
Abstract
Introduction
Personality traits, specifically neuroticism, are related to stress in surrogate decision-makers (SDMs) in outpatient settings. We hypothesized that intrinsic traits are related to SDM stress in the intensive care unit (ICU) to determine if personality considerations should be included in interventions to support SDMs.
Methods
Eligible participants (adult SDMs of non-capacitated ICU patients) completed validated questionnaires including stress (Impact of Events Scale-Revised, IES-R) and personality (Big Five Inventory, BFI) within 72 hours of ICU admission and again at 3 months post-ICU discharge (in addition to a qualitative interview). Bivariate Pearson correlations explored the relationship between BFI and IES-R at each time point (95% CI) and t-tests explored the relationship between stress and COVID-19. Mixed-methods analysis integrated qualitative and quantitative data.
Results
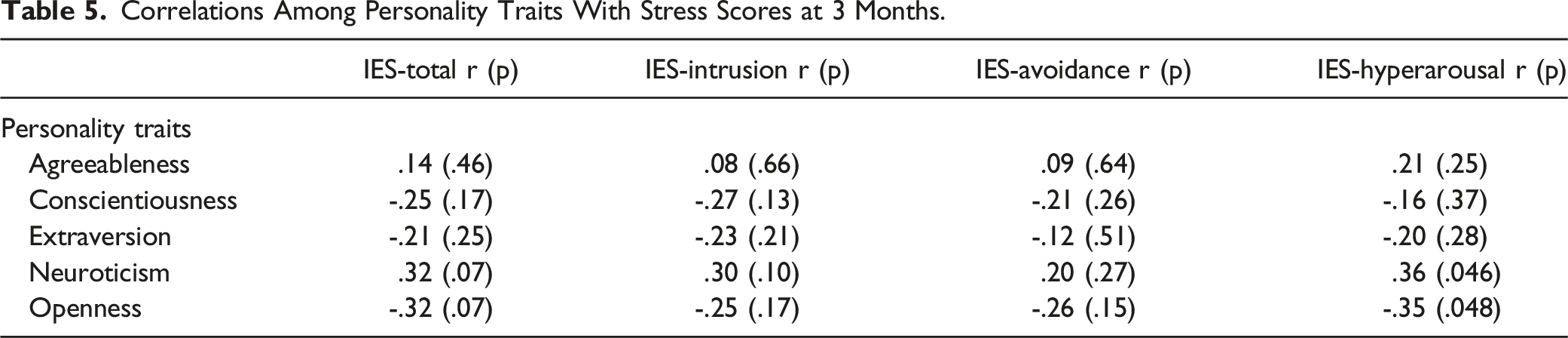
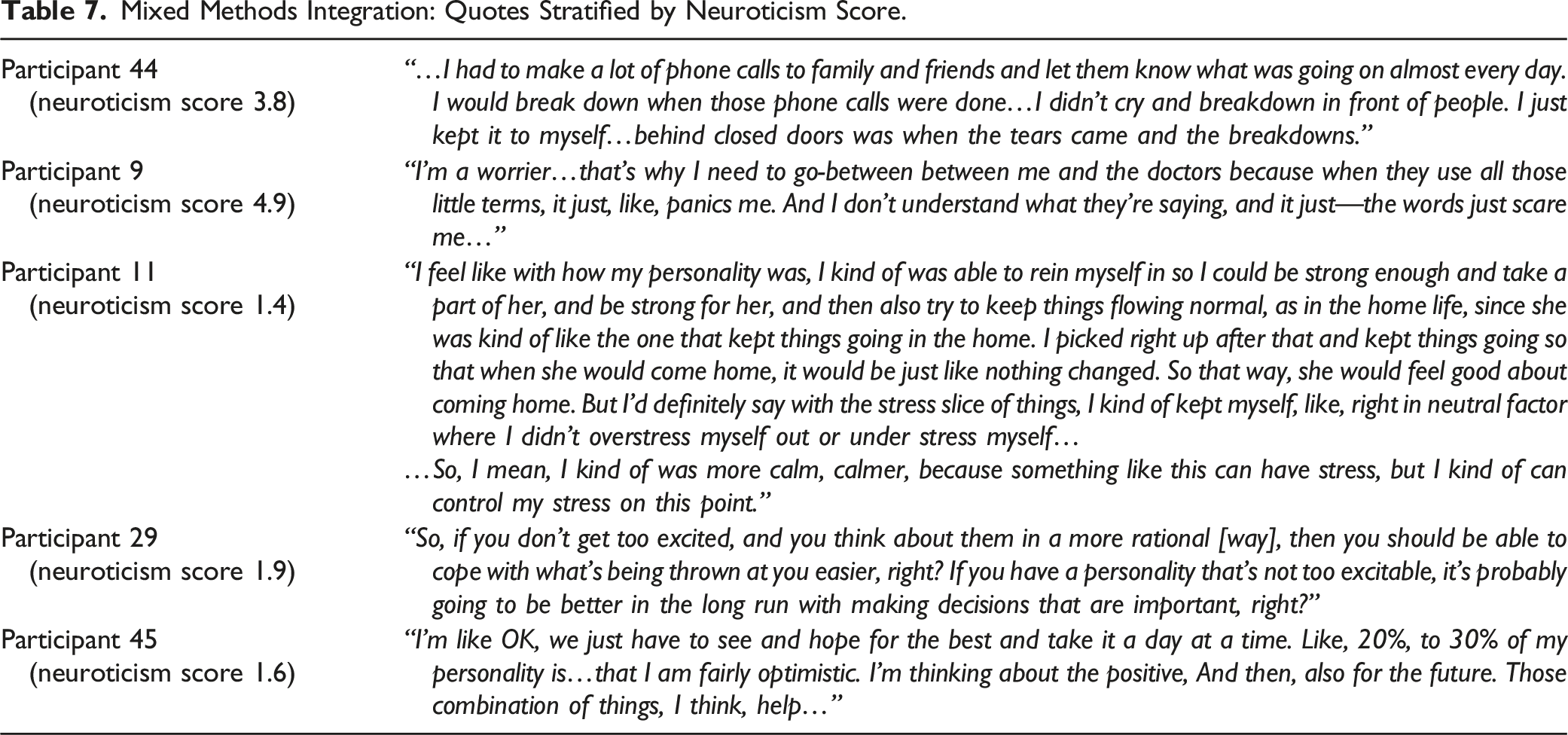
Of 32 SDMs, 71.9% were female, 93.8% white, and 97.0% were family members. Neuroticism was not significantly correlated to IES-R at 72 hours (r = 0.09; p = 0.64), but r increased 3 months post-discharge (r = 0.32; p = 0.07). Other BFI traits did not show similar patterns. Total stress was greater in surrogates of COVID-19-positive patients (COVID-19-positive: 60.6; COVID-19-negative: 49.8; p = 0.025). Mixed-methods analysis demonstrated that participants with high neuroticism scores had poorer emotional regulation than those with low neuroticism scores.
Conclusions
This study supports that personality, particularly neuroticism, influences the stress of SDMs in the ICU. Further study of personality traits may identify surrogates who are at higher risk of stress-related disorders, which can guide future interventions.
Keywords
Introduction
The experience of having a family member in the intensive care unit (ICU) can be very stressful for surrogate decision-makers (SDMs). Previous studies have shown that surrogate decision-makers for ICU patients experienced high levels of psychological and physical symptoms such as fatigue and poor appetite after their loved one was admitted to the ICU. 1 Simply receiving care in an ICU may lead to a series of complications that has been labeled post-intensive care syndrome-family, which includes post-traumatic stress disorder. 2 To address this problem, many interventions related to decision-making and decisional support have been designed and implemented. However, few have demonstrated success in reducing stress for these decision-makers. 3 This may be, in part, because the interventions used cognitive-focused approaches such as an online decisions aid and knowledge tools4,5 or are broadly targeted to any and all surrogate decision-makers in the ICU. 6 In the absence of success in interventional research, recent work has begun to focus on gaining a better understanding of how intrinsic traits such as personality traits and decision-making style impacts the way family members experience the stress of having a chronically ill loved one.4,7 Work in this area has shown that numerous factors such as finances, grief, and caregiving demands contribute to stress, which may help explain failures in current interventional approaches.6,8 To date, we have only a rudimentary understanding of how intrinsic traits (such as personality) play a role in the way families experience stress and thus, their outcomes.
It is well established, however, that personality traits, particularly neuroticism, are associated with anxiety, depression, and other conditions, such as substance abuse.9-11 Although to our knowledge there is no research on the role of personality traits in surrogate decision-making in the ICU, there has been some work in other populations. For example, a study found that caregivers of elderly, chronically ill relatives who scored higher on neuroticism were found to have higher scores of depression, anxiety, and loneliness, and lower scores of well-being when compared to other personality traits. 12 Another study found that caregivers of patients with schizophrenia experienced high levels of burden and concluded that personality traits like psychoticism (using the Eysenck’s Personality Questionnaire) 13 increase risk of caregiver burden. 14 Additionally, personality traits in parents of children with spina bifida were found to be stronger determinants of stress than the severity of the child’s disease. 15 We also recently demonstrated an association between Big Five Inventory (BFI) personality types (neuroticism, extraversion, openness, agreeableness, and conscientiousness) and psychological health in surrogate decision-makers of chronically ill patients in that the neuroticism trait was strongly correlated to stress. 7 Therefore, in light of these relationships in other caregiver populations, it is possible that personality plays a role in other contexts, such as the ICU. To our knowledge there is no literature that examines how the personality traits of decision-makers of patients in an ICU setting may relate to outcomes.
The objective of this mixed methods study is to begin to explore potential relationships between personality traits and psychological outcomes of surrogate decision-makers of ICU patients. We hypothesize that personality traits, specifically neuroticism, are associated with stress-related outcomes. Since the study was conducted in the height of the pandemic, we also explored whether stress-related outcomes were related to a diagnosis of COVID-19.
Methods
Overview of Study Design
This explanatory, sequential mixed methods 16 study was performed at a single, academic tertiary care center in Hershey, PA, from August 2021 to 2022 (during the COVID-19 pandemic). Data was collected at 2 timepoints (at 72 hours post-ICU admission, Phase 1; and at 3 months post-ICU discharge, Phase 2). Quantitative questionnaires assessed participants’ symptoms of PTSD (as measured by the validated Impact of Event Score-Revised; IES-R)17,18 and personality traits (as measured by the BFI.)19,20 Qualitative interviews were conducted to explain how participants perceived that their personality may have played a role in their stress. Surrogates were included in phase 2 regardless of patient disposition from the ICU (including death).
Recruitment
The study was approved by the Institutional Review Board (STUDY00017884). Participants were identified by first screening ICU censuses for patients meeting inclusion criteria receiving care in the medical intensive care unit (MICU), neurological critical care unit (NCCU), Heart and Vascular Institute critical care unit (HVICCU), and surgical intensive care unit (SICU). Inclusion criteria for patients were age greater than 18 years, had a projected ICU stay of greater than 72 hours, and determined to be medically non-capacitated by the healthcare team. Upon identification of patients, the care team identified the surrogate decision-makers of the selected patients. Inclusion criteria for surrogate decision-makers were age greater than 18 years and able to read and write in English. Eligible participants were approached by a research assistant either in person or by phone, depending on availability of the surrogate. Surrogates provided verbal informed consent and could withdraw at any time.
Measures
Demographics and Chart Review
An 18-item questionnaire was completed at baseline to determine the surrogate’s age, gender, race and ethnicity, education level, and relationship to the patient. Surrogates answered a similar set of questions for their loved one.
Personality: Big Five Inventory
Surrogates’ personality traits were measured using the BFI,19,20 a well validated and reliable questionnaire of the five main domains that correspond to thoughts, feelings, and behaviors. Each of the 44 items has a stem beginning with “I see myself as someone who…[e.g., is talkative.]” Participants choose from a 5-point Likert scare as to their level of agreement (1 = disagree strongly; 5 = agree strongly) with each subsequent characteristic. The BFI measures five domains: extraversion, neuroticism, openness to experience, agreeableness, and conscientiousness. Scores are calculated as averages of the scale-specific item responses (ranging from 1-5).19,20 Higher scores correspond to greater levels of that specific personality trait. Surrogates completed this survey once at 72 hours of their loved one’s ICU admission.
Subjective Stress (Symptoms of PTSD): Impact of Events Scare-Revised
The Impact of Events Scale-Revised (IES-R) is a validated 22-item questionnaire that screens for stress-related symptoms including post-traumatic stress disorder (PTSD).17,18 The IES-R was administered at 72 hours of SDMs’ loved one’s ICU admission and at 3 months post-ICU discharge or death. Each item is scored on a 0-4 scale; total scores range 0-88. Total scores of 24-33 indicate subthreshold symptoms of PTSD and scores above 33 are suggestive of PTSD.17,18 The measure contains three subscales that distinguish different stress responses: intrusion (intrusive thoughts, nightmares, intrusive feelings and images, dissociative-like re-experiencing), avoidance (numbing of responsiveness, avoidance of feelings, situations, and ideas), and hyperarousal (anger, irritability, hypervigilance, difficulty concentrating, or a heightened startle response).17,18
Qualitative Interviews
Surrogates also participated in semi-structured interviews 3 months after ICU discharge (see Qualitative Interview Guide in supplemental materials). The interview assessed three constructs: their self-described personality, how their personality related to their stress and coping, and their perceptions of how their personality affected their decision-making. Interviews lasted an average of 22.2 minutes (SD 6.1) and were audio-recorded and transcribed verbatim.
Chart Review for Patient Hospitalization and Outcomes
A chart review was completed on each patient to record age, sex, diagnosis for admission, COVID-19 status, sequential organ failure assessment (SOFA) score and code status on admission, and hospital and ICU length of stay. We also recorded patient ICU discharge disposition or death.
Analysis
Sample Size Determination
Sample size was calculated in terms of precision for estimating a correlation coefficient with an expected correlation coefficient of .5, based on correlation coefficients from prior work.
7
A sample size of 29 participants (assuming two completed timepoints) provides a 95% confidence interval that has width ±.4. In addition, for a two-sided, .05 significance level, paired t-test, the sample size of 29 yields 80% statistical power for detecting an effect size of .54 standard deviation units. Forty-three participants completed questionnaires at 72 hours (Phase 1). Given that 11 participants were lost to follow-up, 32 participants completed Phases 1 and 2 and were included in the final analysis (Figure 1). Consort diagram demonstrating recruitment and retention.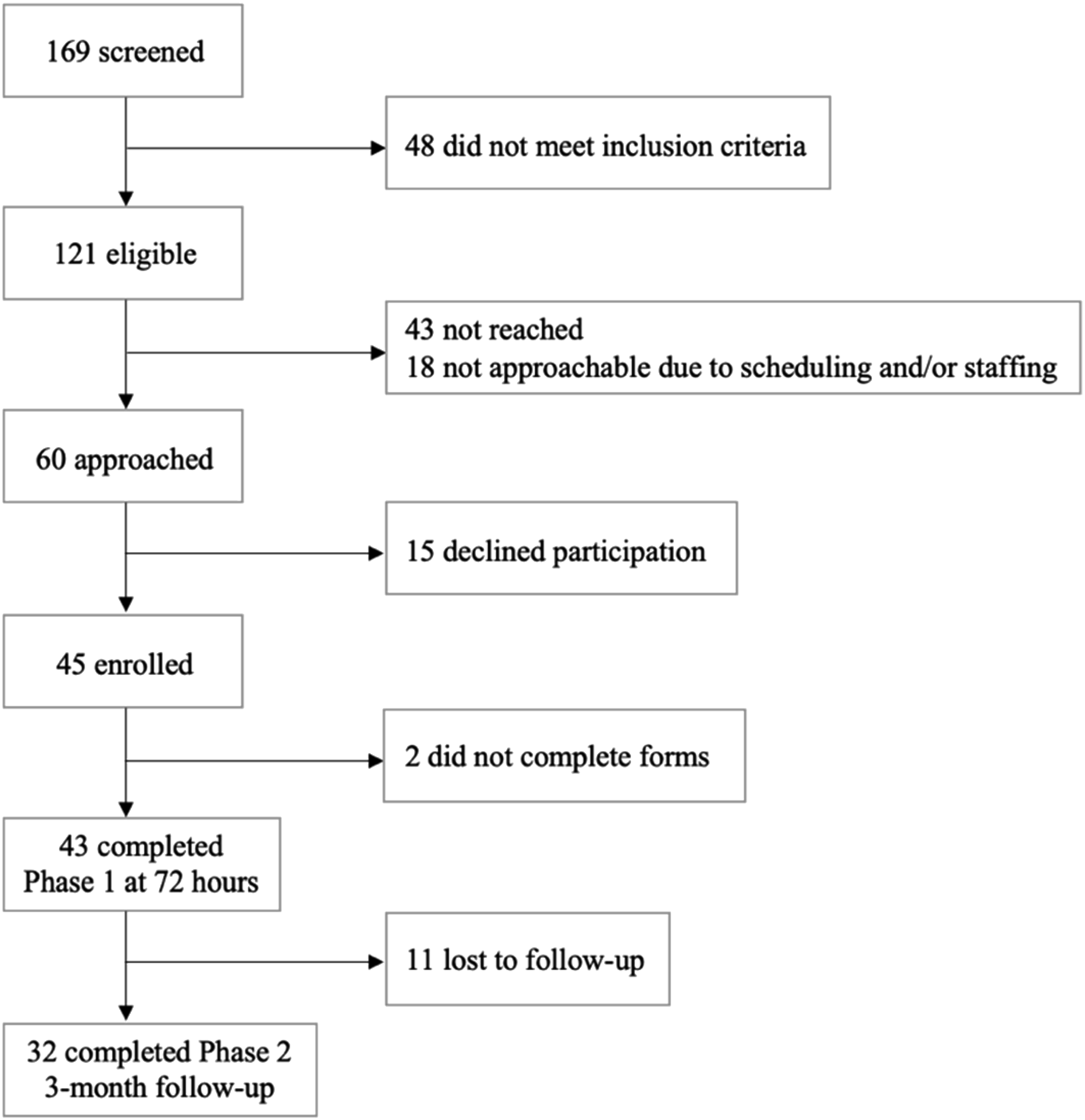
Quantitative Analysis
All quantitative analyses were performed using SPSS Statistics software, version 29.0.0.0 (241). Descriptive statistics were assembled using mean and standard deviation. BFI and IES-R scores were calculated as described in the measures section; means and standard deviations are reported for all BFI traits, total IES-R, and all IES-R subdomains. Bivariate Pearson correlations were performed using a 95% confidence interval to explore the relationship between surrogates’ personality and stress. We performed independent t-tests to determine the relationship between COVID-19 status and total stress. Our analyses excluded participants that did not complete all questionnaires or were lost at 3-month follow-up.
Qualitative Analysis
We applied a phenomenological approach16,21 to conventional content analysis. To do so, analysts independently reviewed transcripts and inductively created preliminary categories and codes. The two analysts then merged codes together to refine the codebook and jointly wrote definitions for each code. Both analysts then used the final codebook by each independently coding the entire dataset using MAXQDA software (Version 2022). Inter-rater reliability was assessed using Cohen’s Kappa reports to guide calibration and resolution of coding discrepancies between coders to maintain kappa >.70 for each code. Final coding reports and patterns were used to generate the final themes. Only themes and subthemes related to this study’s research question are presented. Additional themes (for example, ways surrogates make decisions unrelated to personality, factors that influence decisions, and perceptions about communication) will be reported separately.
Mixed Methods Analysis
In this explanatory, sequential mixed methods study, quantitative findings were analyzed and interpreted first. 21 Then, qualitative themes were integrated by connecting the quantitative data to the qualitative themes by stratifying the themes based on relevant personality traits as measured by the BFI. 22
Results
Participant and Patient Demographics
Demographics of Surrogate Decision-Makers (SDMs).
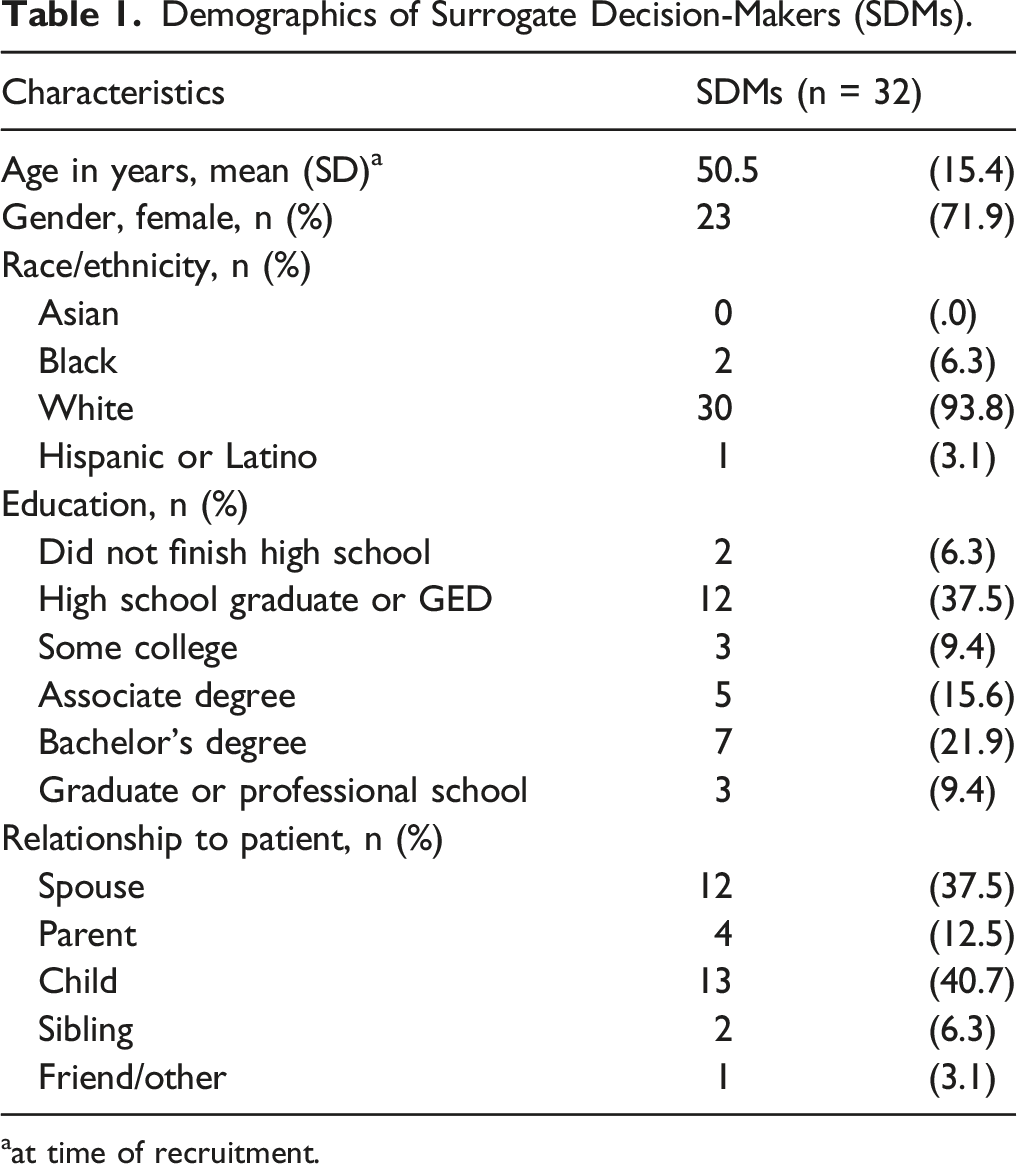
aat time of recruitment.
Patient Characteristics.
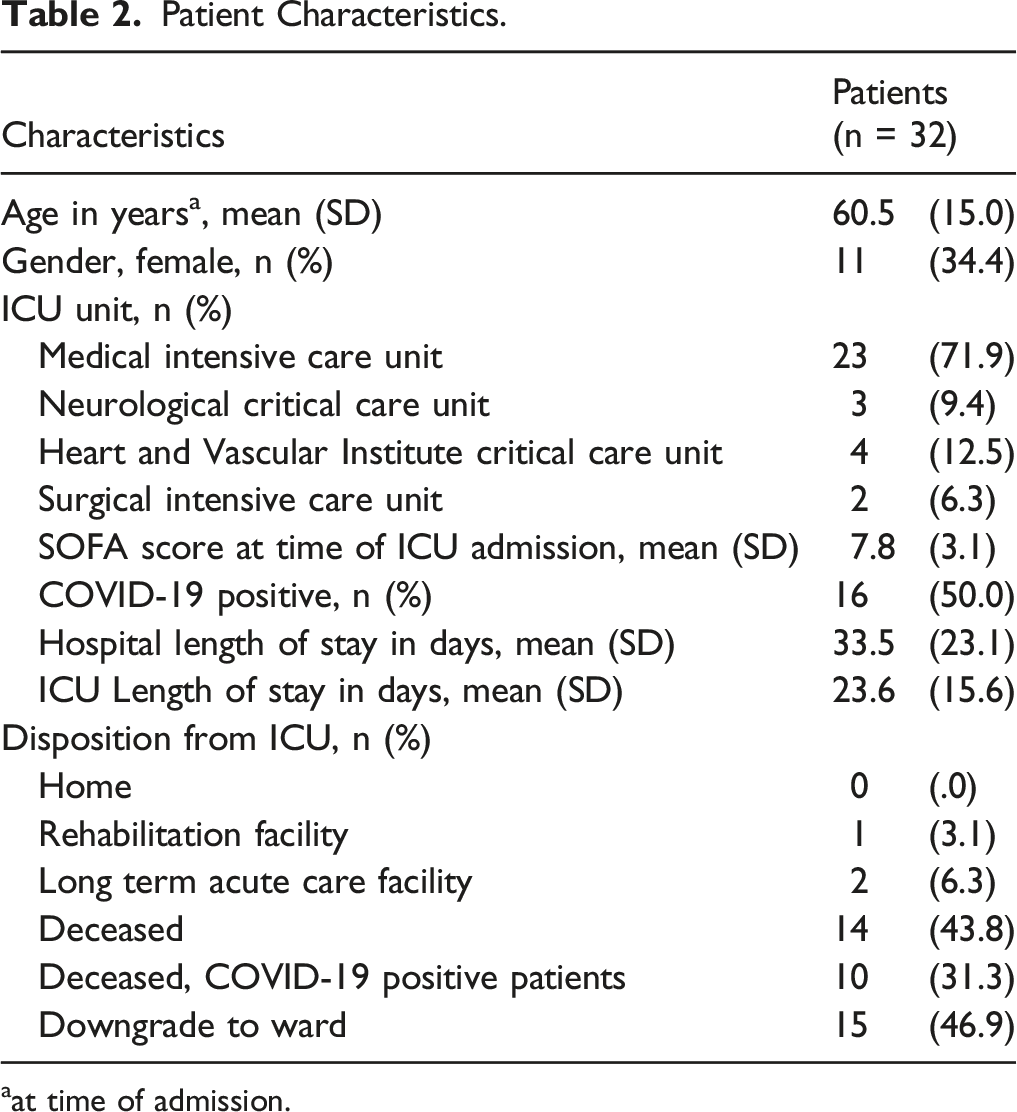
aat time of admission.
Personality Traits and Stress
Descriptive Statistics Reporting Responses on Intrinsic Traits of Stress of Participants. a
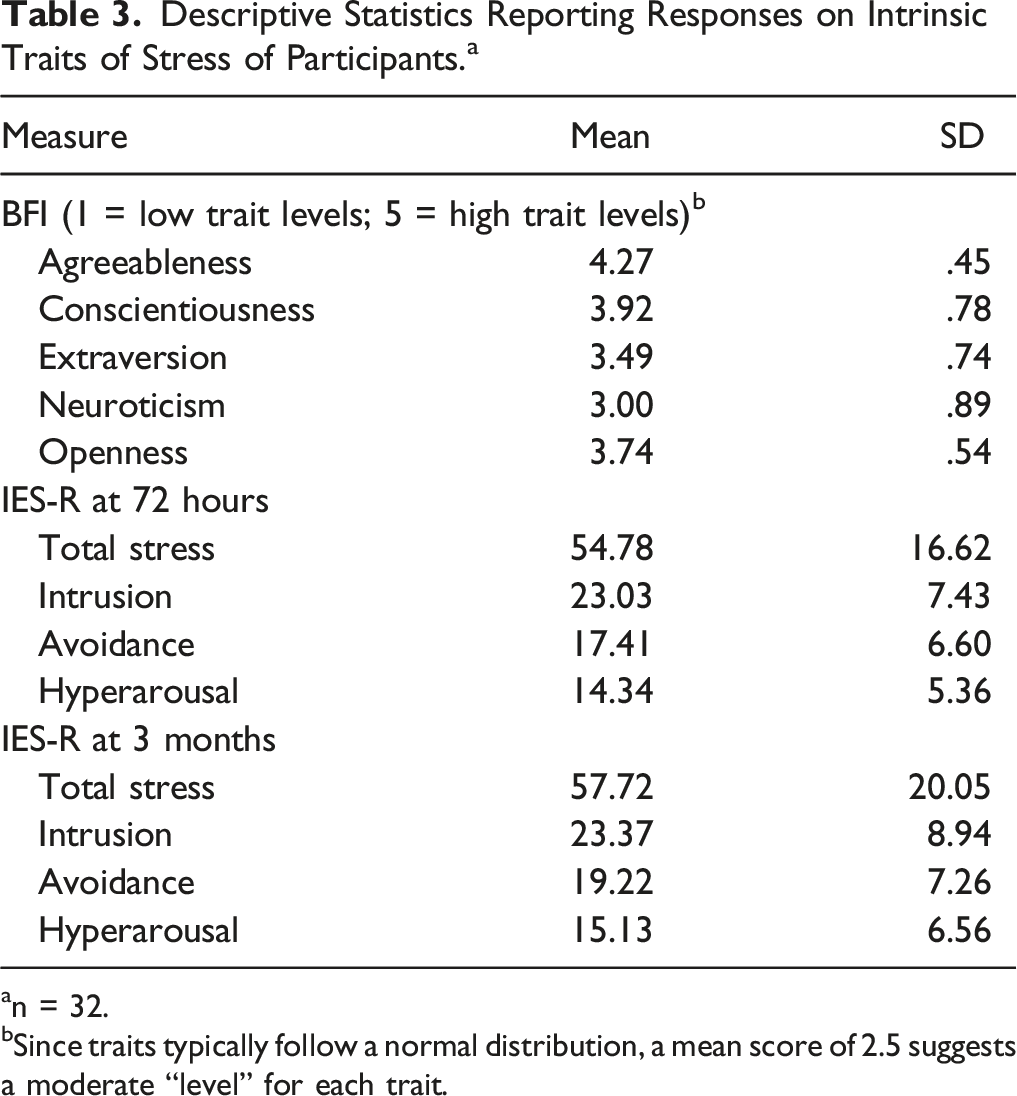
an = 32.
bSince traits typically follow a normal distribution, a mean score of 2.5 suggests a moderate “level” for each trait.
Correlations Analysis: Relationships Between Stress and Personality Traits
Correlations Among Personality Traits With Stress Scores at 72 Hours.
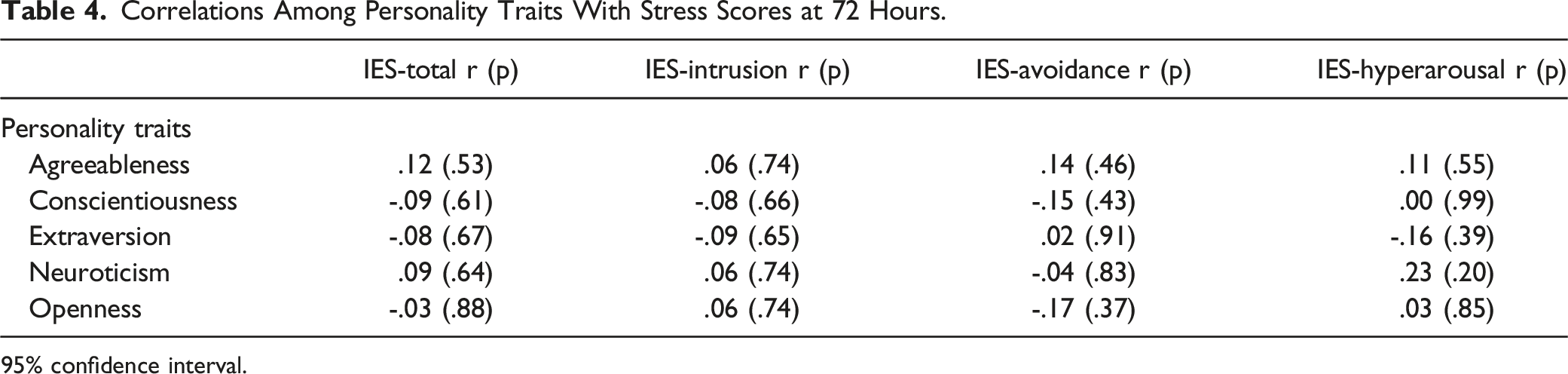
95% confidence interval.
Correlations Among Personality Traits With Stress Scores at 3 Months.
Relationship Between IES-R and COVID-19 Status
Sixteen patients (50.0%) were positive for COVID-19 (Table 2). In response to this observation, we conducted a sub-analysis to determine the role of this diagnosis. At 72 hours and 3 months, total IES-R was not significantly different in surrogate decision-makers of patients with COVID-19 compared to those without COVID-19 (72 hours: P = .10; 3 months: P = .46) (eTables 1 and 2 in supplement). When including all participants who completed Phase 1 (n = 43), total IES-R was higher in decision-makers of patients with COVID-19 than those without COVID-19 (COVID-19-positive: 60.6; COVID-19-negative: 49.8; P = .03) (eTable 3 in supplement).
Qualitative Interviews
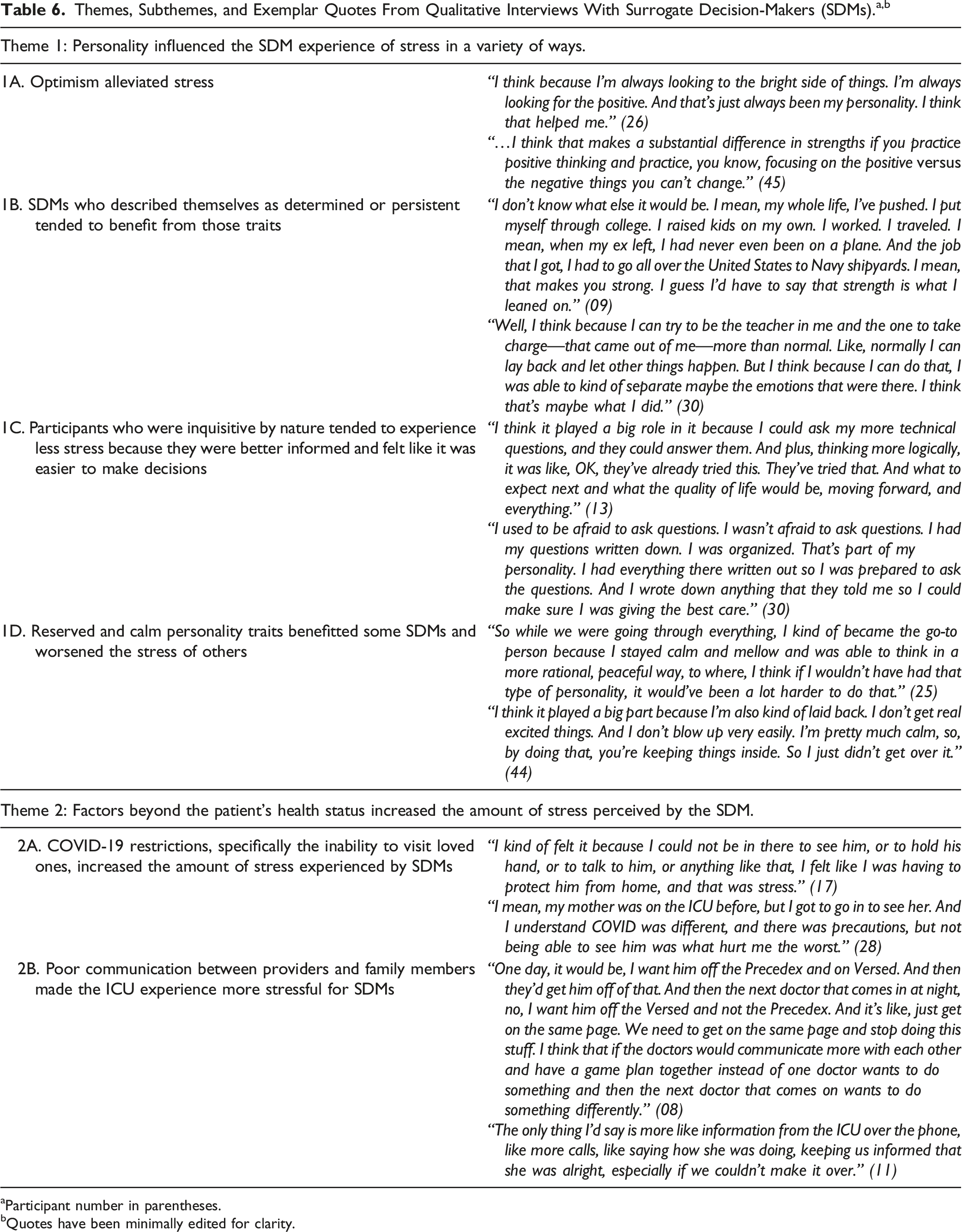
aParticipant number in parentheses.
bQuotes have been minimally edited for clarity.
Theme 1: Surrogates described their personality traits as both a benefit and detriment to their experience of stress
Participants described that the optimistic, determined, and inquisitive components of their personalities improved the ICU experience (Subthemes 1A-1C). Some surrogates who described themselves as reserved found this trait to be helpful, while others found it to be a mechanism of concealment of their emotions (Subtheme 1D).
Theme 2. Factors beyond the patient’s health status increased the amount of stress perceived by the SDM
A substantial proportion of participants cited visitation restrictions as a major stressor during their loved one’s admission (Subtheme 2A). Insufficient communication, both between healthcare teams and between families and providers, also contributed to surrogates’ stress (Theme 2B).
Mixed Methods Integration
Mixed Methods Integration: Quotes Stratified by Neuroticism Score.
Discussion
To our knowledge, this is the first study to examine potential relationships between personality traits and stress in the context of ICU surrogate decision-making. Understanding the stress experience is important because poor psychological outcomes (such as anxiety, depression, and PTSD) are known to be prevalent in surrogate decision-makers of ICU patients. 1 Prior research seeking to support family members and improve these psychological outcomes after decision-making has had mixed results.4-6 Given that the association of personality traits of surrogate decision-makers and stress have been demonstrated in other settings,7,11,23 we investigated the relationship between personality and stress in the ICU setting. This study did not demonstrate a quantitative relationship between personality and stress, although qualitative findings provided some insights into how participants view the way their personality played a role in their ICU experience, suggesting that a relationship may be present. Thus, although the study was underpowered to detect quantitative associations, the qualitative data helped elucidate a potential relationship. When we integrated our mixed methods data, we found that participants with low scores on the neuroticism scale seemed to describe better emotional regulation (using layman’s terminology) than those with high neuroticism scores. This is notable because the relationship between poor emotional regulation and neuroticism is well-established. 10
In addition to being underpowered, it is possible that our quantitative data did not yield significant relationships as a result of the high-stress, life-or-death nature of the ICU experience. The high-stress experience of the ICU may have simply overrode any relationship between personality and stress in this context. Further, the COVID-19 pandemic, which introduced additional stresses and potentially confounding issues related to visitation restrictions may have impacted our findings.24,25 Our sub-analysis exploring the role of COVID-19 found that decision-makers for patients with COVID-19 did indeed have higher stress scores than those without COVID-19. Thus, the impact of the COVID-19 pandemic may have ‘washed out’ the relationship between personality and stress.
Strengths and Limitations
Strengths of this study include the use of a well validated personality index and a mixed methods approach that provided insight not yielded from the quantitative findings alone. This study was limited by small sample size, lack of power, and a non-diverse, largely white, female population. Further, our power calculations did not include considerations for multiplicity corrections, and COVID-related analyses were post-hoc; thus findings should be interpreted with caution. Last, additional confounders that may have contributed to participants’ perception of stress, including death or final disposition, social support systems, family dynamics, and illness narrative and disease type, among other variables, were unmeasured.
Implications for Clinical Practice
Our findings suggest that it might be beneficial to consider personality traits when designing interventions intended to support surrogate decision-makers in the ICU. Surrogates may respond well to interventions tailored to their personality trait profiles since personality is linked to coping and emotional regulation.26-28 Further, using a personality assessment (such as the Big Five Inventory) may help to quickly identify individuals with personality profiles at highest risk for poor psychological outcomes using this brief and simple screening tool. Such screening would permit a tailored approach to surrogate support that attends to personality traits and may help address poor psychological outcomes associated with ICU surrogate decision-making. More research in this area is warranted to further elucidate if and how personality traits play a role in the ICU experience. Thus, attending to the wide range of needs of surrogate decision makers, rather than a ‘one-size fits all’ approach, may help to improve interventional efficacy.
Conclusion
Personality traits, particularly neuroticism, may influence the stress experience in surrogate decision-makers of ICU patients. Research to understand if and how personality traits relate to psychological outcomes and decision-making may help improve efficacy of interventions intended to support surrogates of ICU patients.
Supplemental Material
Supplemental Material - Relationships Between Personality Traits and Perceived Stress in Surrogate Decision-Makers of Intensive Care Unit Patients
Supplemental Material for Relationships Between Personality Traits and Perceived Stress in Surrogate Decision Makers of Intensive Care Unit Patients by Brody Greenleaf, Andrew Foy and Lauren Van Scoy in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
We thank the following people for their assistance in this study: Maria Katsaros, Morgan Loeffler, Pamela Witt, and the Penn State College of Medicine Qualitative and Mixed Methods Core. We also would like to thank Drs. Vernon Chinchilli and Chloe Bliton for their expertise on biostatistics and personality traits, respectively.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences (UL1 TR002014).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.