
Abstract
Background
Palliative Care also encompasses the dimension of spiritual pain. Pastoral care workers and chaplains are specialists in the provision of spiritual care. Decreasing religious affiliation and increasing spiritual diversification in modern societies raise the question of the function of pastoral care.
Aim
The goal of this study is to answer the question of what pastoral care workers can offer to dying residents in hospices and palliative care units.
Design
A qualitative interview study was designed to explore the specific perspective of pastoral care workers in a multidisciplinary environment. The study is based on differentiation theory which is particularly well adjusted to reveal differences in perspectives in so called ‘holistic’ care settings. The reporting follows the COREQ guidelines.
Setting
Problem centered interviews were conducted at five hospices and two palliative care units.
Results
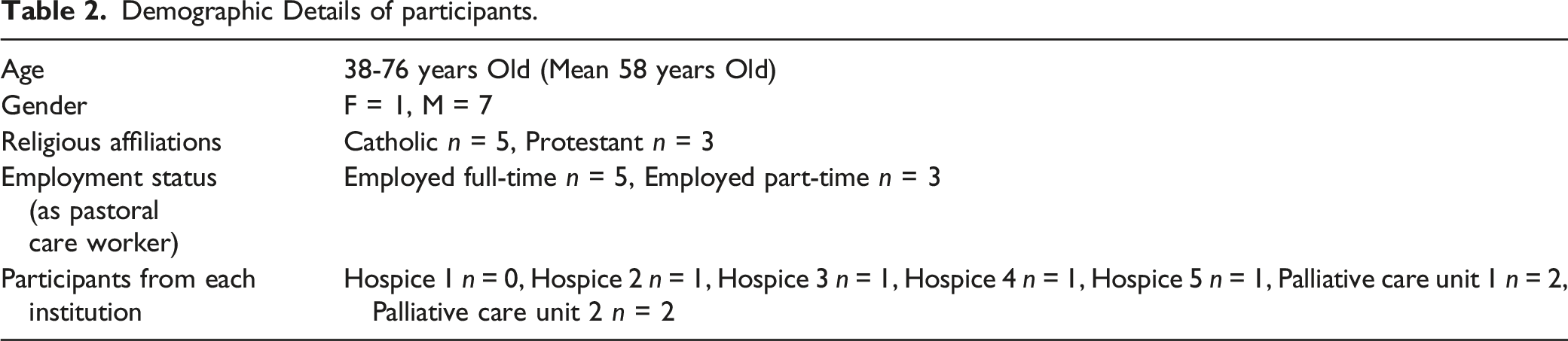
Eight pastoral care workers were interviewed (5 Catholic, 3 Protestant, mean age of 58 years). The analysis of the interviews revealed three major themes: (A) Self-positioning in relation to the organization, (B) Offering conversations to patients and relatives, (C) Performing religious rituals. Minor themes were: mediating conflicts between patients, relatives and staff, sensing moods in silence with patients and organizing workshops for staff.
Conclusion
In modern hospice care, pastoral care workers routinely address the problem of making death more tangible and of answering the unanswerable question of what comes afterwards. Through this, they support dying residents in hospices and palliative care units in dealing with the inexplicability of death.
Introduction
Pastoral care workers and chaplains play a fundamental role when it comes to the provision of spiritual care in hospice and palliative care. Apart from physicians, pastoral care workers are the only professional group in palliative care that are descendants from the long tradition of the ‘classic’ professions. 1 Historically, their task was to treat the problem of theodicy 2 and to perform rituals at the deathbed. 3 Today, pastoral care workers and clergy are facing the challenge of simultaneously holding up religious traditions while also adapting to a changing societal environment and – especially in the German context – to an increasingly secular clientele. Yet, there remains a relatively strong demand for spiritual or religious interventions of pastoral care workers in palliative care, even though the percentage of patients and family members with strong religious beliefs has progressively decreased.4-6 Following a functional understanding of religion, 7 this can be considered as an indication that pastoral care workers address a problem in a modern and differentiated society that goes beyond the scope of spiritual or religious confessions.
Religious affiliations of the general population in Germany have been in decline for several decades – only 10% state that religion is very important in daily life. 8 World views have become increasingly secular and religiously diverse. 9 Particularly the population of the eastern regions (former GDR) remains distanced towards religion. 9 Thierfelder argues that these secular tendencies lead to an increasing popularity of the term “spiritual care”, which seems to replace the traditional theological German term “Seelsorge” (Soul Care). 10
According to the concept of total pain, spiritual pain is a distinct type of pain that is considered to be equally as important as other types of pain. 11 The concept of spirituality is often connected to a dying patient’s need for meaning, purpose, transcendence and hope. 12 There is a growing body of evidence which emphasizes the importance of spiritual care.13,14 On the basis of this evidence, important practice recommendations for the treatment of spiritual pain through pastoral care workers have been developed. 15 Even though physicians, nurses, social workers or hospice volunteers should all provide spiritual care as part of comprehensive palliative care,16,17 the treatment of spiritual pain is considered to be the professional domain of pastoral care workers.
While the current body of literature is quite impressive regarding the evidence gathered for positive effects of spiritual care provision by chaplains and pastoral care workers, there seems to be an answer missing to the question of why the demand for pastoral care workers is still high and what they specifically offer in a modern, mostly secular society. With a functional perspective, this question can be rephrased as: which problem do pastoral care workers attempt to solve?
Methods
Research Question
What do pastoral care workers offer to dying patients in hospices and palliative care units?
Design
The research was carried out as an exploratory and qualitative study. The design is based on differentiation theory. The sociological differentiation theory is the longest-serving concept of a theory of modern societies, which has undergone numerous changes since the classics of the discipline (Durkheim, Weber, Simmel, Parsons) and probably culminates in Niklas Luhmann’s sociological systems theory. 18 This theory is of particular interest for qualitative empirical research insofar as it allows to observe the difference between professional perspectives, speaker positions, validity claims and interests seriously and with theoretical expertise, especially in fields characterized by multidisciplinary settings and different perspectives. 19
Setting
The interviews were conducted at five hospices and two palliative care units. Only one hospice was not affiliated with any religion.
Participants
The selection process of study centers was focused on nationwide coverage (North, South, East, West). Included as participants in this study were pastoral care workers with frequent contact with patients. Consequently, the criteria for exclusion were little experience in palliative care and/or little contact with patients.
Sampling
The study design is aiming at the observation of typical patterns in the data material. To achieve this, the sample must remain homogenous.
Recruitment
For the selection of participants, the project was presented during the multi-professional staff meetings. Relevant staff members were asked to participate. There were no interactions with the participants prior to the study.
Data Collection
Problem Centered Interview Protocol.

Analysis
The data analysis was guided by the principles of functional analysis.21,22 Recurring patterns and themes indicate an issue being addressed by the participants, that is a constitutive part of what we consider to be a perspective. We are interested in how different perspectives emerge and stabilize themselves through describing and addressing different problems (see design). This is what we call the function of a specific perspective, which is, in this case, the pastoral care workers perspective
To achieve this, the transcripts of the interviews were analyzed with MAXQDA 2022. They were coded in a two-step process: The first step was an exploratory reading of the interviews, freely coding the material (open coding). After that, the different codes were reduced to three to five major themes with corresponding categories and subcategories for each participant group (axial coding). Here, the definition of a major theme was that a certain topic was mentioned in every interview of one participant group. For example, all pastoral care workers talked about conversations with patients and relatives, which means that this is clearly a major theme in the material. Minor themes were also coded. These are topics that come up repeatedly but not in every interview. During the coding process, the themes, categories and subcategories were modified and revised. Table 3 represents the final coding tree. Figure 1 is a visual representation of the research process. The analysis was reflectively accompanied by repeated data sessions of the research team (two full professors, one of them a theologist, one senior researcher, three research assistants, three student assistants: 3 male, 6 female). There was no feedback on the results by the participants in the study. Flowchart of the research process.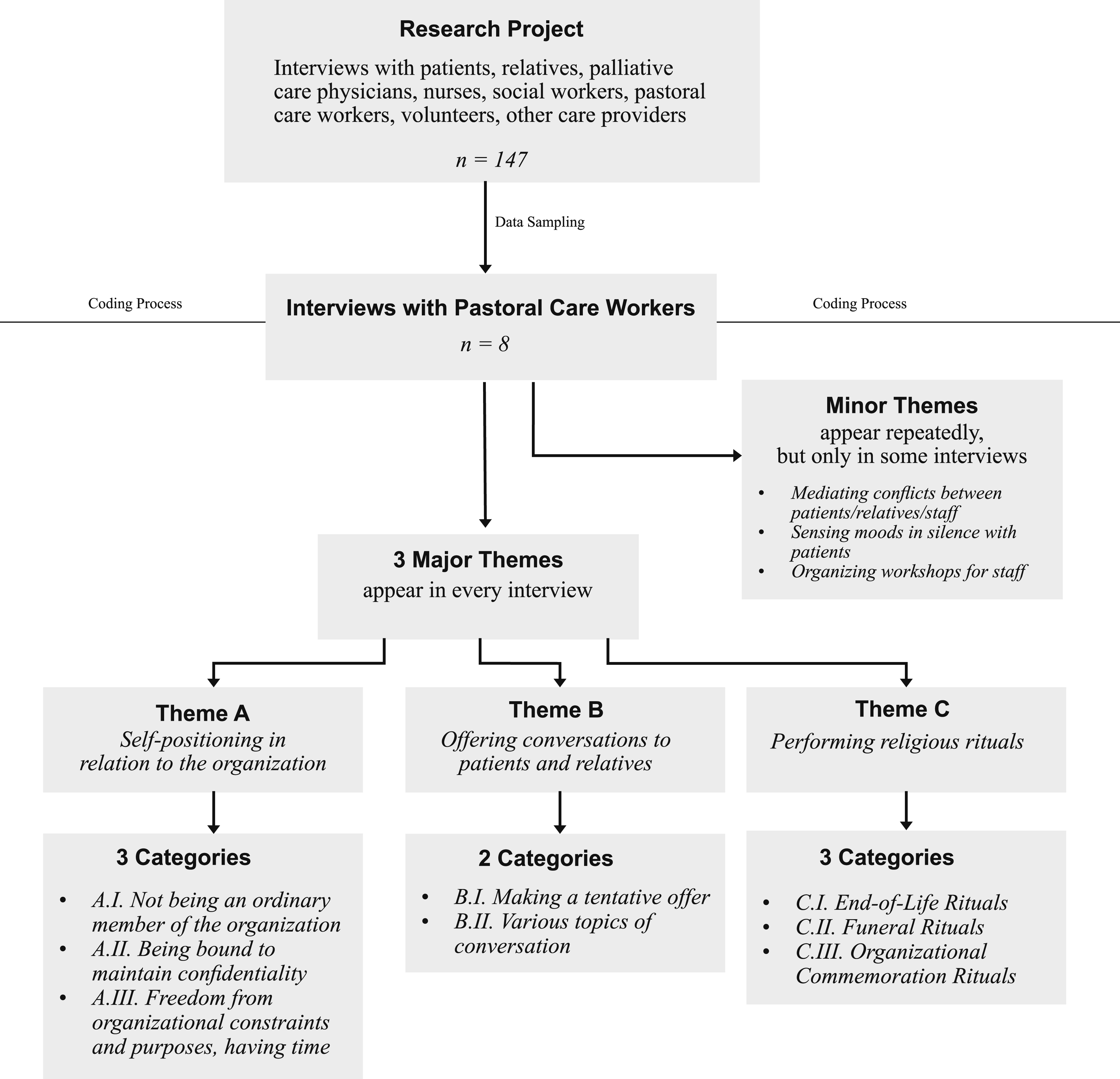
Ethical Issues
The study was approved by the Ethics Committee of the Faculty of Medicine at LMU Munich (Az-558-15, 30.11.2017). All participants were provided with information both on the project and on data-protection. All participants confirmed that they were willing to participate in the study.
Results
Demographic Details of participants.
Themes
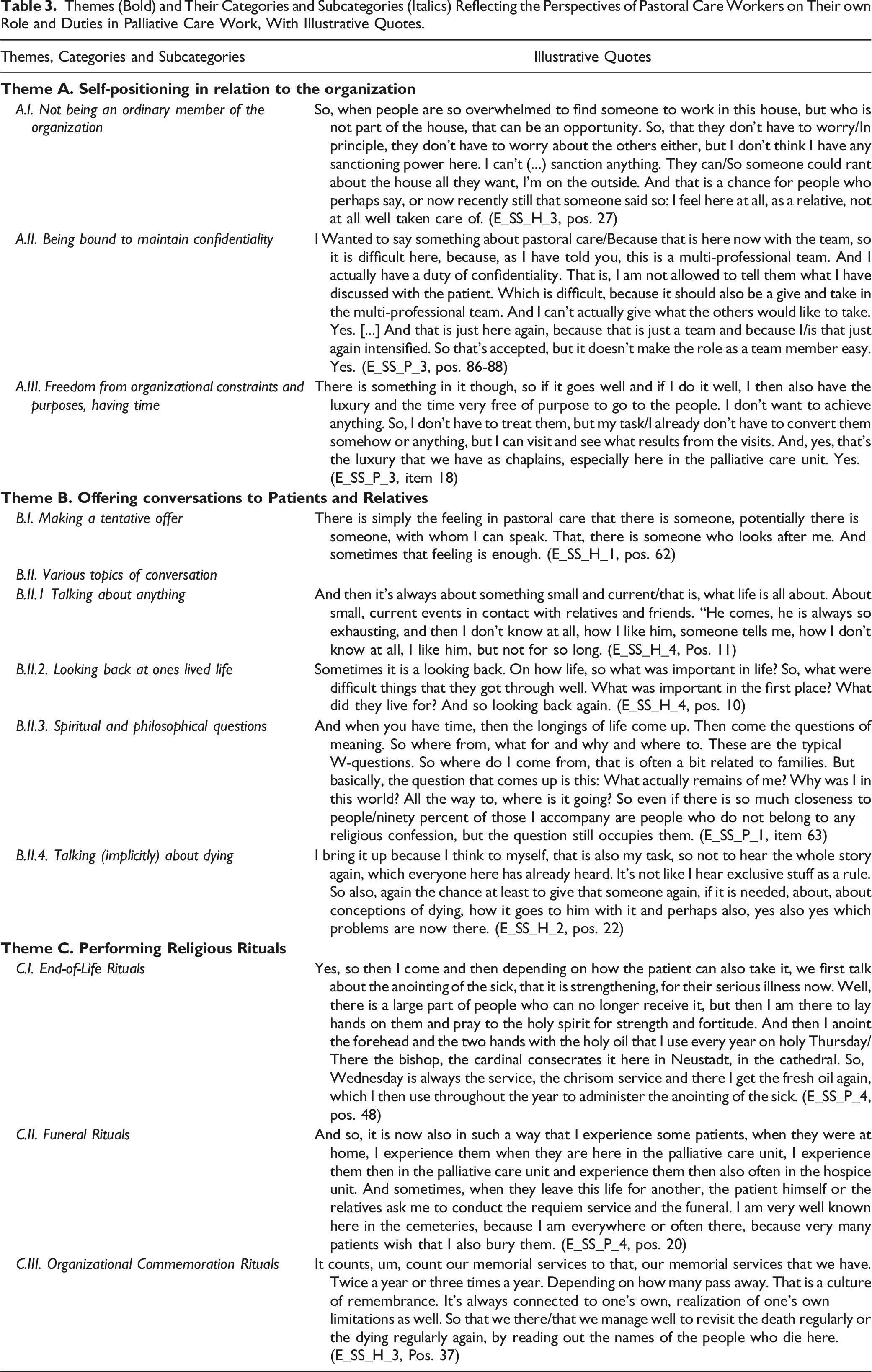
Three major themes emerged from the pastoral care workers’ statements and are presented in Table 2 with examples. Minor themes were about mediating conflicts between patients/relatives/staff, sensing moods in silence with patients and organizing workshops for staff.
Theme A: Self-Positioning in Relation to the Organization
Not Being an Ordinary Member of the Organization
Themes (Bold) and Their Categories and Subcategories (Italics) Reflecting the Perspectives of Pastoral Care Workers on Their own Role and Duties in Palliative Care Work, With Illustrative Quotes.
Being Bound to Maintain Confidentiality
In the interaction with patients, this confidentiality opens a situation of mutual trust in which the patients and residents can “tell the chaplains the most personal things” (E_SS_P_1, pos. 107). This repeatedly leads to the question, “What of this am I allowed to say to the team now, and what falls under pastoral confidentiality?” (E_SS_P_1, pos. 107) Thus, the pastoral care workers describe that they participate only to a limited extent in the open exchange of information about the patient during the multi-professional team-meetings. One pastoral care worker described this as “difficult [...], because there should also be a give-and-take in the multi-professional team. And I can’t actually give what the others would like to take. [...] So this is accepted, but it doesn’t make the role as a team easy” (Table 3, A.II.).
Being Free From Organizational Constraints and Purposes, Having Time
Freedom from organizational constraints and “freedom of purpose” (E_SS_P_2, pos. 66) are central to pastoral care in the interviews. Pastoral care workers are not bound to strict procedures or tasks and do not have to achieve any specific results in the organizational context: “do not treat”, “do not achieve anything” (Table 3, A.III.). Their field of activity is initially undefined and arises situationally onsite in contact with the patients who want to take up the offer of pastoral care. Pastoral care workers are able to spend a lot of time with the patients, but they are free to decide in which way they want to spend their time: “Yes, so that is then our area, isn’t it? Where then perhaps someone says: 'Yes, what should I do now?' Can the pastoral care here perhaps take the time to do nothing and this doing nothing, so sitting there and looking at the person or perhaps saying a word, this is perhaps in the end nevertheless an important action, or an important situation, even if thereby no decisive act comes out more or so” (E_SS_P_2, pos. 98)
Theme B: Offering Conversations to Patients and Relatives
Offering and holding conversations seems to take up most of the pastoral care workers’ time. This task is mentioned frequently in all interviews.
Making a Tentative Offer
The decisive factor for the emergence and course of the conversations is the focus on the needs of the patient. Above all, an offer should be made that can be accepted regardless of the patient’s denomination but can also be rejected without negative consequences: “It is an offer that is open to everyone. It is not forced on anyone, but is intended to open up a possibility, a space, in order to...yes, in order to enter into conversation.” (E_SS_H_1, pos. 20) One’s own role as a pastor can be an obstacle if it is directly associated with death or religious proselytizing: “So if I say that I am the pastor here, then it can happen that someone in our environment is frightened and says, either I’m about to die now or someone wants to proselytize me, right?” (E_SS_P_2, pos. 14)
Topics of Conversation
The content of the conversations is also determined by what the patients bring to the conversation. Often it is about everyday things, sometimes they look back on life, sometimes spiritual or philosophical topics are discussed, sometimes dying itself becomes an explicit topic (Table 3, B II). In this context, dying is described by pastoral care workers as a topic that is “in the air” based on the organizational context (E_SS_P_3, pos. 26) and is also always present in an unspoken and implicit way. The purposelessness of the conversations, which is emphasized again and again, gives the conversation a value independent of the content. Thus, it is just as possible to talk about the Football World Cup with pastoral care workers as it is to talk about dying: “So, if I chatter away […] let’s say about the World Cup, then I don't have to have a bad conscience afterwards, right? That I have now frittered away my time with them.” (E_SS_P_2, pos. 72) “[…] up to the question, which comes again and again, which representatives of the church have to answer all the more. ‘Do you really believe that there is something more?’ Yes? Then you are automatically in this conversation. The important thing is not to avoid it then.” (E_SS_P_1, pos. 131).
The assumption here is, that anything the patient wants to talk about can be discussed with the pastoral care workers, but there are also typical questions addressing the specific role of the interviewee like the ultimately unanswerable question of what comes after death.
Theme C: Performing Religious Rituals
Performing religious rituals in the palliative care organizations is mentioned as a very important domain in all interviews and described as a ‘unique selling point’ of the pastoral care workers as “official messengers of the church” (E_SS_H_2, pos. 104). “So, based on the profile it is, as a pastor you have something of your own [...]. That is something that nobody here can or is allowed to do” (E_SS_P_3, pos. 92).
End-of-Life Rituals
In the interviews, (religious) rituals at the end of life are mentioned, which are supposed to be meaningful and comforting for the patients and relatives. The basis for this is, as with all other offers of pastoral care, the patient’s wish. The rituals described range from classical religious forms (e.g., praying together, lighting candles, blessing, singing religious songs, celebrating religious festivals, offering church service, hearing confessions, anointing the sick) (Table 3, C.I.) to a ‘freer’, more unconventional interpretation of religious rituals. “I don’t have to baptize anyone here, I don’t have to hear anyone’s confession, I don’t have to anoint anyone. People can say that themselves if they need it and then we can see what free, religious, spiritual rituals we can find here” (E_SS_H_3, pos. 28). It is crucial that something is individually meaningful to the patient and transcends the organizational setting: “[I]t is ultimately about signs that express something that perhaps transcends our everyday world, let me call it that, alright?” (E_SS_P_2, pos. 106)
This opens up the possibility of still doing something meaningful and comforting in the face of death. One pastoral care worker relates: “[A]lso I just ask if it would do good if I prayed or if it would do good if I lit a candle or something. So that's what I ask. […] So, there are inconsolable situations and of course, I let him talk, if someone talks, but most of the time, a ritual helps” (E_SS_P_3, pos. 38).
Religious rituals are also described as helpful for the relatives of the dying because they offer certainty in a situation which is characterized by uncertainty: “So, relatives more often have the question: How can we bring this to a good end? Who will be there when the transition comes? So, to have someone at this interface between heaven and earth, who should be able to do this A as a role and B: if they, let's say, have met the pastor, i.e., me, they also trust him to do this well. [...] him, who is, so to speak, a bit in no man's land. They say: Right now, I don't know how I could do it properly and well. I would need someone who can manage the situation well now.” (E_SS_H_3, pos. 31)
Pastoral care workers and their rituals allow for a clearer ‘roadmap’ at the “interface between heaven and earth” and can also shape and moderate the transition from life to death for the patient’s loved ones at the deathbed.
Funeral Rituals
Even after patients die, the competencies of pastoral care workers are still needed. Interviewees recounted that they often officiate at the funerals of patients they have visited in hospice or palliative care or perform similar farewell rituals. “[W]hen they then go from this to the other life, the patient himself or also the relatives ask that I also then hold the requiem service and the funeral. So, I am very well known here in the cemeteries, because I am everywhere gladly or often there, because very many patients wish that I also bury them” (Table 3, C.II.). Unlike other palliative care staff, whose responsibilities generally end when patients die or shortly thereafter, the scope of pastoral care workers points beyond the death of patients.
Organizational Commemoration Rituals
This includes farewell rituals within the organizational context. Especially hospice units regularly hold “memorial ceremonies,” “memorial services,” or other commemorative events for those who have died in the organization, which are intended to express a “culture of remembrance” (Table 3, C.III.). These remembrance rituals also appear to be in response to a need among the organization’s staff to “revisit dying on a regular basis” (Table 3, C.III.). For example, the staff of one hospice unit regularly reads out all the names of those who have died: “But that's also important for us, for everyone who works here. To hear and read the name and then say, gosh, look, you remember that one, was -, those were all people who ended their lives here. And everyone has their own story.” (E_SS_H_3, pos. 37)
Discussion
The interviews reveal a wide variety of tasks pastoral care workers fulfill in hospices and palliative care units. However, their work seems to be focused around three major themes, as our results showed: Firstly, they position themselves at a distance to the usual routines of palliative care work. They repeatedly describe themselves as being outside of the organization of the hospice unit. The fact that they do this so frequently underscores that this is an expectable role description. A study from the UK confirms this finding, in which chaplains describe their role as “very peripheral”. 23 Secondly, they engage in conversations with patients and family members, irrespective of their religious affiliation. These conversations can be about anything and aren’t necessarily about death and dying but they may also deal with this subject. Studies from Australia and Northern Ireland also found evidence for the relatively minor relevance of religious affiliation and the high relevance of communication skills such as kindness, listening and being non-judgemental.24,25 And thirdly, they perform various religious rituals, where again, they don’t necessarily talk directly about death, but they may touch upon it. In conclusion, it seems like pastoral care workers, through their self-description of having distance towards the organization, are able to represent a position that gives meaning to what comes after death, to answer unanswerable questions – or in other words: to transcend the immanent. The traditional form for this is typically called religion. And yet, whether someone is religious or not, the question remains: “Do you really believe that there is something more?” It’s not about faith, it’s about the “something more”. Pastoral care workers represent this idea of “no man’s land” by their specific outstanding position in the organization without having to directly mention it.
There is some literature on pastoral care workers that focuses on the standardization of spiritual care provision through guidelines and practice recommendations.15,26,27 In the German context of this study, those guidelines are also provided by organizations like the “Diakonie” or the German Society for Palliative Medicine (DGP). 28 The literature is ambivalent when it comes to the empirical evidence in favor or against standardization. Proponents of standardization argue that the provision of spiritual care needs to be streamlined and standardized in order to establish scientific evidence for outcomes and to be officially recognized, especially by health insurance providers. 10 Our results show that a beneficial factor for the quality of spiritual care from the perspective of pastoral care workers is precisely the non-standardization of their work. This is what allows them to describe themselves as being free from organizational constraints (Table 3, A.III.). Standardization of spiritual care could also be accompanied by bureaucratization. Best et al. report that documentation is “an essential part of the job”. 29 On the contrary, according to our data, documentation is rarely mentioned, which could indicate that it is not considered to be an important part of spiritual care provision. This critique of standardization as well as the minor importance of documentation in our data might be because pastoral care workers and chaplains in Germany are not paid by health insurance providers, but instead are mostly employed by churches, which allow them to work more independently than in American or Australian contexts. Thus, German pastoral care workers might feel very little need to display the outcomes of their work to other stakeholders in the field. This independence could also be an explanation for the fact that we did not find any reports of stress and time constraints in our data, as other studies have. 23
According to Mayr et al., types of rituals serve as interruptions that create moments of reflexivity. They put the organizational flow and the efficiency of its routines on hold and allow the organization to remember and then ‘forget’ the dead. 30 In addition to this, pastoral care workers are able to describe themselves as representants of the liminal space which is the before-mentioned “no man’s land”, especially through the emphasis on the performance of rituals, since they allow them to serve as a symbol of what comes after death without having to talk about it directly.
What This Study Contributes
What this study contributes to literature about pastoral care is an exploration of its position and function in modern society, which struggles to deal with death and dying on the individual level. Thomas Quartier stated that rituals consist of two main aspects: structure and meaning. 3 We find that pastoral care workers engage in both aspects: Through their rituals, pastoral care workers can give meaning to the dying process and death, which transcends the meaning the organization is able to provide, thus creating a kind of ‘re-enchantment of death’. It is the tradition of the profession of pastoral care workers that allows them to function as a representant of this transcendent meaning. Their rituals also create structure in that they can still be performed after the death of a patient, thus providing relatives with continuity in the face of the discontinuity of death. Rituals serve as a kind of ‘roadmap’ that guides relatives through the process of dying, death and bereavement. This is not something specific for German pastoral care workers, since a study from the UK confirms this finding. 23 The function of pastoral care workers for modern society could thus be described in an abstract way as the representation of transcendence, both in meaning and in structure.
Limitations and Future Directions
The scope of this study is limited by its focus on the situation in Germany. A strength of our sample is that it covers data from very different German regions, which is important due to the federal structure of the country. We interviewed pastoral care workers in hospices and palliative care units, but it was not our goal to study the differences in these settings. Concluding from our discussion, future studies should further explore the issue of standardization from the perspective of pastoral care workers. While it might be a necessary requirement for the recognition of spiritual care provision, it could as well turn out to be an inhibiting factor for the quality of care from the perspective of pastoral care workers. A more systematic focus should be placed on the institutional arrangements (organizational structures, finances, standards and guidelines) in which pastoral care work occurs, since they have a significant impact on the provision of care.
Conclusion
In modern hospice care, pastoral care workers routinely address the issue of functioning as a representative of death and in answering the unanswerable question of what comes after death. Our data shows that they profit from the very special organizational role of not being obliged to the organization. This creates an opportunity that in this multi-professional context, a particular position is able to grasp the “something more” that the other professions cannot get a hold of.
Footnotes
Acknowledgments
The authors thank Dipl.-Soz. Katharina Mayr (KM) and Dr. Andreas Walker (AW), who participated in the data collection.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Deutsche Forschungsgemeinschaft; 343373350