
Abstract
Introduction
Surgical oncology patients have a high symptom burden and increased risk of morbidity. The aim of palliative care is to evaluate and treat the patient in a holistic manner focusing on the unique attributes of each patient. This goal-concordant approach could help surgical patients cope with the stress and uncertainty that often accompany serious illness and surgery, improving overall outcomes. This qualitative analysis sought to explore whether unmet specialist palliative care or end-of-life needs exist in this population.
Methods
Qualitative interviews were completed with a subset of participants in a randomized, controlled trial of a specialist palliative care intervention for patients undergoing abdominal oncologic surgery. The interview guide sought to elicit respondents’ perceptions of palliative care and end-of-life needs perioperatively and postoperatively. Recurring themes were identified by two independent coders.
Results
Analysis of 47 interview transcripts revealed few serious concerns about end-of-life issues, however appreciation for the supportive presence offered by palliative care was present. Among participants who received specialist palliative care, many found the intervention helpful, but few were able to articulate issues that the intervention improved.
Conclusion
These findings suggest low levels of unmet palliative care needs among this population, which is consistent with the results of the parent trial. Targeting patients with a higher symptom burden perioperatively may allow for improved symptom management and better adherence to the treatment plan postoperatively, as well as be a more focused use of specialist palliative care clinicians’ efforts.
Keywords
Introduction
Since the 2005 recommendation by the American College of Surgeons to increase the use of palliative care involvement in the care of surgical patients with serious illness, research about the role of primary vs specialty palliative care in the perioperative period has increased. 1 Primary palliative care includes basic symptom management and care decisions for patients with serious illness often provided by the primary medical team, whereas palliative care specialists are trained to manage difficult-to-control symptoms, complicated care decisions, and multifaceted family dynamics, while incorporating emotional and spiritual needs into each individual’s care plan.2,3
While an interdisciplinary team approach has demonstrated a reduction in postoperative complications among older adult surgical populations, palliative care consultation was notably absent from this team. 4 Prior research has documented the importance of specialist palliative care for surgical patients, however a standard of when to introduce palliative care has been poorly defined. 5 Although abdominal surgery for cancer entails high symptom burden and high morbidity and mortality, the benefits of palliative care involvement in these patients has not been fully explored.5-7 While much of the research has been focused on clinical outcomes, it remains imperative that patients’ experiences are analyzed to better capture the complex needs in this population. This qualitative analysis sought to examine palliative care and end of life needs in surgical patients with and without a specialist palliative care intervention to uncover developing themes and to identify possible unmet needs.
Methods
Participants and Sample Size
Qualitative interviews were conducted with patients participating in the
A subset of participants was offered the opportunity to take part in a qualitative interview during their 1-month trial follow up. Purposive sampling was used to maximize diversity. 10 We stratified patients into 8 groups based on age (younger than 65 vs 65 and older), sex (men vs women) and trial group assignment (intervention vs usual care) and aimed to conduct 6 interviews in each group. Participants were compensated $50 for their time. SPQR Guidelines for qualitative research were followed for analysis and reporting of information garnered during the interviews. 10
Instrument Development
A semi structured interview guide (Appendix 1) was developed based on the surgical and palliative care expertise of the principal investigator of the SCOPE trial and a senior investigator with expertise in qualitative interview design and analysis. 9 Different questions were included for the intervention and control patients about their understanding and experience with specialist palliative care. Questions exploring supportive care needs during the perioperative and postoperative period were also analyzed and previously reported. 9
Data Collection and Analysis
Interviews took place by phone in hour-long sessions between July 2019 and September 2021. Participants granted permission for audio recording and professional transcription of the interviews. 11 NVivo 12 was used to code and analyze deidentified transcripts using standard methods. 12 The trial’s principal investigator (MCS), who is a surgeon and palliative care physician, and an experienced qualitative researcher (CD) served as coders. Using an inductive, iterative process they reviewed transcripts and developed a code book and independently coded the same transcripts until they consistently reached 80% concurrence in their coding. After this point, 1 reviewer coded each transcript with every eighth transcript coded by both to confirm 80% concurrence was maintained. No a priori conceptual model was used to generate the code book. The team then generated code summaries for each code to serve as the basis for analysis.
Results
Participant Characteristics.
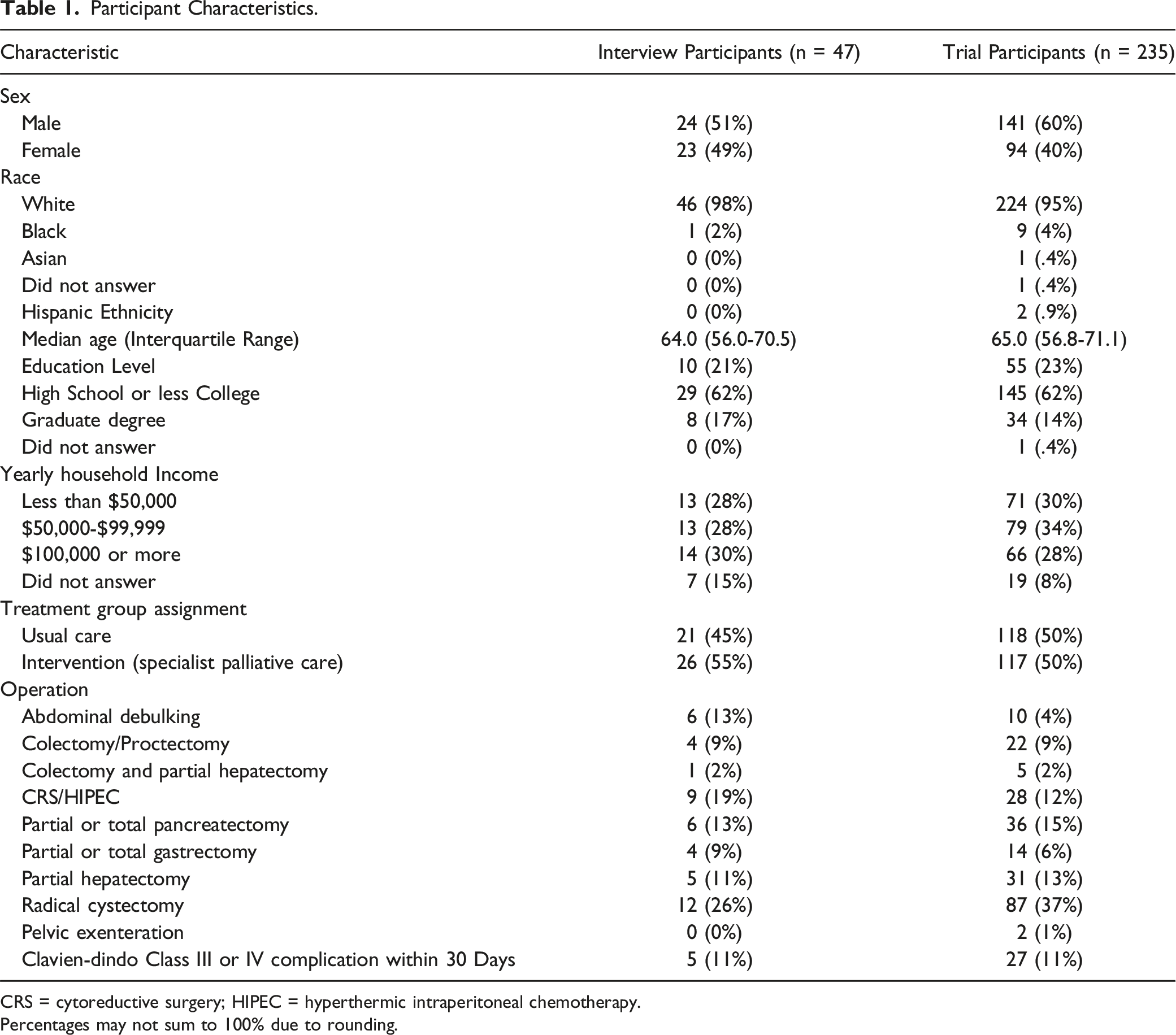
CRS = cytoreductive surgery; HIPEC = hyperthermic intraperitoneal chemotherapy.
Percentages may not sum to 100% due to rounding.
Impressions of Specialist Palliative Care
Usual Care Group
Usual Care Group Impressions of Specialist Palliative Care.
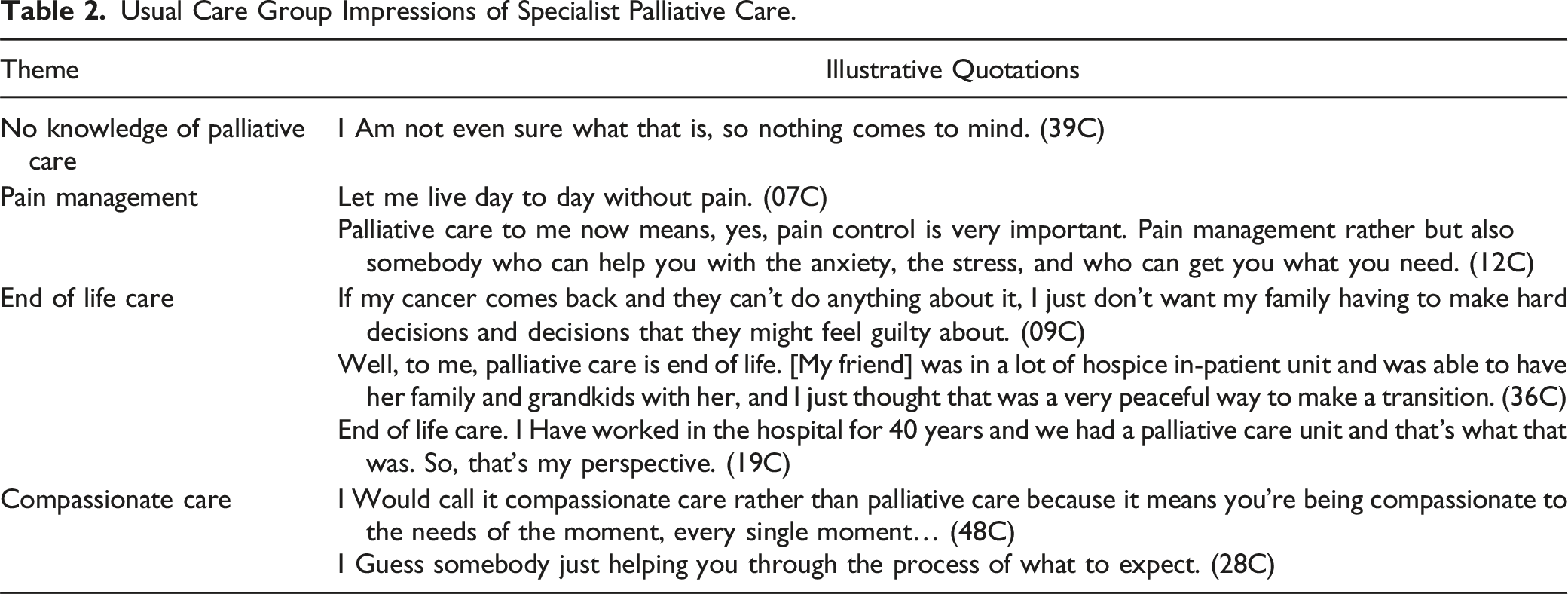
Several participants also linked palliative care to end of life care. Interviewees described palliative care as synonymous with hospice care, as a place people go when their life expectancy is limited, and their care needs are great. A few participants also associated palliative care with getting their affairs in order with appropriate documentation so family knew of their wishes should they decline. “If my cancer comes back and they can’t do anything about it, I just don’t want my family having to make hard decisions and decisions that they might feel guilty about” (09C).
Interestingly, a small number of interviewees reported that palliative care should not be considered end of life care, that the support palliative care provides encompasses much more than the final days of life. “I would call it compassionate care rather than palliative care because it means you’re being compassionate to the needs of the moment, every single moment…” (48C).
Intervention Group
Intervention Group Experience With Specialist Palliative Care.
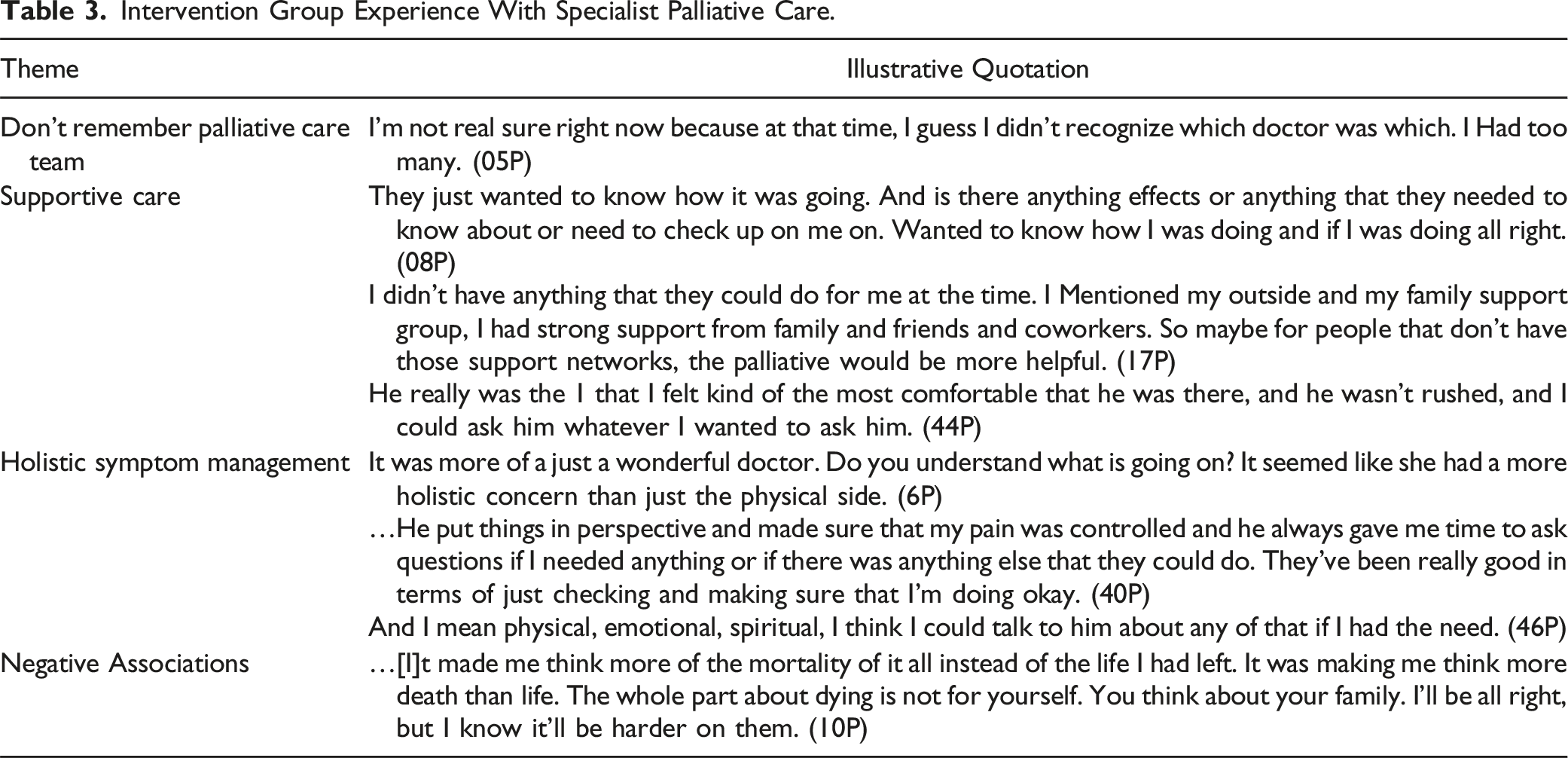
Several participants recognized the involvement of palliative care but had difficulty recalling specifics about their conversations other than noting the interaction was positive. When patients were able to specify what the palliative care providers did, one major theme that stood out was supportive care. Participants felt supported and listened to by the palliative care providers pre- and postoperatively. “They just wanted to know how it was going. And is there any effects or anything that they needed to know about or need to check up on me on. Wanted to know how I was doing and if I was doing all right” (08P).
Some interviewees described their interaction with palliative care as a holistic approach to symptom control where physical symptoms, emotional distress, and spirituality were addressed in their care. These participants describe the interaction as helpful, expressing appreciation specifically for management of pain and anxiety: “…He put things in perspective and made sure that my pain was controlled and he always gave me time to ask questions if I needed anything or if there was anything else that they could do. They’ve been really good in terms of just checking and making sure that I’m doing okay” (40P). “And I mean physical, emotional, spiritual, I think I could talk to him about any of that if I had the need” (46P).
One interviewee reported a negative interaction with palliative care postoperatively. Questions about family coping and advance care planning left the participant feeling hopeless and depressed. “…it made me think more of the mortality of it all instead of the life I had left. It was making me think more death than life.” Questions about the interviewee’s personal coping however evoked feelings of acceptance of death, which the interviewee was not opposed to discussing. “The whole part about dying is not for yourself. You think about your family. I’ll be all right, but I know it’ll be harder on them” (10P).
End of Life
End of Life Concerns (Both Intervention and Usual Care Group).
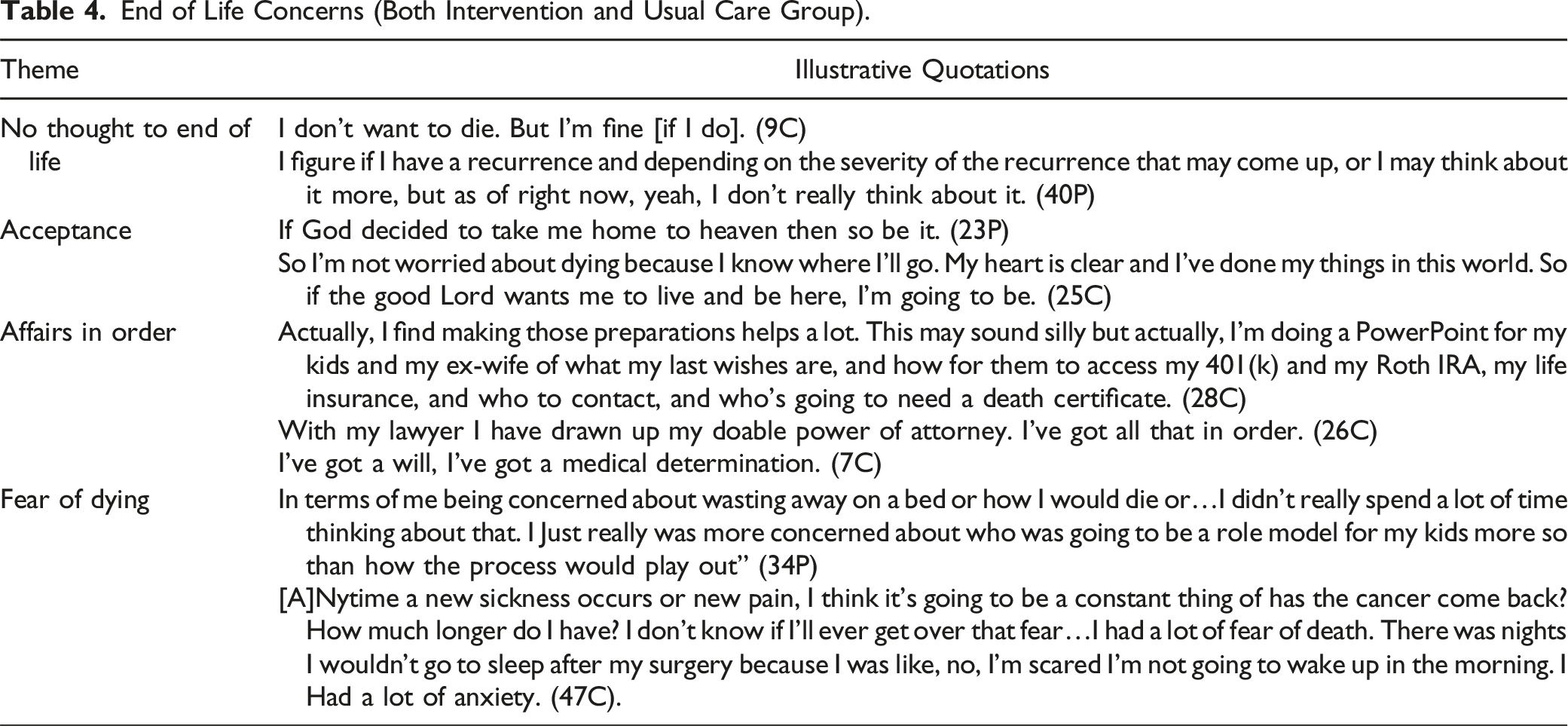
In the context of getting affairs in order, several interviewees talked about ensuring they had a durable power of attorney, living will, or other advance directive in place. Preparing advance directives were for most participants the only mention of advance care planning. Only a few participants reported thinking about how they wanted to die or making plans for their care at the end of life beyond writing an advance directive.
Very few interviewees reported worrying about or fearing their death. Of those who expressed worries, most of the worry was centered on what would happen to their family members once they died, rather than on the dying process or any existential distress about their own mortality. As one participant put it, “In terms of me being concerned about wasting away on a bed or how I would die or…I didn’t really spend a lot of time thinking about that. I just really was more concerned about who was going to be a role model for my kids more so than how the process would play out” (34P). Nevertheless, one participant did speak in depth about experiencing fears of death and dying: “anytime a new sickness occurs or new pain, I think it’s going to be a constant thing of has the cancer come back? How much longer do I have? I don’t know if I’ll ever get over that fear…I had a lot of fear of death. There was nights I wouldn’t go to sleep after my surgery because I was like, no, I’m scared I’m not going to wake up in the morning. I had a lot of anxiety” (47C).
Discussion
These qualitative data collected from a sub-group of patients enrolled in a larger randomized clinical trial of specialist palliative care for surgical patients provide nuance and insight into the results of the parent trial. The SCOPE Trial found no improvement in quality of life for intervention patients compared to control patients, and another similar trial of perioperative specialist palliative care also failed to demonstrate a benefit from the intervention. 13 These qualitative data demonstrate that most intervention group patients did not specifically remember what the palliative care specialists did for them, suggesting that for the most part these patients did not have needs that would make the care received from palliative care specialists salient. Moreover, the widespread lack of concern with end-of-life issues suggests that patients felt a strong need for advance care planning or assistance with medical decision making, which are 2 of the ways palliative care specialists can assist patients.
The qualitative data also offer some guidance on how specialist palliative care might be helpful to surgical patients. In the intervention group, participants who did remember the palliative care team described them as a supportive presence, a team they could count on to address their needs and ensure their wellbeing. Interview participants in the intervention group collectively appreciated the positive presence palliative care offered even though many were unable to recall specific details about the conversations. This is consistent with other findings of the benefits of specialist palliative care support in surgical patients care where often patients describe a non-specific improvement in symptoms and care, while finding it difficult to articulate the value of these interactions.6,14 These results suggest patients may appreciate and value the support of specialist palliative care even if it does not measurably improve patient reported outcomes.
Some intervention group participants did identify specialist palliative care as beneficial in symptom management, especially with respect to pain. Patients facing oncologic surgery often experience a host of complex symptoms perioperatively because of cancer burden and pre-surgical neoadjuvant treatments. Multiple studies have shown improvement in cancer-related symptoms improves quality of life and reduces morbidity in oncology patients1,15,16. Targeting patients with a higher symptom burden pre-surgery may allow for improved symptom management and better adherence to the treatment plan post-surgery, while also improving surgical outcomes.
Most patients reported no serious concerns about end-of-life, and of those that did, the biggest concern was with making financial arrangements for their families. In our interviews, patients were concerned with getting their affairs in order and how the possibility of mortality may affect their family. Taken as a whole, these responses do not suggest a large unmet need for supportive care directed toward end-of-life issues for these patients. The responses do not suggest a widespread appetite for more in-depth advance care planning or for counseling about the dying process. However, a few patients did express serious fears or worries about dying, with 1 describing severe, persistent anxiety that affected recovery from surgery. Previous studies have shown improvement in mood and psychosocial support when specialty palliative care is involved.7,14,15 Identifying patients with significant anxiety and working to address their concerns may improve their treatment and survivorship experiences.
Limitations in this qualitative analysis include the lack of generalizability in a small, relatively homogenous sample. The concerns of a more diverse population may not be adequately represented as this sample has a disproportionate number of non-Hispanic whites with degrees in higher education. Furthermore, this study failed to delineate variances in palliative care engagement before and after surgery, potentially missing an opportunity to identify a subgroup of patiens who might have gained from specialized palliative care support. Even so, this qualitative analysis provides insights into how patients perceive palliative care, and the role specialist palliative care may play in supporting surgical oncology patients in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Cancer Institute (K12CA090625), the National Institute on Aging (R03AG060085, K76AG068436), and the National Center for Advancing Translational Sciences (UL1TR000445).
Disclaimer
The views expressed in this article are those of the authors and contributors and do not necessarily reflect those of Johns Hopkins University or any other organization to which the authors are affiliated.