
Abstract
Background
Palliative care (PC) focuses on the prevention and relief of suffering through the treatment of physical, psychosocial, and spiritual issues associated with serious illness. 1 Despite the increased utilization of PC services in recent years, members of racial or ethnic minority groups utilize them less frequently than non-Hispanic White patients, and patients from minority groups have been shown to have lower rates of hospice utilization and higher symptom burden.2-5 Multiple factors may contribute to this disparity, including mistrust of the healthcare system, lack of understanding about illness severity, and language and other cultural barriers.6-9
Though recent studies are limited, the positive impact of racial, ethnic, cultural and language concordance between patients and clinicians has been demonstrated in general medical populations.10-15 Concordance in these domains may be particularly important in PC given the focus on serious illness conversations and end-of-life care, which can be emotionally intense and require advanced communication skills. 16 As similar studies for PC populations have not yet been published, we examined registry data of racial and ethnic composition and language skills of hospital PC patients and clinicians in California where nearly 44% of households speak a language other than English at home, with nearly 70% of those households speaking Spanish, to understand the degree to which concordance between these groups may exist.17,18
Objective(s)
To characterize and compare the racial and ethnic background and language fluency among clinicians and their patients in inpatient PC settings in California.
Methods
The Palliative Care Quality Network (PCQN) was established in 2009 as a quality improvement collaborative comprised of interdisciplinary PC teams across the United States. 19 Until a recent merger with other registries, 94 PCQN member teams collected standardized data on all clinical encounters. Optional data elements included race/ethnicity and preferred language of patients. We used PCQN data from inpatient PC teams that collected data on patient race/ethnicity and language. Because data is collected from clinical encounters that took place during hospital admissions, it reflects contact between patients and members of the PC team that occurred exclusively in the hospital setting. Of the eighteen teams that collected data on race/ethnicity and language (REL) for over 85% of their patients, 15 were in California. We therefore limited our analysis to PCQN teams in California.
Between February 2021 and August 2021, we contacted those 15 California PCQN inpatient PC teams to request information about the self-reported race/ethnicity and language skills of the clinical team members working at each site during the timeframe for which they submitted patient data. We sent a survey by email to the director of each PC team, who then distributed the survey to their team members. These requests were followed by both reminder emails and/or a phone call to the service directors. Each team member was asked to report only their role on the team (physician, nurse, etc.), their race(s) and ethnicity (ies), and languages spoken fluently. Race/ethnicity categories for the survey matched the categories for the patient data set.
We compared data from PCQN clinical team members with those of the patients seen by each team to examine concordance. We defined racial/ethnic concordance as having at least one PC team member from a specific patient-represented racial/ethnic group and language concordance as having as least one team member who was fluent in a preferred patient language other than English. We excluded individuals with race/ethnicity and/or language reported as “other.” Because patients with certain serious illnesses may receive care within a larger region for subspecialty services, the catchment area for a given PC team can be wide. Because California is a very large state with patients generally receiving care within a region (Northern or Southern relative to the common dividing line of San Luis Obispo), we divided data from participating teams and their patients into these geographic areas to better reflect regional clinician and patient compositions. Five of the 15 teams were in Northern California and ten were in Southern California.
Continuous variables were summarized using means (95% confidence intervals [CI]) and medians (with range). Frequencies were calculated for categorical variables. We used chi-squared tests (
Results
We received survey responses from 9 of the 15 teams (60%). Fifty-one clinicians completed the survey, representing 80% of the total number of clinicians. Three responding teams were in Northern California and six were in Southern California, representing 60% of teams contacted in each region. Of the 6 teams that did not respond, 4 were in Southern California and 2 in Northern California.
Patient and Clinician Characteristics Across Surveyed Inpatient Pc Programs.
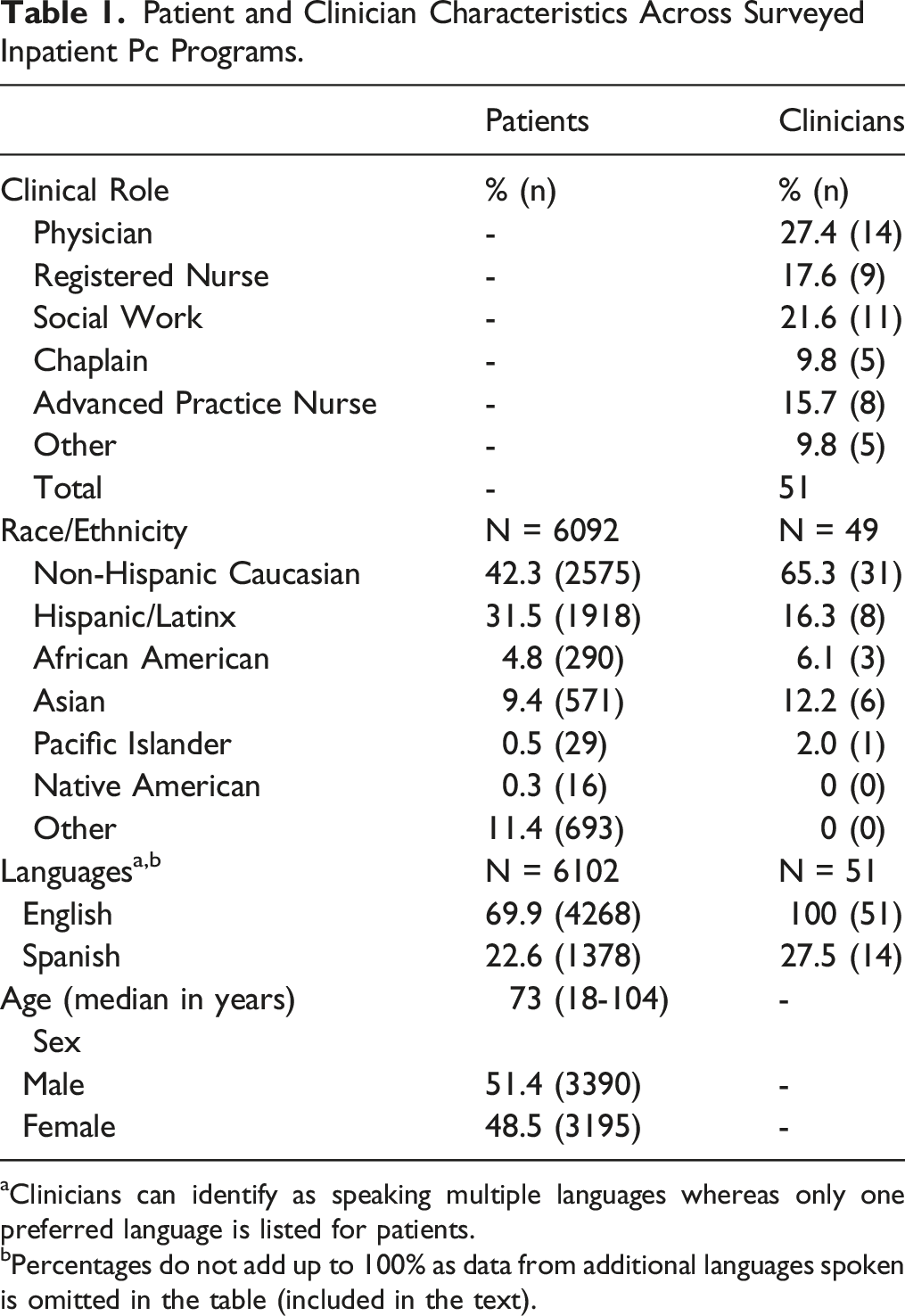
aClinicians can identify as speaking multiple languages whereas only one preferred language is listed for patients.
bPercentages do not add up to 100% as data from additional languages spoken is omitted in the table (included in the text).
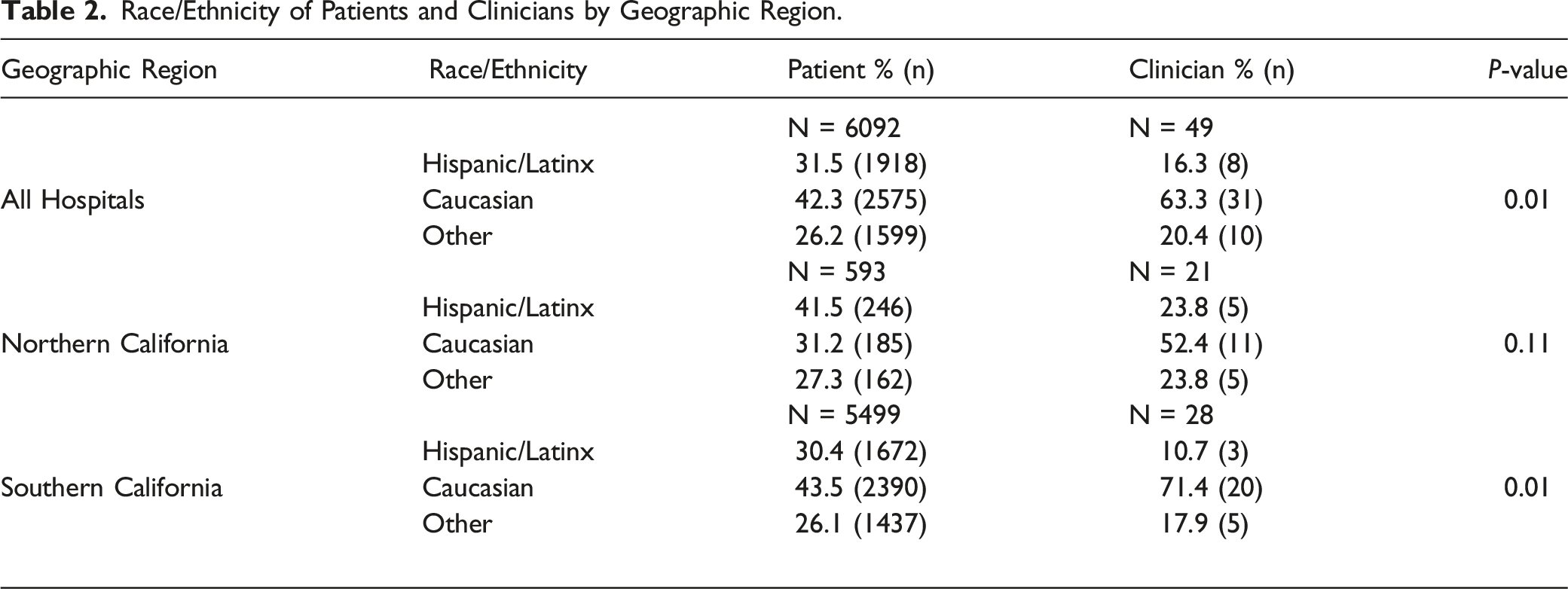
Race/Ethnicity of Patients and Clinicians by Geographic Region.
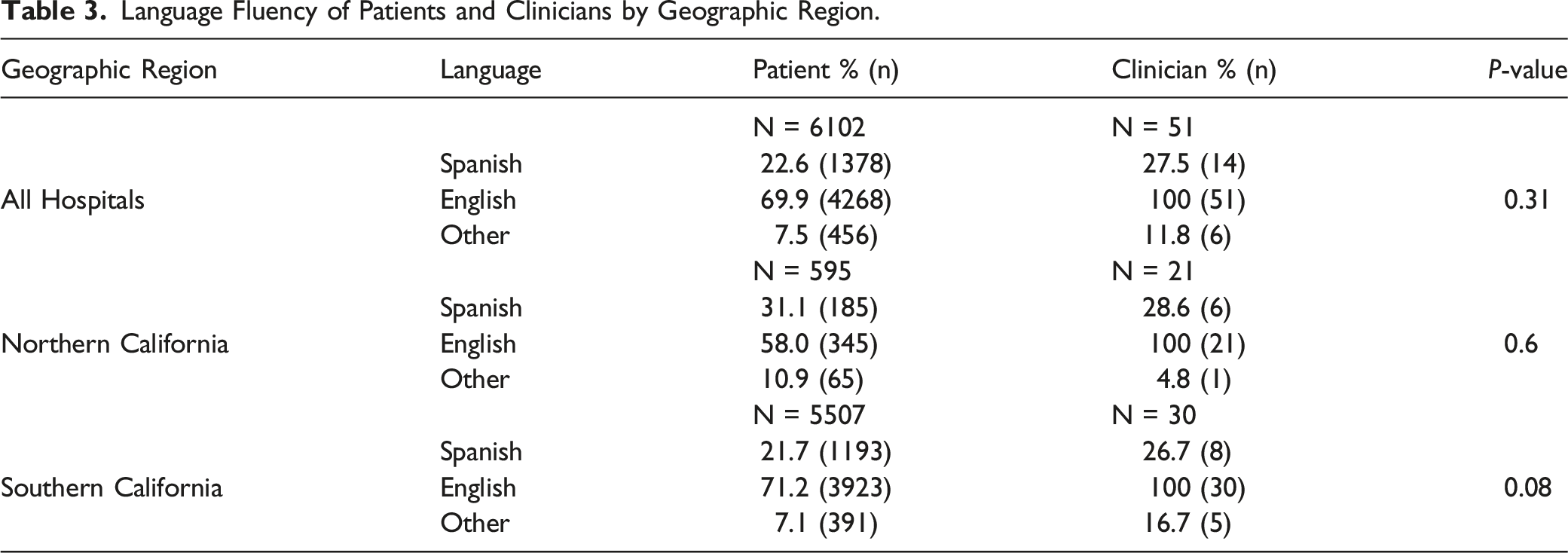
Language Fluency of Patients and Clinicians by Geographic Region.
All clinicians reported fluency in English and 14 of the 51 respondents (27.5%) also reported fluency in Spanish (see Table 1). Two clinicians (3.9%) also spoke Vietnamese, 2 spoke Tagalog (3.9%), one reported fluency in Korean (1.9%) and one spoke another language listed as “other” (1.9%). Among patients, a majority (69.9%) preferred English and 22.6% had Spanish listed as their preferred language. Small numbers of patients were listed as having other preferred languages, including Tagalog (1.6%) Mandarin (1.5%), Vietnamese (1%), Cantonese (.8%), Korean (.6%) and “other” (2%).
Six of the 9 teams had at least one Spanish-speaking clinician (5 teams with one Spanish speaker and one team with 2 Spanish speakers) and all cared for Spanish-speaking patients. English fluency was higher among clinicians than patients (100% vs 69.9%) and similar proportions of patients and clinicians reported fluency in Spanish (22.6% vs 27.5%, P = .31).
Among the different clinical disciplines, we found that Spanish-speakers were more commonly found among social workers (45%) followed by physicians (35.7%), advanced practice nurses (25%), chaplains (20%) and nurses (11%). Eight of the 9 teams had at least one clinician fluent in another language in addition to English and 7 had at least one non-White clinician. Of the clinicians who identified as Hispanic/Latinx the majority were social workers (62.5%), followed by physicians, nurses, and chaplains, each making up 12.5%.
We compared patient characteristics of PC teams that did not respond to the survey about clinician REL data with patients of the teams that did respond to the survey and found no clinically meaningful differences between the 2 groups in terms of the reported sex or age of patients (Female: 48.0% vs 48.5, P < .001; age 73.4 vs 72.9 years, P < .001). Patients cared for by PC teams that responded to the survey were less likely to be White (46.3% vs 59.9%) and more likely to be Hispanic/LatinX (29.3% vs 27.0%), Black (6.9% vs 2.4%), or Asian (13.3% vs 7.8%) (P < .001). Similarly, for preferred language spoken, patients of responding PC teams were less likely to prefer English (68.7% vs 80.9%), and more likely to report speaking Spanish (21.1% vs 14.6%), and Chinese (4.5% vs .8) (P < .001).
Discussion
Concordance of race, ethnicity and language has been shown to positively impact patient outcomes and experience in primary care settings and can help to mitigate disparities in care.10-15 We found significant differences in the racial/ethnic distributions of Hispanic/Latinx patients and clinicians in the state of California overall, with the greatest difference among the populations of clinicians and patients in Southern California. While the vast majority of responding teams had at least one non-White clinician, this still represents a marked difference from the California population, which is only 35% White non-Hispanic. Nearly half of the teams (4 of the 9) did not have a clinician who identified as Hispanic/Latinx despite serving a significant patient population from that racial/ethnic background. Given studies to date suggesting the importance of racial/ethnic concordance, this disparity raises the question of whether a lack of representation of Hispanic/Latinx clinicians relative to the patient population may be contributing to relatively lower palliative care utilization of these patient populations.
With regard to language, 6 of 9 teams had at least one Spanish speaking clinician. Having even one team member fluent in a language other than English has the potential to meaningfully address a language disparity. However, depending on the workflow and capacity of multilingual team members, one’s ability to focus on seeing patients for whom they can provide language-concordant care may vary substantially. While we found the proportions of palliative care clinicians and patients who speak Spanish fluently was similar overall, having a third of teams without a Spanish-speaking clinician, and 5 of 9 teams with only one Spanish-speaking clinician greatly reduces the likelihood of language concordant encounters.
Interestingly, teams that did not respond to the REL survey had greater proportions of patients who were White and primarily English-speaking compared to patients cared for by teams that did respond to the survey. It may be that these teams do not perceive a reason to collect REL data. Because we do not have REL data about the clinicians on those teams, we cannot assess whether those clinician teams may reflect the patient population more closely than the responding teams. However, even these teams see a sizable proportion of patients who are non-White and who are not English speaking and highlight the need for more thorough and consistent data collection about REL characteristics of both patients and clinicians.
This study has several limitations. First, we analyzed data for inpatient PC teams in California, so our conclusions may not be generalizable in other states or in outpatient PC settings. Second, the ability in this study to accurately characterize the racial/ethnic background of patients is hindered by a standardized approach to collection of these elements by all PC teams. The race/ethnicity data in the PCQN registry is populated by the electronic medical record of reporting teams and most, if not all, of these do not allow patients to choose multiple categories of race/ethnicity. If we hope to explore healthcare disparities in the field of PC, we need accurate and consistent data that is not currently widely available. Lastly, we were only able to collect and analyze data about the racial/ethnic background and languages spoken by clinicians caring for a population of patients rather than specific REL data for individual patient-clinician interactions. The PCQN dataset does not provide that level of detail. We hope to be able to evaluate the extent to which individual Spanish-speaking patients are cared for by Spanish-speaking clinicians and whether REL concordance has any impact on clinical outcomes in future studies. Data about individual patients was not available to us for this study, though the population-level analyses still contribute new information to an area where little currently exists and can inform future studies.
Our study demonstrated significant differences in the populations of Non-Hispanic White and Hispanic/Latinx and Spanish-speaking patients and clinicians with many teams having no member that speaks a language other than English. Because prior studies demonstrate the benefits of culturally concordant care, further investigation is required to investigate the impact of both cultural and linguistic differences on the quality and frequency of PC services utilized by patients from minority populations, as the impact of each category of concordance may be distinct. For example, the impact on communication, trust and rapport building when a patient interacts with a clinician who shares their racial/ethnic identity may be different from the connection they may perceive with a team member who can easily and clearly communicate with them in their preferred language and different types of concordance may impact different outcomes. More widespread and detailed data from a national registry could be of great help in understanding these issues. Identifying, understanding, and addressing REL disparities on individual, organizational, and societal levels, including exploration of the impact of the racial/ethnic makeup and language skills of PC clinicians and whether and how the use of interpreters and cultural brokers impact quality is essential to providing equitable palliative care. Until we can accurately measure potential disparities in these areas, we cannot begin to adequately address them with the goal of providing the best quality PC for all patients who need it.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was generously supported with funding from the Hellman Foundation.