
Abstract
Background
Communication is one of the central axes around which end-of-life care revolves in the context of palliative care. Communication of bad news is reported as one of the most difficult and stressful tasks by palliative care professionals. Therefore, the aim of this study is to identify aspects related to the communication of bad news in palliative care in Spain.
Methods
Descriptive cross-sectional study. An ad hoc questionnaire was designed and sent by e-mail to all palliative care teams in Spain.
Results
Overall, 206 professionals (102 nurses, 88 physicians and 16 psychologists) completed the questionnaire. A total of 60.2% considered their communication of bad news skills to be good or very good. This was related to older age, experience in both the profession and palliative care, and to having received specific postgraduate training (P < .001). Around 42.2% perform communication of bad news with the patient first, which is associated with lower skill (P = .013). About 78.15% of the professionals do not use any specific protocol.
Conclusion
This study suggests that patients access palliative care with little information about their diagnosis and prognosis. The barriers identified in the communication of bad news are the lack of specific education and training in protocol management, the difficult balance between hope and honesty, the young age of the patient, and the family.
Keywords
Introduction
In the context of illness and end-of- life, palliative care (PC) professionals are in permanent contact with death, as well as with patients and families who are suffering. In addition to the emotional burden that caring for this type of patient can entail for the professionals themselves, it involves handling complex situations in daily practice that often involve an ethical dilemma. 1
Several studies concur that the difficulty in communicating bad news (CBN), especially when it involves the revelation of a diagnosis of a terminal disease or an unfavorable prognosis, is one of the most relevant ethical aspects in PC, and one of the most stressful for professionals.2,3
Bad news is understood as any information that negatively affects the patient’s expectations of themselves or their future. It entails the perception of a physical or mental threat and the risk of being overwhelmed by the patient’s own ability to cope with it. 4 In the setting of PC, this may include information about diagnosis, prognosis, the futility of treatment, or treatment withdrawal, among other things.
Communication is one of the central axes around which end-of-life care revolves. 5 In fact, it is considered the basis of the relationship between professional, patient and family. 6 A great deal of research underlines the importance of effective communication and its positive impact on the palliative patient and their environment. 7 In our setting, a study carried out in Granada, Spain, among patients admitted to a PC unit, showed that patients who were fully informed of their diagnosis and prognosis maintained more fluid communication than those who were not, or only partially, informed. 8
The CBN and, in general, communication in an end-of-life setting is reported as one of the most difficult and stressful tasks by PC professionals. 9 The most important barriers for effective CBN include intrinsic factors related to the physicians, patient-related factors, and institutional factors such as the lack of specific protocols or training. Moreover, the lack of skills to develop honest and effective communication around death is an aspect recurrently reported in the literature.10-12
As a result, professionals are striving to develop strategies to improve this communication. Starting conversations about everything surrounding death early on, providing information on an ongoing basis, offering hope in the face of life-threatening illness, and adapting the content of the message to the patient’s ability to understand, are some of the strategies that increase the effectiveness of communication. 13
The CBN requires a comprehensive approach, skills, and knowledge by the professional involved. Different protocols or clinical practice guidelines have been developed to help professionals with this task.11,14,15 In the field of PC, perhaps the most widely used protocol is the one known as SPIKES. 16 It is developed in 6 stages that must be followed in sequence: Setting, Perception, Invitation, Knowledge, Empathy, Strategy and Summary. Another of the most frequently referenced protocols is Rabow and McPhec’s ABCDE. 17 Similar to the previous one, it proposes a CBN using 5 steps: Advance preparation; Build a therapeutic environment/relationship; Communicate well; Deal with patient and family reactions; Encourage and validate emotions.
In our Mediterranean cultural environment, the literature reporting on the way in which PC professionals communicate bad news is scarce. This study aims to delve into this aspect, showing a vision at the national level, to provide a cultural and anthropological view of existing studies. Therefore, the objectives of the study are to find out and identify aspects related to the communication of bad news in PC; to determine the level of knowledge about the diagnosis and prognosis of patients at the time of access to PC; and to identify the use of specific protocols for the communication of bad news.
Methods
Study Design
To achieve the proposed objectives, a descriptive cross-sectional study was designed. An ad hoc questionnaire was developed (due to the lack of validated scales in the communication of bad news) and sent by e-mail to all the PC teams in Spain included in the latest directory of PC resources published by the Spanish Society for Palliative Care in 2016. Beforehand, the questionnaire was reviewed by five external PC experts (two physicians, two nurses and one psychologist; all working in PC units and with more than 10 years of experience in the field) to ensure its adequacy and comprehensibility. The questionnaire used in this study was designed to collect, in addition to a series of sociodemographic data, aspects involved in CBN related to both the patient and the professional, from the perspective of the latter.
A research proposal was presented and, after evaluation of ethical aspects, was approved by the Ethics Committee of the Comillas Pontifical University on June 5, 2021.
All information related to the study has been treated as strictly confidential and in accordance with European Regulation 2016/679 of April 27, 2016, and the Spanish Ley Orgánica 3/2018, of December 5, on Personal Data Protection and guarantee of digital rights, as well as the Biomedical Research Law 14/2007 and its 2016 update.
Subjects
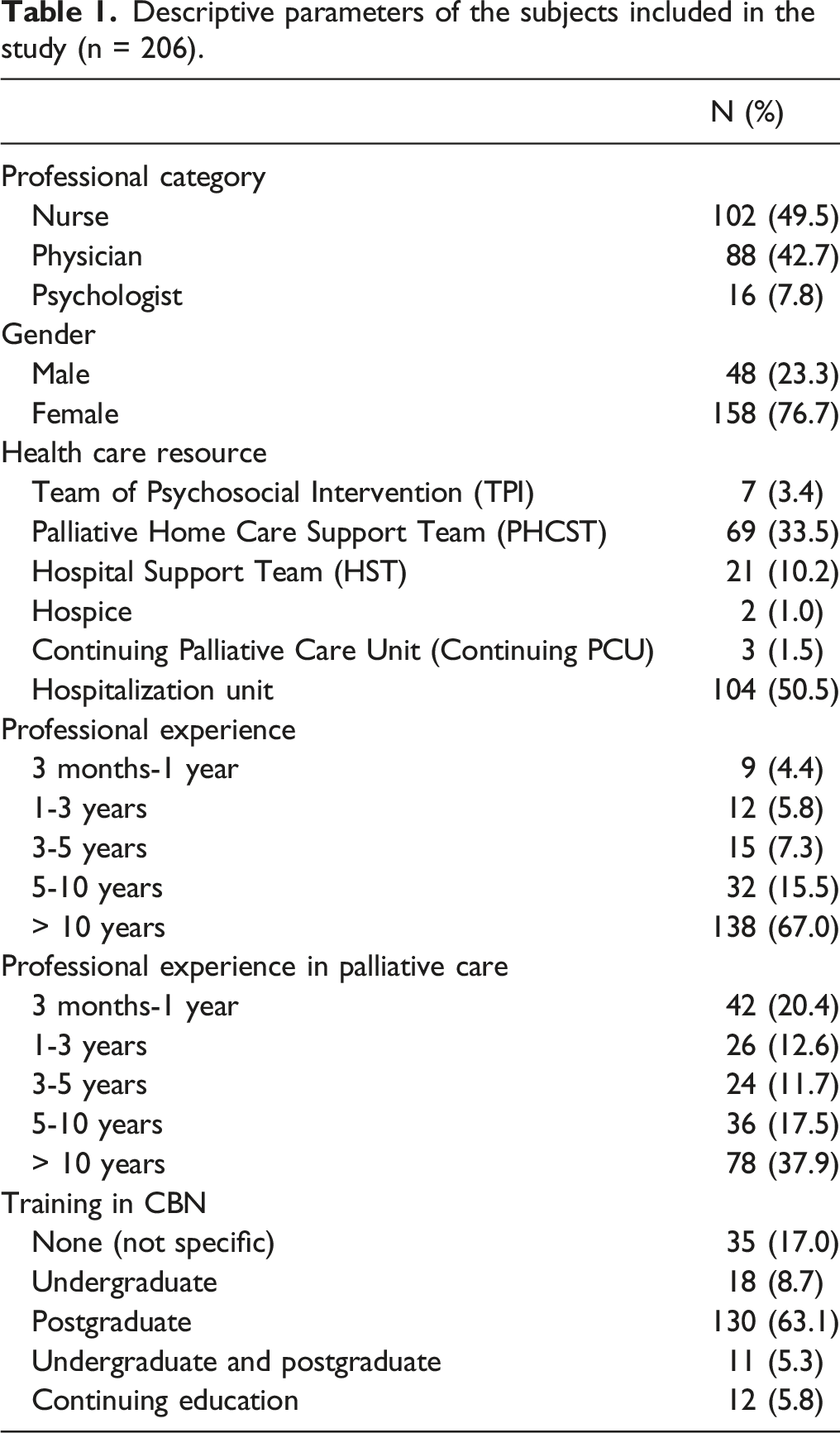
Descriptive parameters of the subjects included in the study (n = 206).
Data Analysis
A descriptive analysis of the data was performed for quantitative variables including mean, median, and standard deviation (SD); and for categorical variables, absolute and relative frequencies.
Subsequently, an inferential analysis was performed to see the differences between the different professionals and the correlation with the different variables in the study. Correlations or associations between variables were sought using Pearson’s or Spearman’s correlation coefficients depending on the normality of the quantitative variables contrasted, or the Chi-square or Fisher’s exact test for categorical variables. In the case of ordinal qualitative variables, the one-way ANOVA or Kruskal-Wallis test was applied. The distribution of the quantitative variables analyzed was tested using the Kolmogorov-Smirnov test. The differences found in the bivariate statistics were considered statistically significant for a value of P < .05.
Microsoft Forms (2016) was used in the development of the questionnaire, and the data obtained in the assessments were transferred to a Microsoft Excel database (MS Excel. Version 16.20. Redmond, WA: Microsoft Corp.) and once refined, for final analysis, put through the statistical program SPSS® for Windows®, version 24.0 (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.).
Results
A total of 206 valid questionnaires were collected, of which 52.9% were completed by professionals working in the Community of Madrid and 15% in the Autonomous Community of Andalucía. The rest of the questionnaires were distributed evenly among the other autonomous communities of Spain. The mean age of the participants was 42.7 (SD 11.3) years, 76.7% being women.
A complete report of the questionnaire and results are shown in Table 2.
Regarding the distribution of the sample by professional category, 49.5% were nurses and 42.7% were physicians. Slightly more than half (50.5%) worked in inpatient PC units, while 33.5% worked in home teams and 10.2% in hospital support teams. 100% of the psychologists in the sample belonged to psychosocial care teams. Professional experience was greater than 10 years in 67% of the cases, although this same professional experience in the specific field of PC was only attained by 37.9% of the sample. While 74.2% of the subjects had received specific training in bad news communication through postgraduate or continuing education programs, in only 16.8% of the cases had this training been promoted and financed by the institution for which they worked.
If we consider the level of information with which patients access PC, in relation to their pathology, the professionals consider that the best-informed patients which access PC are oncology patients, while the geriatric patients are less informed. Specifically, in the opinion of the professionals, only 1.5% of patients access PC fully informed of their diagnosis and .5% of their prognosis. This contrasts with the high percentage of patients, 69.9%, who, according to the experience of the professionals, often or very often ask to be informed, even if it is bad news. In the case of the family/primary caregiver, complete information about the diagnosis is given in only 1%, and the prognosis in 1.5% of cases at the time of accessing PC. In addition, in 62.6% of the questionnaires, we found that the family was opposed to the patient being informed.
Descriptive Analysis of the Questionnaire items by professional category (n = 206).
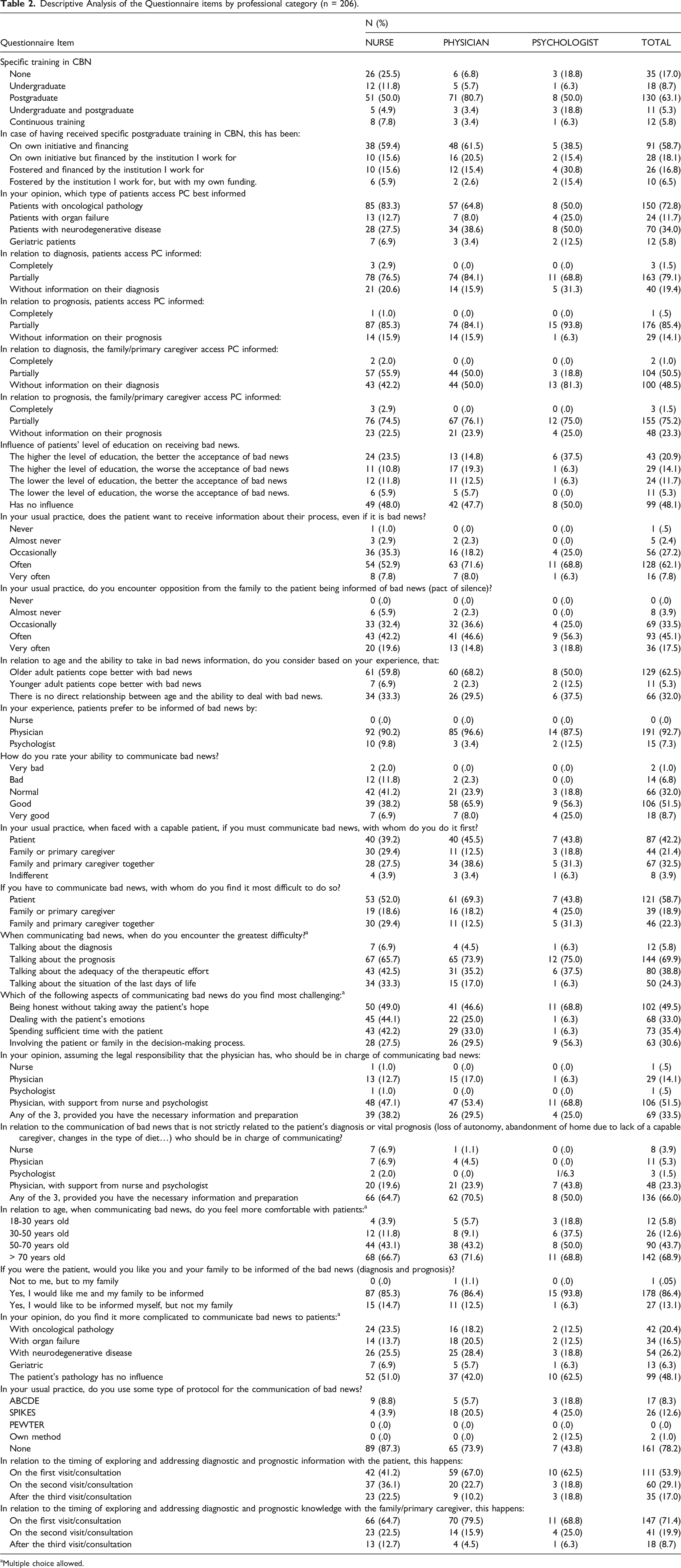
aMultiple choice allowed.
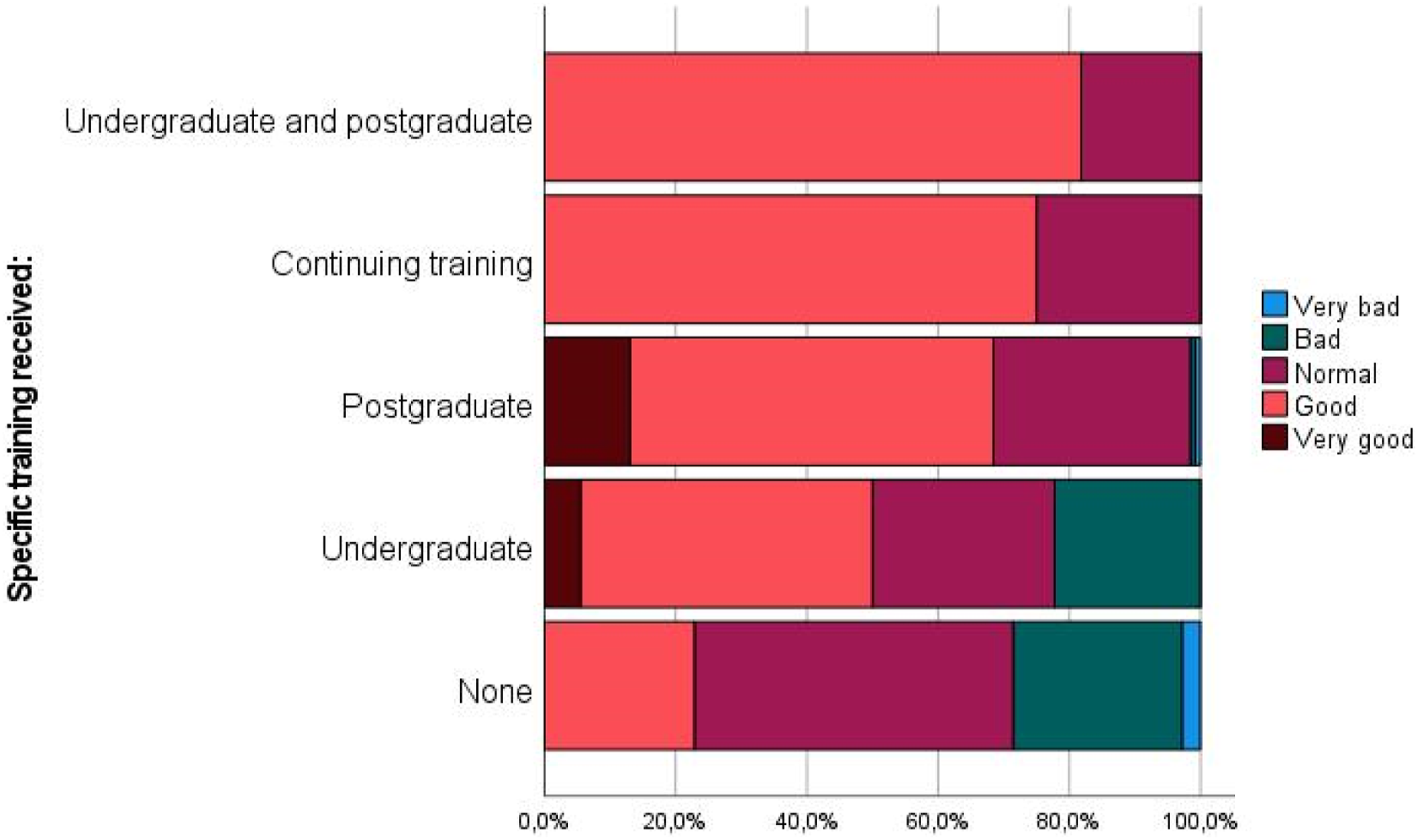
Relationship between CBN skill (Likert 1 - very bad; 2 - bad; 3 - normal; 4 - good; 5 - very good) and specific training received. Kruskall Wallis test showing statistical significance between none-continuing education (P = .002), none-postgraduate (P < .001), none-undergraduate and postgraduate (P < .001), and undergraduate-postgraduate (P = .035).
Although, in the opinion of the professionals, patients prefer to be informed by the physician in 92.7% of cases, only 14.1% consider that the physician should be the only one to inform the patient. If the communication of bad news is not strictly related to the patient’s diagnosis and/or prognosis, this percentage drops to 5.3%. The communication of bad news is considered as more difficult if it is with the patient (58.7%), and if it is related to the prognosis (69.9%). In contrast, 94.2% of the professionals do not find it difficult to talk about the diagnosis. As for other aspects of CBN, the most difficult aspect is perceived as being honest without taking away the patient’s hope (49.5%). The least difficult aspect is perceived as involving the patient or family in the decision-making process, which is referred to as a difficult aspect in 30.6% of the cases.
If they must communicate bad news about the process of the disease, 42.2% of the participating subjects communicate it first with the patient themselves, 32.5% communicate it to patient and family at the same time, and 21.4% communicate it first to the family or main caregiver. Within the group of subjects who have not received postgraduate training, if we consider the relationship between the skill expressed for CBN and to whom they communicate first, we find significant differences between a lower skill and communicating first to the family (P = .013), or jointly with the patient and family (P = .011). This does not occur among those who received postgraduate training (P = .437).
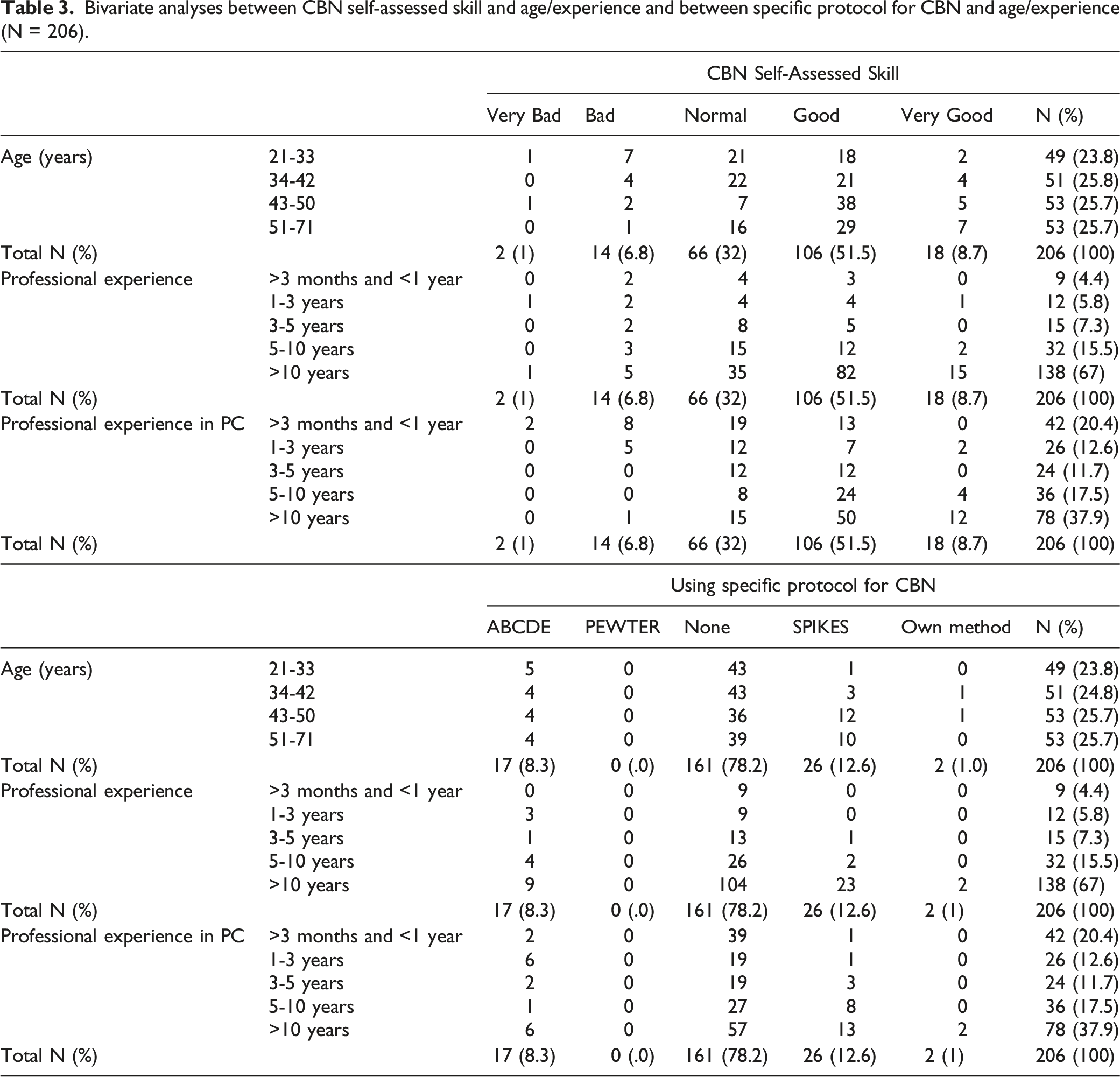
Bivariate analyses between CBN self-assessed skill and age/experience and between specific protocol for CBN and age/experience (N = 206).
Discussion
Overall, 206 professionals completed the questionnaire and the main results are discussed below. A total of 60.2% considered their CBN skills to be good or very good. This was related to older age, experience in both the profession and in PC, and to having received specific postgraduate training. Around 42.2% perform CBN with the patient first, which is associated with lower skill. Approximately 1.5% of patients access PC fully informed of their diagnosis and .5% of their prognosis according to feedback from professionals. Within CBN, 69.9% of the professionals find it more difficult to discuss prognosis. About 78.1% of the professionals do not use any specific protocol for CBN. The use of protocol is associated with greater skill for CBN and with having greater experience in the specific field of PC.
Training appears to be a key element in CBN. However, the percentage of professionals in the sample who received training in this area as part of their university degree is very low. Although there is a consensus in the literature on the need to incorporate communication techniques in the training of health professionals, this is still a pending issue. 18 The data of the professionals in our sample who received undergraduate training in CBN do not differ from those reported in studies of similar characteristics.19-21 A high percentage of the sample reported having received postgraduate training in CBN, generally on their own initiative and with their own funding. This training correlates significantly with improved communication skills. Many studies have shown significant progress in this regard following the development of specific training activities.22,23 An experimental study carried out among Iranian nurses concluded that there were significant differences between the control group and the experimental group after the implementation of a course in communication skills. The improvement not only affected the skill, but also their involvement in the CBN process. 24
Sixty-eight percent of the subjects in the sample considered their CBN skills to be good or very good. Similarly, 68.3% of a sample of different health professionals in a study by Attivissimo et al. 20 reported having good or very good skills after having undergone a training program on CBN in patients with advanced disease. Slightly higher (82%) is the percentage of 226 physicians, mostly internists or oncologists, from Italian university hospitals who claimed to have good or very good skills in CBN. Although only 9% had received specific training, more than half reported having acquired skills through their own experience and/or observation of other colleagues. 21 In this sense, our results reflect that skill is also positively correlated with experience.
Even though it is the patient, those with the capacity to do so, who should be informed first and foremost, and it should be the patient who consents to this information being shared with those close to them, the percentage of professionals who prioritize CBN with the family can be considered high, as in the study by Ichikura et al. 25 on more than 1200 hospitals with oncology and PC services. According to the questionnaire, the professionals reported feeling more comfortable if CBN is with the family, and this perception is related to a lower ability to perform CBN.
Previous studies have shown that CBN is one of the most complex and stressful aspects of clinical practice for professionals.2,3,25,26 However, the results obtained suggest important differences between communication regarding diagnosis and prognosis. Only 5.8% reported difficulty when talking about diagnosis, while discussions about prognosis were reported as difficult by 69.9% of the sample. Despite the benefit it provides to patients, 27 sharing prognostic conversations by professionals to a lesser extent seems to be a universalized aspect. 28 Within CBN, being honest without taking hope away from the patient is perceived as the most complicated part both in our sample and in previous studies.16,20,21 The results show that the difficulty increases as the patient’s age decreases. In a study carried out in the United Kingdom, patient age was also reported as a stressor factor at the time of CBN by oncology nurses. 29
As reported by the clinician respondents, about 69.9% of patients show frequent or very frequent interest in receiving information about their process, despite the fact that it is bad news. The willingness of patients to discuss their prognosis has already been reported in the literature.30,31 A recent systematic review of 41 articles relating to a cumulative population of more than 27,000 patients concluded that, on average, 61% of patients were willing to discuss their prognosis. 32 Despite this, the percentage of patients who are fully aware of their diagnosis and prognosis is very low. This differs from other studies in which this knowledge is higher. Similarly, different studies carried out in recent years in our setting quantify the percentage of well-informed patients as much higher. Heterogeneity in the methodology and time of collection of the variable, as well as differences between the perception of the patient and the professional, may be the reason for the difference in results.33,34 In contrast to the patient’s desire to be informed, we found a large number of professionals who reported finding opposition on the part of the family when it came to maintaining CBN with the patient. It is common for the family to protect the patient, and to be reluctant to receive information related to end-of-life. 35
The use of specific protocols for CBN is recommended in the literature. 36 However, their use by our sample is very scarce. Nevertheless, these results are in line with those obtained by Attivisimo et al. 20 and Messerotti et al. 21 where the use of strategies for CBN is used by 23.5% and 38% of the sample, respectively. Despite this, in both studies, most of the participating professionals stated that the use of a specific protocol would be very useful for them.20,21 This low rate of protocol use is also reflected in a recent review that included 86 studies on communication and PC. 37 While the lack of specific guidelines is one of the reasons reported by practitioners for poor CBN,35,38 there are an increasing number of guidelines and protocols available to practitioners. 39 This suggests that the real problem is not the absence of guidelines, but possibly a lack of training in their use. In our sample, a greater ability for CBN and a greater degree of professional experience were related to a greater use of protocols, a finding that would support this assumption.
Limitations
Several actors are involved in the communication of bad news, mainly the health professional and the patient. This study was aimed at health professionals in the field of palliative care, so only a partial view of reality was obtained. It would be desirable also to consider the perception of patients and their families, thereby sharing experience and jointly defining ideal CBN protocols. Therefore, the internal validity of the study may be affected by possible information and/or selection biases. Internal validity may also have been affected by the response rates and self-selection of those who chose to answer the questionnaire. In addition, external validity is affected because we did not reach the estimated sample size. Therefore, the data are not extrapolable to the target population, and studies are needed to expand the sample.
Conclusions
The results of this study suggest that patients access PC with little information about their diagnosis and prognosis, with conversations about the latter being the most difficult for professionals to deal with in dialogue with the patient. The barriers identified in CBN are the lack of specific education and training in protocol management, the difficult balance between hope and honesty, the young age of the patient, and the family. Professionals report having good CBN skills, but the use of protocols is very scarce.
Footnotes
Acknowledgments
We would like to thank Belén Martinez Cruz, Mónica Dones Sánchez, Roberto Alvarez Álvarez, Diego Ruiz López and Jaime Boceta Osuna for their contribution to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.