
Abstract
General inpatient (GIP) hospice care is used only minimally for hospice patients, and more than a quarter of Medicare hospice facilities do not provide GIP care. To determine the impact of hospices’ capacity to provide on emergency department use during hospice enrollment and live discharge from hospice, we used Surveillance, Epidemiology, and End Results-Medicare linked data and CMS Provider of Services data from 2007 to 2013 from ten states and two metropolitan regions. Grouping hospices into three GIP care provision categories: 1) no-GIP; 2) GIP-contract; and 3) GIP-IHF where hospices directly provide GIP care in their own inpatient hospice facility (IHF), we built a multilevel logistic model that accounted for unobserved hospice characteristics. Nearly 9% of the study sample received GIP care, of which 82% received such care in the last week of discharge. GIP-IHF hospices had lower live discharge rates than no-GIP hospices (AOR: .61; 95% CI: .47-.79; P < .001) and GIP-contract hospices (AOR: .84; 95% CI: .70-1.00; P < .05). Similarly, GIP-contract hospices were also associated with a decreased risk of live discharge, compared to no-GIP hospices (AOR: .76; CI: .62-.92; P < .05). There was no difference in emergency department use between no-GIP hospices and hospices with such capacity. Our results suggest that hospices capable of providing GIP care have lower live discharge rates than their counterparts. However, the fact that GIP care tends to be provided too close to death limits its effectiveness in preventing avoidable emergency department use
Keywords
Introduction
The Medicare Hospice Benefit (MHB) is available to Medicare beneficiaries with a life expectancy of 6 months or less who forego curative treatment. 1 Medicare Conditions of Participation require a Medicare-certified hospice to demonstrate that it can provide the following four levels of care to meet patients’ needs: 1) routine home care (RHC), or default level of care if other levels of care are not provided; 2) continuous home care (CHC), or intensive at-home care by a nurse or aide for periods of a pain or symptom crisis; 3) inpatient respite care (IRC), or inpatient care to relieve the patient’s primary informal caregiver temporarily; and 4) general inpatient (GIP) care, or pain or symptom management that cannot be provided outside of an inpatient setting. 2 In 2020, RHC comprised 98.7% of Medicare hospice beneficiary total days, GIP care accounted for just 1.0% of hospice care days; CHC and IRC accounted for the remaining .4%. 3 Amid concerns that GIP care has been steadily decreasing over time, this study focuses on GIP care, one of the three non-default levels of hospice care used relatively minimally given that the MHB affords all four to meet patients’ clinical needs.
According to the Office of Inspector General (OIG) report, 4 a hospice plays a larger role in determining patients' access to GIP care rather than the patient’s needs. Hospices that used their own or leased inpatient hospice facility (IHF) 5 provided GIP care to 35% of their beneficiaries compared to hospices that used hospitals or SNFs and provided GIP to just 12% of their beneficiaries in 2011. The OIG also reported that 27% of all Medicare hospices did not provide a single day of GIP care to their beneficiaries in 2011. This finding was unexpected because the purpose of the OIG study and its subsequent studies was to investigate potential fraud and abuse in hospices using GIP care.6,7
Despite concerns about hospices’ underutilization and overutilization of GIP care, few empirical studies have examined whether (1) hospices that underutilize GIP care perform relatively poorly in key patient outcomes; and whether (2) hospices that can directly provide GIP care in their IHFs perform better than hospices that only refer patients to contracted facilities for GIP care. In this study, we examined the independent effect of GIP-provision capacity on hospice patients’ ED use during hospice enrollment and the live discharge rate while controlling patient factors and hospice factors known to be associated with each of the outcomes. We hypothesized that hospices equipped with full capacity to provide GIP care might be more efficient at anticipating, preventing, and treating pain and symptoms than those with limited or no capacity, resulting in better performance in preventing emergency department (ED) visits during hospice enrollment and live discharges from hospices. Although some ED visits are not avoidable, other ED visits can be attended to with GIP care.8,9 ED visits tend to result in hospitalizations, and subsequently live discharge from hospices. 10 Live discharge is considered problematic when followed immediately by hospitalization and subsequent re-admission to hospice or when followed by hospitalization with the patient dying in the hospital. 11 Problematic live discharges may be attributable mainly to hospice-initiated discharges under the circumstances where a hospice is trying to avoid costly hospitalizations or hospices have no contracted facilities to send the patient for GIP care.10,12 In addition, early live discharge (first 7 days) and late live discharge (days 180+) are monitored as hospices’ quality of care measures. 13 Live discharges that occur too early or too late may indicate hospices’ inappropriate practices. 10
Methods
Study Cohort
We used Surveillance, Epidemiology, and End Results (SEER) - Medicare-linked data to identify individuals with lung, bone, brain, liver, pancreatic, and stomach cancers diagnosed between 2007 and 2012. 14 For individuals with multiple cancer types, we chose the first-diagnosed cancer as the index cancer. We identified and selected those who enrolled in in-home hospice programs between 2007 and 2012, as noted in MHB claims, following the index cancer diagnosis. By focusing on in-home hospices, we excluded those individuals who received GIP care in inpatient settings after being discharged from hospitals. We limited the population to those aged 66 years and older at the time of hospice enrollment with at least 1 year of continuous fee-for-service (FFS) Medicare Part A and Part B enrollment prior to hospice enrollment. For individuals with multiple hospice discharges during the study period, we selected only the first episode. We followed the patients until the end of 2013 and excluded those still in hospice care at the end of 2013. In addition, we excluded those individuals who received care from hospices outside of SEER areas because we focused on hospices operating in SEER areas. This study was determined to be exempt by California State University, Northridge Committee for Protection of Human Subjects.
Variables
Outcome Measures
For the ED use outcome, we linked MHB beneficiary records to ED claims data. This allowed us to determine ED visits during hospice enrollment and ED visits in the month prior to hospice enrollment. We did not consider an ED visit occurring on the same day of admission to hospice or live discharge from hospice to be an ED use during hospice enrollment. 8 For the live discharge outcome, we identified three hospice discharge types: death, live discharge due to transferring to another hospice, and live discharge for other reasons. We considered any non-death discharge to be a live discharge for this study. The 2007 National Home and Hospice Care Survey showed that patients switched to another hospice for many reasons, one of which included “because another hospice provides GIP”. 15 Our analysis of tracking those who moved to another hospice also showed that 32% received GIP care in another hospice. We conducted a sensitivity analysis where we excluded live discharges due to transfer to another hospice to examine if the findings remained consistent.
Hospice characteristics
Emergency Department Rate and Live Discharge Rate by Patient and Hospice Characteristics.
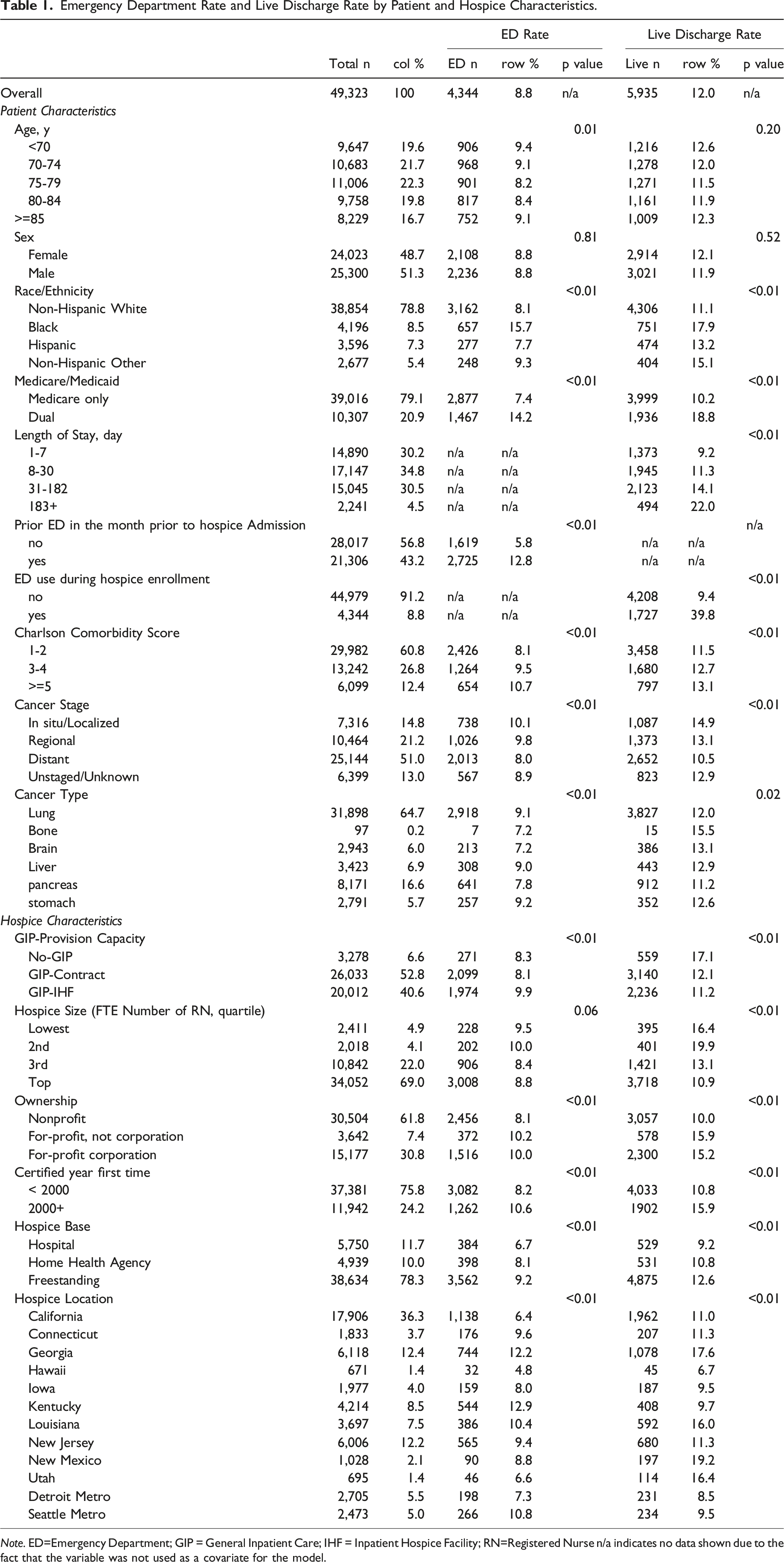
Note. ED=Emergency Department; GIP = General Inpatient Care; IHF = Inpatient Hospice Facility; RN=Registered Nurse n/a indicates no data shown due to the fact that the variable was not used as a covariate for the model.
Patient Characteristics
The cohort consisted of 49 323 patients with selected cancer types who enrolled in home-based hospice programs between 2007 and 2012 and were followed through discharge by the end of 2013. Table 1 presents patient characteristics of the cohort related to the two outcome measures. We included three demographic variables (age, sex, and race/ethnicity). As a surrogate for socioeconomic status (SES), we included dual status (i.e., having both Medicare/Medicaid as an indicator of low SES). In addition, we analyzed four clinical variables as risk-adjusting measures to account for differences in patient health status and clinical factors that were present before hospice enrollment: ED use in the last month prior to hospice enrollment, Charlson Comorbidity Index, cancer stage, and cancer type. Inpatient Hospital Stay, Outpatient, and Carrier (physician/supplier) Claims were used for computing the Charlson Index based on ICD-9CM diagnosis codes for up to 1 year before hospice enrollment.17,18
There is one notable difference in covariates between the ED use model and the live discharge model. Since ED use was conceptualized as occurring during hospice enrollment, we did not use variables that occurred during hospice enrollment. By comparison, for the model of the live discharge that signals the end of hospice enrollment, we included the length of stay and ED use during hospice enrollment instead of ED use in the month prior to hospice enrollment.
Statistical Methods
Numerical variables were described as means and percentiles. Categorical variables were described as totals, frequencies, and row/column percentages. We chose multilevel logistic models for our outcomes for two reasons: (1) the method explicitly accounted for correlations in outcomes among patients enrolled in the same hospice, and (2) the method allowed us to obtain findings adjusted for unobserved hospice characteristics (e.g., hospice-specific efforts to reduce ED use) that we were not able to include in the model. 19 All reported P values were 2-tailed. For all tests, P < .05 was considered statistically significant. All statistical analyses were performed using STATA SE version 17.0 (STATA Inc).
Results
ED Use During Hospice Enrollment
Table 1 presents rates of ED use during hospice enrollment. Of the study cohort, 8.8% had at least one ED visit during hospice enrollment. ED use among patients of GIP-IHF hospices was higher (9.9%) in comparison with no-GIP hospices (8.3%) and GIP-contract hospices (8.1%) (all P < .01), which was opposite to our hypotheses. There was a notable difference in ED use when comparing patients with and without ED visits in the month prior to hospice enrollment (12.8% vs 5.8%; P < .01). Moreover, being Non-Hispanic Black was associated with increased ED use (15.7%) compared to being Non-Hispanic White (8.1%), Hispanic (7.7%), and Non-Hispanic other (9.3%) (P < .01). Having dual status also increased the risk of ED use in comparison with having Medicare only. A higher comorbidity score was associated with a higher ED use rate.
Multilevel Logistic Model for Emergency Department Use During Hospice Enrollment (N=49,323).
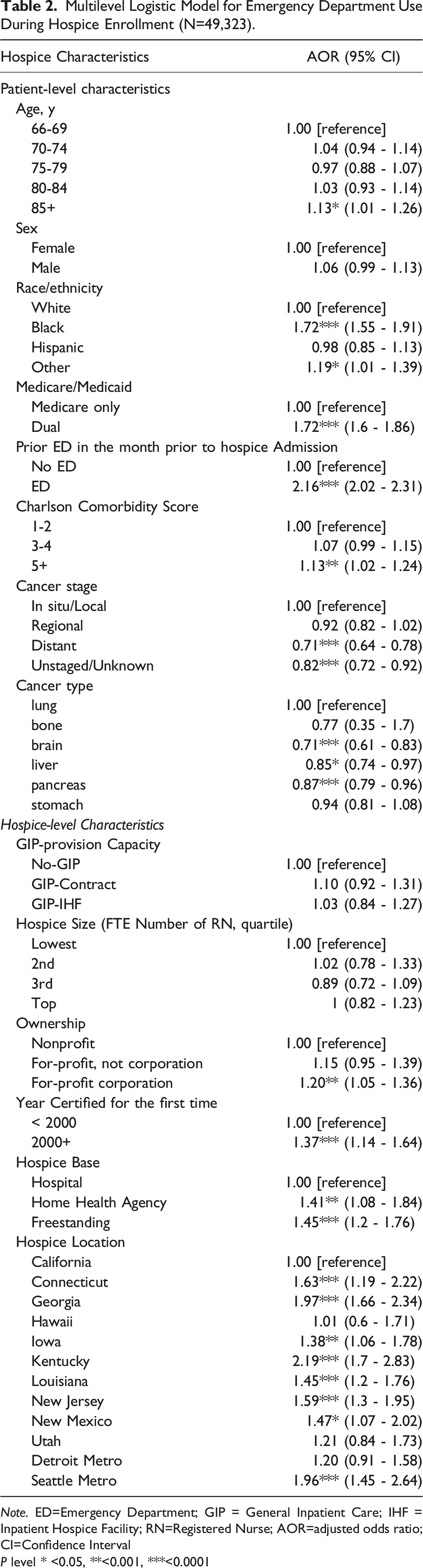
Note. ED=Emergency Department; GIP = General Inpatient Care; IHF = Inpatient Hospice Facility; RN=Registered Nurse; AOR=adjusted odds ratio; CI=Confidence Interval
P level * <0.05, **<0.001, ***<0.0001
Live Discharge
Table 1 also presents the unadjusted rates of live discharge. Of the study cohort, 12% had a live discharge (including discharges due to transfer to another hospice). The live discharge rate was lower among GIP-IHF hospices (11.2%) and GIP-contract hospices (12.1%) compared with no-GIP hospices (17.1%). There was a hugely notable difference in live discharge when comparing patients with and without ED visits during hospice enrollment (39.8% vs 9.4%). Dual status had a higher live discharge rate (18.8%) than Medicare only (10.2%). A longer length of hospice stay was associated with an increased risk of live discharge. A higher comorbidity score was associated with an increased risk of live discharge.
Multilevel Multivariable Logistic Analysis Adjusted for Case Mix, Hospice-Level Characteristics.
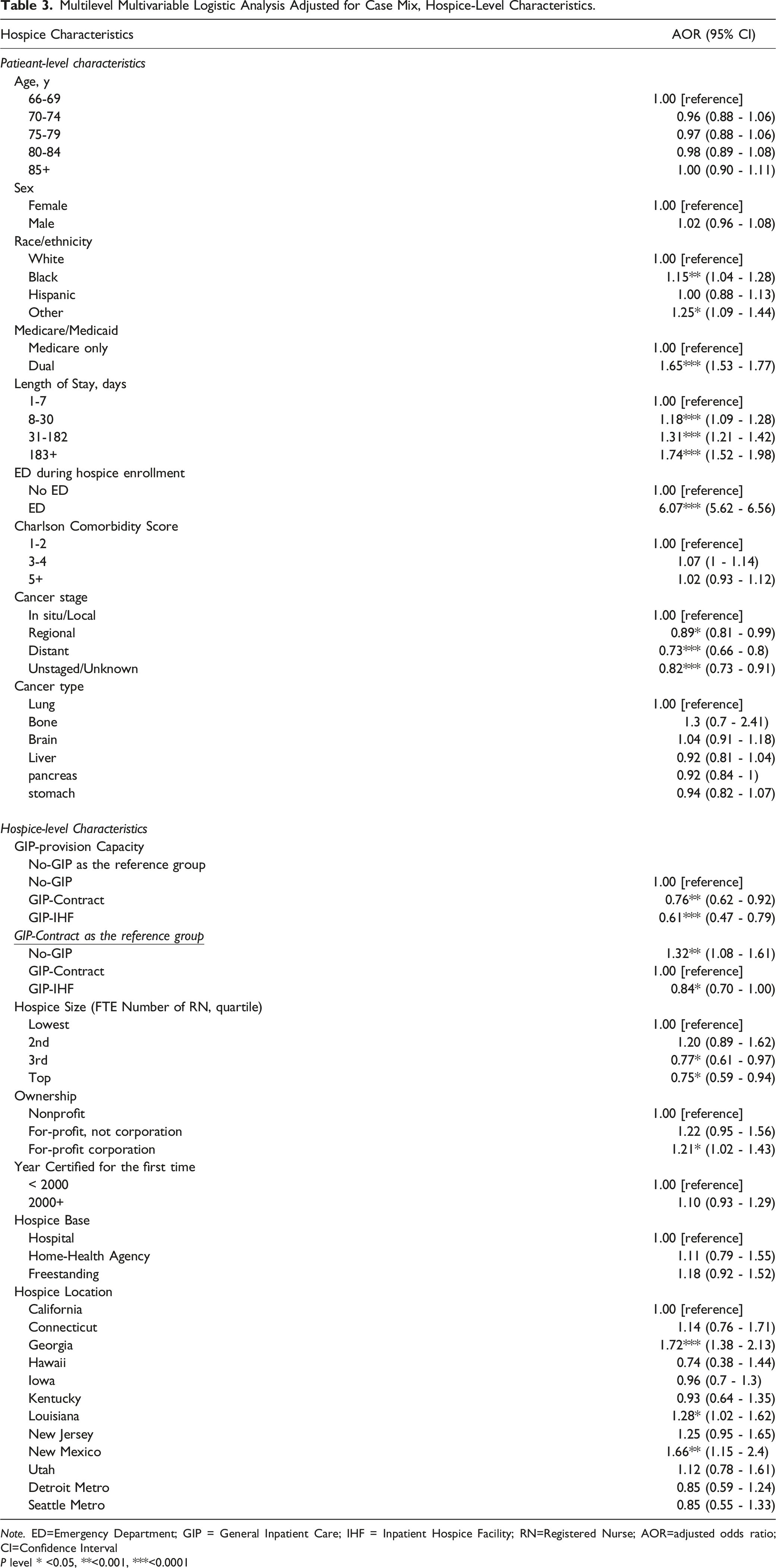
Note. ED=Emergency Department; GIP = General Inpatient Care; IHF = Inpatient Hospice Facility; RN=Registered Nurse; AOR=adjusted odds ratio; CI=Confidence Interval
P level * <0.05, **<0.001, ***<0.0001
Discussion
This study provides empirical evidence that hospices with the capacity to provide GIP care were associated with decreased risk for live discharge among their patients, even after adjusting for case mix and hospice-level factors known to be related to live discharge. Specifically, the association was robust to adjustment for hospice ownership and hospice size, thus reflecting the association of GIP-provision capacity with live discharge independent of ownership and hospice size. This finding supports CMS’ recent decision that the Hospice Quality Reporting Program (HQRP) include GIP care provision as one of hospice process measures starting in October 2021. 13 We also found significantly better performance in live discharge by hospices with IHF than by GIP-contract hospices. We speculate that GIP-IHF hospices might be more capable and willing to provide GIP care to patients with severe cancer pain 20 than GIP-contract hospices. This finding is consistent with studies reporting a significantly higher satisfaction level among caregivers of patients treated at an IHF than in other settings. 21
Unadjusted results showed that hospices having an IHF had a higher rate of ED use during hospice enrollment than GIP-contract hospices relying on contract per patient or hospices with no GIP care capacity. We speculate that this may be partially attributable to our definition of ED visits during hospice enrollment. That is, since we did not consider an ED visit occurring on the same day of live discharge to be an ED use during hospice enrollment, this may have led to more counting of ED visits in a hospice that can prevent live discharge among those with uncontrollable pain/symptom who arrived at ED. When hospice is unable to provide GIP care, a patient may be discharged alive from hospice on the same day as an ED visit. By comparison, hospices with an IHF or relying on contracts may be more effective than no-GIP hospices at reducing live discharge after ED visits occur. In interviewing hospices across the U.S., a study found that once a hospice patient is admitted into a hospital following an ED visit, live discharge is often the only choice unless that hospital can offer GIP care because of an existing contractual relationship. 22 By comparison, if the patient’s hospice has an IHF, ED staff may transfer the patient to the IHF. 23 Furthermore, after adjusting for covariates, the differences in ED use during hospice enrollment were no longer significant. This suggests that hospices with an IHF might see patients with more complex or severe illness than two other types of hospice. Finally, the lack of a positive effect of the GIP-provision capacity factor on ED use during hospice enrollment may not be surprising given GIP care tends to be provided near the end. For GIP to be effective, it may need to be provided timely or proactively to help prevent ED visits.
Our study has several strengths. Prior research has focused on the relationship between live discharge and hospice characteristics such as ownership status or hospice size and patient-level characteristics such as insurance type.10,24,25 While we examined these variables and found their relationship with live discharge generally consistent with previous studies, our examination widened the scope of potential determinants to include hospice-level capacity to provide GIP care. Future research should build upon our research here and examine the degree to which GIP-provision capacity (and the capacity for other non-default levels of care) may influence hospice quality outcomes. Better understanding the importance of the capacity of higher levels of care in terms of quality and cost outcomes could aid policymakers in determining future CMS regulations for its Conditions of Participation for hospices.
The OIG reports mentioned earlier did not differentiate between in-home hospice patients and hospice patients who never left a hospital or an IHF and likely may have only received GIP care shortly before death. By excluding the latter patients and focusing only on patients who started hospice at home with the default level of care, the study herein can provide a better understanding of the GIP-provision capacity factor influencing hospice quality outcomes. Another strength of this study is that it is based on large population-based data, which allowed us to exclusively analyze six poor-prognosis cancer types. Focusing on patients with poor prognosis cancers was relevant in that ED visits or live discharges were more likely due to acute crisis rather than pursuing curative care or being no longer eligible for hospice care.
There are several limitations to our study. First, we limited our study population to MHB beneficiaries with traditional FFS Medicare because SEER-Medicare linkage data only provides FFS claims data, used to create the Charlson Comorbidity Index measures and ED visits prior to and during hospice enrollment. However, our exclusion of Medicare Advantage plan MHB beneficiaries may not be too problematic. This is because Medicare Advantage penetration during our study years was not as high as in recent years. Another limitation is that despite our efforts at correctly categorizing hospices regarding GIP-provision capacity, we could not exactly match a patient to a hospice with a correct classification. This was mainly due to the fact that hospice classifications for the same hospice could change over time. For example, a hospice considered to have an IHF may have started operating the IHF in the middle of the study period. Unfortunately, detailed data on IHFs such as the establishment year is not readily available, hampering a study of IHF-related performance measures.
Conclusion
In this study, hospices with no GIP capacity or limited GIP capacity were less likely to decrease live discharges than hospices with IHF. Current efforts to increase the GIP reimbursement rate and include GIP provision as part of hospice performance measures may improve access to GIP care.26,27 There is, however, a need for further policy changes in light of the continuing decline in GIP utilization. Even though hospice surveyors are required to determine the presence of a GIP contract, the infrequent conducting of hospice surveys and the lack of sanctions for not having a contract may have contributed to the declining rate of GIP care. An appropriate level of enforcement of hospice compliance with GIP contracts in place should be considered as part of a hospice reform effort. It is especially important to apply this to the certification of new hospices in regions with high hospice growth rates. Finally, for GIP services to be effective, a significant improvement in timely access to hospice care should come first. Relatedly, GIP care immediately before death or live discharge may indicate the limited role of GIP care in preventing disruptions such as ER/hospitalization occurring while in hospice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 10.13039/100000009; Foundation for the National Institutes of Health; 1P20MD003938