
Abstract
Background
We describe two complex cases in the setting of COVID-19 at the End of Life, to enhance learning for all patients.
Case Presentation
Maintenance of sustained comfort in two cases required multiple drugs, specifically selected for symptoms that necessitated three separate pumps delivering continuous 24-hour subcutaneous infusion.
Case Management
Management of sustained comfort included opioid, midazolam, anti-secretory, diclofenac for intractable temperature, phenobarbital for extreme agitation, in one, where seizure activity was present, while insomnia, was a prominent feature of another. Management of Akatasia was also required.
Case Outcome
Attention to each individual patient’s rapidly evolving symptoms, during the dying phase, with a thorough differential diagnosis, wa s vitally important in the context of a ‘Good Death’. This was achieved in both cases, reflected by evidence at the bedside of comfort and a minimum need for ‘as required’ drugs in the last days of life.
Conclusions
COVID-19 being a new illness, we need to prospectively study the symptom burden/clustering at End of Life and learn from management of this new disease for other illnesses also. Further research is required to develop protocols on; when does Midazolam dose reach tolerance and when should an alternative drug such as phenobarbital for sustained Gamma-Aminobutyric Acid effects be initiated; examine the optimal approach to sustained temperature control; be cognisant of extrapyramidal side effects of drugs used at End of Life and consider looking at a lack of need for ‘as required’ drugs in the last days of life as an outcome measure of sustained comfort.
Background
Agitation and delirium are common in COVID-19 infection, particularly in the severely ill, and those requiring Palliative Care.1–3 Recommendations exist for the management of delirium in patients with COVID-19, with prevention and environmental management remaining a cornerstone of delirium care. 4 If disease is thought to be reversible, particular care should be taken with medications that have an associated risk of respiratory depression, including opioids and benzodiazepines.4,5 In End of Life (EoL) care, however, these medications may be warranted and perspectives from several countries have acknowledged the role of midazolam as first line for management of agitation in COVID-19.4–6 In severe cases of agitation, however, midazolam may not prove fully efficacious. 6 Recognition of precipitants and further treatment options are of paramount importance if severe agitation occurs during COVID-19 infection requiring EoL Care. 1
We present two cases of severe agitation and other complex symptom burden, in the setting of COVID-19 and EoL Care, and discuss their management from a specialist Palliative Care perspective.
Case Descriptions
Case 1
Drugs used in last 5 days of Life.
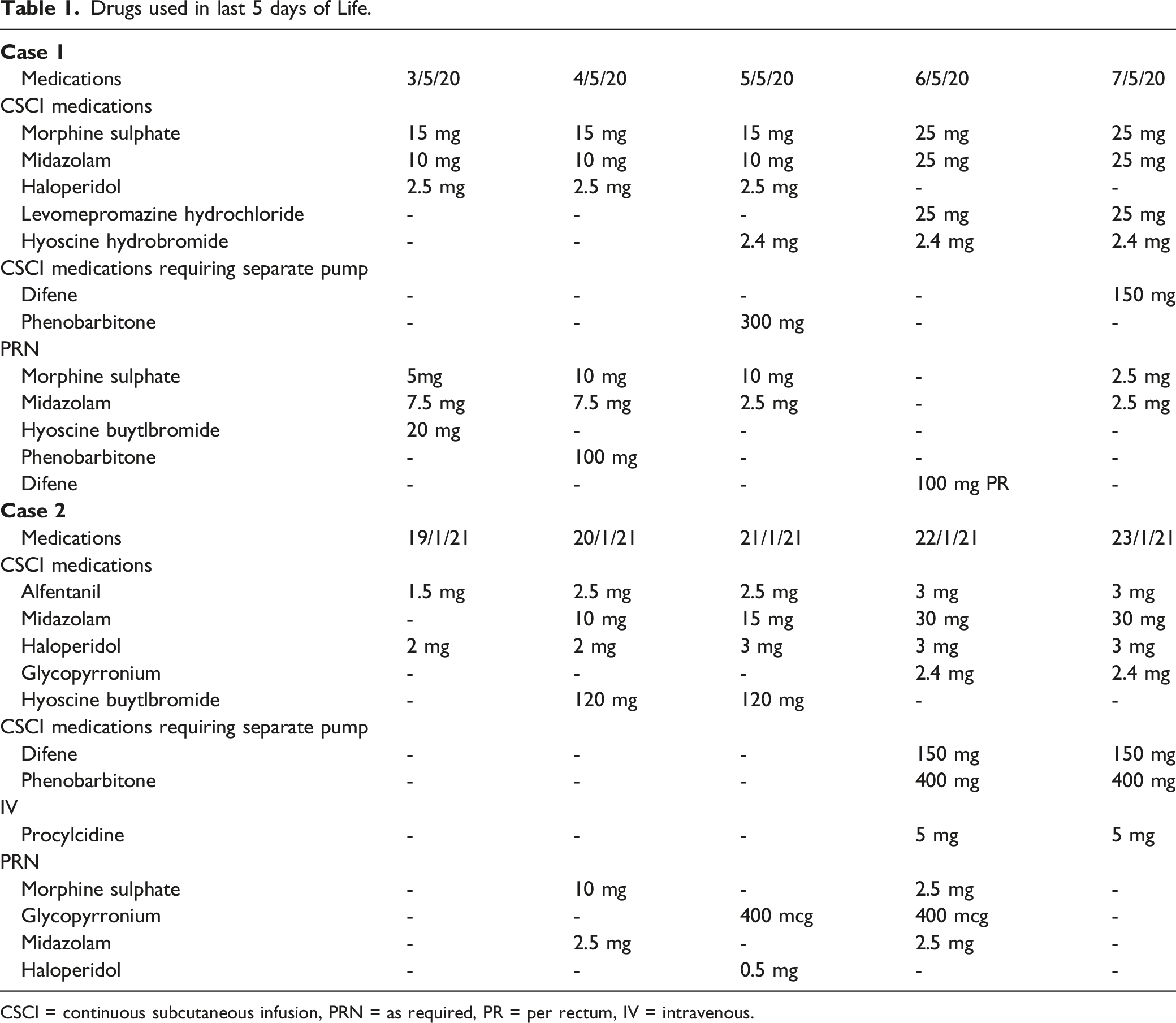
CSCI = continuous subcutaneous infusion, PRN = as required, PR = per rectum, IV = intravenous.
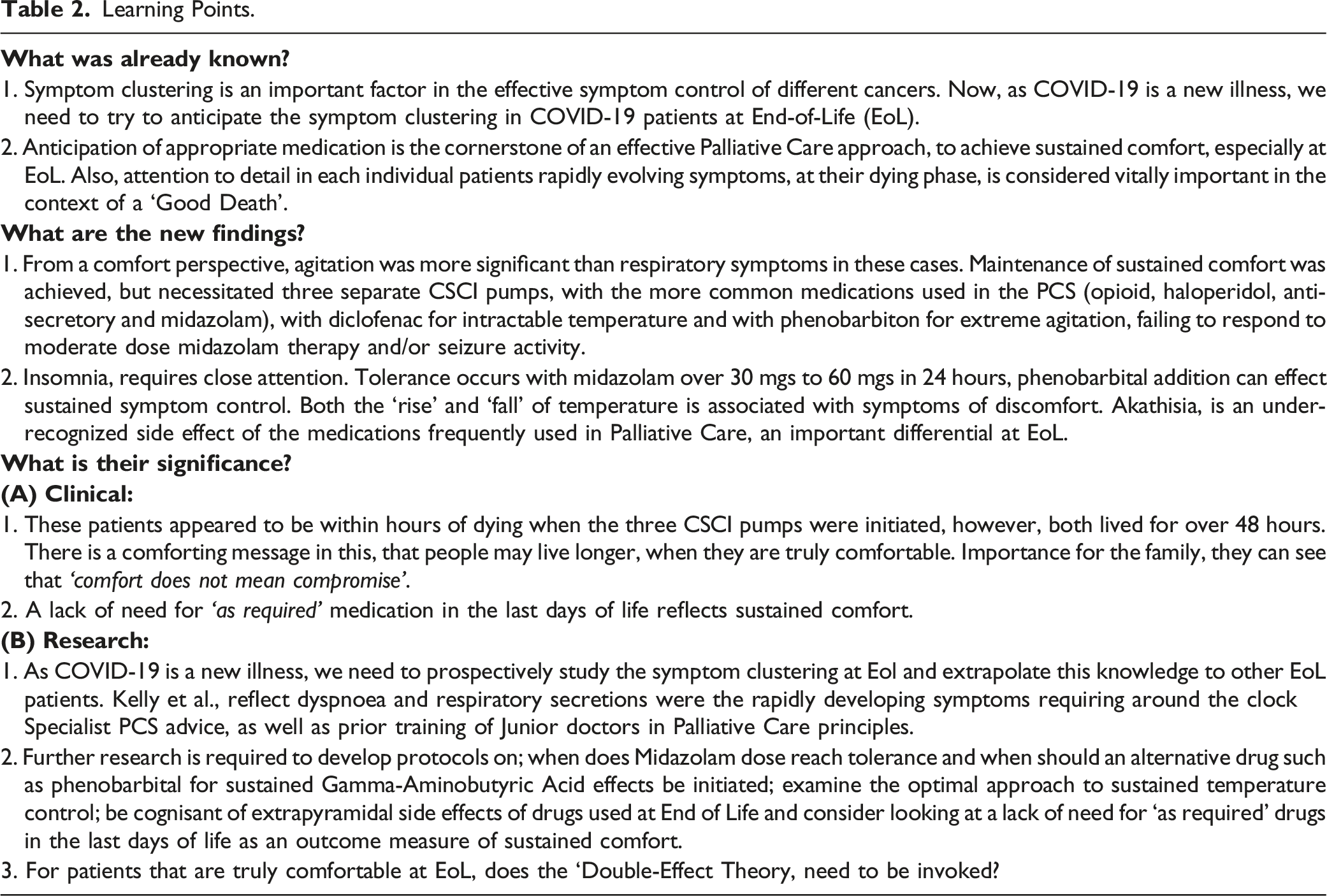
Learning Points.
Case 2
A 73 year old female patient with multiple co-morbidities; Ischaemic heart disease (Coronary Artery Bypass Graft in 2008, Non ST Elevation Myocardial Infarction in 2017); Mechanical Aortic Valve Replacement; Type 2 Diabetes; Dyslipidaemia: Chronic Obstructive Airways Disease; Gout; Fibromyalgia; Depression; Hypothyroidism; Triple Negative Breast Cancer 2020; Osteoporosis; Fracture right distal Radius 2017; Unstable Gastrointestinal Bleed 2020 rendering her unfit for Mastectomy and/or Chemotherapy, was admitted to Hospital unwell at home for 2 days with shortness of breath, fatigue and diagnosed with a chest infection. During this admission, the chest infection was being managed for medical reversibility, however unfortunately she contracted COVID-19. Prior to this nosocomial infection, the patient had been on a CSCI for symptom management for three days, which included Alfentanil, Haloperidol and Midazolam. Opioid and midazolam were for respiratory effort and general distress. The Haloperidol dose was 2 mgs S/C over 24 hours and was prescribed for delirium felt to be associated with the chest infection. The question of a trial of steroids was considered, however, this was not given as it could have aggravated her delirium and could potentially reactivate her previous significant gastrointestinal bleed. 7 During the course of her infection, she was recognised to be actively dying, her CSCI was increased and she was referred to the PCS. Her symptoms proved difficult to manage in the days before PCS review, receiving Morphine Sulphate 2.5 mgs twice S/C and Midazolam 2.5 mgs twice S/C three days before PCS review, with limited effect. She had no PRN drugs two days before PCS review and the day before PCS review, she received Morphine Sulphate 2.5 mgs four times S/C, Midazolam 2.5 mgs S/C once as well as Glycopyrronium 0.6 mgs S/C once, all with limited effect. While respiratory symptoms and secretions were controlled, she appeared to be intermittently agitated and in distress. Normal causes of distress were ruled out: pain, increased respiratory effort, full bladder, constipation and meningism. She was experiencing episodes of apparent rhythmic movement that, on occasion, were associated with pyrexia. These were thought to potentially represent either atypical seizure episodes or rigors by the primary team. On the day of PCS review, significant dose midazolam and paracetamol, however, failed to control these symptoms. Following review, she was commenced on phenobarbital and diclofenac in two separate CSCI, (Table 2). Phenobarbital was prescribed to cover seizure-like activity and diclofenac to help keep the temperature from rising. As the movements were also considered to possibly represent an extrapyramidal side effect ie akathisia associated with increased doses and sustained need for Haloperidol, intravenous (IV) Procyclidine 5 mgs, (an anticholinergic drug used in our service for over two decades to help reverse the symptoms of akathisia) was also administered.8,9 As the patient required ongoing Haloperidol, the Procyclidine was continued at 5 mgs IV daily until death. These interventions vastly improved symptoms, with the patient remaining comfortable and the abnormal movements, agitation and pyrexia settling within hours of their institution. She passed away peacefully in hospital a few days later, requiring no further PRN medications, after commencement of Diclofenac, Phenobarbital and Procyclidine.
Discussion
We describe two complex cases of PCS management in the setting of COVID-19 at EoL. Maintenance of sustained comfort was achieved, but necessitated three separate CSCI, pumps, one with the more common medications (opioid, haloperidol, anti-secretory and midazolam) one with diclofenac for intractable temperature and one with phenobarbital for extreme agitation, one in which timing of suffering from insomnia urgently required comfort, one with possible seizure activity and failing to respond to midazolam therapy.
In the first case, severe insomnia was experienced following COVID-19 infection. This became so overwhelming that it caused almost psychotic agitation. Insomnia, even as an isolated symptom, requires close attention.2,3,10 This symptom did not respond at all, even temporarily to PRN doses of midazolam, but dramatically improved with the addition of phenobarbital. This case also reflects the difficulty, very early in the Covid-19 pandemic, to understand the full complexity of the patients case, while providing advice by phone over a weekend on-call. The very helpful involvement of an Oncology Clinical Nurse Specialist, who was the only visitor allowed, was reassuring to aid proper decision making. Similarly, in the second case, the addition of phenobarbitone was associated with sustained symptomatic improvement. Midazolam acts by direct activation of gamma-aminobutyric acid (GABA). Known as the ‘brakes of the brain’, GABA mediates inhibitory functions, leading to anxiolytic, sedative, muscle relaxant and anti-convulsant actions. Tolerance has been shown with doses of midazolam over 30-60 mgs S/C in 24 hours, therefore, addition of another agent, can effect speedy and sustained symptom control. 11 As phenobarbital is a very effective antiepileptic, it’s use ensured control of any seizure activity as well as relaxing the patient.
Phenobarbital is a long-acting barbiturate with sedative, hypnotic, and anticonvulsant properties, and is indicated in EoL Care in the setting of severe and overwhelming agitation, as a third line agent.12–15 Phenobarbital acts by prolonging and potentiating the action of GABA on GABAA receptors and, at higher concentrations, directly activating receptors. 16 Phenobarbital is one of the longest-acting barbiturates available, and remains in the body for 2-7 days. Hence, for first case, the lack of availability of the drug over a long weekend was, fortunately, not problematic. Phenobarbital should be administered in a separate syringe driver to other medications, as it is oily and does not mix with other drugs and significant interindividual variations in pharmacokinetics and pharmacodynamics should be taken into account. 16 In both cases, the patients lived longer than expected after phenobarbital infusion was commenced. Comfort appeared to be a main factor in both patients living for days, rather than the originally clinically expected death within hours.
Both cases also describe the effective use of subcutaneous diclofenac for intractable pyrexia in COVID-19. If paracetamol is not achieving full control of hyperpyrexia, the addition of a non-steroidal anti-inflammatory (NSAID) is essential to achieve sustained comfort. Both the temperature ‘rise’ and ‘fall’ is associated with symptoms of discomfort. 17 The only NSAID studied in a CSCI pump is diclofenac. Diclofenac, therefore, should also be prescribed as an anticipatory drug, in case of need. If needed for pyrexia as well as paracetamol, this in our service, indicates that regular diclofenac should be prescribed, to ensure all steps are taken to keep the temperature down. For patients with potential risks from diclofenac, then the benefits are weighed against the risks for each individual patient.
Akathisia is also described in one case, which is an under-recognized side effect of the antiemetic and antipsychotic medications frequently used in Palliative Care. It is broadly defined as a subjective sense of restlessness which onsets after Dopamine D2 receptor blockade and involvement of serotonergic mechanisms in the pathophysiology of akathisia is now well recognised.9,18 Treatment options are drugs that influence relevant neurotransmitter functions, like anticholinergics, beta-blockers and benzodiazepines. 9 Our service has used anticholinergics for over two decades, with benefit. As our Pharmacy has the anticholinergic, Procyclidine, this is the one used in the second case, at a dose of 5 mgs IV daily. If we can stop the culprit drug, this is only used once. It occurs as part of the wider group of extra-pyramidal side-effects. Diagnosis of akathisia is challenging due to the wide variation in symptoms experienced, as well as the potential for misdiagnosis; existential anxiety, agitation, terminal delirium, restless leg syndrome or drug withdrawal. Our second case outlines the importance of a high clinical suspicion for akathisia. The symptom can be difficult to assess and easily missed, usually occurring after day 10 on culprit drug. It may be a source of significant discomfort for the patient and is very important to out-rule when the patient is unconscious. 18 A high index of suspicion should, therefore, be applied in the setting of agitation and recently established or increased antipsychotic/anti-emetic treatment. Once recognized, it appears to respond effectively and rapidly to treatment with IV anti-cholinergic medications. Recognition of akathisia remains a challenge and, in the future, it may be possible that physician countertransference could be used as a tool for recognition, as it has been for identification of patients with depression among the Palliative Cohort. 19 Another important and rare side effect to be aware of at EoL is agitation secondary to hyoscine hydrobromide, sometimes used for extreme chest secretions. 20
Symptom clustering is an important factor in the effective symptom control of different cancers. 21 Given that COVID-19 is a new illness, we need to try to anticipate the symptom clustering/bother at Eol.22,23 Kelly et al, report on dyspnoea and respiratory secretions as the rapidly developing symptoms requiring urgent Specialist PCS advice, as well as prior training of junior doctors in Palliative Care principles. 24 A request was also sent out to all our hospital service Pharmacies to insure phenobarbital was in stock, early in the Covid-19 pandemic. A hospital policy was written with the rationale for use of phenobarbital, but its use was reserved for prescribing by the PCS consultants, as it is not a commonly used drug in other areas of medicine.
Sustained comfort is the cornerstone of a good, dignified dying process. One reliable outcome factor to confirm that this has been achieved is that the patient did not require multiple PRN medications at EoL. For both of these patients, sustained comfort was achieved as excessive PRN medications were not needed in the last 48 hours of life. There is a comforting message that people may live longer, when they are truly comfortable. The ‘Double-Effect Theory, ie“permissibility of an action that causes a serious harm, such as the death of a human being, as a side effect of promoting some good end”, did not, therefore, need to be invoked. 25 This factor has importance for the family, they can see that ‘comfort does not mean compromise’. Considering the inability to spend time with their loved one, due to COVID-19 strict protocols, limited time with their loved one, if any time at all, the knowledge that comfort has, indeed, been achieved is invaluable. In both cases, family members wearing full personal protective equipment were allowed to visit for short periods during the EoL phase.
David Shore quotes, “Confidence and trust is an intricate component of achieving good outcomes for patients”. 26 The illness trajectory of this patient cohort with COVID-19 is such that many patients are at EoL by the time of referral to the Hospital Specialist PCS, resulting in a short duration of the team’s involvement. The priority, therefore, is effective, rapid symptom control, awareness of each individual’s quality of dying, with the capacity to respond around-the-clock to rapidly escalating symptomatology, while being mindful to minimise the transmission of the virus to other vulnerable patients and staff.
Footnotes
Acknowledgment
Thanks to the generous donation of the Mayo/Roscommon Hospice Foundation for kindly funding free access to all to the full content of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.