
Abstract
Introduction
The majority of patients with cancer receive antimicrobials during terminal admissions, in palliative care units, and at the time surrounding death—even in the absence of infection.1-8 In fact, one systematic review reported that more than 50% of patients with advanced cancer at the end of life (EOL) received antimicrobials (n = 15 studies). 2 Prophylactic and empiric antimicrobial use is common in cancer patients due to immunocompromised states and resultant non-specific signs of infection. Although antimicrobial stewardship programs (ASPs) identify EOL antimicrobial use as aggressive care, 9 appropriate practice guidelines are lacking. 10
Predictors of EOL antimicrobial use are multifactorial and may include: insufficient prescriber knowledge of benefits and risks, a desire to respect patient or surrogate decisions, and beliefs that antimicrobials are less invasive than other therapies or that they palliate symptoms.11-13 To our knowledge, there is no high-level evidence to support antimicrobial use for relief of distressing symptoms, with the exception of pain secondary to urinary tract infection at EOL (prescriptive use poorly defined).3,4,14-16 Furthermore, when a patient’s prognosis is estimated as weeks-to-months, there is little data to support survival benefits,5,17 and conversely, continued use for those imminently dying may hasten death. 16
Frequent and long-term use of broad-spectrum antimicrobials at the EOL can cause adverse drug events (e.g., diarrhea, end-organ toxic effects, venous access complications, infection control consequences).18-21 Antimicrobial resistance is problematic among patients with foreign devices such as urinary catheters or central access lines, both frequently used at the EOL. 22 Antimicrobials can also increase the administration of unnecessary invasive testing, such as blood cultures or radiological imaging.4,23,24 EOL antimicrobial use is associated with longer hospital length of stays, barriers to accessing community-based or hospice services, and myriad other clinician and financial costs to patients and health organizations.4,24-27
The absence of consistent guidelines for antimicrobial stewardship in cancer patients at EOL leads to prescriber variation. Examining the covariates of EOL antimicrobial use may support the development of training and clinical interventions to promote evidence-based practice, prevent avoidable harm, and reduce unnecessary spending while enhancing goal-concordant EOL care. The purpose of this study is to understand disease characteristics and specific factors associated with antimicrobial use in the last 7 days of life among hospitalized patients with solid tumor cancers.
Methods
Design
We used a retrospective cohort design and included adult patients (age ≥18) with solid tumors admitted to non-intensive care unit (ICU) inpatient services who died during an admission longer than 3 days. Patients admitted to a solid tumor service and subsequently transferred to the ICU during the same admission were included. All hematologic malignancies and bone marrow transplants were excluded given the immunosuppressive nature of the illnesses and treatment. All admissions occurred between January 1, 2019, and December 31, 2019, at a highly specialized tertiary cancer center hospital in New York. Our Institutional Review Board approved this study prior to data collection (#21-408).
Data Collection
Electronic medical records (EMRs) were used to identify and classify patients who received and did not receive antimicrobials in the last seven days of life. Data was limited to the last seven days of life and included demographic information, prescriptions, clinical notes, pathology reports, and diagnostic tests. We excluded antimicrobials administered via inhalation or ear, eye, or topical application, as well as prophylactically dosed acyclovir and sulfamethoxazole. Clinical notes, orders, pathology reports, the Surveillance, Epidemiology, and End Results (SEER) Program, and International Classification of Disease (ICD)-10 codes were used to identify cancer types.28,29
We collected “do not resuscitate” (DNR) orders; rapid response team activations; and palliative care, infectious disease, or ICU consultations. All outpatient orders prior to admission and pre-existing foreign devices (e.g., urinary catheter, central venous catheter, or mechanical ventilation) placed in the community were excluded. EOL care orders were defined by use of an EOL order set. A templated “goals of care” discussion note in the EMR, implemented in late 2019, was used to identify goals of care documentation and EOL conversations. Additionally, clinical notes were scanned for “end-of-life” and “goals of care” text were then classified accordingly.
Metastasis was defined as a tumor spread to areas of the body distant or remote from the primary site. 28 Suspected signs of infection were identified if there was at least one reading of an elevated White Blood Cell Count (WBC) (≥11.0 × 10^9/L), 30 hypotension (systolic ≤85 and diastolic ≤50), or fever (≥100.4 degrees F/38 degrees C). Neutropenia was classified as WBC ≤1 × 109/L per established guidelines and institution standards. 31 Positive blood cultures were identified by microbiology test results identifying one or more organism growing in the blood samples collected, excluding coagulase-negative staphylococci. Heart rate was identified as non-specific and therefore excluded.
Data Analysis
RStudio Software (Rstudio version 4.0.5) 32 was used to calculate descriptive statistics for patients with and without antimicrobial use. Pearson’s Chi-square or Fisher’s exact test was used to determine statistical significance among categorical variables and Wilcox rank-sum for continuous variables.
Results
Patient Characteristics
Of 25,566 admissions in 2019, 943 (3.7%) were terminal admissions. Among terminal admissions, 633 (67%) patients met inclusion criteria; 376 (59%) patients with solid tumors received antimicrobials (AM+) within the last 7 days of life and 257 (41%) did not (AM-). supplemental material Table 1 summarizes the demographic data of both groups. More than half of the total sample were male (n = 345; 54%) and identified as non-Hispanic (n = 546; 86%). The most frequent solid tumor cancer types were lung (15%), breast (12%), and colorectal (8.8%) (supplemental material Table 1). Over three-quarters of both AM- and AM + patients had metastatic disease (78% and 79%, respectively). Neither the underlying cancer type nor presence or absence of metastatic disease significantly altered antimicrobial prescribing rates (P = .8) (supplemental material Table 1). AM + patients were significantly older than AM-patients (P = .012). AM + patients were more likely to have foreign devices in the form of urinary catheters, central venous catheters, and mechanical ventilation (all P < .001).
Antimicrobial use
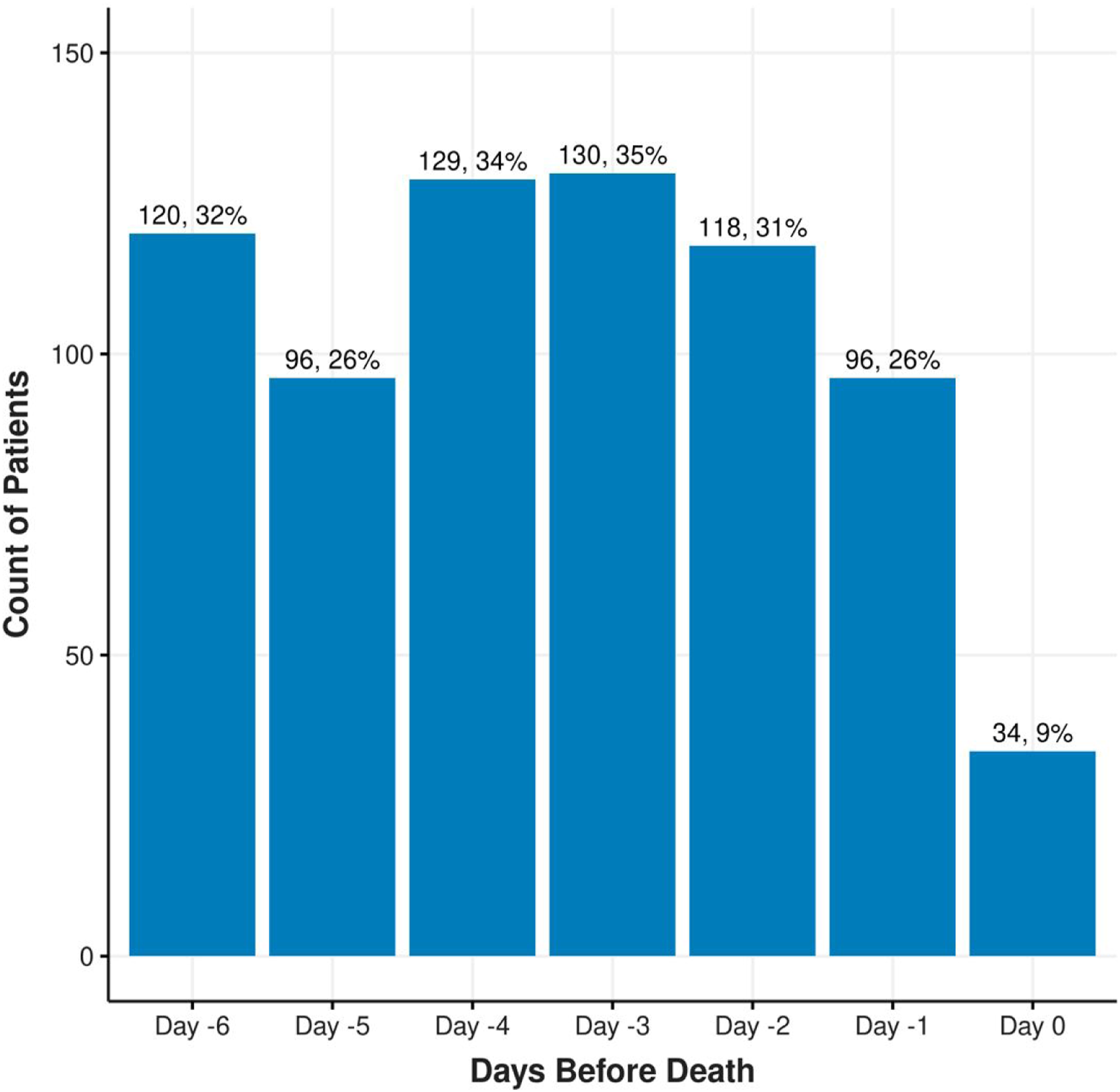
The most prescribed antimicrobial agents were the penicillin class (65%), intravenous vancomycin (49%), and meropenem (19%). Piperacillin-tazobactam was the most frequently used within in the penicillin class (97%). The frequency and types of antimicrobials administered are described in Figure 1. The number of patients with new antimicrobial orders in the 7 days leading up to their death (day 0) is shown in Figure 2. On the day of death, 34 patients (5%) were given a newly prescribed antimicrobial. The frequency of antimicrobials administered to patients during the last 7 days of life. Percentages will not add up to 100% as patients may have received multiple types of antimicrobials. Each bar represents the total number of unique patients with that antimicrobial type among the number of patients in the AM + cohort (n = 376). The frequency of new antimicrobial administrations during the last 7 days of life. Percentages will not add up to 100% as patients may have received antimicrobials on different days. Each bar represents the total number of unique patients who received antimicrobials on the specified day among the number of patients in the AM + cohort (n = 376).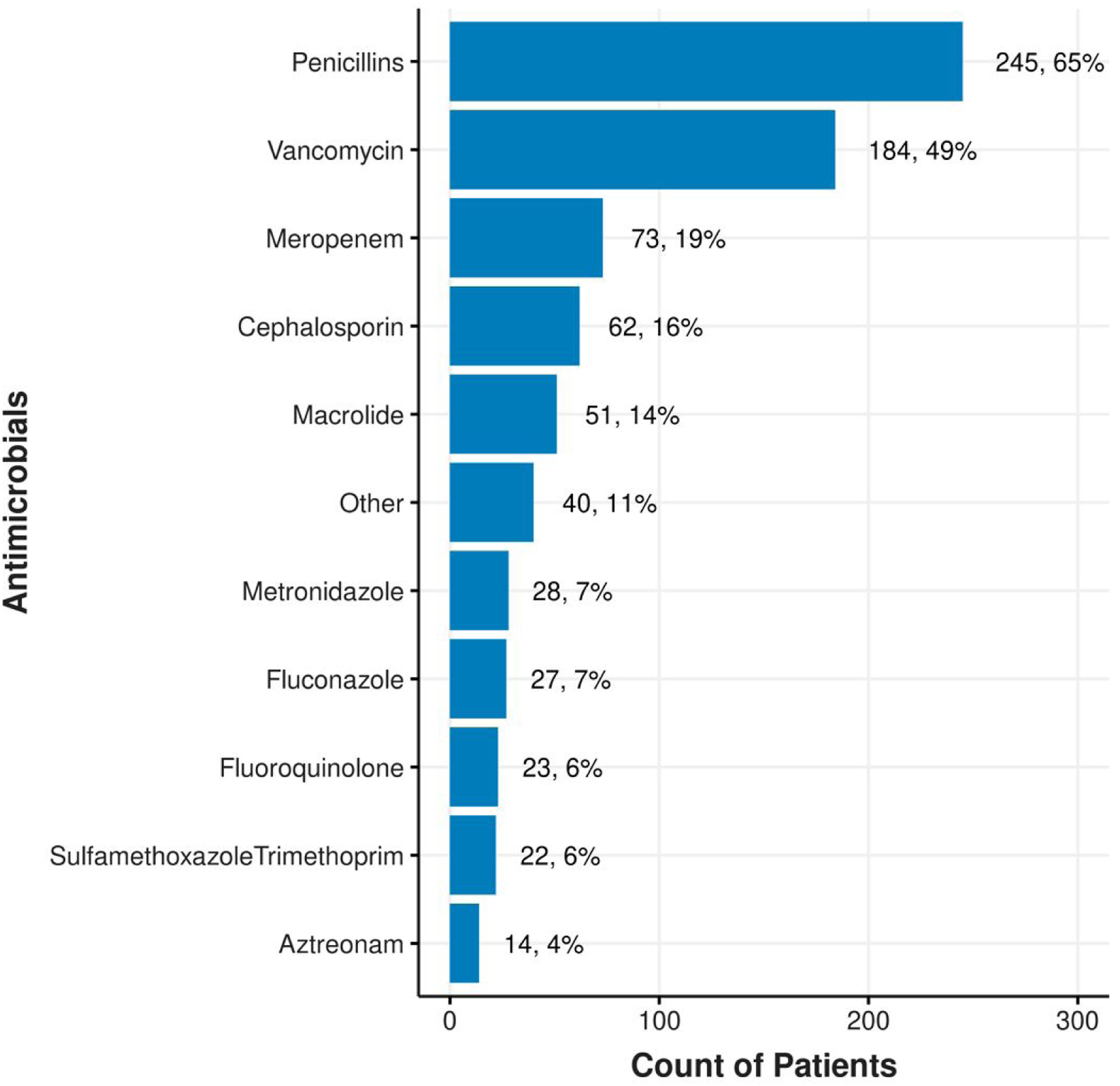
Suspected Signs of Infection
The frequency of neutropenia (P < .001) or suspected signs of infection such as leukocytosis, fever, or hypotension (all P < .001) were significantly higher in the AM + group (supplemental material Table 2). The AM + group had more results of a positive blood culture (not considered a contaminant) (P = .029). There was no difference in antimicrobial use among patients who had pathogens isolated from other sites, including respiratory, gastrointestinal, and urinary tracts (all P > .05) (supplemental material Table 4).
Diagnostic Testing
Aside from testing for stool pathogens, AM + patients received significantly more laboratory and radiologic testing in all categories (supplemental material Table 3). Laboratory testing included blood, respiratory, and urine cultures (all P < .001). AM + patients received significantly more imaging, including chest-abdomen-pelvis computed tomography (CT) imaging and mobile chest X-rays (both P < .001).
Characteristics of Terminal Admission
There was no significant difference in the number of EOL discussions or EOL care orders between groups (P = .055) (supplemental material Table 5). The AM + group had higher advance care planning EMR documentation in the form of DNR orders (P < .001) and a durable power of attorney by means of a health care proxy (P < .001). However, there was no significant difference in antimicrobial use with the presence of a documented goals of care discussion in the EMR (P = .8). Notably, we did not manually review charts to determine if advance care planning documentation included discussions about continuing or discontinuing antimicrobials. More AM + patients received a palliative care or infectious disease consultation (P = .17, P < .001 respectively) and died in the ICU (P < .001). Although AM + patients were more likely to have a visit from the rapid response team than the AM-cohort (10 vs 3 respectively), this result was not statistically significant (P = .2).
Discussion
While other reports have described antimicrobial use in patients with advanced cancer7,24 and those receiving hospice or palliative care,3,4,6,33 this study fills a substantive gap related to terminally ill hospitalized patients. The frequency in which antimicrobials were used at the EOL—59% in the last week of life and 5% on the day of death—was consistent with other studies.2,4,7,24 Our findings provide a unique clinical picture of patients with cancer who more commonly receive antimicrobials at EOL: those more likely to be older, with clinical signs of infection, who receive diagnostic and radiologic testing, and those with higher rates of palliative care or infectious disease consultations. Other variables significantly associated with EOL antimicrobial use included the presence of an indwelling foreign device, mechanical ventilation, completed advance directives, orders for EOL care, and death in the ICU.
Antimicrobials are often started empirically based on suspicion of infection. Patients living with cancer are at higher risk of infection at the EOL due to immunocompromised states, comorbidities, or chemotherapy use.5,17,34 Although patients in our study were more likely to have antimicrobials prescribed if they had clinical signs of infection, these are nonspecific and may overlap with signs of imminent death. 35 In addition, the work-up of suspected infection often includes diagnostic testing (e.g., radiology, laboratory) which can be a source of pain and discomfort at the EOL. Clinicians may feel obliged to correct abnormal laboratory results or act on radiology results which may lead to a cascade of interventions that have little benefit and may inadvertently increase suffering by prolonging the natural dying process. 17 Similarly, clinicians may be using antimicrobials to manage distressing EOL symptoms (e.g., dyspnea, pain) despite evidence-based practice guidelines.4,36 Rather, when the prognosis is deemed poor and clinical signs of death are evident, aggressive management of symptom burdens at the EOL and goal-concordant transitions in care (e.g., hospice, refusal of “heroic” or “aggressive” interventions, allowing for natural death/DNR) may substantially reduce non-beneficial use of antimicrobials and, more importantly, reduce distress for dying patients. Such interventions may include the evidence-based use and appropriate titration of opioids to mitigate moderate-to-severe cancer pain and breathlessness, as well as other controlled essential medicines (e.g., benzodiazepines, anticonvulsants) to alleviate symptoms and address underlying sources of discomfort.37-40
Baghban & Juthani-Mehta 5 have proposed an algorithm to navigate antimicrobial use at the EOL in which a comprehensive discussion about goals of care is required. However, antimicrobials are often omitted during advance care planning discussions, partly due to a lack of training. 41 Antimicrobial administration at the EOL is often perceived as relatively benign compared to other more invasive interventions such as mechanical ventilation or vasopressors.5,7 Like other EOL treatment decisions, prescribers may have ethical concerns, or worry patients and families may “lose hope” or feel abandoned if they discuss withholding/withdrawing antimicrobials. 19 In addition, patients or families may choose to forego some invasive treatment options (e.g., cardiopulmonary resuscitation, intubation, tracheostomy) but opt to continue antimicrobials despite recommendations against their use. A review of antimicrobial use in an Australian hospital found more than one-third of patients decided to continue antimicrobial treatment following discussions on their non-beneficial use. 8 Although we found no significant differences in antimicrobial use and documented goals of care, the complexity of discussions surrounding treatment preferences is exacerbated by prognostic uncertainty and novel oncologic treatment options for patients with cancer.
Initiating conversations about antimicrobials at the EOL earlier and in the context of the patient’s core values may improve goal concordant treatment. Incorporating the discussion of antimicrobials during the completion of advance directives or Medical Orders for Life-Sustaining Therapies forms may assist clinicians to formally document and respect patients’ EOL wishes. Data shows there are significantly more (P < .0005) antimicrobials prescribed when limits on use are not detailed in advance directive documents. 25 However, even with these documents completed, patients may not have discussed care preferences with their assigned health care agents and loved ones, requiring clinicians to be well equipped to address goals of care “just in time.” In cases of indecision or clinical uncertainty, use of time-limited trials may allow for a short-term trial of antimicrobial treatment while patients, families, and the medical team reach consensus. 42 When antimicrobial therapy discontinuation is recommended, interdisciplinary approaches are needed to optimize clinical communication, anticipate symptom management, and respond to rapid changes in patient condition.43,44
Our study reinforces the challenge of practicing antimicrobial stewardship for cancer patients in end stages. Education on the current evidence and potential for antimicrobial associated harms along with the use of a decision-making algorithm may assist clinicians to engage in shared decision-making with patients and families.5,14 Efforts to incorporate antimicrobials in advance care planning and improve EMR documentation of completed goals of care discussions are needed.15,33,45 Importantly, advance care planning must be understood as an iterative intervention, requiring revisiting by all members of the interdisciplinary team throughout the course of illness, during care transitions and treatment choice points, and at the EOL. 46 Integrating advance care planning in this manner and in keeping with a patient’s preferences can foster trust and relationship building between clinicians and patients and better prepare surrogates to make future decisions for patients while minimizing surrogates’ potential for decisional conflict.47,48 While clinicians may be familiar with the need to review resuscitation preferences during the hospital admission, there is an opportunity to normalize and prioritize the discussion of antimicrobials into serious illness conversations.
Consultation with infectious disease and palliative care specialists can help support clinicians in delivering recommendations about antimicrobial use at the EOL. Similar to our results, others 13 have also found infectious disease consultation resulted in increased antimicrobial prescribing and longer days on therapy, which is likely related to infection severity and complexity. Although we found antimicrobial use was not reduced with specialist palliative care involvement, this association has been shown in other studies. 2 Some reasons for this diversion from previous findings may be due to the presence of advanced disease and multiple complications arising from novel and aggressive cancer care in our sample.13,14 Given the increase in clinical acuity and complexity, involvement of both palliative and infectious disease specialty services may assist with challenging clinical decision-making and provide additional support for the primary interdisciplinary oncology team.
Limitations
The retrospective nature of the study was dependent on the EMR, and as such, we were unable to determine the indication for antimicrobial prescribing, radiology results, or if a patient had symptoms associated with positive diagnostic results. Documents were not manually reviewed to uncover if discussion of antimicrobials were included in progress notes or goals of care discussions. In addition, charts were not reviewed to determine whether diagnostic testing was a result of antimicrobial use or indicated prior to the initiation of antimicrobials. The number of antimicrobials discontinued before the day of death was not included in this study due to the unreliable nature of the EMR. To avoid confounding the results of this study, only patients with solid tumors were included due to the differences in immunosuppression and widespread use of prophylactic antimicrobials in hematologic malignancies. In addition, we did not limit the cohort to those with suspected signs of infection.
We did not consider the proximity of palliative care service involvement in relation to time of death. Given that services like palliative care are relationship-based approaches intended to be integrated into serious illness care starting at time of diagnosis,38,39 it is possible that specialist palliative care consulted closer to death may have been less effective in addressing goals of care discussions that included antimicrobial use in some cases. In addition, the number of patients receiving exclusively comfort-focused care may have been higher than identified because a formal EOL order set was not implemented at this cancer center until September 2019. Lastly, results of this study may not be generalizable to the general oncology population receiving care outside of a highly specialized tertiary cancer center with robust specialty services.
Implications
A key clinical implication of these findings is the need for primary palliative care capacity development for the entire interdisciplinary team in keeping with national cancer and palliative care clinical practice guidelines.38,39 Support for the development of primary palliative care communication would provide infectious disease clinicians with the skills needed to elicit patient goals, values, and preferences including the use of antimicrobials and other invasive interventions at EOL.39,49,50 As clinicians strengthen their confidence and clinical acumen to manage new symptom onset in the EOL setting, they may feel encouraged to question antimicrobial use when misaligned with patient values and goals and strategize appropriately. Further, antimicrobial stewardship programs can be a useful resource to guide and support clinicians in navigating decisions about antimicrobials at the EOL; however, these programs are not readily available. 44 A survey of ASPs found that only 64% had programs that monitor antimicrobial use at the EOL and only 36% of hospitals had ASPs that offered guidance for patients receiving comfort measures only. 44
Additional research is needed to evaluate antimicrobial use in patients receiving exclusive comfort-focused care and those patients who elect hospice services, differences in prescribing by race or ethnicity, comparison across groups of patients who did and did not have suspected signs of infection, as well as factors influencing the antimicrobial decision-making in the last 7 days of life. Although beyond the scope of this study, further investigation with chart review may provide a better understanding of the context of goals of care conversations, whether antimicrobials were mentioned, and how the integration and quality of antimicrobial discussions subsequently impacted prescribing and utilization. In addition, qualitative study of clinician, patient, and family perceptions on antimicrobial use may deepen our understanding on how antimicrobials are viewed by various stakeholders at the EOL.
Conclusion
This study reinforces the variation in practice of antimicrobial prescribing for solid tumor cancer patients at the EOL. Most of the hospitalized cancer patients in our sample received antimicrobials at the EOL, which were associated with invasive interventions that may interfere with experiencing comfort at the EOL. Factors associated with antimicrobial use at the EOL were identified, which can help inform institutional clinical practice guidelines and subsequent education and training efforts in primary palliative care, advance care planning, and antimicrobial prescribing. Formal collaboration with the Infectious Disease Society of America and the American Academy of Hospice and Palliative Medicine may be conducive to the development of best practice standards that guide the use of antimicrobials at the EOL and their incorporation into advance care planning. These results add to a growing body of literature on evidence about EOL antimicrobial use and can inform methods to reduce avoidable harm and promote comfort in patients with cancer with suspected or confirmed infection during the time surrounding death.
Supplemental Material
Supplemental Material - Factors Associated with Antimicrobial Use at the End-Of-Life Among Hospitalized Cancer Patients
Supplemental Material for Factors Associated with Antimicrobial Use at the End-Of-Life Among Hospitalized Cancer Patients by Shila Pandey, Renee Wisniewski, Sejal Morjaria, Anabella Lucca Bianchi, Tiffanny Newman, Carrie Tan, William E. Rosa, and Catherine S. Finlayson in American Journal of Hospice and Palliative Medicine®.
Footnotes
Acknowledgments
The authors thank Wen-hsing Yang, MSN, RN for assistance with literature review and Johnny F. Leung for assistance with data extraction.
Author Contribution Statement
All authors participated in data collection, analysis, preparation and editing of the manuscript.
Declaration of Conflicting Interests
The authors declare no conflict of interest.
Ethics Approval
This study was approved by the Institutional Review Board of Memorial Sloan Kettering Cancer Center before the collection of data (#21-408).
Funding
All authors except C.S.F. received funding from the NIH/NCI Cancer Center Support Grant P30 CA008748.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.