Introduction: The hospice-in-place program at Vanderbilt University Medical Center (VUMC) is available to patients and families who elect for hospice benefits and are too unstable to be transported for hospice care. The goal of this study was to assess the satisfaction of family members of patients who died while hospitalized at VUMC and received hospice-in-place compared to the families of patients who did not receive hospice care. Methods: Next-of-kin satisfaction was measured through the administration of qualitative interviews and quantitative questionnaires. Semi-structured interviews were audio-recorded, and transcripts were analyzed using an iterative inductive-deductive approach to develop a conceptual framework. Participants were also asked to respond to a 10-question satisfaction questionnaire. Results: Forty participants were enrolled: 20 next-of-kin of patients who received hospice-in-place and 20 next-of-kin of patients who passed without hospice. Factors influencing satisfaction were organized into a conceptual framework with three categories: individual-level factors, systems-level factors, and modifying factors. For the questionnaires, the hospice-in-place group had a mean satisfaction score of 4.54 (0.76) out of five, while the non-hospice group had a mean score of 4.14 (1.00). A comparison of the two groups’ responses did not show a statistically significant difference (P = 0.06). Discussion: Quantitative findings of this study showed improved satisfaction but were unable to show a significant difference in satisfaction with hospice-in-place compared to traditional care. Questionnaire results suggest that both types of care yield high satisfaction scores and are successfully supporting patients and families. The conceptual framework also adds to the understanding of end-of-life experiences at VUMC.
Confronting death is undoubtedly difficult, and coping with grief can have lasting and profound impacts on surviving relatives. Preparing patients and their families for the end of life can benefit everyone involved.1-3 Hospice care is 1 option that may reduce the emotional and decisional burdens on loved ones as they navigate loss.
Hospice care seeks to alleviate pain and manage symptoms of the terminally ill, while preparing patients and their families for death. Over the last 2 decades, the use of hospice services has risen dramatically. In 2000, 21.6% of patients who died were receiving hospice services compared to 50.4% of patients in 2015.4 The efficacy of hospice care in supporting patients and their families at the end of life is well documented.3,5,6 Patients receiving hospice services have better symptom control, their wishes are met, and they have improved quality of life.5,6 Families and caregivers also benefit: their informational needs are met, and they are better able to resume their lives after death compared to families who did not receive hospice services.5 Patients and family members generally express a preference for at-home compared to inpatient hospice care.7 However, patients are not always stable enough to be transferred home or to a hospice facility, and hospital-based end-of-life care is sometimes necessary.
The hospice-in-place program at Vanderbilt University Medical Center (VUMC) is an insurance benefit available for patients who would like hospice benefits and are too unstable to be transported home or to a hospice facility.8 Any hospital bed at VUMC can be converted into a hospice bed, eliminating the need for relocation within the hospital. Outside hospice vendors partner with clinical staff so patients receive hospice care from staff they already know8. Inpatient hospice benefits also extend to family members and include support from social workers and chaplains, financial planning and notaries, funeral planning assistance, support groups, and individual bereavement counseling for up to 13 months after the death of a loved 1.8
The primary goal of this study was to assess the self-reported satisfaction of family members of patients who died during a hospitalization at Vanderbilt University Medical Center and received hospice-in-place, compared to the families of patients who died during a hospitalization and did not receive hospice care. We hope to determine whether hospice-in-place at VUMC is better than traditional care at supporting families with a relative at the end of their life.
Methods
Forty participants, which included the next-of-kin or medical decision makers listed in the medical record for patients who died during a hospitalization at VUMC, were enrolled in this study. Enrollment letters explaining the purpose and requirements of the study were sent to prospective participants within 4 to 6 weeks following the death of their relative, and enrollment was offered prospectively until twenty participants whose relatives received hospice-in-place and twenty participants whose relatives did not receive hospice care agreed to join the study.
The self-reported satisfaction of surviving family members was measured through the administration of qualitative interviews and quantitative questionnaires. This project was approved by the Vanderbilt University IRB (IRB#201128).
Two trained research assistants performed brief phone interviews with participants using a scripted list of open-ended questions developed in collaboration with the Vanderbilt University Qualitative Research Core (VU-QRC).9 Questions covered participant experiences with the care received, the trajectory of emotions and grief after death, communication with the care team, and the decision to pursue or forgo hospice care. Audio recordings were stored on a secure, encrypted drive until transcribed by an IRB-approved service (https://rev.com).
Qualitative data coding and analysis was managed by the VU-QRC. A hierarchical coding system was developed and refined using the interview guide, study aims, and a preliminary review of the transcripts. Definitions and rules were written for each coding category. Top-level categories in the coding system were (1) circumstance of admission, (2) emotions, (3) attitudes and beliefs, (4) experience with VUMC, (5) interactions, (6) resources provided by Vanderbilt, (7) communication, (8) coping, grief, and acceptance, (9) hospice care, (10) quality of life, (11) barriers and facilitators, and (12) temporal codes. The coding system (see supplemental material) had 12 major themes (eg, coping with grief, quality of life). Each category had 2-13 subcategories, some of which included 2 additional levels of hierarchical division. Trained coders first established reliability in using the coding system on 2 transcripts, reconciling any discrepancies, and independently coded the remaining transcripts. Coded transcripts were then combined and sorted by code. The transcripts, quotations, and codes were managed using Microsoft Excel and SPSS version 28.0.
In addition to qualitative interview responses, participants were also asked to respond to a 10-question questionnaire. Participants rated their satisfaction with various elements of hospital care (eg quality of care, responsiveness to concerns, communication). Six items were scored using a five-point Likert scale (1 = poor, 2 = fair, 3 = good, 4 = very good, 5 = excellent) and 4 using a three-point scale (1 = No, not at all, 3 = Yes, somewhat, 5 = Yes, definitely). A total satisfaction score was calculated as the mean of all response ratings. Scores were then compared between groups using the Mann-Whitney U test, a non-parametric t-test. Statistical analysis was performed in R.
Results
A total of 144 next-of-kin were invited to participate in the study to achieve an enrollment of 40 participants: 20 for hospice-in-place and 20 for the non-hospice group. For the hospice-in-place group, 70% (14/20) of patients were admitted and died from acute conditions. For the non-hospice group, 65% (13/20) of patients died from acute conditions.
Interview Results
The coded transcripts were analyzed using an iterative inductive-deductive approach,10,11 resulting in a conceptual framework. Inductively, we sorted quotes by coding categories to identify higher order themes and relationships between themes. Deductively, we were guided by the Health Belief Model (HBM), a long-standing psychosocial theory of health decision making.12 We also used the Consolidated Framework for Implementation Research (CFIR), a common framework used to assess contextual factors.13 The analysis was iterative in that the conceptual framework was theoretically informed, while the specific content of the framework was derived from the coded interview data.
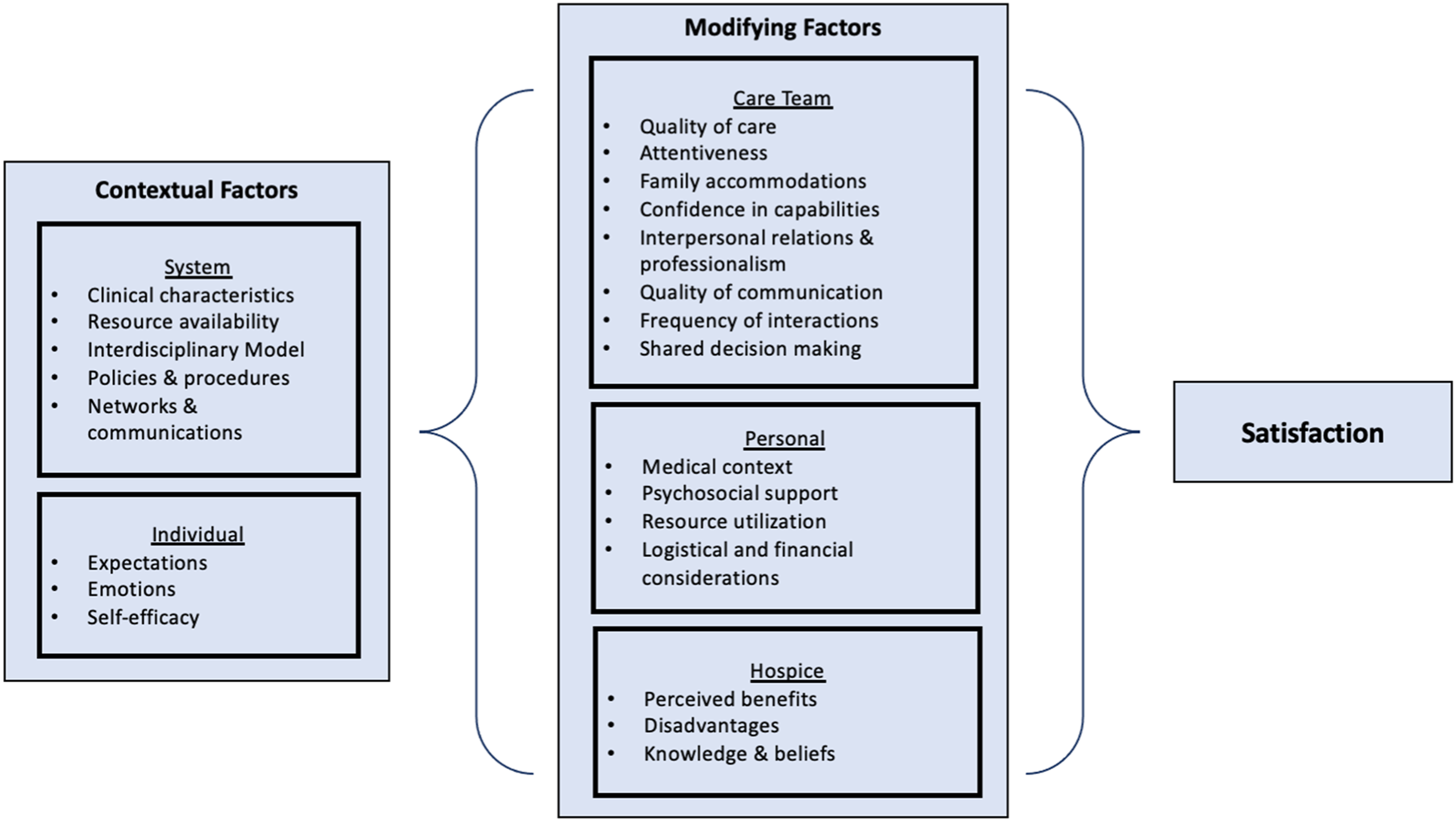
Figure 1 presents the conceptual framework describing self-reported satisfaction of family members of patients who died during a hospitalization. This framework was developed to integrate a broad range of factors into a holistic understanding of patient and family satisfaction with end-of-life care. Major factors influencing overall satisfaction were organized into 3 categories: individual-level, systems-level, and modifying factors. The left column represents systems- and individual-level contextual factors that broadly applied to all participants. The central area, labeled “Modifying Factors”, highlights several individual factors experienced by participants which contributed to their overall satisfaction. In the remainder of the results, we will discuss each element of the conceptual framework in further detail. Supporting quotes are provided in tables, identified by ID numbers referencing the table number and section.
Integrative conceptual framework of overall satisfaction with end-of-life care.
Individual Level Factors
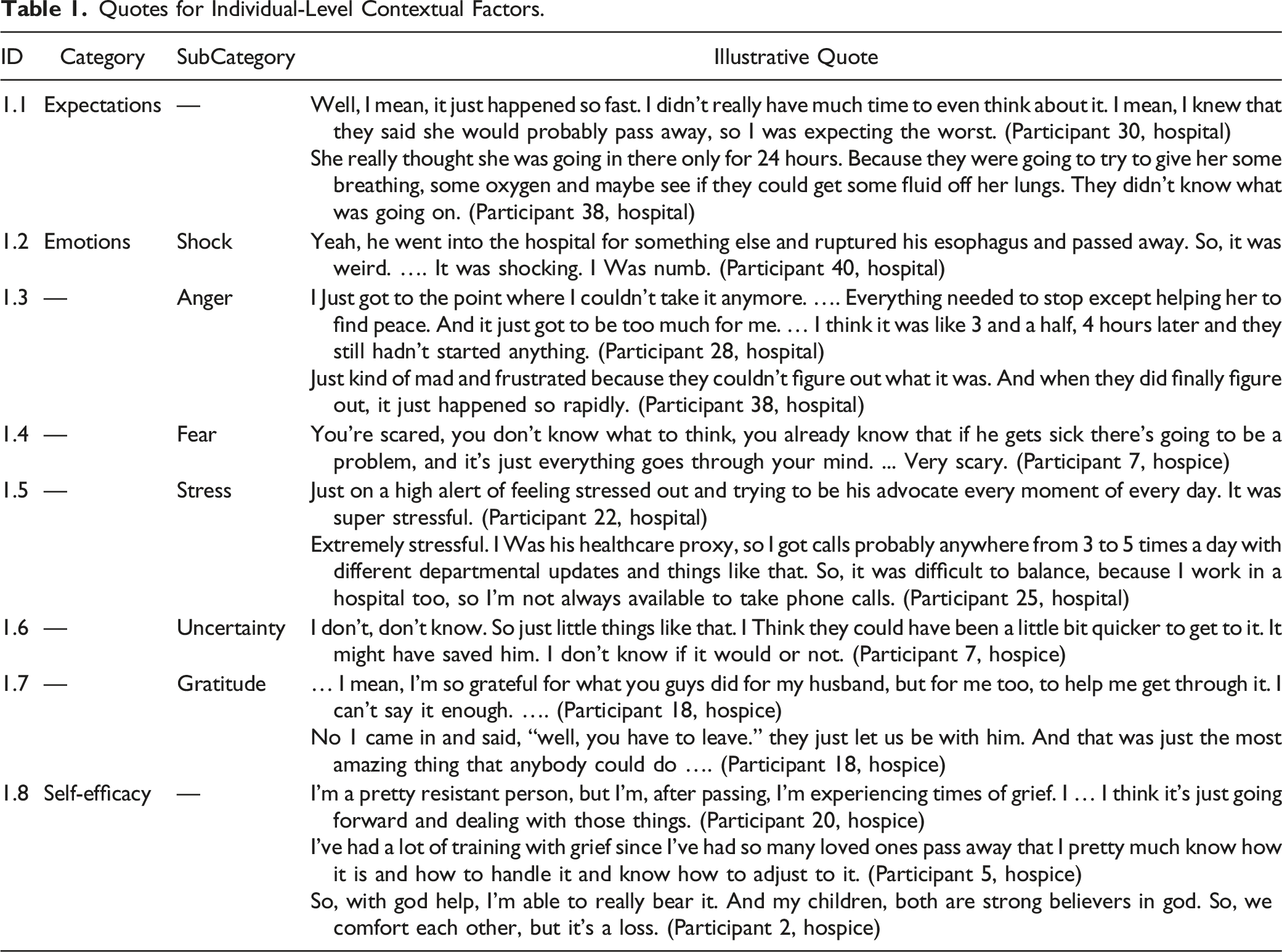
Table 1 organizes the individual-level contextual factors influencing overall satisfaction into a table with illustrative quotes.
Quotes for Individual-Level Contextual Factors.
ID
Category
SubCategory
Illustrative Quote
1.1
Expectations
—
Well, I mean, it just happened so fast. I didn’t really have much time to even think about it. I mean, I knew that they said she would probably pass away, so I was expecting the worst. (Participant 30, hospital) She really thought she was going in there only for 24 hours. Because they were going to try to give her some breathing, some oxygen and maybe see if they could get some fluid off her lungs. They didn’t know what was going on. (Participant 38, hospital)
1.2
Emotions
Shock
Yeah, he went into the hospital for something else and ruptured his esophagus and passed away. So, it was weird. …. It was shocking. I Was numb. (Participant 40, hospital)
1.3
—
Anger
I Just got to the point where I couldn’t take it anymore. …. Everything needed to stop except helping her to find peace. And it just got to be too much for me. … I think it was like 3 and a half, 4 hours later and they still hadn’t started anything. (Participant 28, hospital) Just kind of mad and frustrated because they couldn’t figure out what it was. And when they did finally figure out, it just happened so rapidly. (Participant 38, hospital)
1.4
—
Fear
You’re scared, you don’t know what to think, you already know that if he gets sick there’s going to be a problem, and it’s just everything goes through your mind. ... Very scary. (Participant 7, hospice)
1.5
—
Stress
Just on a high alert of feeling stressed out and trying to be his advocate every moment of every day. It was super stressful. (Participant 22, hospital) Extremely stressful. I Was his healthcare proxy, so I got calls probably anywhere from 3 to 5 times a day with different departmental updates and things like that. So, it was difficult to balance, because I work in a hospital too, so I’m not always available to take phone calls. (Participant 25, hospital)
1.6
—
Uncertainty
I don’t, don’t know. So just little things like that. I Think they could have been a little bit quicker to get to it. It might have saved him. I don’t know if it would or not. (Participant 7, hospice)
1.7
—
Gratitude
… I mean, I’m so grateful for what you guys did for my husband, but for me too, to help me get through it. I can’t say it enough. …. (Participant 18, hospice) No 1 came in and said, “well, you have to leave.” they just let us be with him. And that was just the most amazing thing that anybody could do …. (Participant 18, hospice)
1.8
Self-efficacy
—
I’m a pretty resistant person, but I’m, after passing, I’m experiencing times of grief. I … I think it’s just going forward and dealing with those things. (Participant 20, hospice) I’ve had a lot of training with grief since I’ve had so many loved ones pass away that I pretty much know how it is and how to handle it and know how to adjust to it. (Participant 5, hospice) So, with god help, I’m able to really bear it. And my children, both are strong believers in god. So, we comfort each other, but it’s a loss. (Participant 2, hospice)
Expectations
Participants discussed the anticipated outcomes at the time of hospitalization. The perceived illness severity impacted the family’s preparedness for the end of life. Some participants described the loss as an expected outcome, whereas others were unprepared for death (1.1).
Emotions
Having someone you care for die in the hospital was associated with a wide range of emotions, both positive and negative. Many participants discussed feelings of shock and confusion at the loss of their relative, especially when the death was not anticipated (1.2). Feelings of anger, frustration, or resentment were commonly reported. Discussion primarily centered around negative interactions with staff members or anger about institutional policies, such as insurance coverage (1.3). Several participants discussed feelings of fear, especially regarding the uncertainty of the outcome (1.4). Participants described the stressful nature of the hospital stay or attributed feeling stressed to their responsibilities as healthcare proxy and/or conflicting obligations with work (1.5). Participants discussed feelings of uncertainty about the outcome and uncertainty, or regret, in the context of whether anything could have been done to prevent death (1.6). Gratitude for the care received or support from the care team was frequently reported by participants, as was gratitude for accommodations made for the family (1.7).
Self-Efficacy
Participants discussed the belief in their ability to cope with loss. Some were confident that they were emotionally resilient, whereas others referenced previous experiences with grief that they felt allowed them to cope. Other participants called on their faith or social support networks to help handle the loss (1.8).
Systems-Level Factors
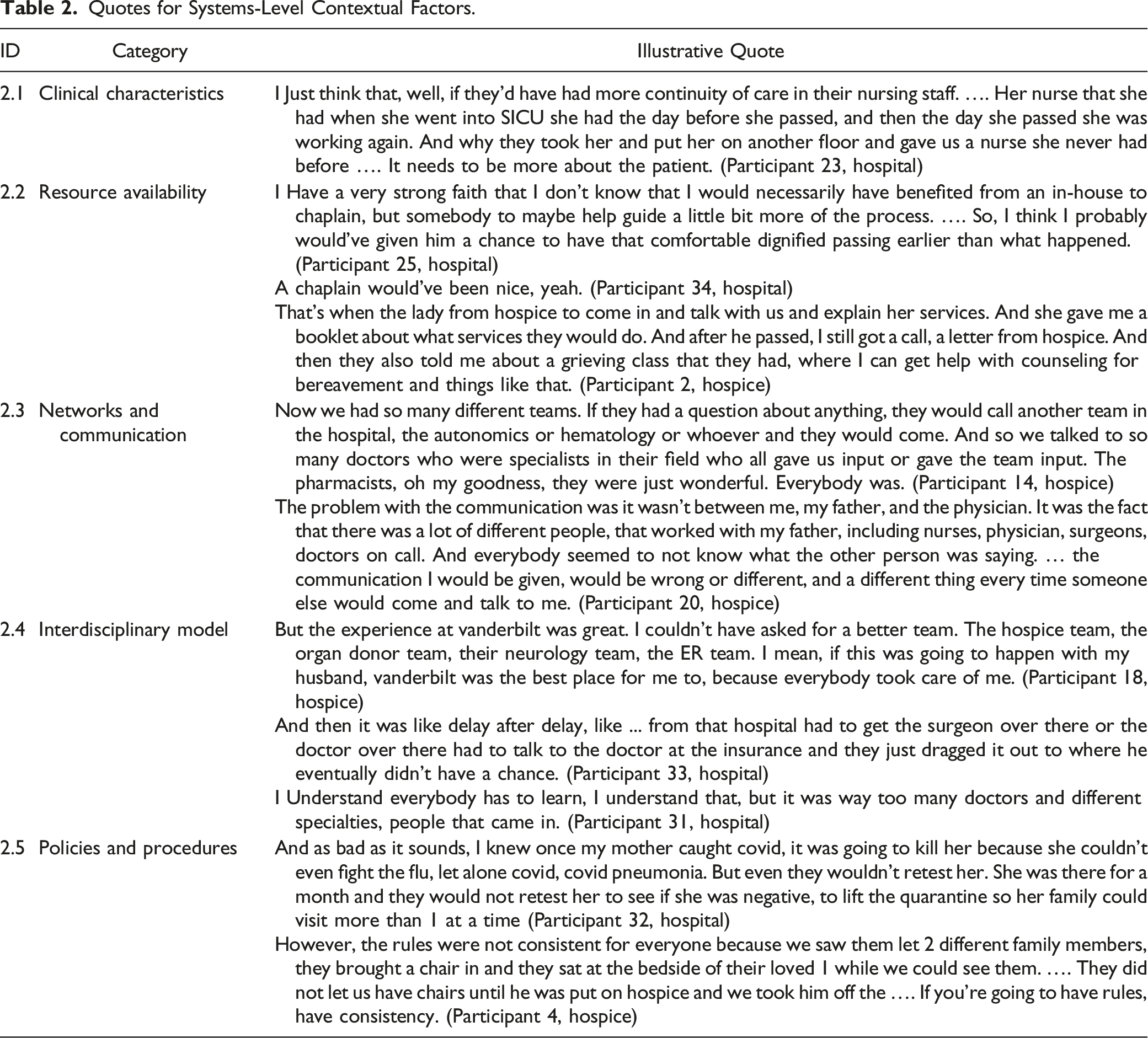
The systems-level context includes the hospital setting, protocols for delivering care, resources available, quality of interdisciplinary teamwork, and the frequency and quality of communication with staff members. Table 2 outlines systems-level contextual factors, along with illustrative quotes. Participants discussed the role of clinical characteristics, including the setting of care, staffing dynamics, and shift assignments, in their overall satisfaction. Some participants reported feeling unsupported due to a lack of continuity of care that resulted from shift changes and inconsistent staffing (2.1). VUMC provides several resources to patients and families, including chaplains and religious personnel, bereavement counseling, hospice services, social workers, and financial planning services. The availability and timeliness of these resources influenced overall satisfaction (2.2). Communication and the quality and effectiveness of these communication networks were important factors. Some participants described their satisfaction with the communication networks across multiple services and care teams, while others expressed frustrations with inefficient communication protocols (2.3). VUMC is a large, academic institution with multidisciplinary care teams. Participants frequently reported their satisfaction with this multi-level, interdisciplinary healthcare model. However, many participants also discussed its challenges, particularly delays in care delivery. Because care teams are often comprised of medical students, residents, and junior physicians, some participants also expressed dissatisfaction with the interdisciplinary care model (2.4). Participants discussed institution-wide policies and procedures at Vanderbilt, particularly those pertaining to COVID-19. Often, they were dissatisfied with isolation protocols for COVID-positive patients or reduced visitor allowances. Other participants described frustrations with the inconsistent enforcement of institution-wide policies (2.5).
Quotes for Systems-Level Contextual Factors.
ID
Category
Illustrative Quote
2.1
Clinical characteristics
I Just think that, well, if they’d have had more continuity of care in their nursing staff. …. Her nurse that she had when she went into SICU she had the day before she passed, and then the day she passed she was working again. And why they took her and put her on another floor and gave us a nurse she never had before …. It needs to be more about the patient. (Participant 23, hospital)
2.2
Resource availability
I Have a very strong faith that I don’t know that I would necessarily have benefited from an in-house to chaplain, but somebody to maybe help guide a little bit more of the process. …. So, I think I probably would’ve given him a chance to have that comfortable dignified passing earlier than what happened. (Participant 25, hospital) A chaplain would’ve been nice, yeah. (Participant 34, hospital) That’s when the lady from hospice to come in and talk with us and explain her services. And she gave me a booklet about what services they would do. And after he passed, I still got a call, a letter from hospice. And then they also told me about a grieving class that they had, where I can get help with counseling for bereavement and things like that. (Participant 2, hospice)
2.3
Networks and communication
Now we had so many different teams. If they had a question about anything, they would call another team in the hospital, the autonomics or hematology or whoever and they would come. And so we talked to so many doctors who were specialists in their field who all gave us input or gave the team input. The pharmacists, oh my goodness, they were just wonderful. Everybody was. (Participant 14, hospice) The problem with the communication was it wasn’t between me, my father, and the physician. It was the fact that there was a lot of different people, that worked with my father, including nurses, physician, surgeons, doctors on call. And everybody seemed to not know what the other person was saying. … the communication I would be given, would be wrong or different, and a different thing every time someone else would come and talk to me. (Participant 20, hospice)
2.4
Interdisciplinary model
But the experience at vanderbilt was great. I couldn’t have asked for a better team. The hospice team, the organ donor team, their neurology team, the ER team. I mean, if this was going to happen with my husband, vanderbilt was the best place for me to, because everybody took care of me. (Participant 18, hospice) And then it was like delay after delay, like ... from that hospital had to get the surgeon over there or the doctor over there had to talk to the doctor at the insurance and they just dragged it out to where he eventually didn’t have a chance. (Participant 33, hospital) I Understand everybody has to learn, I understand that, but it was way too many doctors and different specialties, people that came in. (Participant 31, hospital)
2.5
Policies and procedures
And as bad as it sounds, I knew once my mother caught covid, it was going to kill her because she couldn’t even fight the flu, let alone covid, covid pneumonia. But even they wouldn’t retest her. She was there for a month and they would not retest her to see if she was negative, to lift the quarantine so her family could visit more than 1 at a time (Participant 32, hospital) However, the rules were not consistent for everyone because we saw them let 2 different family members, they brought a chair in and they sat at the bedside of their loved 1 while we could see them. …. They did not let us have chairs until he was put on hospice and we took him off the …. If you’re going to have rules, have consistency. (Participant 4, hospice)
Modifying Factors
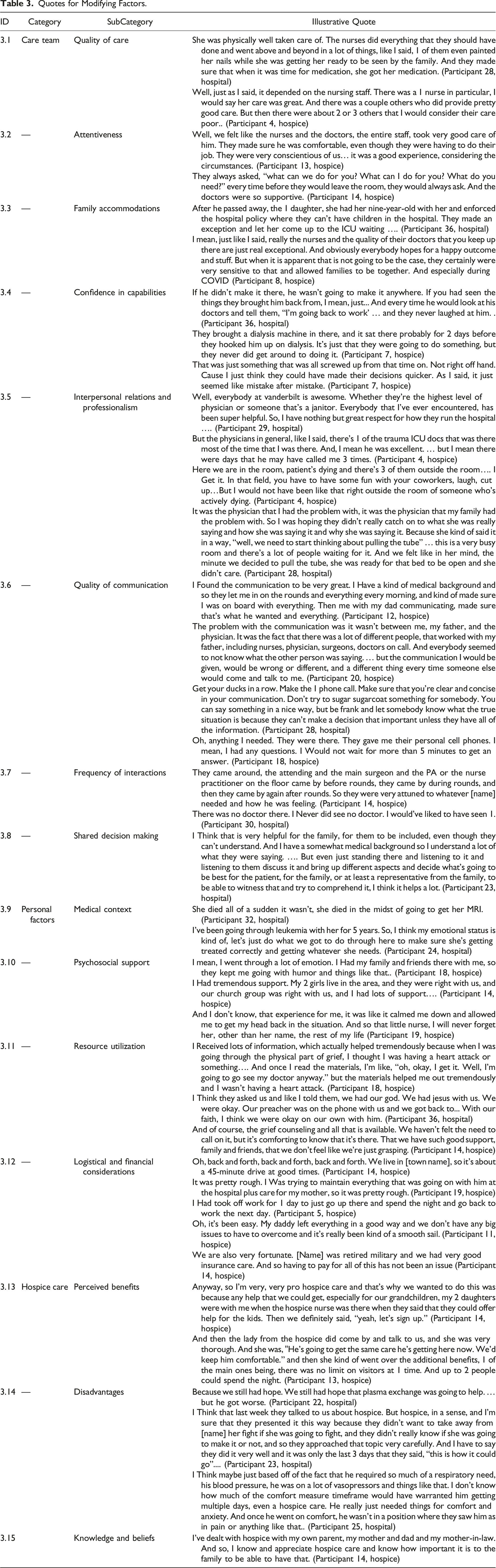
In addition to individual- and systems-level factors, 3 sets of modifying factors were identified: experiences with the care team, personal factors, and attitudes and beliefs about hospice care. Table 3 organizes these factors with illustrative quotes as examples of each.
Quotes for Modifying Factors.
ID
Category
SubCategory
Illustrative Quote
3.1
Care team
Quality of care
She was physically well taken care of. The nurses did everything that they should have done and went above and beyond in a lot of things, like I said, 1 of them even painted her nails while she was getting her ready to be seen by the family. And they made sure that when it was time for medication, she got her medication. (Participant 28, hospital) Well, just as I said, it depended on the nursing staff. There was a 1 nurse in particular, I would say her care was great. And there was a couple others who did provide pretty good care. But then there were about 2 or 3 others that I would consider their care poor.. (Participant 4, hospice)
3.2
—
Attentiveness
Well, we felt like the nurses and the doctors, the entire staff, took very good care of him. They made sure he was comfortable, even though they were having to do their job. They were very conscientious of us… it was a good experience, considering the circumstances. (Participant 13, hospice) They always asked, “what can we do for you? What can I do for you? What do you need?” every time before they would leave the room, they would always ask. And the doctors were so supportive. (Participant 14, hospice)
3.3
—
Family accommodations
After he passed away, the 1 daughter, she had her nine-year-old with her and enforced the hospital policy where they can’t have children in the hospital. They made an exception and let her come up to the ICU waiting …. (Participant 36, hospital) I mean, just like I said, really the nurses and the quality of their doctors that you keep up there are just real exceptional. And obviously everybody hopes for a happy outcome and stuff. But when it is apparent that is not going to be the case, they certainly were very sensitive to that and allowed families to be together. And especially during COVID (Participant 8, hospice)
3.4
—
Confidence in capabilities
If he didn’t make it there, he wasn’t going to make it anywhere. If you had seen the things they brought him back from, I mean, just... And every time he would look at his doctors and tell them, “I’m going back to work’ … and they never laughed at him. . (Participant 36, hospital) They brought a dialysis machine in there, and it sat there probably for 2 days before they hooked him up on dialysis. It’s just that they were going to do something, but they never did get around to doing it. (Participant 7, hospice) That was just something that was all screwed up from that time on. Not right off hand. Cause I just think they could have made their decisions quicker. As I said, it just seemed like mistake after mistake. (Participant 7, hospice)
3.5
—
Interpersonal relations and professionalism
Well, everybody at vanderbilt is awesome. Whether they’re the highest level of physician or someone that’s a janitor. Everybody that I’ve ever encountered, has been super helpful. So, I have nothing but great respect for how they run the hospital …. (Participant 29, hospital) But the physicians in general, like I said, there’s 1 of the trauma ICU docs that was there most of the time that I was there. And, I mean he was excellent. … but I mean there were days that he may have called me 3 times. (Participant 4, hospice) Here we are in the room, patient’s dying and there’s 3 of them outside the room…. I Get it. In that field, you have to have some fun with your coworkers, laugh, cut up…But I would not have been like that right outside the room of someone who’s actively dying. (Participant 4, hospice) It was the physician that I had the problem with, it was the physician that my family had the problem with. So I was hoping they didn’t really catch on to what she was really saying and how she was saying it and why she was saying it. Because she kind of said it in a way, “well, we need to start thinking about pulling the tube” … this is a very busy room and there’s a lot of people waiting for it. And we felt like in her mind, the minute we decided to pull the tube, she was ready for that bed to be open and she didn’t care. (Participant 28, hospital)
3.6
—
Quality of communication
I Found the communication to be very great. I Have a kind of medical background and so they let me in on the rounds and everything every morning, and kind of made sure I was on board with everything. Then me with my dad communicating, made sure that’s what he wanted and everything. (Participant 12, hospice) The problem with the communication was it wasn’t between me, my father, and the physician. It was the fact that there was a lot of different people, that worked with my father, including nurses, physician, surgeons, doctors on call. And everybody seemed to not know what the other person was saying. … but the communication I would be given, would be wrong or different, and a different thing every time someone else would come and talk to me. (Participant 20, hospice) Get your ducks in a row. Make the 1 phone call. Make sure that you’re clear and concise in your communication. Don’t try to sugar sugarcoat something for somebody. You can say something in a nice way, but be frank and let somebody know what the true situation is because they can’t make a decision that important unless they have all of the information. (Participant 28, hospital) Oh, anything I needed. They were there. They gave me their personal cell phones. I mean, I had any questions. I Would not wait for more than 5 minutes to get an answer. (Participant 18, hospice)
3.7
—
Frequency of interactions
They came around, the attending and the main surgeon and the PA or the nurse practitioner on the floor came by before rounds, they came by during rounds, and then they came by again after rounds. So they were very attuned to whatever [name] needed and how he was feeling. (Participant 14, hospice) There was no doctor there. I Never did see no doctor. I would’ve liked to have seen 1. (Participant 30, hospital)
3.8
—
Shared decision making
I Think that is very helpful for the family, for them to be included, even though they can’t understand. And I have a somewhat medical background so I understand a lot of what they were saying. …. But even just standing there and listening to it and listening to them discuss it and bring up different aspects and decide what’s going to be best for the patient, for the family, or at least a representative from the family, to be able to witness that and try to comprehend it, I think it helps a lot. (Participant 23, hospital)
3.9
Personal factors
Medical context
She died all of a sudden it wasn’t, she died in the midst of going to get her MRI. (Participant 32, hospital) I’ve been going through leukemia with her for 5 years. So, I think my emotional status is kind of, let’s just do what we got to do through here to make sure she’s getting treated correctly and getting whatever she needs. (Participant 24, hospital)
3.10
—
Psychosocial support
I mean, I went through a lot of emotion. I Had my family and friends there with me, so they kept me going with humor and things like that.. (Participant 18, hospice) I Had tremendous support. My 2 girls live in the area, and they were right with us, and our church group was right with us, and I had lots of support…. (Participant 14, hospice) And I don’t know, that experience for me, it was like it calmed me down and allowed me to get my head back in the situation. And so that little nurse, I will never forget her, other than her name, the rest of my life (Participant 19, hospice)
3.11
—
Resource utilization
I Received lots of information, which actually helped tremendously because when I was going through the physical part of grief, I thought I was having a heart attack or something…. And once I read the materials, I’m like, “oh, okay, I get it. Well, I’m going to go see my doctor anyway.” but the materials helped me out tremendously and I wasn’t having a heart attack. (Participant 18, hospice) I Think they asked us and like I told them, we had our god. We had jesus with us. We were okay. Our preacher was on the phone with us and we got back to... With our faith, I think we were okay on our own with him. (Participant 36, hospital) And of course, the grief counseling and all that is available. We haven’t felt the need to call on it, but it’s comforting to know that it's there. That we have such good support, family and friends, that we don’t feel like we’re just grasping. (Participant 14, hospice)
3.12
—
Logistical and financial considerations
Oh, back and forth, back and forth, back and forth. We live in [town name], so it’s about a 45-minute drive at good times. (Participant 14, hospice) It was pretty rough. I Was trying to maintain everything that was going on with him at the hospital plus care for my mother, so it was pretty rough. (Participant 19, hospice) I Had took off work for 1 day to just go up there and spend the night and go back to work the next day. (Participant 5, hospice) Oh, it’s been easy. My daddy left everything in a good way and we don’t have any big issues to have to overcome and it’s really been kind of a smooth sail. (Participant 11, hospice) We are also very fortunate. [Name] was retired military and we had very good insurance care. And so having to pay for all of this has not been an issue (Participant 14, hospice)
3.13
Hospice care
Perceived benefits
Anyway, so I’m very, very pro hospice care and that’s why we wanted to do this was because any help that we could get, especially for our grandchildren, my 2 daughters were with me when the hospice nurse was there when they said that they could offer help for the kids. Then we definitely said, “yeah, let’s sign up.” (Participant 14, hospice) And then the lady from the hospice did come by and talk to us, and she was very thorough. And she was, "He’s going to get the same care he’s getting here now. We’d keep him comfortable.” and then she kind of went over the additional benefits, 1 of the main ones being, there was no limit on visitors at 1 time. And up to 2 people could spend the night. (Participant 13, hospice)
3.14
—
Disadvantages
Because we still had hope. We still had hope that plasma exchange was going to help. … but he got worse. (Participant 22, hospital) I Think that last week they talked to us about hospice. But hospice, in a sense, and I’m sure that they presented it this way because they didn’t want to take away from [name] her fight if she was going to fight, and they didn’t really know if she was going to make it or not, and so they approached that topic very carefully. And I have to say they did it very well and it was only the last 3 days that they said, “this is how it could go”.... (Participant 23, hospital) I Think maybe just based off of the fact that he required so much of a respiratory need, his blood pressure, he was on a lot of vasopressors and things like that. I don’t know how much of the comfort measure timeframe would have warranted him getting multiple days, even a hospice care. He really just needed things for comfort and anxiety. And once he went on comfort, he wasn’t in a position where they saw him as in pain or anything like that.. (Participant 25, hospital)
3.15
Knowledge and beliefs
I’ve dealt with hospice with my own parent, my mother and dad and my mother-in-law. And so, I know and appreciate hospice care and know how important it is to the family to be able to have that. (Participant 14, hospice)
Care Team
Participants’ perceived quality of care received influenced satisfaction with the experience (3.1). The attentiveness of the care team to the needs of patients and their families, particularly the nursing staff, was a common theme reported by many participants (3.2).
Participants discussed instances where accommodations were made for families to be together and the positive impact these experiences had on overall satisfaction. Some participants were impressed with the accommodations made for children, whereas others expressed gratitude for accommodations made in light of COVID-19 visitor restrictions (3.3).
Participants expressed confidence in the capabilities of the care team in caring for their relative, whereas others shared their frustrations with the perceived competency of the care team (3.4). Interpersonal relationships, including emotional support provided by the care team, and the professionalism of the staff influenced overall satisfaction. In some instances, staff were perceived as unprofessional, rude, or had poor bedside manner (3.5). In addition to systems-level communication networks, the individual-level communication between patient, families, and providers, as well as the quality and effectiveness of this communication, was very important. Participants reported communication from excellent to terrible, all of which having a bearing on their perceived satisfaction. Some participants discussed the importance of clear and direct communication for patients and families without a medical background. They also expressed satisfaction with the methods of communication and the accessibility of providers when they had questions (3.6). In addition to quality of communication, frequent communication with the care team and the accessibility of physicians were important (3.7). Participants discussed the importance of shared decision making and being included in discussions and care decisions (3.8).
Personal Factors
The patient’s medical context and reason for admission, as well as the severity of their condition, played a role in managing the family’s expectations of outcomes. Examples of chronic conditions that led to the final hospital admission were: organ failure requiring transplant, cancer, and COVID-19 infection with multiple chronic comorbidities. Acute events necessitating admission included: stroke, suicide, shortness of breath, ruptured aneurysms, septic shock, and car accidents. Some participants described the shock and suddenness of death for which they were unprepared. In contrast, others discussed emotional preparedness for the outcome of death (3.9). Many participants discussed the importance of psychosocial support to their wellbeing during the end of life. Social support from family, friends, the church, or other community-based groups was an important factor for many participants. Psychosocial support provided by hospital staff and the care team also positively influenced the hospital experience (3.10). In addition to the availability of resources provided by VUMC, the decision of participants to utilize these resources played a role in their experience. Not all participants required the resources offered to them; many discussed their strong faith or existing support networks outside of Vanderbilt (3.11). Participants discussed a number of logistical and financial considerations that served as barriers or facilitators during the time of hospitalization. Barriers discussed were conflicting obligations with work, geographic barriers and travel, and existing family responsibilities. Facilitators included advanced financial and funeral preparations that minimized the family’s burden of decision making and military health insurance that reduced financial concerns (3.12).
Hospice Care
While only half of the participants enrolled in this study received hospice care, it served as a modifier of satisfaction for this group. The reasons for choosing hospice-in-place contributed to the overall satisfaction with the hospital experience. Participants discussed several perceived benefits of hospice-in-place care, including emotional support, grief counseling, keeping their relative comfortable and pain-free, the increased number of allowed visitors, and additional help navigating end-of-life planning (3.13). Participants whose relatives did not receive hospice care discussed the disadvantages and the reasons they chose not to pursue it. The most common reason for foregoing hospice-in-place care was not wanting to give up hope of recovery or take the fight away from the patient. Other participants did not believe hospice care was warranted based on the timeframe or severity of their relative’s condition. They felt that their relatives were comfortable and able to die without additional comfort measures (3.14). Existing knowledge and beliefs about hospice care was a major factor in participants’ decisions to choose hospice-in-place care. Many participants had had previous experience with other family members on hospice and were familiar with its benefits (3.15).
Satisfaction Questionnaire Results
The hospice-in-place group had a mean (standard deviation) questionnaire score of 4.54 (.76), while the non-hospice group had a mean score of 4.14 (1.00). A comparison of the 2 groups’ responses approached, but did not reach, statistical significance (P = .06).
Discussion
We investigated whether the inpatient hospice program at VUMC was associated with increased satisfaction for patients and their families. Results of the quantitative analysis approached but did not show a statistically significant difference in satisfaction, although hospice-in-place appeared to offer a slight edge over traditional hospital services. Regardless, both groups reported high satisfaction scores on the questionnaire, suggesting that both options are successful in supporting patients and families.
Participant quotes provide a deeper understanding of the experiences of patients and families. Previous studies of family member satisfaction with hospice care have identified modifying factors including: regular communication, shared decision making, quality patient care and confidence in clinicians, and emotional support provided to patients and families.14-17 Results of our qualitative analysis found many of the same factors to be important in determining overall satisfaction, but also revealed a more nuanced approach to each factor (see Figure 1). In addition to regular, timely communication, patients and families also value honest, clear, and concise communication. Effective communication networks and cross-communication between departments, as well as the frequency and method of communication, are also important. Patients and families value quality patient care and confidence in clinicians, as well as a number of other modifying factors related to the care team. Additional factors contributing to overall satisfaction were: family expectations, resource availability and utilization, institutional policies, and external barriers and facilitators, including support networks and logistical or financial considerations.
The utilization of inpatient hospice services was an important modifying factor of satisfaction for families that chose it. Many participants had previous positive experience with hospice care for other family members and were familiar with its benefits. Interestingly, the benefits of hospice-in-place discussed by participants were also found to be important factors of satisfaction described by all participants, not only those whose family members were on hospice. While all patients and their families value these factors, inpatient hospice services may be more equipped to facilitate their administration and distribution.
Limitations
A potential limitation of this study is that the findings are only applicable to the hospice-in-place program at Vanderbilt University Hospital. The results may not be generalizable to the broader Vanderbilt University Medical Center or to other institutions, and there could be a number of unrecognized biases due to how the study population was selected. Additionally, the method of sending enrollment letters and surveying the family members of recently deceased patients may have introduced response bias and therefore this study may not truly represent the experiences of the majority of Vanderbilt patients.
This study is also limited by its small sample size. A future large-scale study may be better able to determine whether there is a difference in family member satisfaction between the hospice-in-place and non-hospice groups.
Finally, because patients were not randomly assigned to conditions, the groups likely differ in other ways than receiving, or not receiving, hospice care. Questions about improved satisfaction with an in-hospital death when the patient was provided with hospice care would be more definitively answered with a randomized trial that includes multivariate matching to further control for confounding characteristics.
Conclusion
Overall, the findings of this study suggest that end-of-life care at Vanderbilt, whether hospice-in-place or traditional hospital care, is successfully supporting both patients and their families. Future research may be able to show benefits of hospice-in-place care in terms of family satisfaction when directly compared to traditional hospital care. This study adds to the understanding of patient and family experiences with inpatient hospice and end-of-life care at Vanderbilt University Medical Center, which will be valuable for hospital administrators to improve the program to most benefit patients and their families.
Supplemental Material
Supplemental Material - The Efficacy of Hospice-In-Place Care Versus Traditional Inpatient Care
Supplemental Material for The Efficacy of Hospice-In-Place Care Versus Traditional Inpatient Care by Emily Butler, Claire Hanson, Taaseen Khan, Tuzo Mwarumba, Derek Daniels, Maxim Turchan, Kemberlee Bonnet, David Schlundt, Kelly Harper, Marc Bennett, and David Charles in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material - The Efficacy of Hospice-In-Place Care Versus Traditional Inpatient Care
Supplemental Material for The Efficacy of Hospice-In-Place Care Versus Traditional Inpatient Care by Emily Butler, Claire Hanson, Taaseen Khan, Tuzo Mwarumba, Derek Daniels, Maxim Turchan, Kemberlee Bonnet, David Schlundt, Kelly Harper, Marc Bennett, and David Charles in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material - The Efficacy of Hospice-In-Place Care Versus Traditional Inpatient Care
Supplemental Material for The Efficacy of Hospice-In-Place Care Versus Traditional Inpatient Care by Emily Butler, Claire Hanson, Taaseen Khan, Tuzo Mwarumba, Derek Daniels, Maxim Turchan, Kemberlee Bonnet, David Schlundt, Kelly Harper, Marc Bennett, and David Charles in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Emily Butler
Kelly Harper
Supplemental Material
Supplemental material for this article is available online.
References
1.
WrightAAZhangBRayA, et al.Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA. 2008;300(14):1665-1673. doi:10.1001/JAMA.300.14.1665
2.
OrnsteinKAAldridgeMDGarridoMMGorgesRMeierDEKelleyAS. The association between hospice use and depressive symptoms in surviving spouses. JAMA Intern Med. 2015;175(7):1138. doi:10.1001/JAMAINTERNMED.2015.1722
3.
MasonTMTofthagenCSBuckHG. Complicated grief: Risk factors, protective factors, and interventions. J Soc Work End Life Palliat Care. 2020;16(2):151-174. doi:10.1080/15524256.2020.1745726
4.
TenoJMGozaloPTrivediAN, et al.Site of death, place of care, and health care transitions among US medicare beneficiaries, 2000. JAMA. 2018;320(3):264. doi:10.1001/JAMA.2018.8981
5.
CurrowDCAgarMRPhillipsJL. Role of hospice care at the end of life for people with cancer. J Clin Oncol. 2020;38(9):937-943. doi:10.1200/JCO.18.02235
6.
KumarPWrightAAHatfieldLATemelJSKeatingNL. Family perspectives on hospice care experiences of patients with cancer. J Clin Oncol. 2017;35(4):432-439. doi:10.1200/JCO.2016.68.9257
7.
HigginsonIJSen-GuptaGJA. Place of care in advanced cancer: A qualitative systematic literature review of patient preferences. J Palliat Med2000;3(3):287-300. doi:10.1089/jpm.2000.3.287
FeredayJMuir-CochraneE. Demonstrating Rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5(1):80-92.
11.
AzungahT. Qualitative research: deductive and inductive approaches to data analysis. Qual Res J. 2018;18(4):383-400. doi:10.1108/QRJ-D-18-00035
12.
RosenstockIMStrecherVJBeckerMH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175-183. doi:10.1177/109019818801500203
13.
DamschroderLJReardonCMWiderquistMAOLoweryJ. The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci. 2022;17(1):1-16. doi:10.1186/S13012-022-01245-0
14.
OngJBrennsteinerAChowEHebertRS. Correlates of family satisfaction with hospice care: General inpatient hospice care versus Routine home hospice care. J Palliat Med. 2016;19(1):97-100. doi:10.1089/JPM.2015.0055
15.
RhodesRLMitchellSLMillerSCConnorSRTenoJM. Bereaved family members’ evaluation of hospice care: what factors influence overall satisfaction with services?J Pain Symptom Manage. 2008;35(4):365-371. doi:10.1016/J.JPAINSYMMAN.2007.12.004
16.
HollandJMKeeneJRKirkendallALunaN. Family evaluation of hospice care: Examining direct and indirect associations with overall satisfaction and caregiver confidence. Palliat Support Care. 2015;13(4):901-908. doi:10.1017/S1478951514000595
17.
VirdunCLuckettTDavidsonPMPhillipsJ. Dying in the hospital setting: A systematic review of quantitative studies identifying the elements of end-of-life care that patients and their families rank as being most important. Palliat Med. 2015;29(9):774-796. doi:10.1177/0269216315583032
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.