
Abstract
Introduction
Most patients with terminal illnesses prefer to receive care at home in their last 6 months of life. 1 With a growing older adult population in Hong Kong with longer life expectancy, there has been increasing recognition that the tertiary healthcare system may struggle to meet older people’s end-of-life needs. 2 A systematic review identified the necessity of developing end-of-life care services in primary healthcare settings in Hong Kong to address the increasing need that was not met in the tertiary sector. 3 Home-based end-of-life care has garnered substantial global attention in recent years, 4 as it implements person-centered care and encourages medical-social cooperation to ensure the delivery of appropriate care for older people. 5 Home-based end-of-life care serves patients with an estimated prognosis of 12 months or fewer, 6 whereas hospice care typically targets those with a shorter life expectancy of ≤6 months. 7 Hospice care was provided by a team of medical nurses, social workers, chaplains, home care aides, and volunteers, 8 and home-based end-of-life care also employs an interdisciplinary approach. With the backup of medical services, it is possible to provide end-of-life care for clinically stable patients with short life expectancies at home. 9 Home-based care offers a new way of caring for terminally ill individuals and their family caregivers (FCs), allowing them to receive or provide care in comfortable and familiar environments, especially when this enables them to avoid hospitalization and institutional care.
FCs may need to be substantially involved in home-based end-of-life care and face significant challenges; however, their preparedness for caring for end-of-life patients at home is often presumed and over-estimated.10,11 They may need to undertake numerous unfamiliar roles, including providing different types of direct care, coordinating resources, and being care planners.12,13 They may need to manage physical symptoms, provide psychosocial support, assist with financial matters, communicate with medical staff and social care providers, and help to fulfill patients’ unfinished business, such as making wills. Research has indicated that caregivers of end-of-life patients reported experiencing more physical difficulties and facing greater challenges in decision-making than other caregivers. 14 FCs who independently cared for homebound older adults or patients with advanced cancers experienced a higher care burden.15,16 Even with other family members’ support in caregiving, managing family relationships and complicated family dynamics can challenge FCs in rapidly changing and distressing circumstances.4,17 Demoralization is a common experience for FCs, and being well-prepared for their complex roles could help lower their care burden.11,18
Although multiple randomized controlled trials have demonstrated the effectiveness of home-based end-of-life care in managing patients’ symptoms,4,17 these patient-oriented models recognized FCs primarily as caregiving partners for formal caregivers rather than as secondary service recipients.4,19 Nursing skills and other caregiving training could enhance FCs’ role instrumentally,4,19 but their individual needs are often overlooked, such as personal difficulties in adapting to the caregiving role. Negative caregiving experiences or perceived care burdens may suppress FCs’ role functionality, 20 which could further compromise patients’ benefits from home-based end-of-life care models. 21 Given the importance of sustaining home-based end-of-life care, it is essential to address FCs’ psychological distress as well as patient care. 22 However, evidence of the effectiveness of the family-centered, home-based end-of-life care model is scant.
End-of-life caregiving at home by FCs can be a relational experience, as FCs are physically and emotionally connected with terminally ill patients and often prioritize patient’s needs over their own.13,23 FCs’ psychological well-being could fluctuate with the patient’s physical health, pains, mobility, and disease trajectory. 24 Open family conversations related to illness have been shown to contribute to fewer symptoms of depression or prolonged grief disorders in FCs. 25 Enhancing FCs’ sense of connectedness through appreciation from other family members and effective communication with healthcare professionals24,26 can mitigate the negative effects of FCs’ caregiving. 27 Primary caregivers for end-of-life patients are usually spouses and adult children, and they have different characteristics and strengths and adopt heterogeneous strategies to cope with caregiving challenges. 28 Further research is necessary to investigate the relational experience in end-of-life caregiving and to differentiate the focus of providing interventions for spousal and adult-children caregivers.
The Integrated Community End-of-life Care Support Team (ICEST) model represents a shift from a patient-oriented to a family-centered care approach. In the patient-oriented model, the primary focus was on providing physical, psychosocial, spiritual, and practical care for terminally ill individuals, with no active interventions for their caregivers or families.29,30 This ICEST model has established a seamless referral system that enables the medical staff of tertiary hospitals to discharge and then refer appropriate end-of-life patients to the community-based interdisciplinary service team. The ICEST, comprising doctors, nurses, social workers, personal care workers, and volunteers, follow up and support community-dwelling patients with terminal illnesses and their FCs promptly. The team uses an iterative “assessment-planning-intervention” cycle to actualize person-centered, needs-driven, home-based care. Ongoing assessments identify the needs of families at critical transition points throughout patients’ disease trajectories, such as disease exacerbation, significant changes in family functioning, or insufficient social support. Assessments inform the choice of interventions tailored to patients’ and FCs’ needs. Besides comprehensive patient care, the family-centered model empowers FCs through psychoeducation, counseling, and caregiving skill training and fosters constructive dynamics through family communication, conferences, or activities.
Methods
Study Design and Participants
The ICEST model is an element of the service model of the Jockey Club End-of-life Community Care (JCECC) project. This paper aims to evaluate the ICEST model’s effects on FCs and explore its differential effects on spousal and adult-children caregivers. The study was a prospective, cohort, multicenter evaluation. The Human Research Ethics Committee of the University of Hong Kong approved the study (Reference No.: EA1902039). Written consent was obtained from participants to join the study.
The purposive sample was identified and referred by medical staff in the palliative care, oncology, medicine, and geriatrics units of partnered hospitals in Hong Kong. Patients should be 60 years or above, have a life expectancy of 12 months or less, and prefer living at home. FCs were included in this study if they were: (1) aged 18 years or above; (2) the primary FC; (3) communicated in Cantonese; (4) had no cognitive deficits; and (5) were not receiving other formal community services for older adults or caregivers.
Data Collection
The ICEST team contacted the patients or their family caregivers, processed the intake, conducted clinical assessments, and arranged service provision based on the individual needs of each case once they received the referrals. They collected demographic information and outcome measures of end-of-life patients and their FCs through in-person interviews during home visits between Jan. 2019 and Dec. 2021. Repeated outcome measures were conducted at baseline (T0) and 3 months after the service commencement (T1). Assessment at T1 was not applicable if care recipients died before T1. This paper focuses on FCs’ outcomes before the patients’ death, including caregiving strain, depression, worries about patients, perceived social support, intimate relationships with patients, and family agreement on treatment/care plans.
Measurements
FCs’ demographic characteristics included age, gender, educational level, employment status, chronic illnesses, type of relationships, and co-residence with patients. Variables related to care demands included extra care duties for other family members, availability of other FCs as helping hands, and the caregiving tasks they undertook (ie, physical, practical, medical-related, psychosocial, and financial support). The intensity of involvement scored on a 5-point Likert scale (0 = “not at all” to 4 = “always”).
Caregiving strain, depression, and worries about patients were measured by the Chinese version of the modified caregiver strain index (C-MCSI), patient health questionnaire-2 (PHQ-2), and an item from the integrated palliative outcome scale (IPOS), respectively. The C-MCSI with excellent internal reliability (Cronbach’s α = .91) 31 contained 3 subscales of perception of caregiving, empathetic strain, and adjustment demands. 32 The PHQ-2 with good internal reliability (Cronbach’s α = .76) 33 was scored 0 to 6. The IPOS item on worries about patients was rated from 0 (“not at all”) to 4 (“always”) 34 Perceived support on practical concerns and information provision, intimate relationships with patients, and family agreement on treatment and care plans were rated from 0 (“insufficient/very distant/great disagreement”) to 4 (“very sufficient/very intimate/consensus reached”).
Statistics
Descriptive statistics summarized sample characteristics. Differences in characteristics between sub-groups were tested using χ2 tests for categorical variables and independent-sample t-tests for continuous variables. Paired t-tests analyzed changes in caregiving strain, psychological distress, and relational conditions between T0 and T1, and Cohen’s d indicated effect sizes. Generalized linear models (GLM), a repeated measures analysis, assessed changes in outcomes of spouse and adult-children caregivers over time, and a pairwise comparison was used to detect differences between these 2 groups at T0 and T1. The cases that completed the assessments were included for analysis, and P-values <0.05 indicated statistical significance. Data analyses were conducted in IBM SPSS 27.0.
Results
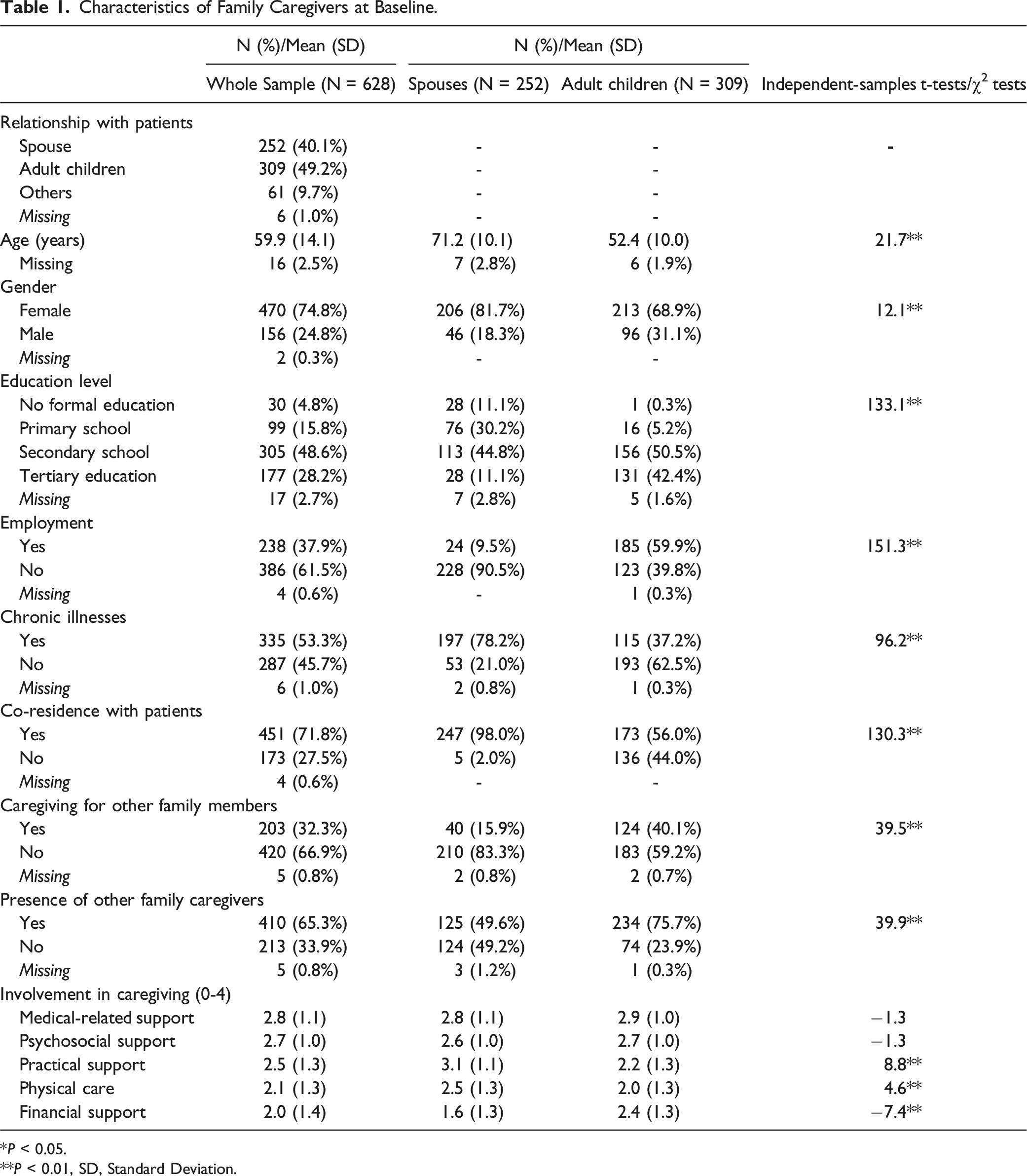
There were 251 of 628 FCs enrolled in the evaluation completing both T0 and T1 assessments (Figure 1). Except for education level, FCs completing T1 and drop-outs had no significant differences in characteristics (Suppl Table 1). As Table 1 showed, FCs’ mean age was 59.9 (SD = 14.1), and 74.8% were female. Around 80% of them had completed secondary education or above. FCs mainly comprised patients’ spouses (40.1%) and adult children (49.2%). Almost all spouses lived together with terminally ill patients, as did 56.0% of adult children. Spouses were older, less well-educated, and poorer in health, while more adult children handled tasks and extra care duties for other family members. Adult children were more likely to have other family members available as supporting hands in caregiving. Spouses and adult children had no significant difference in their involvement in medical and psychosocial support. However, spouses provided more physical and practical support, while adult children offered more financial assistance. Flowchart of participants.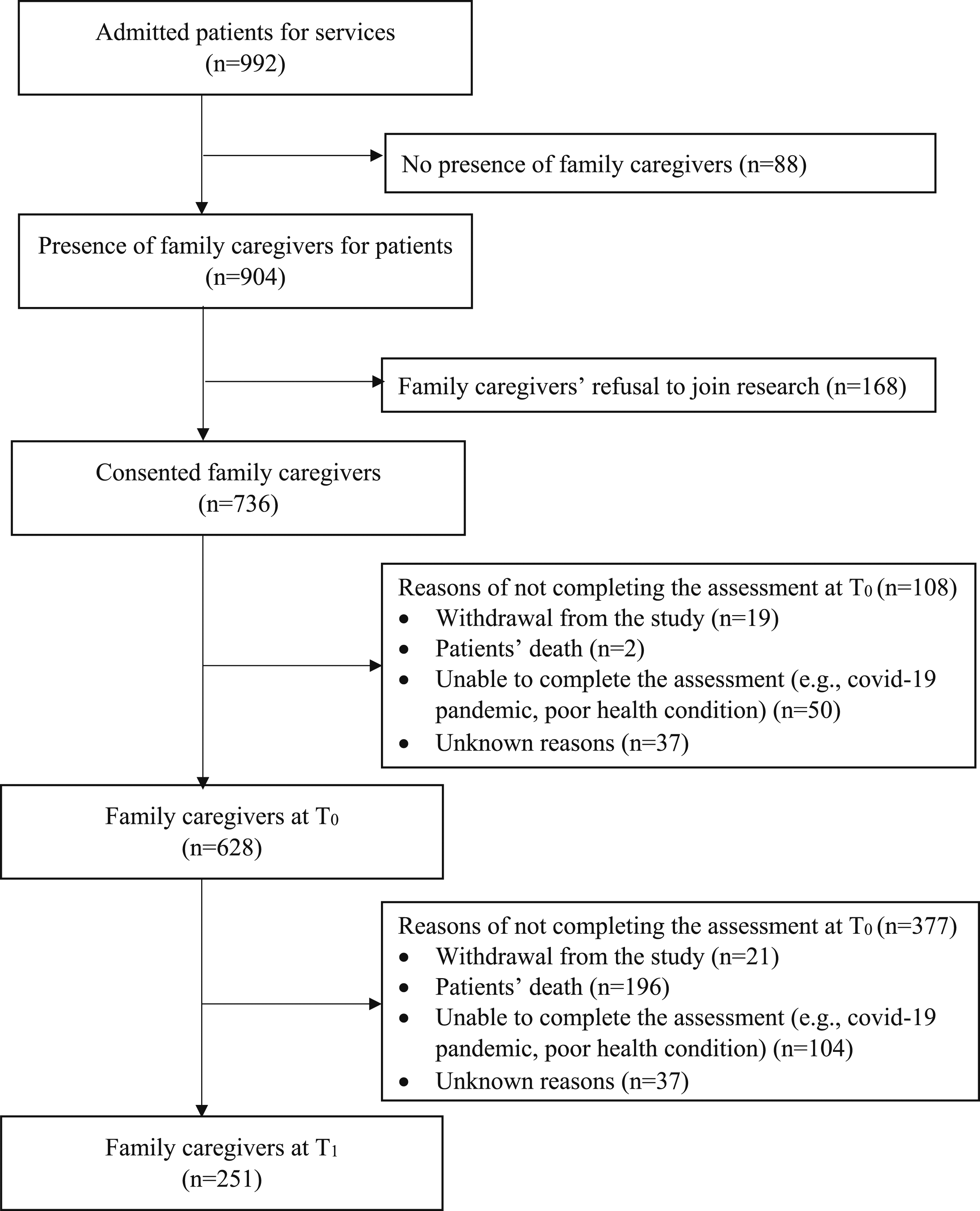
Characteristics of Family Caregivers at Baseline.
*P < 0.05.
**P < 0.01, SD, Standard Deviation.
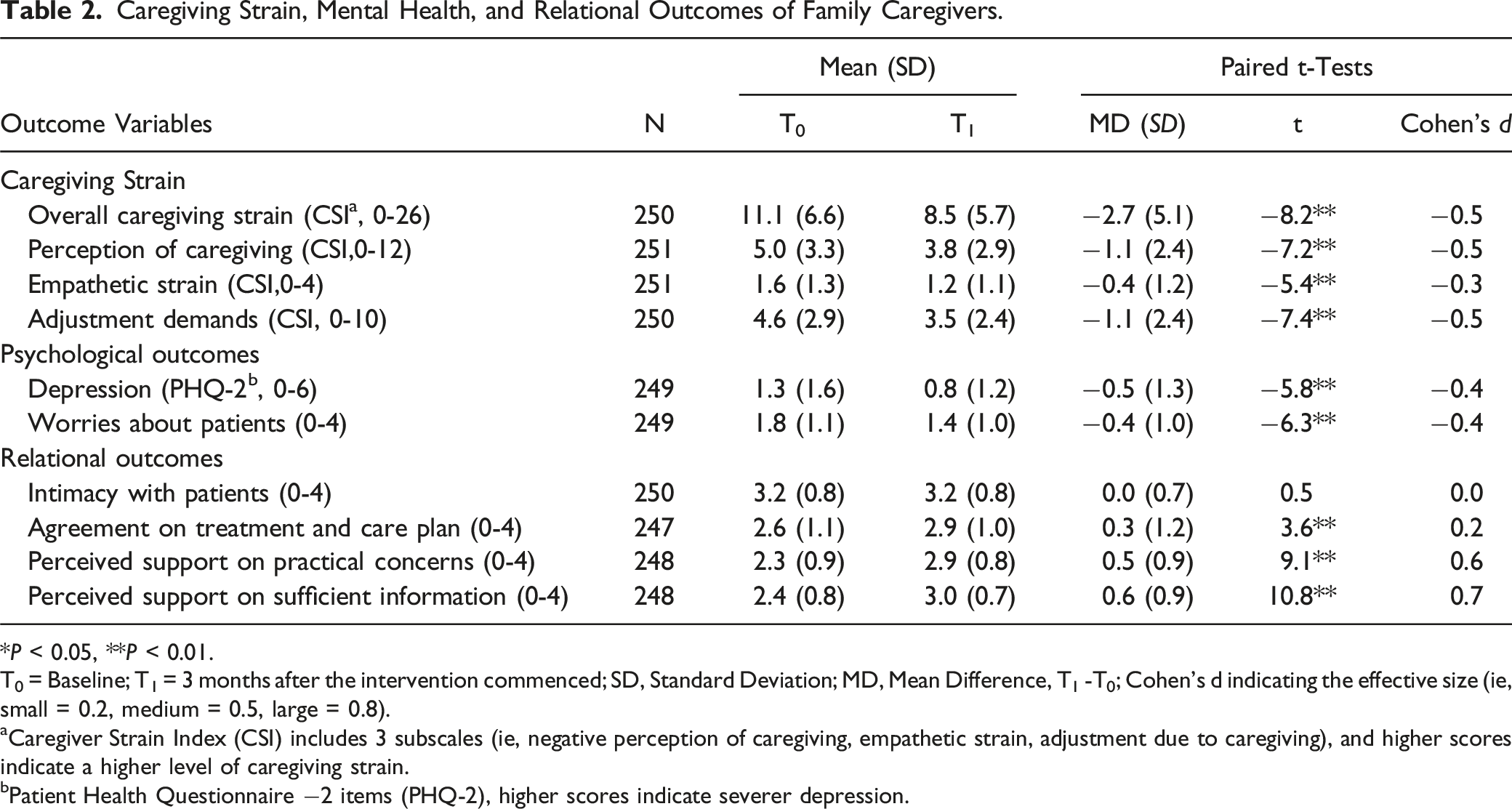
Caregiving Strain, Mental Health, and Relational Outcomes of Family Caregivers.
*P < 0.05, **P < 0.01.
T0 = Baseline; T1 = 3 months after the intervention commenced; SD, Standard Deviation; MD, Mean Difference, T1 -T0; Cohen’s d indicating the effective size (ie, small = 0.2, medium = 0.5, large = 0.8).
aCaregiver Strain Index (CSI) includes 3 subscales (ie, negative perception of caregiving, empathetic strain, adjustment due to caregiving), and higher scores indicate a higher level of caregiving strain.
bPatient Health Questionnaire −2 items (PHQ-2), higher scores indicate severer depression.
Difference in Caregiving Strain and Mental Health Within and Between Spouses and Adult Children.
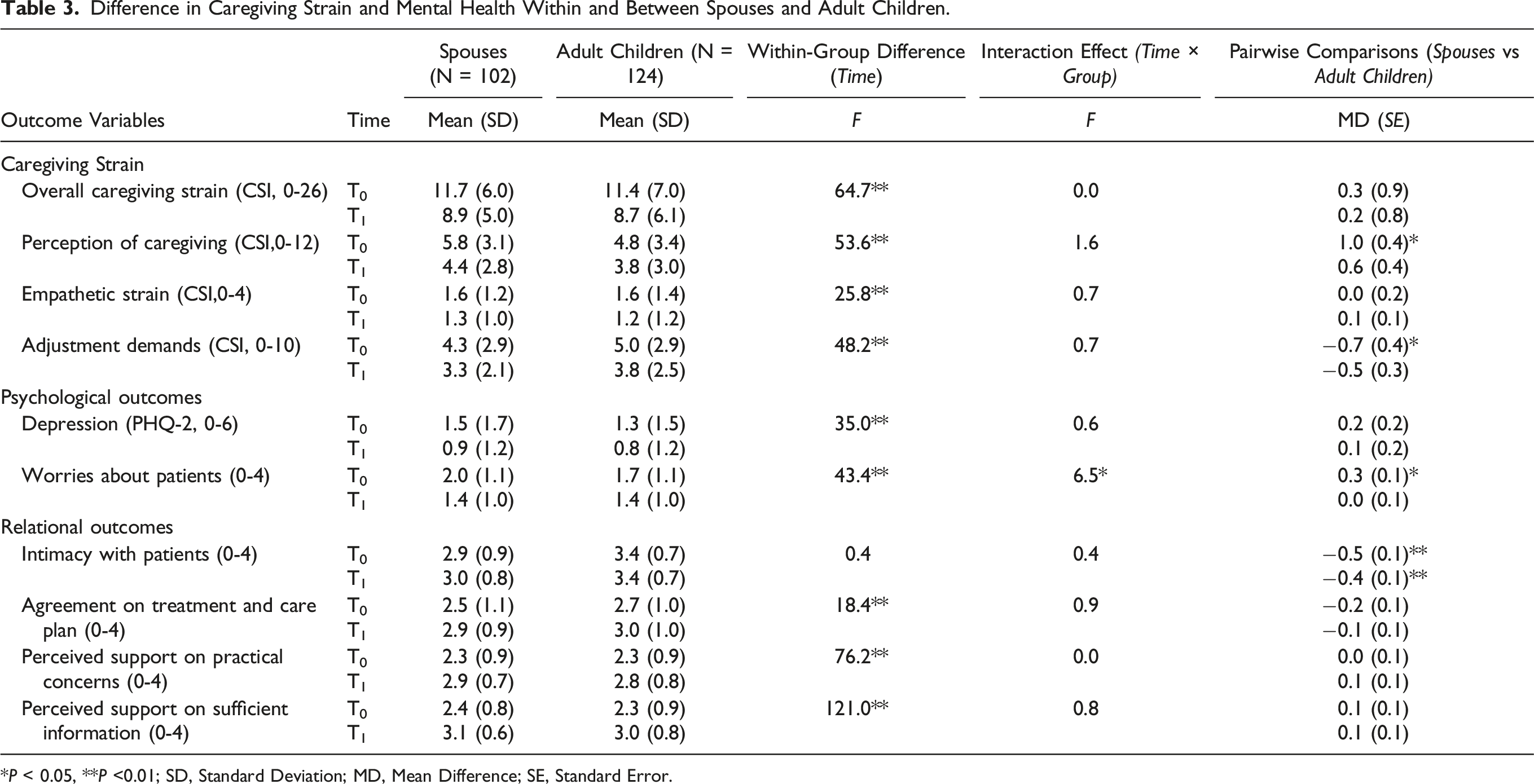
*P < 0.05, **P <0.01; SD, Standard Deviation; MD, Mean Difference; SE, Standard Error.
Discussions
This is the first paper to report the impact of the family-centered home-based end-of-life care model (ie, the ICEST model) in Hong Kong on FCs’ outcomes and relationship experience. This study advanced the understanding of end-of-life care from a family system perspective. Caregiving strain for spouses and adult children was reduced, albeit in different dimensions. The critical finding upon which to tailor future strategies for caregiver support might further improve the effectiveness of home-based end-of-life care.
From Patient-Oriented to Family-Centered Care
Our study indicated that a family-centered approach effectively reduced caregiving strain. The effect size of reduced adjustment demands was twice that reported in the patient-oriented model, 30 which suggests the family-centered ICEST is more effective in reducing caregiving strain than the individual care approach. Caregiving strain was associated with the need to adapt to the changes and disruptions in their lives as caregiving demands increased. Research also indicates that FCs’ caregiving strain is not static but dynamically changes based on disease trajectories, caregiving intensity, and availability of external supports.35,36 The ICEST model recognized and addressed FCs’ challenges, including adapting to multiple new roles, maintaining connectedness with patients and others, and self-isolation due to fear of burdening others. 23 The model used a multi-pronged approach to adjust for caregiving strain. The ongoing assessments identified the family’s needs and monitored the patient’s condition. Intensive support was provided during critical transitions, and continuous capacity building for FCs was achieved through practical support, skills enhancement, and psychosocial counseling to facilitate their role adaptation.
Psychological Distress and Relational Experience
The ICEST model benefited FCs mentally and psychologically, manifesting in their reduced depression and worries. The model strengthened FCs’ support within and outside the family system to establish a well-connected and collaborative caregiving environment for end-of-life caregivers, as social connectedness was a protective factor for FCs’ mental health.27, Internally, family-centered activities aimed to facilitate genuine family communication, positive family dynamics, and decision-making on critical issues. Externally, informal caregivers usually had difficulties in acquiring sufficient practically-focused information efficiently, 37 and information acquisition related to illness could increase their sense of control over the situation. 38 The model increased FCs’ access to information and community resources, which provided extra options to assist them in addressing practical concerns. Sufficient support could be a plausible factor that relieved FCs’ psychological distress.
The ICEST model emphasized relational factors and expanded end-of-life care to include family care, acknowledging the importance of a healthy family system in high-quality and sustainable care. The initial level of intimacy with patients was high in spousal and adult-children caregivers, and the ceiling effect may limit improvements. Such intimacy could contribute to FCs’ willingness to provide consistent care. In our study, FCs were highly involved in medical-related, physical, psychosocial, practical, and financial support. Intensive caregiving demands from various forms of support could result in excessive interruptions to FCs’ daily lives or self-isolation.23,39 Since openly discussing demise and death can be difficult in the Chinese community, 40 escape-avoidance coping strategies can often alleviate FCs’ psychological distress and family conflicts.41,42 The downside is that a lack of constructive conversations may lead to inadequate preparation for unsolved issues or unfinished wishes. The family-centered model utilized family-centered activities to foster genuine communication and decision-making, which optimized the relational experience and resolved disagreements on treatment/care plans, leading to higher family consensus. This practice respects patients’ autonomy and considers the participation of FCs in end-of-life care.
Differential Effects on Spouses and Adult Children
Spouses and adult children reported high baselines of caregiving strain, but the types of caregiving strain and stressors differed. Spouses held more negative perceptions of caregiving, while adult children reported more adjustment demands. Spouses usually lived with end-of-life patients and provided intensive physical and practical support. They generally viewed caregiving as a marital responsibility,43,44 which could be a reason for their reluctance to burden others in their networks. 28 Only half of spousal caregivers received other FCs’ support, and the solo caregiving could be too physically demanding for them, of whom most were female older adults. Due to the aging effect, 13 spouses reported physical decline, chronic illness, and frailty over the study period. Without sufficient support, some spouses were unable to handle increasing caregiving demands as end-of-life drew nearer. Female caregivers were less likely to discuss disease-related issues with patients 45 and tended to focus on caregiving difficulties. 46 The ICEST model appeared to address the spousal caregivers’ needs well, as evidenced by the fact that they had a greater reduction in anxiety than adult-children caregivers. The model helps reshape their perceptions and reduce their helplessness and worries by gaining new caregiving experiences full of emotional, instrumental, and informational support. 47
Adult children were not involved as often as spouses in physical and practical support; instead, they provided medical-related, psychosocial, and financial support to end-of-life patients. Adult children did not consider compassionate duties for their terminally ill parents as an obligation; on the contrary, filial responsibility added meaning to care.43,44 They maintained a relatively close relationship with end-of-life patients. Half of the adult children worked in paid employment, and end-of-life patients were often not the only family members for whom they cared. Working caregivers and those who cared for more than one family member usually experienced heavier care burdens.35,48 Thus, engagement in multiple concurrent roles was their challenge. Adult children may spend more effort in role adaptation as end-of-life caregivers, balancing expectations and adjusting their lives and responsibilities physically, psychologically, and practically. The ICEST model did not fully address adult children’s concerns about fulfilling the multiple roles; therefore, it is understandable why their worries and anxiety were not reduced as much as spouses’.
Implications and Limitations
The ICEST model could efficiently address the needs of FCs with different characteristics facing various challenges. Our findings could inform future intervention designs for spousal and adult-children caregivers. Capacity building for spousal caregivers needs to consider their frailty and enhance their acceptance of external supports. The focus of supporting adult-children caregivers should address the challenges of acting in different roles and dealing with family obligations. 49 Family activities should highlight the benefits for end-of-life patients and their FCs with open conversations, mutual love, a sense of togetherness, and positive family dynamics.
Due to ethical considerations, the study adopted a pre-post-test design rather than a randomized controlled trial. All participants were Chinese, and the findings should be cautiously interpreted when generalizing them to other cultures and contexts. FCs’ participation was voluntary, and FCs tended to have an intimate relationship with, or a strong willingness to take care of, their terminally ill family members. Future studies could explore the experiences of less-motivated FCs and the effectiveness of a family-centered intervention on those with poor relationships with care recipients. Process assessments could be added to the ICEST model to investigate the important ingredients in complex interventions.
Conclusion
The ICEST model effectively reduced caregiving strain, alleviated psychological distress, enhanced perceived social support, and resolved treatment/care plan disagreements for spouses and adult children. For spouses, the most effective support focused on changing negative perceptions of caregiving; for adult children, the focus was on coping with multiple tasks and complex expectations associated with various roles. Improving family dynamics and cohesiveness have the potentials to further improve patients’ and their FCs’ psychological well-being. Future modifications to the ICEST model might focus on promoting positive care experiences and building resilient family systems.
Supplemental Material
Supplemental Material - Differential Effects of an Integrated Community-Based End-Of-Life Support Team (ICEST) Model for Terminally Ill Older Adults on Spousal and Adult-Children Caregivers
Supplemental Material for Differential Effects of an Integrated Community-Based End-Of-Life Support Team (ICEST) Model for Terminally Ill Older Adults on Spousal and Adult-Children Caregivers by Amy Yin Man Chow, Anna Yan Zhang, Kelly Tsz Ching Wong, Iris Kwan Ning Chan, Genevieve Ataa Fordjour, Xuechen Xiong, Vivian Wai Qun Lou, and Cecilia Lai Wun Chan in American Journal of Hospice and Palliative Medicine®.
Footnotes
Acknowledgments
The authors sincerely appreciate the participation of older adults with terminal illnesses and their FCs in this study. We also thank the NGO partners of the JCECC project, including the Hong Kong Society of Rehabilitation, S.K.H Holy Carpenter Church District Elderly Community Centre, St. James Settlements, and Haven of Hope Sister Annie Skau Holistic Care Centre, for the participant recruitment and implementation of ICEST model. Please see the details at ![]() .
.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hong Kong Jockey Club Charities Trust initiated and funded the JCECC project. The evaluative study of the ICEST model as part of the JCECC project is also funded.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.