
Abstract
Objective
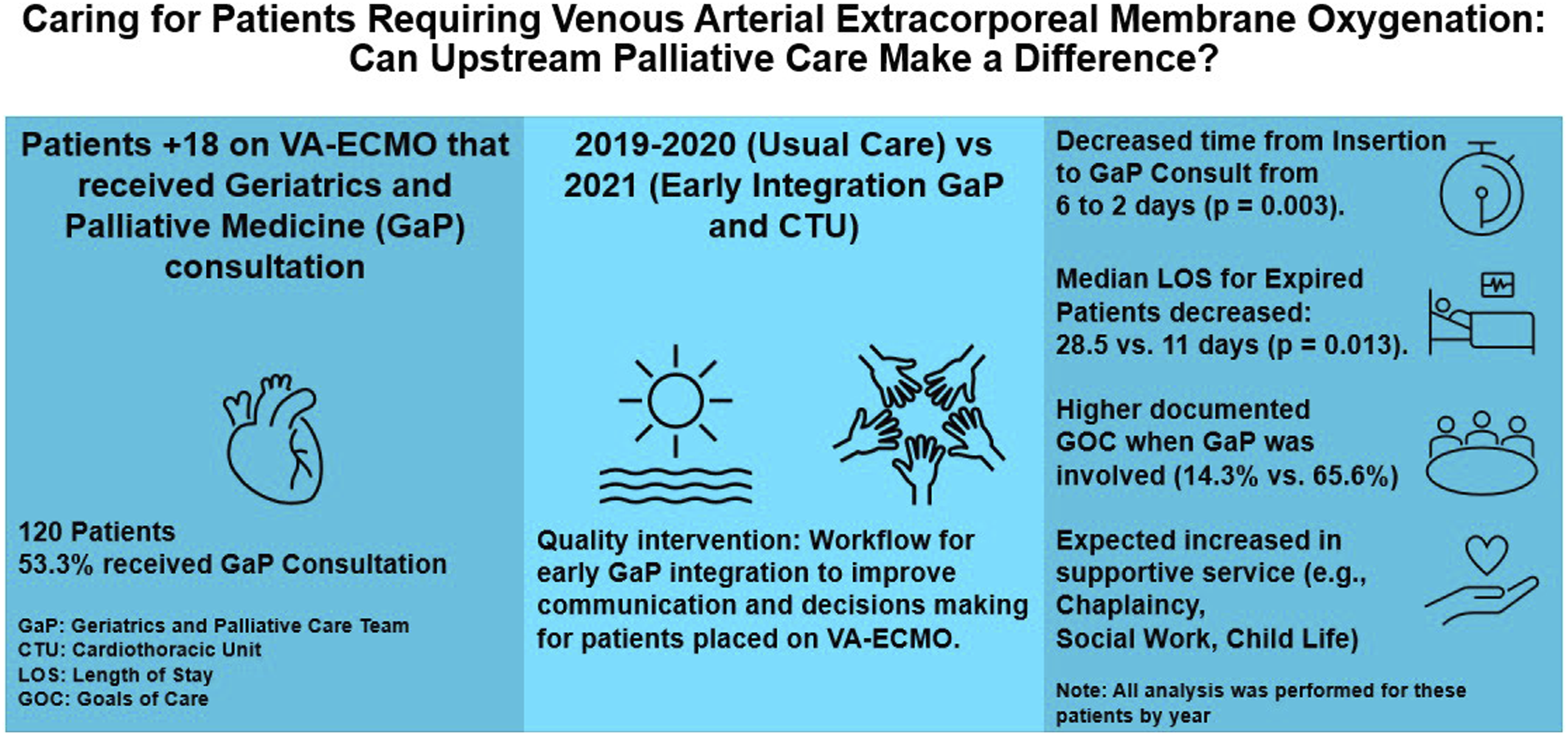
Palliative care consultation is relevant for patients requiring Venous-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO); however, evidence is limited to support its value. For this population, we compared length of stay (LOS) (primary outcome), operational metrics and goals of care (GOC) frequency before and after a collaboration between cardiothoracic (CT) surgery and Geriatrics and Palliative Medicine (GaP).
Methods
Retrospective chart review of patients (18+) admitted to a quaternary center that required VA-ECMO between 2019-2021 and received GaP consultation. Demographics, LOS, times to consult, illness severity, GOC, and outcomes were analyzed.
Results
120 patients met inclusion criteria and 64 (53.3%) had GaP consultation. No differences were observed regarding demographics and insertion status (emergent vs elective). Median (IQR) days to GaP consult for 2019, 2020 and 2021 were 6.5 (4.0-14.5), 5.0 (2.0-11.0) and 3.0 (2.0-5.0), respectively (P = .006). Median days from insertion to consult for 2019, 2020 and 2021 were 6.0 (4.0-20.0), 3.0 (1.0-6.0) and 2.0 (1.0-4.0) (P = .003). Among survivors, over the 3-year course, median LOS was not statistically different. Between expired patients, median (IQR) LOS for 2019, 2020, and 2021 was 28.5 (23.0-40.0), 12.0 (8.0-14.0), 11.0 (5.0-17.0) days (P = .013). For patients not seen by GaP, 8 (14.3%) GOC notes were documented, compared with 42 (65.6%) for patients seen. Mortality was similar (53.6% vs 53.1% [GaP]).
Conclusion
For patient on VA-ECMO, early GaP consultation may improve hospital LOS and GOC rates. We suggest organizations consider early palliative integration when instituting mechanical circulatory support.
Keywords
Get full access to this article
View all access options for this article.