
Abstract
Clinicians need palliative care (PC) skills to provide good patient care. Primary PC (PPC) is the PC knowledge and skills provided by non-PC specialists and are distinct from specialist PC (SPC), the complex interventions provided by specialty trained clinicians. There is no consensus as to the specific PPC knowledge and skills that should be taught or the methods that should be used. We describe an educational system that incorporates a suite of tools that PC educators can easily adapt to the PC educational requests of training programs to evaluate the PPC educational needs of training programs and then to create customized educational programs that regularly adjusts to the input of trainees and faculty. We hope others can use this program to decrease the burden on the PC educators and provide a tailored PPC education program for training programs within their institutions.
Keywords
Introduction
All clinicians need basic palliative care (PC) skills to provide good patient care. Primary PC (PPC) is the PC knowledge and skills provided by non-PC specialists and are distinct from specialist PC (SPC), 1 which is provided by specialty trained clinicians. Often, PC clinicians are asked to teach PPC to learners at different stages of training and across different specialties. Despite the widespread consensus that some PC knowledge and skills are important for all clinicians, there is no consensus as to the specific PPC knowledge and skills that should be taught or the methods that should be used. The goals of the Palliative Care Education Curriculum (PCEC) are 3-fold – (1) to design a suite of tools that PC educators can quickly and easily adapt to the specific PC educational requests of any training program, (2) to evaluate the PPC educational needs of individual training programs and create customized PCEC programs that regularly adjust to the input of the trainees and faculty, and (3) to create and foster a community of educators interested in improving PPC education within their specialty.
Methods
We identified interested GME programs within a large academic center and used surveys of trainees, primary faculty, and PC faculty to create learning plans individualized for each program. The PCEC program administration consists of the PCEC director (a PC clinician with over 10 years of experience in PC education) and PCEC administrator (a manager who coordinates with participating programs and administers the website). The PCEC liaison of a given program (usually the program director or chief resident) works with the PCEC director to analyze data, decide on survey structure and participants, and create an educational plan for the academic cycle. PC educators are PC clinicians who indicated an interest in teaching PPC topics and volunteered to participate in the PCEC program. IRB approval was obtained.
PCEC Toolbox
Adaptable Didactics
We chose 10 PPC Topics based on the didactics that our PC educators are most frequently asked to give and input from the PCEC pilot programs (see below). The PCEC director coordinated with PC educators on which topics they were interested in teaching. When a program requested one of the 10 PPC topics, we arranged a teaching session with the designated PC educator and the requesting program. The PC educators were thus able to create standard didactics that could be adjusted for the training programs without having to create new presentations for each educational session, thereby becoming more expert at teaching specific PPC topics. If that educator was unavailable, another educator could borrow their presentation, thus decreasing the amount of time recreating educational materials.
Initial Surveys
Needs assessment surveys were created to help guide PPC teaching for the upcoming 6-months using data from the trainees in the program, the primary faculty of the program, and the PC faculty.
Primary Palliative Care Survey Topics.
We collected participant demographics and previous PPC experience. For each of the 10 PC topics, the participants were first asked if the topic was important to their training. If they answered “no,” they were asked about the next topic. If they answered “yes,” they were asked if trainees in their program needed more training on this topic (Figure 1). For example, Internal Medicine residents were asked “Should Internal Medicine trainees know how to lead a family meeting?” If the respondent answered “no,” they would move to the next topic; if the respondent answered yes, the next question would be “Do trainees in your program need more training in leading a family meeting?” Both the Internal Medicine faculty and the PC faculty would answer the same questions regarding the Internal Medicine residents. Creation and analysis of the 3 surveys took approximately 1 hour for each participating program. By limiting the surveys to 10 topics and constraining the questions for each topic, we created a survey that gave a wealth of data and took the average participant between 5-10 min to complete. Initial Survey Question Structure.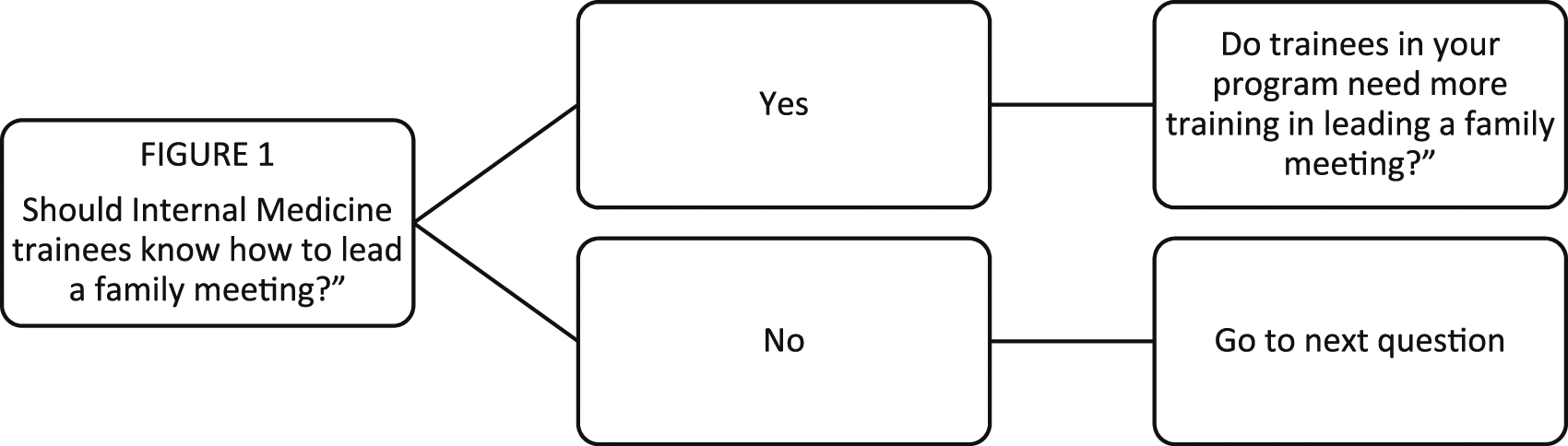
The survey was sent to trainees, primary faculty, and PC faculty through Redcap. Each program chose which trainees would receive the survey and when the survey would be sent, based on the individual characteristics of their program. For example, 1 year fellowship programs may choose to send surveys during the penultimate month of the academic year if they knew historically that the last month of the year trainees may be preoccupied with transitioning to a new position. Each program also chose which primary faculty would receive the survey based on the likelihood that they would be able to assess the knowledge and skills referenced. Prior to surveys being sent out, the leadership of the training program sent a message to the department to explain the project and encourage them to fill out the survey. All PC faculty including physicians, nurse practitioners, and physician assistants were sent the survey for each training program.
Key for Initial Survey.

Example Initial Survey.
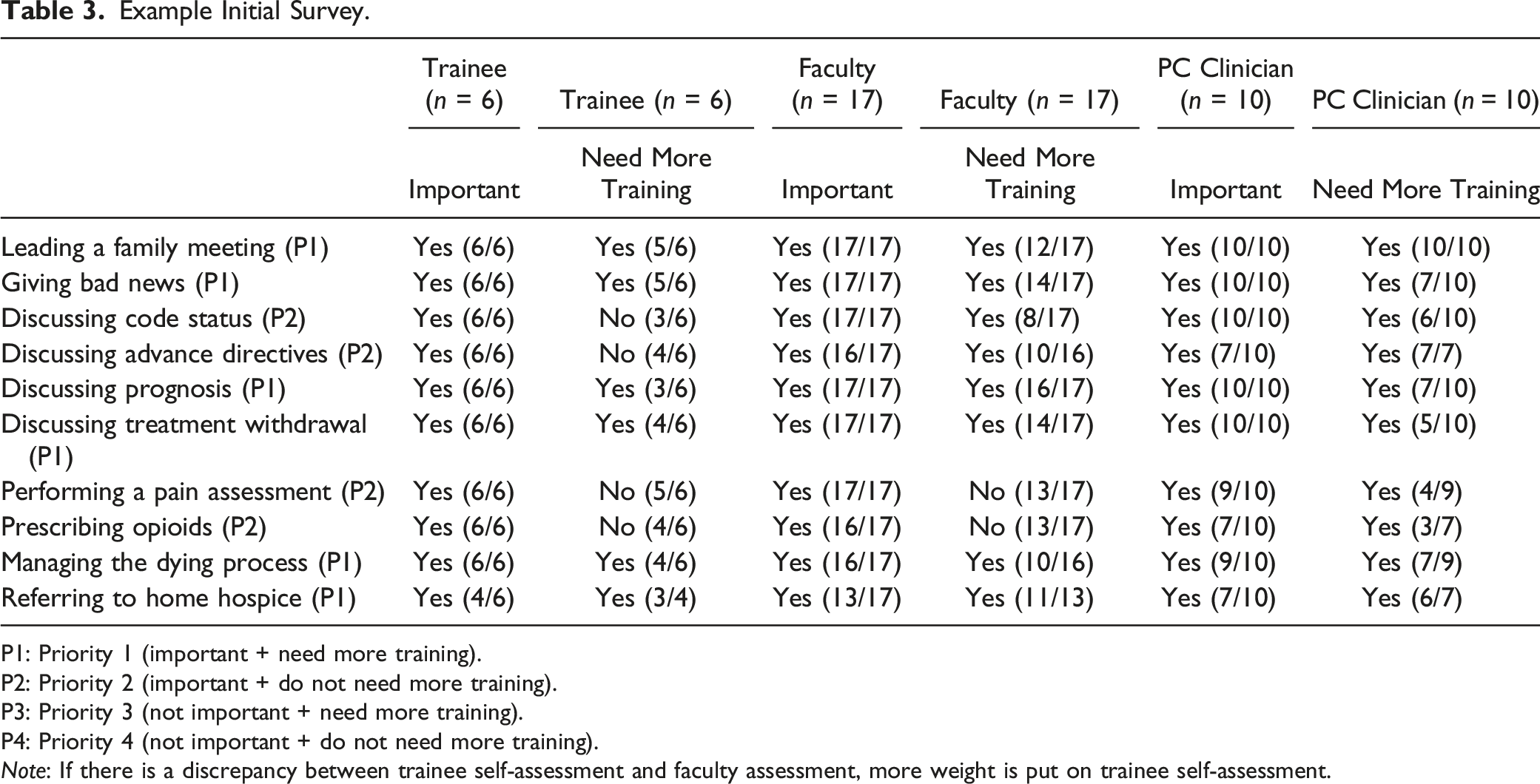
P1: Priority 1 (important + need more training).
P2: Priority 2 (important + do not need more training).
P3: Priority 3 (not important + need more training).
P4: Priority 4 (not important + do not need more training).
Note: If there is a discrepancy between trainee self-assessment and faculty assessment, more weight is put on trainee self-assessment.
After analysis of the initial surveys by the PCEC director and creation of the initial report for the program, the PCEC director and the PCEC Liaison meet for approximately 15-30 minutes to discuss the results and plan for the upcoming academic semester. This meeting allows for input from both the PCEC director regarding recommendations on how to teach the chosen topics (for example opioids taught as didactics in small groups but communication skills taught by role play) as well as the details from the PCEC Liaison about specific needs of the program, allowing for a tailored approach to PPC education for participating programs. Most programs chose to schedule hour-long educational sessions 1 to 4 times per semester and used the assigned priorities to choose the topics for the upcoming semester. The PCEC director would then email the PC educators who had indicated an interest in teaching the requested topics. The PCEC administrator provided a feedback slide to the PC educator to get real time feedback after educational activities, which then could be shared with the PCEC liaison, allowing for continuous assessment of educational interventions. If educational activities were recorded, they were uploaded with permission to an internal PCEC website to create a library of educational videos and resources. The PC educator could also use this feedback as part of their educator portfolio for academic advancement.
Repeat Surveys
Programs completed initial surveys once, during the first enrollment period, then repeat surveys every 6 months thereafter. For multi-year programs, each program decided whether to send the repeat survey to new trainees (usually interns).
Key Repeat Survey.

Example Repeat Survey.
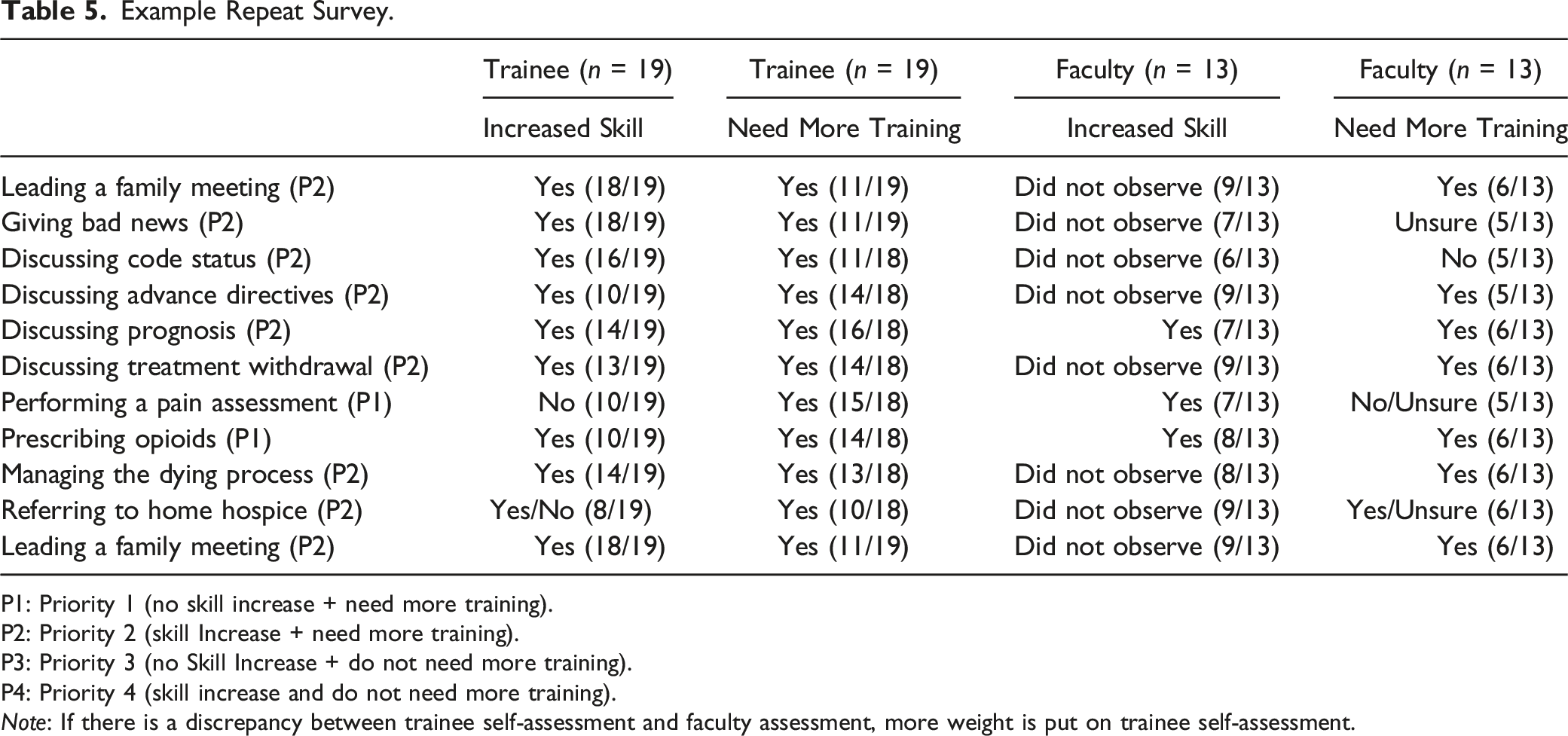
P1: Priority 1 (no skill increase + need more training).
P2: Priority 2 (skill Increase + need more training).
P3: Priority 3 (no Skill Increase + do not need more training).
P4: Priority 4 (skill increase and do not need more training).
Note: If there is a discrepancy between trainee self-assessment and faculty assessment, more weight is put on trainee self-assessment.
Monthly Resources
Each month, the PCEC director sends a PPC resource such as a paper, podcast, Website, or app to the PCEC liaisons who could then pass these resources on to their programs. These emails introduce learners to a variety of PPC topics in different modalities to maintain engagement with the program and to highlight the PCEC website.
PCEC Website
We created a password-protected, institutional website that included a list of participating programs, contact information for the PCEC liaisons, a repository of resources, and the monthly resources sent to the participating programs. We uploaded recorded didactics and plan to have a calendar with online meeting links available so that PCEC community members can see what other programs are learning.
Individualized Educational Programs
Because of the robust and nimble educational infrastructure, each participating program can create an individualized PPC program for their learners that is adjusted twice per academic year based on input form the learners and the faculty, thereby tailoring the PPC education of the current trainees and increasing their investment in their PC education. We have created tools including surveys and didactics which are easily adapted to training programs, therefore decreasing the burden on the PC educators and providing a tailored PPC education program for each program.
Community of Educators
Part of the goal of the PCEC program is to create a community of educators who are interested in identifying and improving the PPC skills and knowledge appropriate for their primary specialty. The PCEC community meets once per year to discuss best practices and to share what is working and what we can improve upon. We work together to write abstracts and papers to share with the wider PC education community both within PC and within the individual specialties. As more opportunities for scholarship and educational training arise, these will be the group of educators that will help shape PPC education for their programs and within their specialties and can be identified within the institution, and beyond, as leaders for PPC education.
Discussion
Over the past 2 years, we have enrolled 9 training programs (Internal Medicine, Med-Peds, Urology, Critical Care, Physical Medicine and Rehab, Geriatrics, Advanced Heart Failure, Radiation Oncology, and Emergency Medicine) within a large academic medical center, approximately 2 programs every 6 months. The PCEC director presents to residency and fellowship directors at GME meetings and calls for enrollment are sent through the GME office and through word of mouth. We hope that the details of the PCEC program provide a model for PC educators interested in streamlining and supporting their colleagues both within PC and within training programs to improve the PPC of trainees outside of the SPC field.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.