palliative care when quality of life is the most important outcome. 12
The mainstay of management of medication-induced akathisia is the reduction in dose of the inciting medication(s), cessation of some or all of these medications, or switching to an alternative with lower risk. 13 In addition, several other medications have been used. These include beta-blockers (eg, propranolol), anticholinergics (eg, procyclidine, benztropine and biperiden), 5-HT2A antagonists (eg, mirtazapine or trazodone), benzodiazepines (eg, clonazepam) and vitamin B6. 13 These have shown variable success.13,14 The evidence for any of these treatments is limited. 13 Regarding non-pharmacological measures, it has been shown that distraction maneuvers reduced motor symptoms in 65% of patients with akathisia. 2
Anticholinergics have been widely used to treat EP side effects; however, Cochrane reviews in 2002 and 2012 studying the use of anticholinergics for the treatment of neuroleptic-induced acute akathisia, found no relevant randomized control trials comparing anticholinergics with placebo. 14 We again found none during our literature review, conducted in 2023. Procyclidine is utilized in our service to treat akathisia due to the senior investigator’s experience of its use. 15 Procyclidine is a synthetic anticholinergic which inhibits the excitatory effects of acetylcholine at the muscarinic receptor. 16 It has an oral bioavailability of 75%, 16 with autonomic effects at a maximum within a half-hour after administration by the intravenous (IV) route and one to two hours after oral delivery. 17
Our aims when undertaking this review were to draw attention to the importance of akathisia as an under-recognised side effect of commonly used antiemetics, highlight the subjective experience of patients suffering from akathisia, examine the effectiveness of procyclidine in its management, and discuss possible future areas of research.
Methods
Over a 7-year period between 2015 and 2022, patients were identified during reviews by the palliative medicine team in a tertiary referral hospital as having developed akathisia secondary to antiemetics. A literature review of the subject of akathisia was undertaken. Ethical approval was granted for the study by the local ethics committee, and information was gathered by undergoing a chart review of each case, including age, gender, diagnosis, treatment, and outcome. The use of medications known to cause akathisia was recorded, including drugs used, durations and doses. Time from initiation of inciting medication(s) to development of akathisia and subsequently the time to diagnosis was also recorded. The management of akathisia was also recorded.
The patients’ description of the sensation in their own words was documented, which on reviewing the literature, is unique to this study. Information was recorded anonymously using a proforma developed for the study and inputted into the spreadsheet software NumbersTM (version 12.1), which was used to analyze data.
Results
Twenty patients were identified in total, twelve female, eight male, median age 61 years. Nineteen patients had malignancy, twelve had metastatic disease. The inciting medications identified are outlined in Figure 1. These include single agents, or combinations of antiemetics used either simultaneously or sequentially without a break between them. Of the fourteen cases where metoclopramide was a inciting medication either alone or in combination with another drug, it had been used at a maximum dose of 30 mg/24hrs in five (35.7%), 60 mg/24 hrs in eight (57.1%) and 80 mg/24 hrs in one (7.1%). Of the eight cases where haloperidol was an inciting medication either alone or in combination, it had been used at a maximum dose of 5 mg/24 hrs subcutaneously (SC) in four (50%). Of the seven cases where levomepromazine was used in combination with other drugs, it was used at a maximum dose of 18.75 mg/24 hrs SC in two (28.6%) and 25 mg/24 hrs SC in one (14.3%). Inciting medications.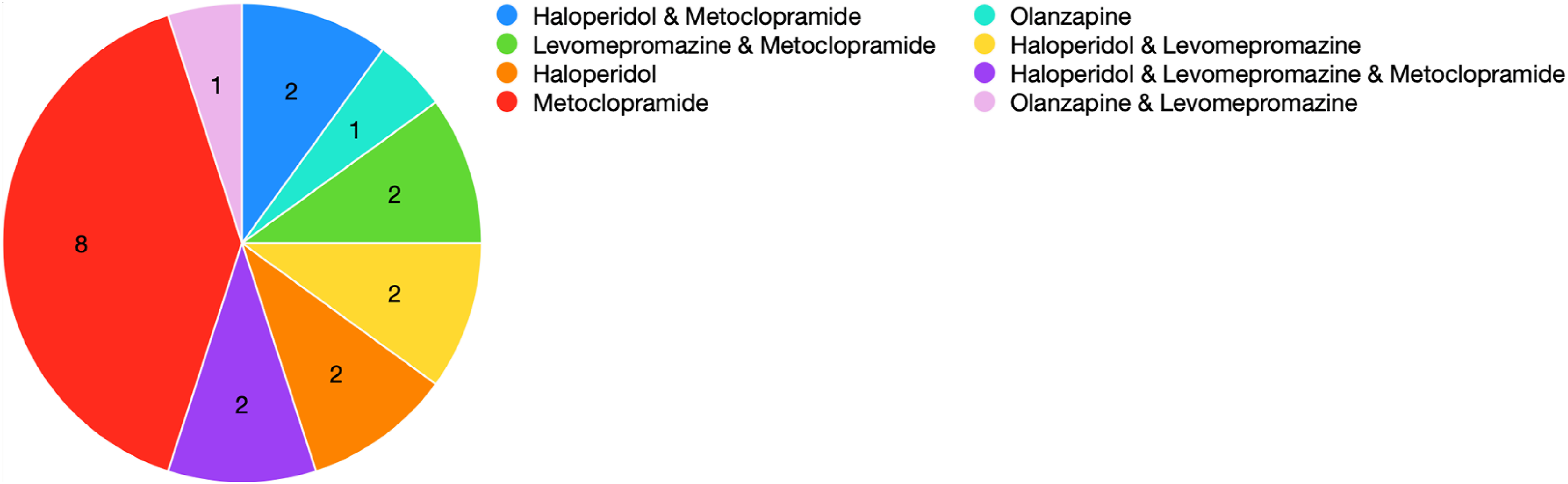
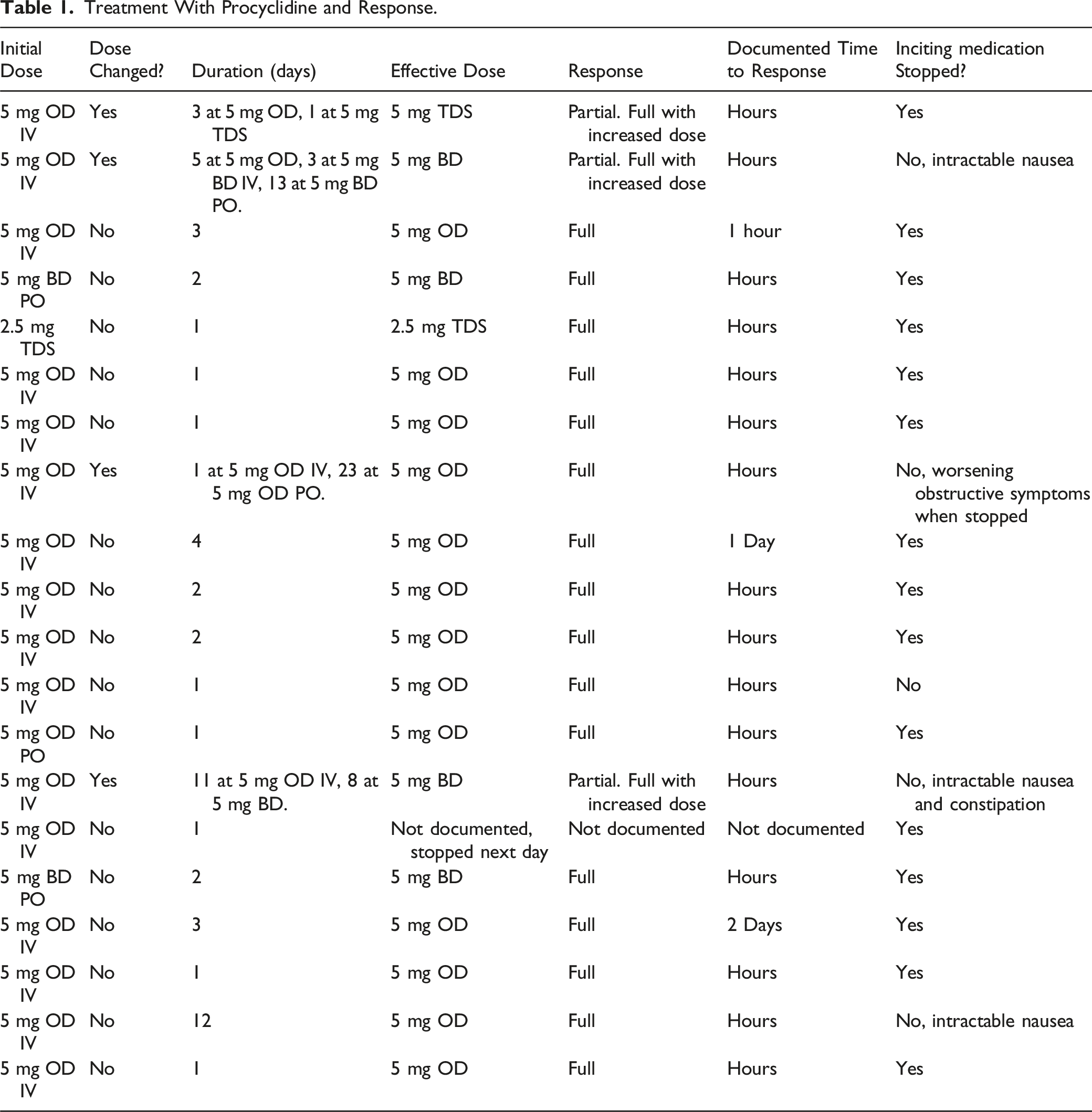
Treatment With Procyclidine and Response.
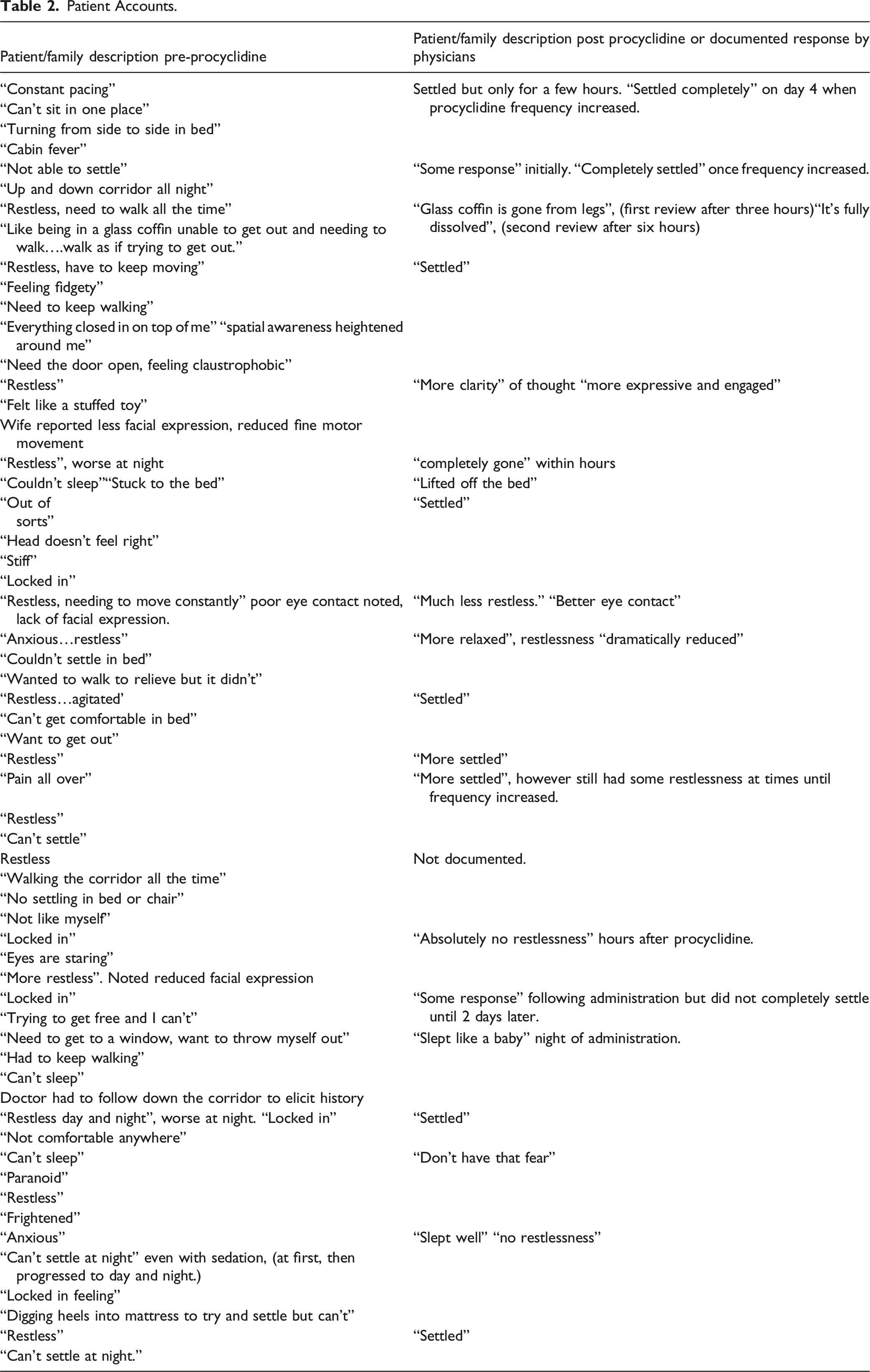
Patient Accounts.
Discussion
Akathisia is a common but often under-recognised side effect of antiemetics and antipsychotics commonly prescribed in palliative medicine. This is shown by the delay in diagnosis noted in our review, and results in unnecessary suffering. As expected, using relatively higher doses of these medications for extended periods of time appeared to increase the risk. Using combinations of antiemetics which can cause akathisia will also increase the risk of its development. It is recommended that wherever possible, a single anti-emetic should be used. 18 Careful history taking by clinicians and being alert to patients’ changing behavior is vital to diagnose this uncomfortable and distressing condition. Including patients’ first-hand accounts of their experiences may inspire readers to be more aware of the possibility of akathisia in their clinical practice.
Antiemetics and Akathisia
Despite common use of drugs causing EP side effects in the palliative care setting, it is sometimes felt that doctors in these settings may not be fully aware of these side effects. 19 Antipsychotics are often used as antiemetics in these settings eg, levomepromazine, olanzapine or haloperidol due to their effective suppression of stimulation of the chemoreceptor trigger zone (CTZ). 20
Haloperidol is one of the most common medications prescribed at EoL, both for its antipsychotic effect in delirium and its anti-emetic effect. 21 A study examining outcomes arising from the use of haloperidol for delirium in a hospice setting found that the incidence of akathisia relating to haloperidol was 11%. 22 A separate Australian study examining 100 terminally ill patients who developed akathisia calculated that exposure to haloperidol conferred an increased risk, with an odds ratio of 18.4. 23
Haloperidol has greatest affinity for D2-receptors amongst commonly used anti-emetics, along with prochlorperazine and droperidol, 24 suggesting an increased risk of EP side effects. There is incomplete evidence for the use of haloperidol for nausea and vomiting in palliative care. 25 Our service uses haloperidol as a third line anti-emetic drug because of its potential to cause extrapyramidal side effects. Regarding treatment of delirium, cognisant of recent research indicating no benefit to using haloperidol vs placebo, 26 and demonstrating increased mortality with haloperidol vs placebo, 27 we concentrate on treating the cause of delirium, as recommended by reviews of delirium management in palliative medicine. 28 We try to avoid prolonged use of haloperidol for either indication, if necessary limiting use to seven to ten days.
Olanzapine has been demonstrated as an effective antiemetic and is available as an oral dispersible tablet, making it easier to ingest. 29 This may be an option as a first-line antiemetic when suppression of the CTZ is required, as it has less affinity for the D2-receptor, 24 and therefore a lower risk of EP side effects than haloperidol or metoclopramide, which are often used in these settings. Olanzapine can also cause appetite stimulation and weight gain which may help patients with anorexia-cachexia syndrome. 30 However, we note that there is still a risk of akathisia with atypical antipsychotics as demonstrated by olanzapine being an inciting medication in two of the patients in this series.
As delayed gastric emptying has been shown to be a common cause of vomiting and the anorexia-cachexia syndrome, 31 the prokinetic metoclopramide is commonly prescribed in oncology or palliative care patients. It is known to cause akathisia. 32 There has been a report of metoclopramide-induced akathisia causing such significant distress that the patient attempted suicide. 33 For patients that require a prokinetic long-term, domperidone is preferred because of its inability to cross the blood brain barrier. 34 Care is suggested with continuation of metoclopramide longer than seven to ten days.
Diagnosis and Treatment of Akathisia with Procyclidine
In our practice, the initial dose of procyclidine was utilized as a test to confirm the diagnosis. The IV route was favored where possible, to ensure absorption as nausea and vomiting was a feature of all patients, and to elicit a rapid response. Procyclidine can cause side effects such as urinary retention, xerostomia, constipation, cognitive impairment, agitation, or in the most severe cases, psychosis.16,35 This is also true of other anticholinergics more often used in EoL care eg, hyoscine hydrobromide. 36 Prolonged use should be avoided if possible, therefore it is best to discontinue the inciting medication.
This series, while small and uncontrolled, has suggested that akathisia may be managed effectively with low doses of procyclidine. There were no adverse effects documented in this retrospective review. Procyclidine appears to be effective both as a treatment and prophylaxis if akathisia-causing medications are continued. A limitation of this study, however, is the possibility that the placebo effect may have played a role in patients feeling subjectively improved post-procyclidine, particularly after the explanation of the treatment. Future controlled trials are required to investigate the effectiveness of procyclidine more conclusively for this indication, as well as that of other treatment options described above.
Protocols to Avoid and Manage Akathisia
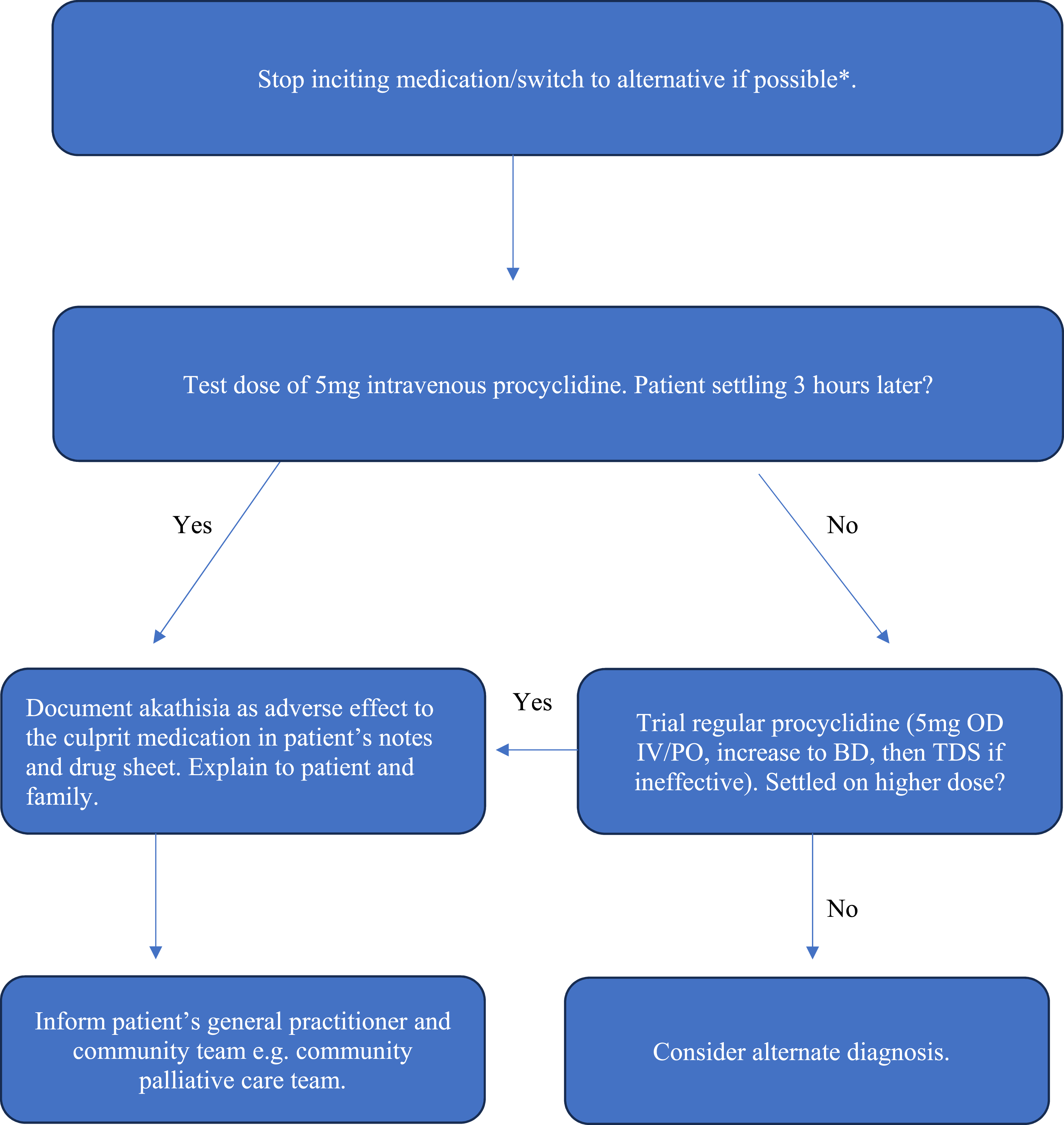
Protocols were developed to reduce the risk of EP side effects, and to guide management of suspected cases of akathisia secondary to medications, as seen in Figures 2 and 3. Protocol to reduce risk of EP side effects. Protocol to Manage EP Side Effects. *Eg, metoclopramide to domperidone, haloperidol to olanzapine. If not possible to stop culprit medication or switch to alternative, consider regular procyclidine eg, 5 mg OD PO for duration of treatment with culprit medication. Increase frequency if required. Monitor for side effects.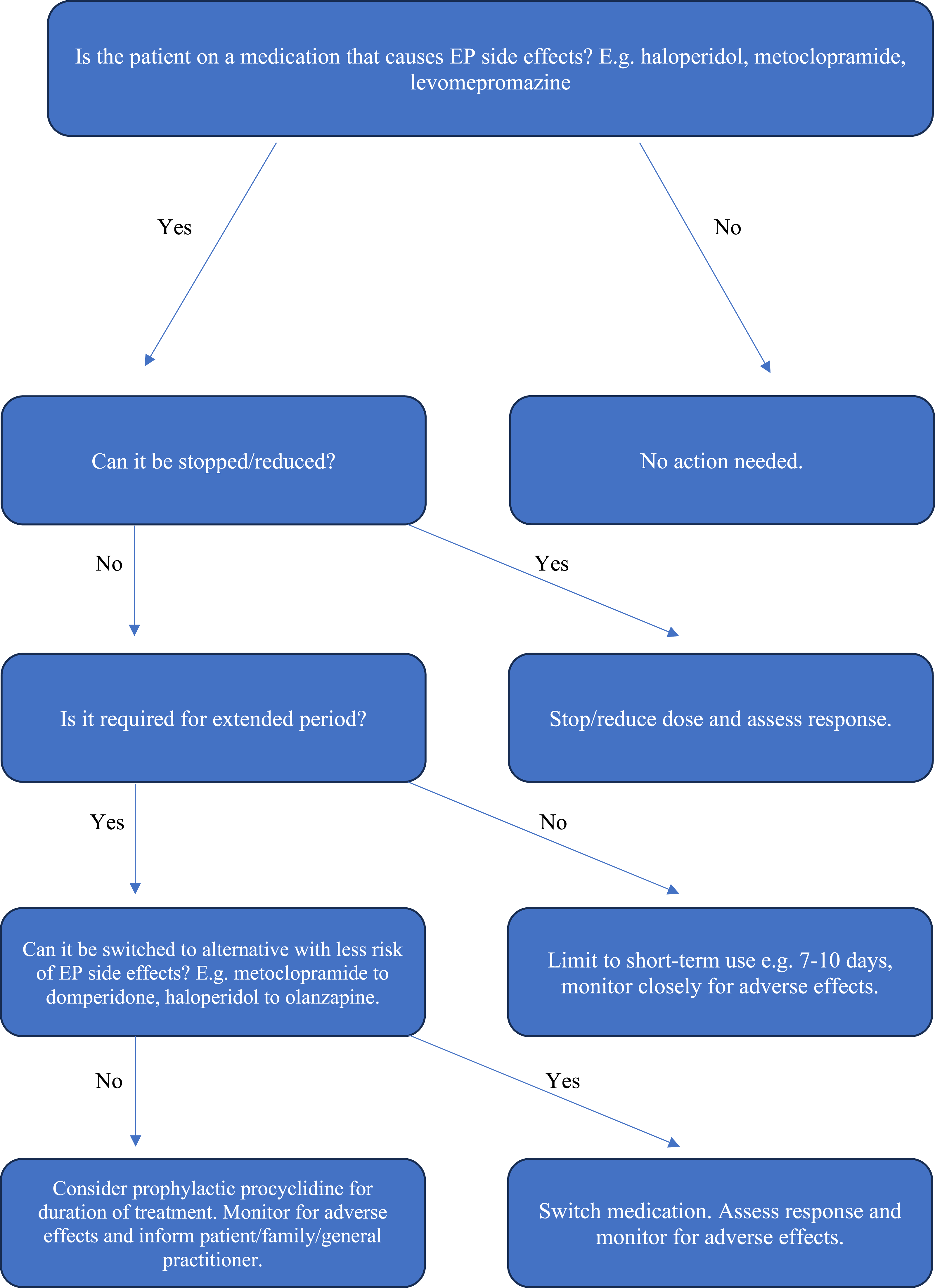
Subjective Outcome Measures for Future Studies of Akathisia
There is a need to develop future studies on akathisia and its most effective treatment options.13,14 However, outcome measures that are used need to address the patient’s perspective. Traditionally, QoL is assessed using self-reported Health Related Questionnaires, 37 which may miss more the unusual symptoms caused by akathisia. Use of validated subjective measures of QoL may assist in early diagnosis of akathisia.38,39 Future studies of akathisia should incorporate such patient-centred outcome measures which address the effect of symptoms on the patient.
Awareness of Extrapyramidal Side Effects
The prevalence of EP side effects needs increased awareness. While acute dystonias are usually immediate and clear in diagnostic certainty, akathisia is more insidious and difficult to diagnose. Prolonged D2-receptor antagonism can proceed to iatrogenic reversible parkinsonism and ultimately, irreversible tardive dyskinesia. 40 Misdiagnosis of these conditions can therefore lead to intense, avoidable suffering.
While our department is particularly careful with akathisia-causing medications and have attempted to reduce their use, there are instances where it is unavoidable. Currently, many of our antiemetic options may lead to EP side effects. It is imperative that further studies are undertaken to examine the effectiveness of future alternatives. Further studies are also required to definitively establish effectiveness and safety of medications to treat EP side effects.
Akathisia and other EP side effects are an underappreciated burden for palliative care patients. However, with increased awareness and vigilance on our behalf as physicians, these side effects can be identified early and managed effectively.
Footnotes
Authorship Statement
DM was lead author. DM and SM undertook the literature review. DM, SM, GK, SL, RM, MB, TMc were involved in collecting data. DM, EM and DW developed the discussion points. DW conceived of the article and oversaw the project. All authors were involved in editing the article.
Author Note
An early version of this case series was presented as a poster at the Irish Association of Palliative Care Research and Education Seminar in February 2022.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research and authorship of this article. They gratefully acknowledge that open access publication was made possible by a generous donation from the Mayo/Roscommon Hospice Foundation.