
Abstract
Background
Today, many older adults use health technologies, approach their final days with laptops, smartphones, and tablets. Telepalliative care is a service that remotely delivers palliative care through videoconferencing, telephonic communication, or remote symptom monitoring. The service meets the needs of patients who want to die at home and reducing unnecessary hospitalizations. The objective of this study is to map the literature on the use of technology by the terminally ill older adult population being cared for at home, to identify which technology systems are in use, to determine how technology can change communication between palliative care professionals and patients, and to explore the strengths or weaknesses patients perceive regarding the use of technology.
Methods
We conducted a scoping review following the methodology of Arksey and O’Malley. A literature search was conducted in the MEDLINE, Embase, Web of Science, SCOPUS, PsycINFO, CINAHL, Ilisi and Google Scholar databases.
Results
Fourteen eligible papers identified various tools available in clinical practice and found that most older adults are comfortable and satisfied using them. Despite being physically distanced from clinicians, patients felt cared for even though eye contact was lacking. Being unfamiliar with technology emerged as a barrier to telepalliative care in addition to difficulties caused by screen size and internet connection problems.
Conclusions
Older adults in palliative care at home perceive technology as a means of receiving efficient care. However, future research is needed to investigate what they look for in a technological tool and to develop more suitable technologies for them.
Clinical Trial Registration
The protocol of this study has been published in the Open Science Framework (OSF) preregistrations at https://osf.io/acv7q to enhance replicability and transparency and reduce any publication or reporting bias.
Keywords
Background
Based on a United Nations report, the global population of individuals aged 65 years and older is anticipated to double, increasing from .7 billion (9%) in 2019 to 1.5 billion (16%) by 2050. 1 Increased longevity implies that many people are living longer with chronic diseases and various comorbidities that complicate the end of life,2,3 characterized by difficult clinical decisions, complex symptom management, 4 psychosocial problems and spiritual distress. 5 This increases the need for palliative care.6,7 Palliative care provides an interdisciplinary and patient/family-centered approach that addresses the physical, psychological, emotional, and spiritual suffering of terminally ill patients and their families. 8 Palliative care can help older adults manage symptoms in the final stage of life and improve their quality of life by considering their needs and requirements.5,9,10 In the last year of life, older adults experience various symptoms, including pain, anorexia, deflected behavior, mental confusion, constipation, insomnia and incontinence problems. 9 Thus, clinicians need to consider the patient’s totality, physical, psychological and social needs, 5 and very often, they must address several problems simultaneously.11,12
Many older people desire to spend their final days at home,9,13 while maintaining social ties with neighbors and family. 14 Home palliative care teams play a crucial role in enabling this scenario and providing patients with a sense of being accompanied instead of being left alone; these teams help patients cope with advanced life-limiting diseases at home by being available at any time to be contacted or to make a home visit. 15
The COVID-19 pandemic created a rapid surge in demand for remote palliative care services, 7 and the use of technology (video conferencing, email, wireless tools) has become common.16,17 There is growing evidence for the usefulness of telehealth in providing health and allied services for older people in various contexts, including geriatrics and gerontology, rehabilitation and palliative care. 18 Digital technologies are progressively employed to bolster wellbeing, foster the autonomy of older adults, and monitor their health. However, older adults may possess limited experience and familiarity with technology, while their chronic conditions can impede the usability of telehealth. This is further exacerbated by the fact that system designers often overlook this age group as potential users.19,20
Telehealth is defined as the “provision of healthcare remotely by means of a variety of telecommunication tools”21,22
In the palliative context, it is known as telepalliative care, a service that remotely delivers palliative care to patients through videoconferencing, telephonic communication, or remote symptom monitoring.23,24 This mode of care delivery could improve the quality of life of care recipients and the accessibility of care services for those who decide to die at home while reducing unnecessary hospital admissions. 21
Telehealth for palliative care patients at home gives patients an increased sense of safety by providing greater and easier access to healthcare professionals and overcoming geographical distances;24,25 it may empower patients to manage their illness, improve patient quality of life, decrease hospital admissions, and improve access to home palliative care services. 26
The use of technology is often associated with youth, but an increasing number of older people are using the internet and connected health technologies. 27 However, older adults, with their frailty and age-related physical or sensory limitations, may encounter obstacles in using devices and software28-30 due to the size of buttons, brightness, text fonts or language used.31-33
Patients who receive palliative care at home report unmet needs, such as the lack of regular communication with clinicians. 21 This may be because different health care staff visit patients, making it difficult for the patients to form relationships with so many caregivers and leaving them feeling that they are not being listened to enough. 33 Communication is an essential component of home palliative care that facilitates the provision of individualized care, 15 and the use of technology systems has a positive impact.34,35
In this new health care trend, many older people approach their final days with their laptops, smartphones, and tablets by their side, and they are increasingly using their devices to access the internet and connected health technologies. 27 For this reason, research is needed to better frame the benefits of these technologies for individuals at the end of life. Given the heterogeneity of the literature, it was decided to choose a scoping review as the study design; In contrast to other reviews, scoping reviews serve the purpose of delineating the fundamental concepts that form the basis of a research field. 36
The objective of this review is to map the literature with respect to the use of technology in the home by the terminally ill older population. In particular, we aim to identify the types of technology systems in use in the world, how technology can change communication between palliative care professionals and patients, and what is known about the strengths or weaknesses regarding the use of technology by patients in palliative care at home.
Methods
To address the aims of this study, we conducted a scoping review, following the 5 stages of the methodology outlined by Arksey and O’Malley 36 and the recommendations of Levac et al. 37 The 5 stages are as follows: 1. Identifying the research question, 2. Identifying relevant studies, 3. Study selection, 4. Charting the data, 5. Collating, summarizing and reporting the results. 34 The Preferred Reporting Items of Systematic reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) checklist guided the reporting of our review. 38
Stage 1: Identifying the Research Question
Objective
The present study is a scoping review on the use of technology at home by the terminally ill older population. The purpose is to identify what types of technology systems are in use, how technology can change communication between palliative care professionals and older adult patients, and what is known about the strengths or weaknesses regarding the use of technology by older adults in palliative care at home. This scoping review will systematically map the relevant research.
The objective is guided by the following research questions: 1. Which technological systems are the most widely used by older people in palliative care at home? 2. How does the use of technology affect and change communication between older adults in palliative care at home and care professionals? 3. What strengths or weaknesses do older patients perceive in using technology for receiving palliative care at home?
Stage 2: Identifying Relevant Studies
Eligibility Criteria
Studies included in the research are relevant to meet the research objectives. All primary studies (qualitative and/or quantitative) were eligible, with no language or date restrictions; an external translator will be involved if necessary. Published studies and gray literature studies were included, excluding dissertations and theses. The target population was patients receiving palliative and/or end-of-life care at home and using technology. We excluded studies reporting the use of only telephones for calling and the use of e-mail for communication but included studies in which technologies also support non-verbal communication in addition to verbal communication between patients and clinicians. Studies were selected if they included adults over age 65. We excluded all review papers and studies with unavailable abstracts and full-texts.
Stage 3: Study Selection
Information Sources
A professional health science librarian (F.R.) in collaboration with the research team prepared the search strategy in the MEDLINE (through Ovid), Embase, Web of Science, SCOPUS, PsycINFO, CINAHL and Ilisi databases. In addition, the grey literature was searched in Google Scholar, grey literature databases, and relevant charity and organization websites.
Search Strategy
The final search results were exported into Mendeley Reference Manager 39 and screened for duplicates. After deleting duplicates, the remaining articles were entered into the Rayyan reviewing system online. 40 All abstracts were screened independently by 2 reviewers (IB and LC). If there was disagreement between the 2 reviewers, a third, more senior reviewer assessed the abstract to determine eligibility for inclusion (ML). All stages of full-text review and data abstraction were performed independently by the 3 reviewers (IB, LC, and DR). Studies that did not meet the inclusion criteria were excluded for documented reasons. Any disagreement between the reviewers was discussed among all team members who determined the eligibility. The search decision process was described using the PRISMA flow diagram. 38 The search strategy is available in the Supplementary Materials. Cohen’s Kappa statistic was used to measure the interrater reliability of the study selection. 41
Stage 4: Charting the Data
We extracted general characteristics of the included studies, such as year of publication, study location, study population, aims of the study, methodology (quantitative vs qualitative), types of technology used (ie, software/hardware), outcome measures (process of care, assessment of patient needs, goal setting, care plans, outcome monitoring, intervention reporting frequency, communication effectiveness, and patient perspectives on positive or negative aspects of technology) and notes on usability or satisfaction.
Stage 5: Collating, Summarizing and Reporting the Results
We collected all the evidence from the included studies by reading them with reference to the 3 research questions and wrote a narrative summary of the studies about the topic. The studies were analyzed in terms of their general characteristics and with special attention to the electronic device and software used by the older adult subjects. Frequencies and percentages were utilized to describe nominal data. The results are presented and categorized into 3 main sections: (1) types of software and devices used by older adults in palliative care at home; (2) the effect of technology use on communication between professionals and patients; and (3) strengths or weaknesses perceived by older adults in the use of technology.
Results
We found 8169 articles, exported them into Mendeley
39
and screened for duplicates. A total of 2936 duplicates were removed, leaving 5233 records. One hundred three articles were found to be eligible. Articles were excluded if they considered the wrong population (eg, caregivers/clinicians; individuals who were not in palliative or terminal care, were not older adults, were hospitalized/ambulatory patients), were the wrong publication type (eg, a dissertation), or used the wrong tools (eg, telephone/e-mail). Studies reporting on both older adult and adult or pediatric populations were included only if relevant measures used for the older adults were reported separately. The 3 independent reviewers resolved any disagreements about study inclusion through discussion; if consensus could not be reached, the senior member was engaged. K was .69 with good agreement. Fourteen studies were included: 8 were quantitative (1 was a protocol), 2 were qualitative, and 4 had a mixed-method design. The search and decision-making process is described using the PRISMA flow diagram
38
in Figure 1. PRISMA flow diagram, 2020.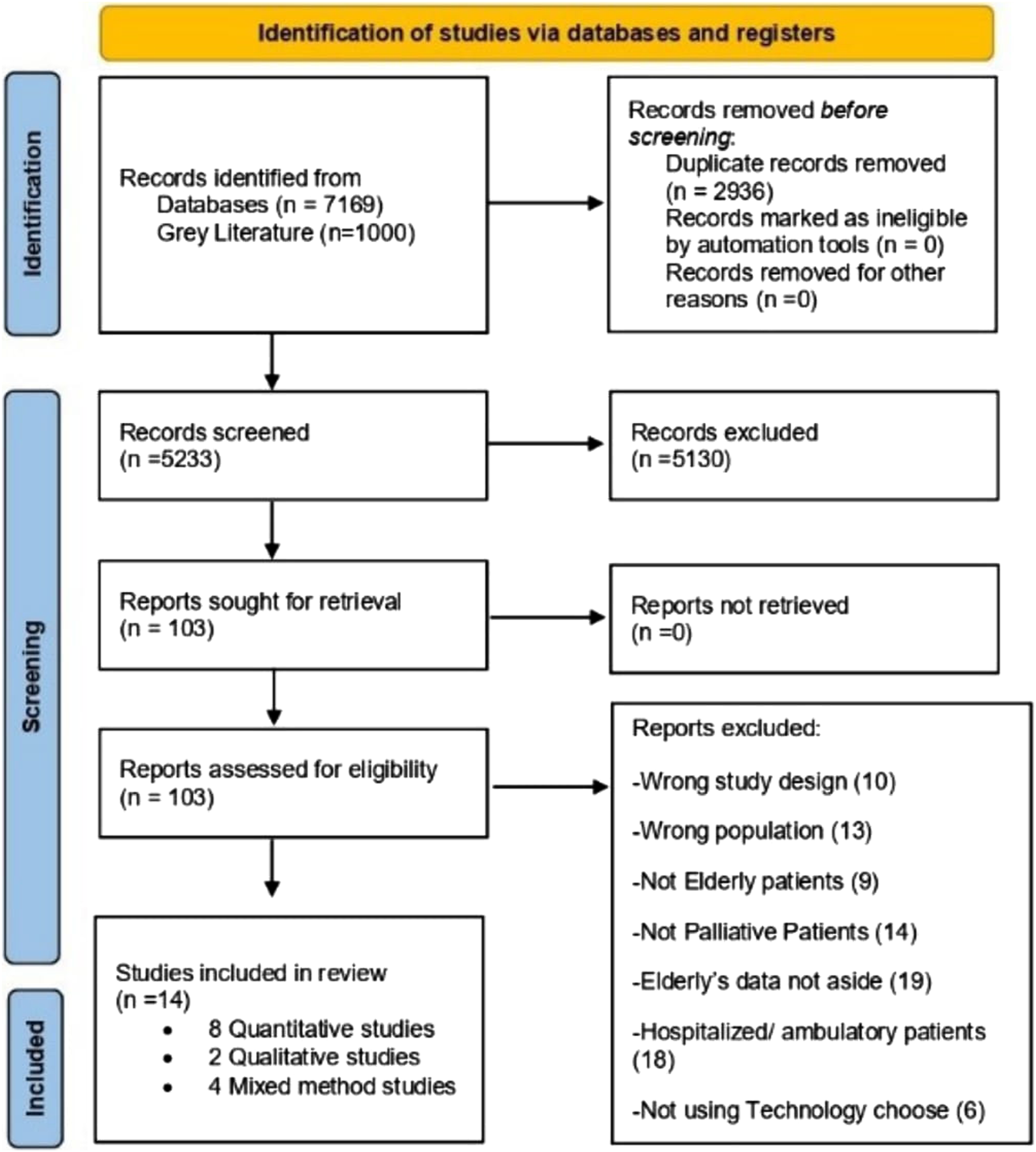
Study Characteristics
General Characteristics of the Included Studies.
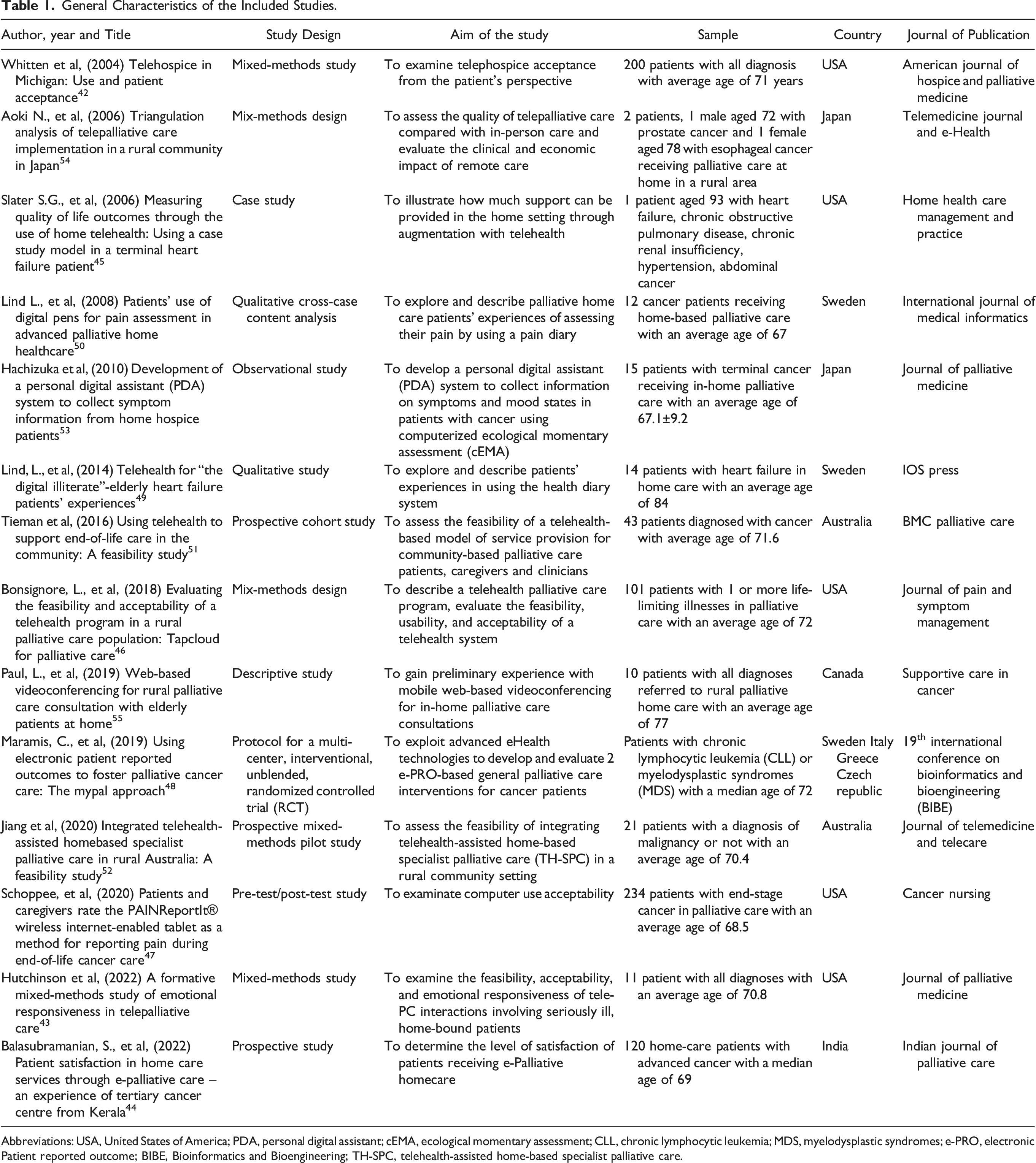
Abbreviations: USA, United States of America; PDA, personal digital assistant; cEMA, ecological momentary assessment; CLL, chronic lymphocytic leukemia; MDS, myelodysplastic syndromes; e-PRO, electronic Patient reported outcome; BIBE, Bioinformatics and Bioengineering; TH-SPC, telehealth-assisted home-based specialist palliative care.
Technology Systems Used by Older Adults in Palliative Care at Home
In the included studies, the most frequent devices used by patients were tablets (21%)43,47,51 and smartphones (21%).42,48,53 2 studies reported the use of computers (14%)44,55 and in 2 studies, the software was usable on any device (14%).46,52 Lind and Karlsson 49 and Lind et al., 50 in their 2 studies, used a pen with an embedded camera on a paper sheet; the other 2 studies used a device for videoconferencing (14%),45,54 1 of which recorded vital signs. The technology offered in the protocol study of Maramis et al 48 was composed of a smartphone and a wristband employed for measuring the physical activity and sleep quality of patients.
Regarding the frequency of use, in 6 studies, patients used the technology every day,47,49-51,53,54 in 1 study monthly, 42 in 5 studies periodically,44,46,48,52,55 and in 2 studies, the frequency of use was not indicated.43,45 Additionally, in 3 studies, the technology was used in case of need.42,51,52
Characteristics of Software and Devices.
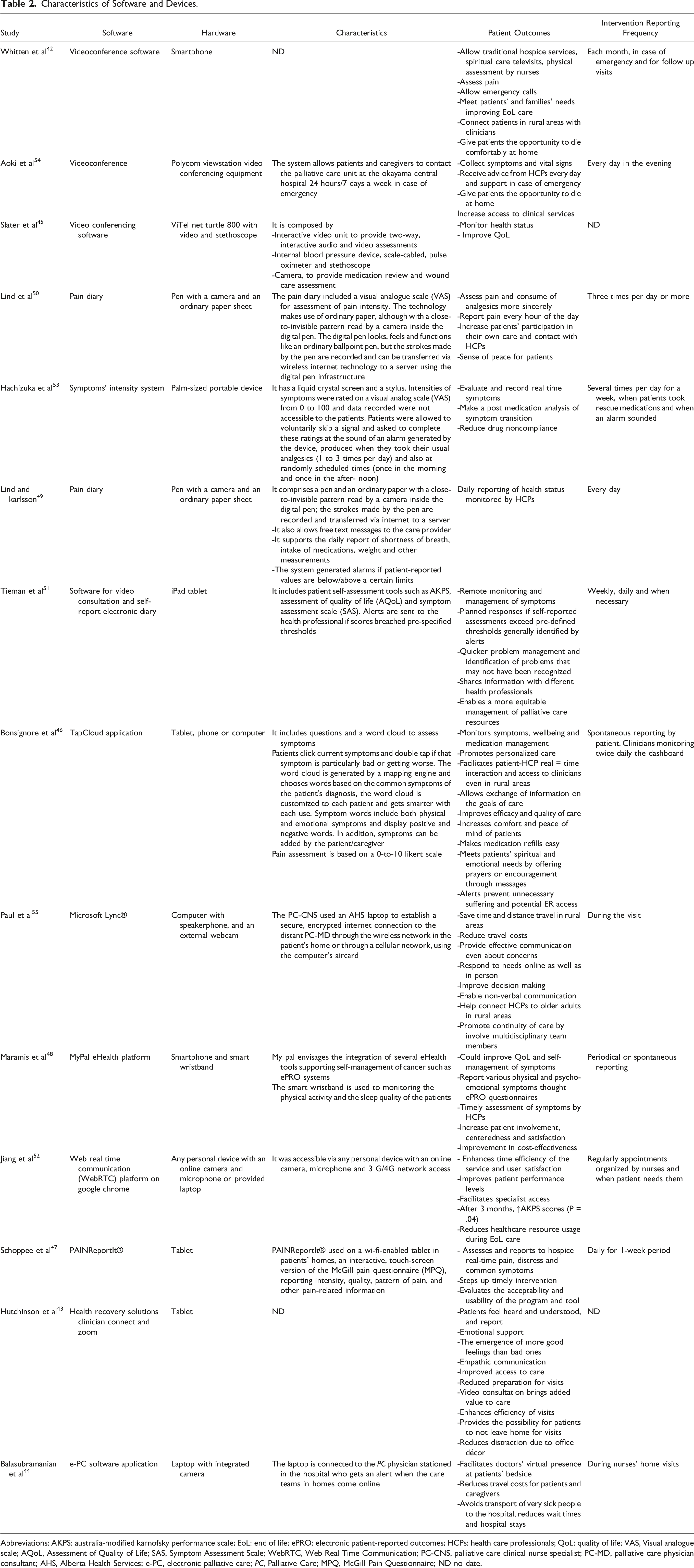
Abbreviations: AKPS: australia-modified karnofsky performance scale; EoL: end of life; ePRO: electronic patient-reported outcomes; HCPs: health care professionals; QoL: quality of life; VAS, Visual analogue scale; AQoL, Assessment of Quality of Life; SAS, Symptom Assessment Scale; WebRTC, Web Real Time Communication; PC-CNS, palliative care clinical nurse specialist; PC-MD, palliative care physician consultant; AHS, Alberta Health Services; e-PC, electronic palliative care; PC, Palliative Care; MPQ, McGill Pain Questionnaire; ND no date.
In 9 studies, patients used different devices and software to hold videoconferences with their clinicians; 5 of these studies used devices that only conducted videoconferences.42-44,52,55 In 2 studies, the hardware also supported peripherals for collecting vital signs, such as blood pressure devices, pulse oximeters, and stethoscopes.45,54 In the study by Tieman et al., 51 the video consultation was associated with a self-report electronic diary made up of the Assessment of Quality of Life (AQoL) questionnaire and Symptom Assessment Scale (SAS). If self-reported assessment scores breached prespecified thresholds, the software sent alerts to the health professional or programmed responses to the patient. 51
In the study of Bonsignore et al., 46 the TapCloud application included a dynamic screen view of words used to describe both physical and emotional symptoms the patient might be experiencing (word cloud). Patients tapped current symptoms and double-clicked to indicate if that symptom was particularly bad or worsening. 46
Hachizuka et al., 53 Schoppee, et al., 47 Lind and Karlsson, 49 Lind et al., 50 and Maramis et al. 48 promoted the self-report of symptoms directly by patients through different devices and software.
Hachizuka et al 53 described an electronic diary in which participants indicated the intensity of their symptoms on a visual analog scale (VAS) with their fingers or a stylus on the screen of a tablet.
Schoppee et al. 47 used the PAINReportIt® on Wi-Fi-enabled tablets to report pain in real time to health care providers, indicating pain location, intensity, quality, pattern, and other pain-related information measured by the McGill Pain Questionnaire (MPQ). Wi-Fi allowed patients to use the anywhere in their homes and not be limited in their movement by the length of an internet cable. 47
Lind et al 50 in 2 studies reported the use of a digital pen, apparently a normal ball-point pen but with a built-in camera that could record and transfer to a server whatever a patient wrote in an ordinary paper diary, with a printed close-to-invisible pattern read by the camera. The diary made it possible to report pain and other symptoms, such as shortness of breath, intake of medications, weight and other measurements.49,50
Maramis et al. 48 presented a new idea for an eHealth tool for the reporting of physical and emotional symptoms using patient-reported outcome (PRO) self-report questionnaires on a smartphone application. Patients in this study also wore a smart wristband to record lifestyle parameters such as physical activity and sleep quality. 48
Technology Impact on Communication Between Older Adults and Care Staff in Palliative Home Care
Twelve studies in this review considered the aspect of communication in the use of technology by older adults in palliative care at home, of which 4 focused only on the older adult population.42-50,52,54,55
Barriers and Facilitators in the use of Technology for Communication Between Patients and Clinicians.
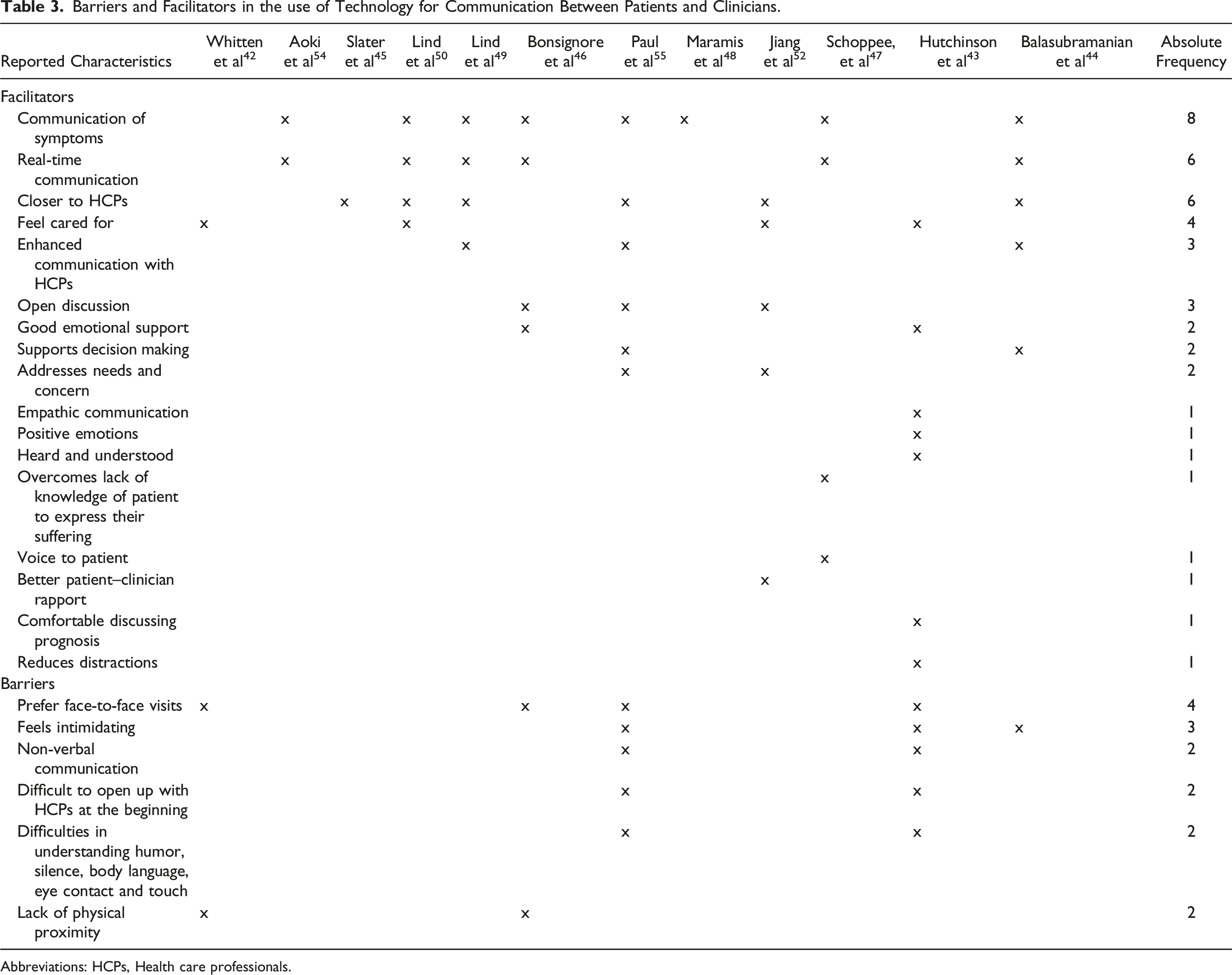
Abbreviations: HCPs, Health care professionals.
Three studies claim that the use of technological tools in home palliative care has a positive impact on communication between clinicians and patients,44,49,55 promoting a stronger connection between the 2 parties than in-person visits.45,49,50,52,55 In the studies of Paul et al 55 and Jiang et al., 52 patients using video conferencing compared to other visit formats, said they could communicate effectively and felt comfortable discussing their concerns.
In studies that used self-reported symptom tools, patients had better communication of symptoms to their clinicians.44,46-50,54,55 Schoppee et al. 47 reported that the software used for self-reporting pain was a clear and concise tool that was easy to understand and offered a method of communicating directly and quickly; they found that the software helped older people who often lacked the language or knowledge to adequately communicate the suffering they were experiencing.
The reporting of symptoms recorded by and available in electronic systems, the opportunity to consult at any time and the advantage of being able to connect multiple professionals to the patient simultaneously improve the decision-making process regarding patient care, as shown by the studies of Paul et al. 55 and Balasubraimanian et al. 44
The screens on devices allow little more than the patient’s face to be seen, which cuts out gestures and body movements that could sometimes be signals for clinicians to continue the conversation or to calibrate communication patterns and words, for example when dealing with thorny issues such as death. Therefore, verbal communication often fails as a key element of dialog; tone of voice can be an aspect that makes people feel empathy and helpfulness, as underscored in the study of Hutchinson et al. 43 The use of humor, silence, interpretation of body language, eye contact and touch remain challenges for digital communication. For example, the use of silence might be misinterpreted by patients as a technological problem. 43
Despite the physical distance between patients and caregivers, patients said they felt cared for, assisted in a positive way,42,43,50,52 and were much more comfortable and relaxed when having a consultation or discussion with clinical staff at home; 43 they cited the lack of distraction due to office décor, which made focusing on conversation simple. 43 However, the presence of multiple team participants in real time was slightly intimidating for some patients. 55
Although physical proximity and eye contact were lacking, some individuals preferred using technology to maintain the relationship with clinicians rather than to initiate it, 55 and some preferred in-person visits over virtual visits.43,46,55
Strengths and Weaknesses Perceived by Older Patients in Using Technology at Home
Strengths and Weaknesses in the use of Technology Among Older Adults in Palliative Care at Home.
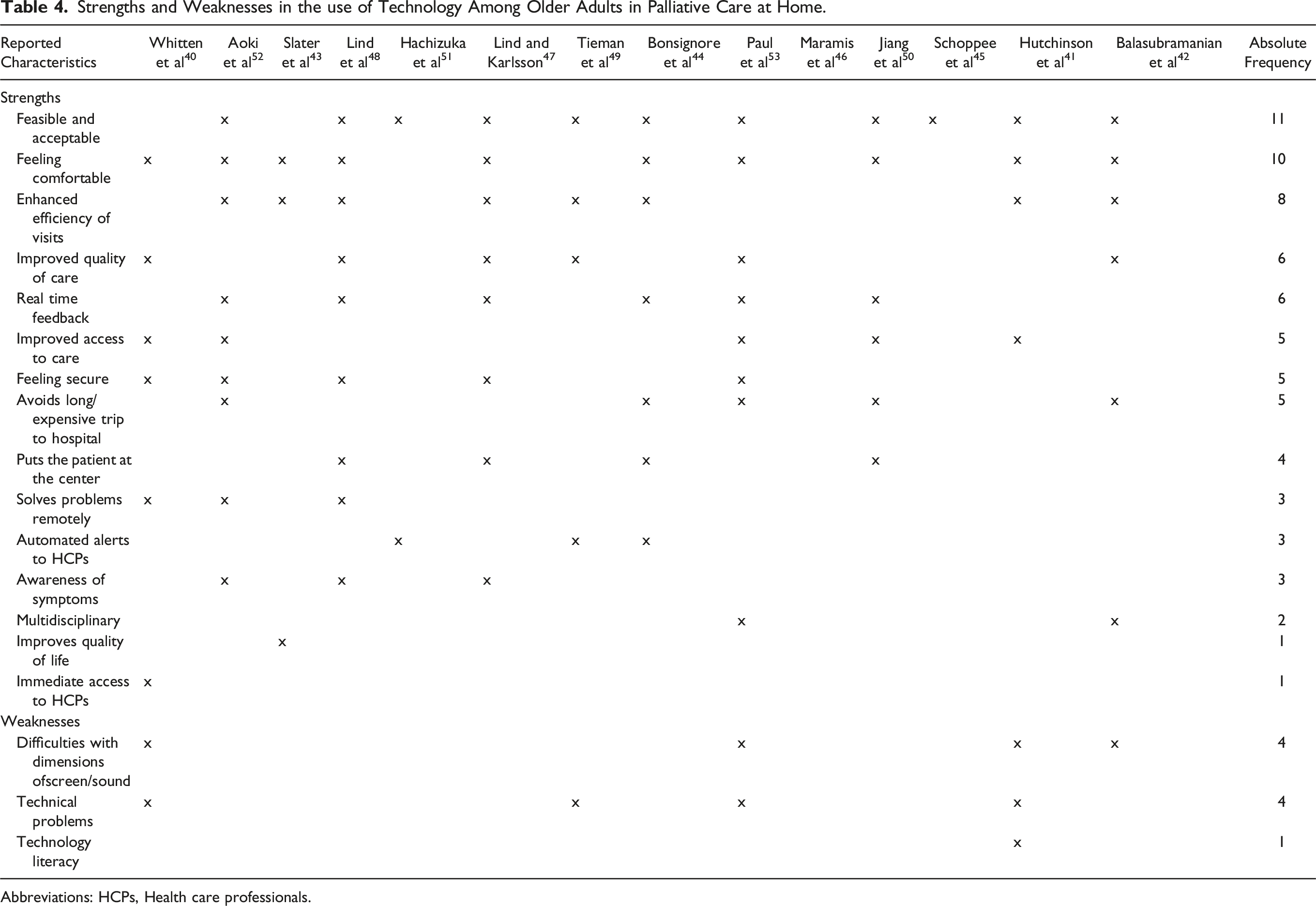
Abbreviations: HCPs, Health care professionals.
Barriers and facilitators in the use of technology perceived by older adults in palliative care at home.
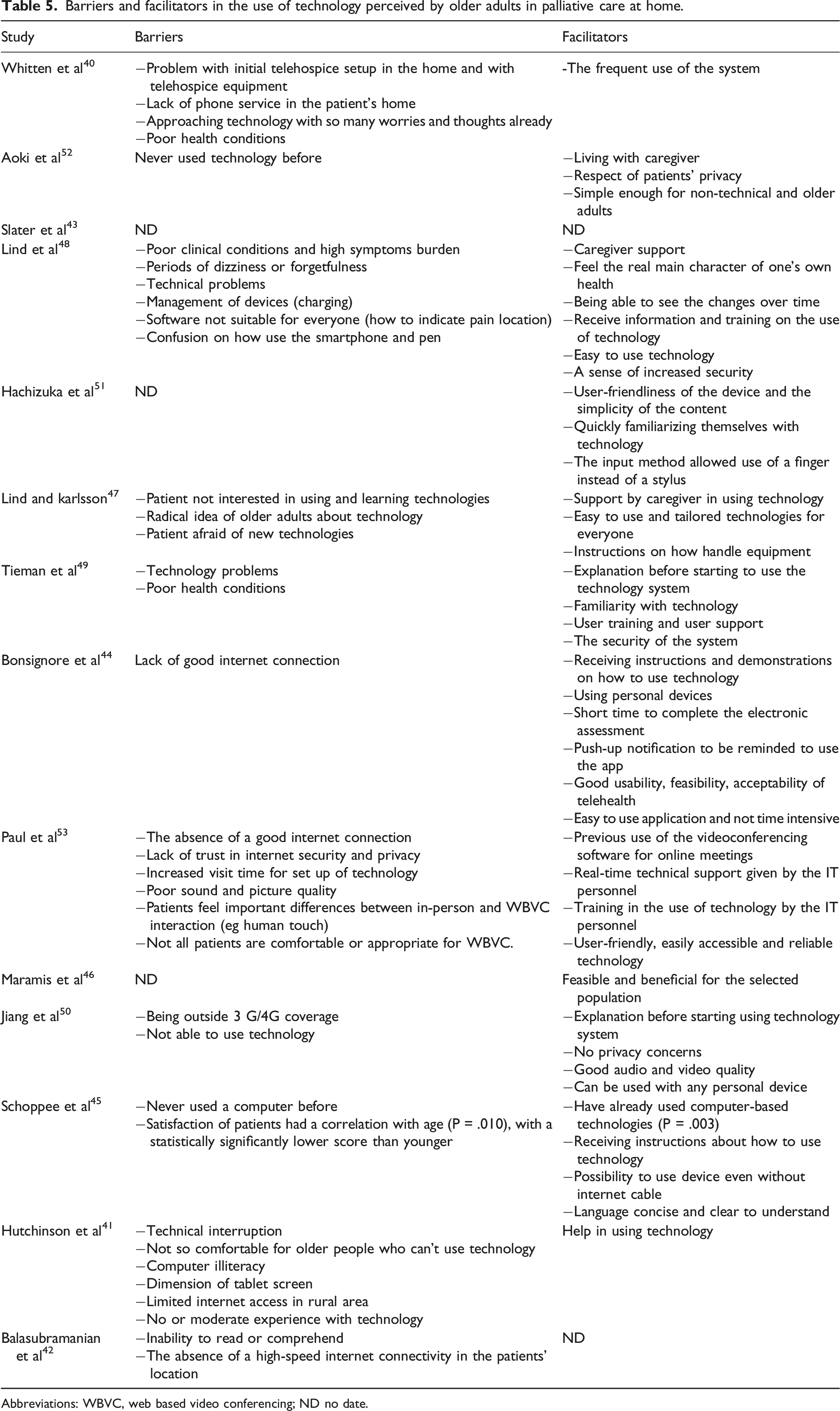
Abbreviations: WBVC, web based video conferencing; ND no date.
Most of the technologies described in the studies of this review were judged to be user-friendly by older adults patients with terminal illness receiving at-home hospice care.42,43,50,53 They reported that the technology was convenient and comfortable in their situations, 52 considering their variable and often poor state of health. 50
The older adults quickly became familiarized with the technology49,53,54 when they had previous experience with computers or other devices,47,51,55 caregivers’ support43,49 and explanations and training before using them.46,47,50-52,55 Computer illiteracy,43,47 radical negative ideas about technology, 49 and technical problems42,43,50,51 were perceived by older adults as barriers to the use of technology.
Remote visits for patients who live far from metropolitan centers, have great importance in reducing the need for travel to face-to-face meetings and improving access to care, as shown in the studies of Whitten et al., 42 Huchinson et al., 43 Aoki et al., 54 Paul et al., 55 and Jiang et al. 52 This type of care makes it possible for patients and caregivers to avoid long and expensive trips to hospitals, and patients prefer their own homes to the hospital environment to continue to carry out normal activities of daily living.54,55
Even with some difficulties in the use of technology due to their age and lack of experience in the use of technology, 52 the older adults quickly familiarized themselves with it.42,50,53 Problems with the equipment were reported, but were not enough to interrupt its use.
The input with a finger facilitated the use of the device in the study by Hachizuka et al, eliminating the need for a stylus to tap answers on the screen. 53
Another system used is the digital pen described by Lind and Karlsson. In 2 studies in which subjects found it very easy to handle and overcame their reticence about using the internet. In another study by Lind et al, 50 there were no particular moments that prevented the use of the pen, but patients had some difficulty with the VAS scale for the reporting of pain in the diary.
One of the problems that older adults have found is the dimension of the device screen, which they perceived as a barrier to the use of the device.42-44,55
The use of the internet is necessary for almost all devices described, so this may represent a problem for people who live in rural areas with less reliable network coverage.43,44,46,52,55
Negative emotions decreased while positive emotions increased following the consultations because patients perceived that they were being totally heard and understood and that they were receiving appropriate emotional support through the technological approach to their care. 44
Some tools, such as those of Timenan et al., 51 Bonsignore et al., 46 and Lind and Karlsson, 49 generated automated alerts when data entered by the patient breached predetermined thresholds; these alerts about emerging patient health issues were sent to health care providers, who could act immediately, preventing unnecessary suffering and potential emergency room visits or hospitalizations.46,49
During the end of life stage, compared to in-person visits, remote visits reduced healthcare resource usage (.13 per capita vs 3.88, effect size: 1.34) and hospital admissions (.02 per capita vs .2, effect size = .65); furthermore, performance status AKPS was better preserved (58.24 vs 43.88, effect size = 1.11), and patients experienced reduced symptom burden and distress, as reported in the study by Jian et al. 52
Another aspect of remote care considered was privacy, which was not perceived as a concern52,54 except in a study by Paul et al., 55 in which older adult individuals expressed skepticism about the identity of distant clinicians.
Discussion
This study spans a wide range of publication years showing an evolution in the technologies used but finding that all had a positive impact on care, even in years when the technology was new, and especially new to the older adult population. We continue to assume that the older adult population is not capable of utilizing technology and that it is a hindrance to them. This review points out how the trend is changing; even older adults feel comfortable with the use of technological tools that are often far from their aptitudes. This is not a point in life when a person easily learns how to use new technologies, but nevertheless, in almost all studies, older people showed great openness to this new approach to care.
From the simplest video calls to remote symptom monitoring systems without the need for calls, technology is able to connect clinicians and patients in even the most remote rural areas. This makes available a health service far from people’s homes, ensuring homogeneous and equitable access to care. In telepalliative care, the technology offers individuals the opportunity to spend the last days of their lives, even the most critical and difficult moments, at home in familiar surroundings with family and friends but still protected by direct and constant contact with clinicians. The preference for eye contact with their clinicians, concerns about privacy, and doubts about who is on the other side of the screen are aspects that could cause patients to lose confidence in health care professionals but, more importantly, these aspects of remote care may leave out a fundamental part of palliative care, which is the aspect of humanization.
In addition, the continuous monitoring of health status and symptoms of patients at home prevents unnecessary prolonged suffering over time and potential emergency room visits or hospitalizations.46,49
The involvement of patients in reporting their symptoms empowers them and increases their participation in their care. They become more aware of the progress of their illness with the highest honesty from their care providers; furthermore, there is a dual intention of these tools, which is not only to highlight a worsening of symptoms so they can be treated but also to provide the patient with the possibility of immediate responses to alleviate pain or other problems. 50
Patients look for simple systems that are suitable for them, for their frailty and progressive deterioration and make their lives easier and more protected; in addition, there is certainly a need for them to receive information about how devices and software work and what value they add to their lives. 50 The training and the instructions are fundamental as well as the support of their caregivers to better use technology at home and to guide them into a new and unexplored world. This review has several limitations. As a scoping review, our objective was to provide a comprehensive description of all available information, which led us to include studies without conducting a formal quality assessment. Furthermore, of the included studies, only 4 exclusively considered the elderly population. The studies that considered different age groups instead may not have been sensitive enough to capture the exclusive specificity of elderly individuals.
Conclusion
This study highlights how older adult are using technological tools to communicate with the world around them. Even in a situation of frailty and complexity such as the end of life, technology can support older adults patients in palliative care at home. These patients perceive these tools as a means to efficient health care by clinicians. Future research should address the development of more appropriate tools for older adults and terminally ill population, considering that over time, the digitized population may grow and change. Details about what older adults look for in a technological tool and their expectations about how those tools can be integrated with care delivery should also be topics for future research.
Supplemental Material
Supplemental Material - Technology to Support Older Adults in Home Palliative Care: A Scoping Review
Supplemental Material for Technology to Support Older Adults in Home Palliative Care: A Scoping Review by Ilaria Basile, Letteria Consolo, Stella Colombo, Daniele Rusconi, Flavia Rampichini, and Maura Lusignani in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.