
Abstract
Keywords
Introduction
Many terminally ill patients aim at spending their end of life at home. However, the physical or mental limitations that terminally ill patients face may prevent them from leaving their house independently, resulting in a large symptom burden and social isolation.1-4 In addition, many at-home family caregivers report caregiver burden, and desire (temporary) relief. 5 Palliative care and hospice services are available to support patients and their families with inpatient and home-based care. In Germany, hospice and palliative care is primarily covered by inpatient, outpatient, and home-based services, which are available to a relatively large number of people compared to the situation in other European countries. Germany is therefore rated highest on 6 levels of palliative care in Europe. 6 In some countries, including Germany, inpatient, outpatient and home-based care services are also supplemented by day care facilities.
In Germany, 2 forms of day care services exist for patients with palliative care needs: (1) day hospices and (2) palliative day care clinics. In both facilities, terminally ill patients are cared for during the day, providing family caregivers temporary relief. Day hospices in Germany have an average daily capacity of 6.6 patients. 7 In addition to administering palliative therapies (eg palliative care, psychological therapy, physiotherapy, art therapy), day hospices aim at allowing patients to rest and facilitating social exchange, to counteract patients’ social isolation. In contrast, palliative day care clinics are attached to a hospital and have an average daily capacity of 3.3 patients. 7 The main focus of these clinics is the administration of medical symptom-relieving treatments, alongside other therapies (eg psychotherapy, physiotherapy). Patients may visit at regular intervals. Since all of the hospital’s specialist departments may be called in to care for a patient, as required, the patient is spared of the need to make several appointments with various outpatient services or to schedule inpatient stays for invasive procedures (eg ascites puncture), as these may also be carried out within the day care clinic.
Currently, only a few hospice and palliative day care facilities exist in Germany. Specifically, an inventory analysis in 2020 identified 13 day hospices and 5 palliative day care clinics. 7 Given the well-developed infrastructure of inpatient, outpatient, and home-based hospice and palliative care services in Germany, the question arises: Are the needs of patients and family caregivers sufficiently covered by existing services? And if not, to what extent might patients and family caregivers additionally benefit from day care services?
The present study aimed at exploring the benefits of hospice and palliative day care services from 2 perspectives: (1) that of day hospice and palliative day care clinic managers, via interviews; and (2) that of representatives of hospice and palliative care services (within hospice and palliative care networks), via focus groups.
Methods
The methods and findings are reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ). 8
Study Design
To elicit the views of experts from inside and outside the facilities, semi-structured telephone interviews were conducted with managers of a select number of day hospices and palliative day care clinics, to capture internal perspectives (January-February 2021), until relative qualitative data saturation was reached. Relative data saturation was defined as the point at which new interviews generated only little or no change to the category system. Additionally, focus groups were run with representatives from the day care facilities’ hospice and palliative care networks, to capture external perspectives. Focus groups were carried out in person, in the relevant local regions (September-October 2021).
Participant Recruitment and Data Collection
Selection criteria for hospice and palliative day care facilities.

In the second step, focus groups were organized, ensuring representation from as many network institutions (and especially care providers) as possible. Inpatient, outpatient, and home-based care services that were local to each day care facility were contacted and asked to participate. Preference was given to providers who had been identified as active network participants by the interviewed managers. Eligible participants had to be aware of the existence of the local day care facility. Focus groups were moderated by 2 out of 3 trained researchers BA, CH (female, health scientist, researcher), and HAAR. A semi-structured interview guide was developed to determine the extent to which participants perceived the day care facilities as integrated into the local care landscape, as well as what challenges existed and what needs could or could not be met by the facilities. Focus group participants were shown select quotes from the facility manager interviews (step 1) as discussion stimuli.
All participants were informed by telephone and in writing about the nature, content, and aim of the study and provided written informed consent prior to participating. The individual qualitative interviews and focus groups were conducted in German, audio recorded, and transcribed verbatim by research assistants (interviews) and an external transcription office (focus groups).
Data Analysis
Qualitative data were coded and analyzed using MAXQDA Plus Portable 2020 software (VERBI Software Consult Sozialforschung GmbH, 1989-2021). All transcripts were coded independently by 2 of the 3 researchers (BA, CH, HAAR). Subsequently, codes and codings were revised by the researchers, in consultation. Finally, a fourth researcher (FAH) assessed coding consistency.
Interviews and focus group transcripts were coded consecutively. First, the qualitative interviews with managers were coded according to Mayring’s 9 qualitative content analysis. Main categories were derived a priori from the interview guide, using a deductive approach. Subcategories were added inductively from the interview material. Second, the focus group data were coded on the basis of the code system developed from the qualitative interviews. New codes were added inductively for emerging issues. No further key themes arose.
Results
Composition of focus group participants.
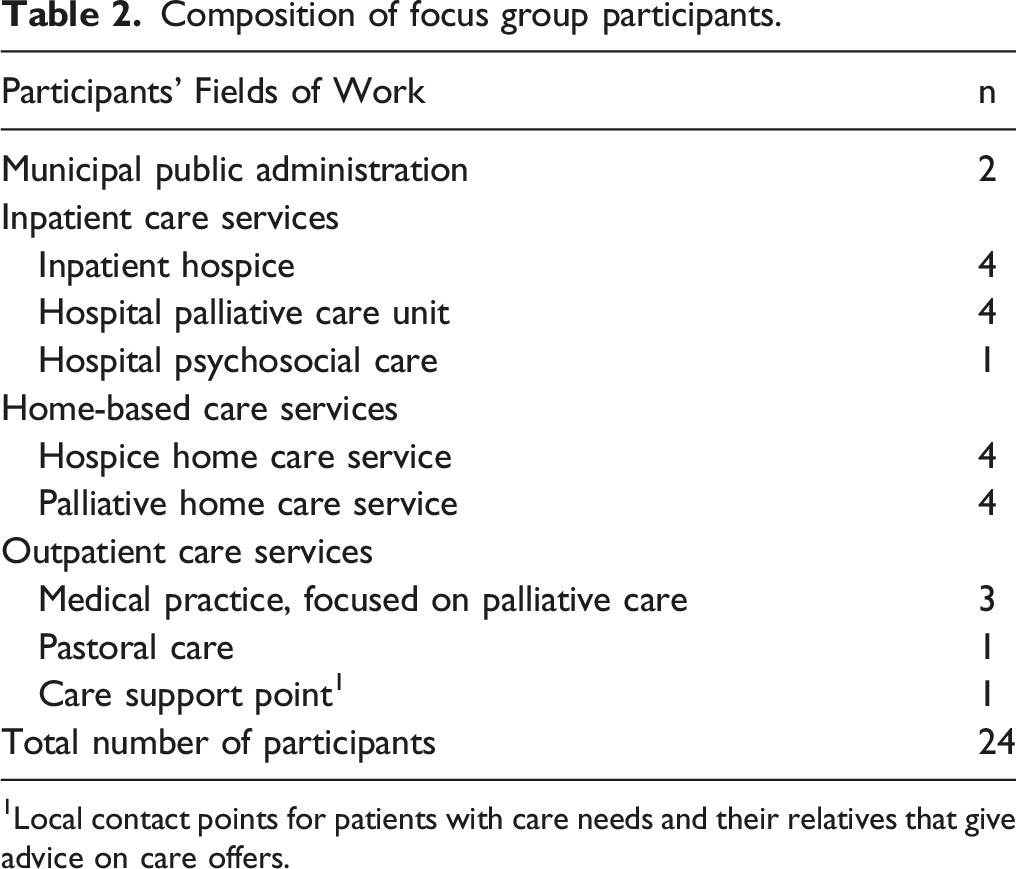
1Local contact points for patients with care needs and their relatives that give advice on care offers.
Main Themes Emerging From the Internal and External Perspectives
Four key themes emerged from the qualitative data analysis, regarding the benefits of day hospices and palliative day care services in Germany: (1) hospice and palliative day care benefits for patients, (2) hospice and palliative day care benefits for family caregivers, (3) regional gaps in palliative care services and how these could be addressed by hospice and palliative day care services, and (4) ideas for optimizing the benefits of hospice and palliative day care services. The contents of the key themes are presented below, with contrasting quotes from the interviews (ie, internal perspective) and focus groups (ie, external perspective).
Hospice and Palliative Day Care Benefits for Patients
The interviewees and focus group participants described that many patients desire to live at home for as long as possible, and thus avoid inpatient stays: “These are mostly patients with a [malignant] tumor disease; (...) they run from 1 doctor to the next. They have endured several hospital stays and, of course, they don’t want to have any more hospital stays” (Manager [M]4, palliative day care clinic [PDC]). Both groups also saw an increase in patient needs for social interaction, due to the growing number of people living alone. Palliative day care clinics and day hospices may address these needs. At the same time, the interviewees and focus group participants reported that various preconditions must be met to allow patients to maximally benefit from day care services: the organization of transport to the facilities, a combination of medical/nursing and psychosocial care, and premises that enable both exchange with other patients and privacy and space for rest and relaxation. Some managers reported that patients rarely need day care services on a daily basis. Rather, for seriously ill people living at home, day care attendance 3 times a week is often sufficient, because the visit, itself, may be experienced as exhausting. However, day care might not meet every patient’s care needs. One care support point representative from a town with a resident day hospice described her experience as follows: “People make a conscious decision to stay at home with this illness, with this dying situation or they want 100% inpatient care right away. (...) When we come to the issue of day care, very few people say: ‘I can imagine that’” (P22).
Hospice and Palliative Day Care Benefits for Family Caregivers
In both the interviews and the focus groups, participants raised the need to protect family caregivers from overburden (an aim of day care services), so they are better “able to bear and endure the ongoing caregiving responsibility at home” (M3, DH). Furthermore, participants perceived it as helpful for family caregivers to have a specific contact person at the day care facility who could provide advice. In a focus group, a social worker at a hospital reported: “I have the impression that some family caregivers are more confident about taking the ill person home with the prospect of the day hospice instead of with the prospect that ‘I am now alone with palliative home care services and outpatient services.’ And even if it doesn’t come that way, there is a certain amount of reassurance. Because they know: ‘I have this option if I can no longer manage it’” (P31, hospital psychosocial care).
Regional Gaps in Palliative Care Services and How These Could Be Addressed by Hospice and Palliative Day Care Services
In the interviews and focus groups, participants generally agreed that both kinds of day care services could close hospice and palliative care service gaps. In particular, day hospices were perceived to provide care for patients who did not fit into other care categories (due to, eg, their young age): “And if we don’t have these day services, even for younger people, where do these people go? (…) Perhaps they are not yet ready for [inpatient] hospice care. They end up in a nursing home because the clinics usually don’t take them” (P24, municipal public administration). Moreover, spending the day with other affected persons was perceived to “protect people from social isolation” (P9, hospice home care services).
Palliative day care clinics, in contrast, were perceived to meet the need of some patients to avoid hospitalization. Managers emphasized that patients’ needs for medical, nursing and psychosocial services could be covered during a single visit, thus preventing the need for several visits to different outpatient specialists: “It is of course great when the patients come to us in the morning and can leave the house [ie palliative day care clinic] after 3, 4, a maximum of 6 hours, perhaps having received an ascites puncture, the psycho-oncologist came, blood was taken, a creative therapist came, and all this in 1 setting (...) where the patient has the feeling that he is the focus, is being understood, can take his time and can go home again on the same day” (M4, PDC). Moreover, both types of day care services were perceived to close a care gap by shortening or even preventing inpatient stays due to caregiver overburden. According to managers and network representatives, hospice and palliative day care services can support the home care situation by providing a constant point of contact for family caregivers, relieving family caregivers for several hours at a time and offering security: “Whether you [go there] once a week or 5 times a week, it’s up to you, but they don’t fall into a hole, they receive high-quality continuing care instead” (M6, DH). Additionally, hospice and palliative day care services were perceived to offer patients who have been discharged from palliative care units or do not yet meet the requirements for inpatient hospice stays a way to maintain contact and benefit from facility structures (eg medical and therapeutic services).
However, some facility outsiders estimated that the target group for which day hospices and palliative day care clinics are most suited is relatively small: “I think it’s a small need overall. (...) I think in the end the [number of] people for whom this fits (…) is minimal, [for whom] really the structure fits – that I’m taken there all day because my wife goes to work” (P25, inpatient hospice).
Ideas for Optimizing the Benefits of Hospice and Palliative Day Care Services
Facility insiders and outsiders offered suggestions for improving the services provided by day hospices and day care clinics to better meet patient and caregiver needs. Representatives from regional hospice and palliative care networks named various aspects that could contribute to needs-based care, including regular consultation hours (particularly within day care clinics), to enable more swift access to services. A resident palliative care physician referred to sporadic appointments after long wait times as “a drop in the bucket” and insufficient to serve patient needs (P14). Concerning day hospices, network representatives recommended adjusting opening hours to meet the needs of family caregivers. In particular, they felt that such measures are needed to accommodate family caregivers who work weekends. Both participant groups saw a need for further optimization of day care services to make them more responsive to patient needs: “I think it really makes sense to look at who is cared for in which day care facility and that the professionalism [ie professionals] that work there also adapt to the people who spend their days there” (M3, DH). However, a hospice home care service employee criticized the increasing differentiation into specialized forms of palliative care, as they perceived this to only benefit a relatively small proportion of patients: “Shouldn’t much more be done for the dying where most people die, namely in hospitals and nursing homes?” (P9).
The interviewed experts considered close cooperation between all hospice and palliative care providers in a network important, and recommended the integration of day care services into care plans at an early stage, in order to maximally benefit seriously ill patients. Additionally, facility insiders and outsiders suggested that patients may be more likely to draw on services from day care facilities located close to home.
Managers, in particular, saw a need for optimization with regard to the funding criteria for day care services. They claimed that, for patients to receive the most benefit, “it is important that the (…) funders also value the human aspect, not only the medical side, but also highly value the relief of the families” (M3, DH), and that the bureaucratic obstacles of applying for funding be reduced.
Discussion
The results of the 2 qualitative work packages with managers of day hospices and palliative day care clinics (ie internal perspective) and representatives from the facilities’ hospice and palliative care networks (ie external perspective) were presented with the aim of exploring the benefits provided by these facilities in Germany. The results of the focus groups suggested that, while inpatient, outpatient and home-based care services may cover the majority of hospice and palliative care needs in Germany, they may not meet all the needs of all patients. For some patients, day care clinics and day hospices may be more appropriate, as they allow them to receive multiple therapies during a single visit. Day hospices typically offer psychosocial/therapeutic treatments, while day clinics may also provide a variety of medical treatments. Due to the opportunity to bundle treatments at these facilities, there may also be less effort involved in coordinating appointments and arranging for transportation. Various studies, drawing on patient surveys, have shown that patients who make use of day care services receive significantly more social support, as well as medical, nursing and therapeutic services, relative to patients who receive only home-based care.1,10-15 This aligns with the present finding that palliative and hospice day care facilities may counteract social isolation and facilitate the bundling of multiple therapies. Bradley et al 10 even found that referrers, as well, tend to appreciate the multiprofessional teams and holistic approach provided by day hospices.
Day care facilities can meaningfully supplement the care of patients who wish to remain at home for as long as possible (and avoid inpatient admission). Additionally, the present results align with previous studies showing that day care services can fulfil the needs of family caregivers for respite and support.10,12,16-18 Specifically, such services may relieve family caregivers for several hours at a time, enabling them to provide more effective care at home and thereby supporting the home care situation.
In line with general recommendations for the integration of (specialized) palliative care,19,20 the experts interviewed in the present study emphasized the importance of the early integration of day care services. However, this suggestion is at odds with German law, which holds that palliative care may only be prescribed in the last months of life.
Strengths and Limitations of the Study
A strength of the present study lies in its inclusion of both supportive and critical external perspectives, to complement facilities’ internal perspectives. The study was also the first to examine the additional benefits provided by palliative day care clinics and day hospices in Germany. A limitation of the study is that it did not present the perspectives of patients and caregivers, themselves.
Conclusion
The results suggest that the palliative care needs of some patients are not comprehensively met by inpatient, outpatient and home-based hospice and palliative care services. Although the target population that is most likely to benefit from day care services is assumed to be relatively small, day care services may meet the individual needs of certain patient groups more effectively than other forms of care – including indirectly, by preventing caregiver overburden. While the expansion of day care facilities would thus be reasonable, such facilities should be aligned with local care structures. Future studies should examine the extent to which the use of hospice and palliative day care services may delay or prevent inpatient admissions and increase the length of time that patients are able to stay at home.
Footnotes
Acknowledgments
The authors gratefully thank all of the interviewed experts for their participation in this study. They also thank their research assistants for transcribing the interview material.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study comprised part of the project “ABPATITE – Improving health care for patients with terminal, progressive illnesses: Status and demand analysis for palliative day care clinics and day hospices and recommendations for health care planning”, financed by the German Innovation Fund of the Federal Joint Committee (G-BA) (Grant N° 01VSF19034). The funder was not involved in the study design, data collection, analysis or interpretation of study data, or the drafting of this article.
Availability of Data and Materials
The datasets analyzed in the present study are available from the corresponding author upon reasonable request.
Consent for Publication
Individual written informed consent for the research team to publish the study results was obtained from all interviewed managers and focus group participants.