
Abstract
Background and Objectives
LGBTQ+ people are more likely to be caregivers for family and friends with life-limiting illnesses than non-LGBTQ+ people. LGBTQ+ caregivers may also experience stigma, bias, and discrimination, in addition to caregiving stress. Yet few studies have elicited LGBTQ+ family caregivers’ perspectives on their end-of-life (EOL) experiences of home hospice.
Research Design and Methods
We conducted semi-structured interviews with LGBTQ+ family caregivers of home hospice patients (N = 20). Following an interpretive descriptive approach, interview data were audio recorded, transcribed, and iteratively coded, and themes were developed and synthesized.
Results
The burden of having to wonder expressed caregivers’ uncertainty and concern about whether their negative experiences were common to all EOL caregivers or stemmed from cultural stigma and provider bias. Participants described how invisibility vs. risks of disclosure, anticipatory anxiety, perceived microaggressions, and protective vigilance increased stress and complicated caregiver-provider communication. Navigating EOL universalities vs. minority realities depicted underlying tensions between commonly assumed universalities of EOL caregiving and LGBTQ+-specific experiences. Providers’ discomfort, awkward communication, lack of access to culturally competent EOL support resources, and broader structural and cultural discrimination eroded their sense of connectedness and safety. Together, these themes characterized the impact of minority stress at EOL.
Discussion and Implications
Our findings suggest that LGBTQ+ hospice caregivers are at risk for minority stress in addition to more common sources of EOL caregiving pressures and thus have specific support and communication needs. Providers must understand this to deliver effective EOL care for all families.
Background
End-of-life (EOL) outcomes are sensitive to the quality of communication between family caregivers and hospice providers.1,2 This may be particularly salient in the home hospice setting, where unpaid family caregivers provide EOL care supported by routine visits from hospice providers. Family caregivers perceive the quality of hospice care in terms of providers’ clinical expertise and skill and their ability to establish trust and mutual respect.3-5 Hospice care providers must develop and maintain effective communication with hospice family caregivers to provide the best care and promote the best outcomes possible. 6
When hospice family caregivers are also members of sexual and gender minority groups (eg, lesbian, gay, bisexual, transgender, queer, and other orientations and genders besides heterosexual, cisgender, or gender binary or LGBTQ+), establishing effective communication and trust may be more challenging due to cultural and structural biases and inequities, the diversity of LGBTQ + identities and experiences, lack of provider knowledge and cultural competency, and LGBTQ + people’s past negative experiences with healthcare.7-9
LGBTQ + patients and caregivers report experiencing discrimination across healthcare settings,10-12 including at EOL. 13 In a recent survey of 865 U.S. hospice and palliative care providers, more than half believed that LGBTQ + patients and caregivers received discriminatory treatment, with nearly a quarter observing discrimination first-hand. 14 Negative interactions with healthcare providers over time can also affect LGBTQ + patients’ and caregivers’ EOL experiences.15,16 Ineffective or invalidating communication may be particularly harmful to gender minority patients and caregivers who continue to experience a high degree of discrimination and whose unique risks to the integrity of their EOL experiences include misgendering (eg, providers using gender-related language that is incongruent with a person’s gender identity) and forced detransition (eg, having gender-affirming care disrupted due to miscommunication and discontinuities along the EOL care continuum).8,17,18
Moreover, LGBTQ + people are more likely than non-LGBTQ + counterparts to be unpaid caregivers for family and friends with chronic and life-limiting illnesses. 19 They are also more likely to report caregiving-related financial strain, loneliness, and discriminatory work policies (eg, time off, family leave), while being less likely to report having conversations with health providers about the support they need to care for the patient or themselves. 20
While person- and family-centered care are foundational tenets of hospice, providers may not understand how structural disparities and personal experiences of minoritized status can shape the EOL experiences of LGBTQ + patients and caregivers. 21 They may also be unaware that they provide services for diverse LGBTQ + patients and caregivers as most hospice agencies do not routinely collect sexual orientation and gender identity (SOGI) data from patients or caregivers or incorporate LGBTQ + cultural competency training into quality standards or measures.22,23
Purpose
We sought to describe LGBTQ + caregivers’ experiences of providing EOL care to a family member or friend receiving in-home hospice services and to elicit their perceptions of 1) factors that shaped their experiences, 2) interactions with hospice providers, and 3) whether LGBTQ + hospice family caregivers and patients have specific or unique communication and support needs.
Methods
Our study design was guided by interpretive description24,25 wherein patterns and themes developed in the analysis are interpreted using relevant frameworks that address clinically significant issues to inform improvements in practice. The University of Utah's institutional review board reviewed and approved all study activities.
Recruitment and Sampling
We recruited a purposive sample of participants from across the U.S. via social media channels of community partners serving LGBTQ + cancer patients and caregivers, posting in a national caregiver organization’s email newsletter, and chain-referral sampling. Multiple methods were used as hospice and cancer family caregivers 26 and LGBTQ + participants27,28 are both historically challenging groups to recruit. Rolling recruitment continued until data saturation was achieved, as evidenced by repeating topics and tropes in participant responses. 29
Eligibility criteria included being a community-dwelling adult ≥18 years of age; self-identifying as LGBTQ+; being a current or past unpaid caregiver for a family member (biological relative or chosen family), friend, or close other with advanced cancer receiving home hospice services; either living or had lived with the care recipient or providing direct care for ≥8 hours/week; and the ability to read and speak English. Potential participants completed electronic consent before interviews and were re-screened to elicit additional detail confirming hospice caregiver status. All participants who screened in and participated received a $50 electronic gift card.
Data Collection
Participants completed a brief self-report demographic form before participating in a semi-structured interview by phone or video conference, depending on their preference. Interviews averaged 45 minutes in length, were audio-recorded, and transcribed following conventions for naturalized transcription. 30
Data Analysis
Five team members coded the data in 2 cycles using NVivo (released March 2020). Each recorded coding and analytic memos throughout that were discussed during team meetings, which facilitated pattern identification and conceptualization of findings. 25 First, coders followed a codebook drafted by the lead author to structurally organize the data by study topic. 31 After reading through all transcripts, each coder applied the codebook to the same 3 transcripts. The coding team met to compare this coding, discuss discrepancies, refine the codebook, and divide the remaining transcripts among coding pairs to code independently. The team compared coding and resolved differences through consensus.
Once all transcripts were structurally coded, teams of 2 coders independently and inductively coded data aggregated by topic. Each coding pair met to review coding and resolve areas of disagreement, and the team met routinely throughout the inductive coding process to discuss and document patterns. Comparative analysis of content and patterns generated the 2 overarching themes and related sub-themes reported here. Finally, consistent with the goal of interpretive description to explain study findings within a heuristic with clinical relevance and concrete application, we interpreted our thematic findings in relation to minority stress theory within the EOL home hospice context.
Results
Participant Demographics and Caregiving Characteristics
Participant Demographic and Caregiving Characteristics.
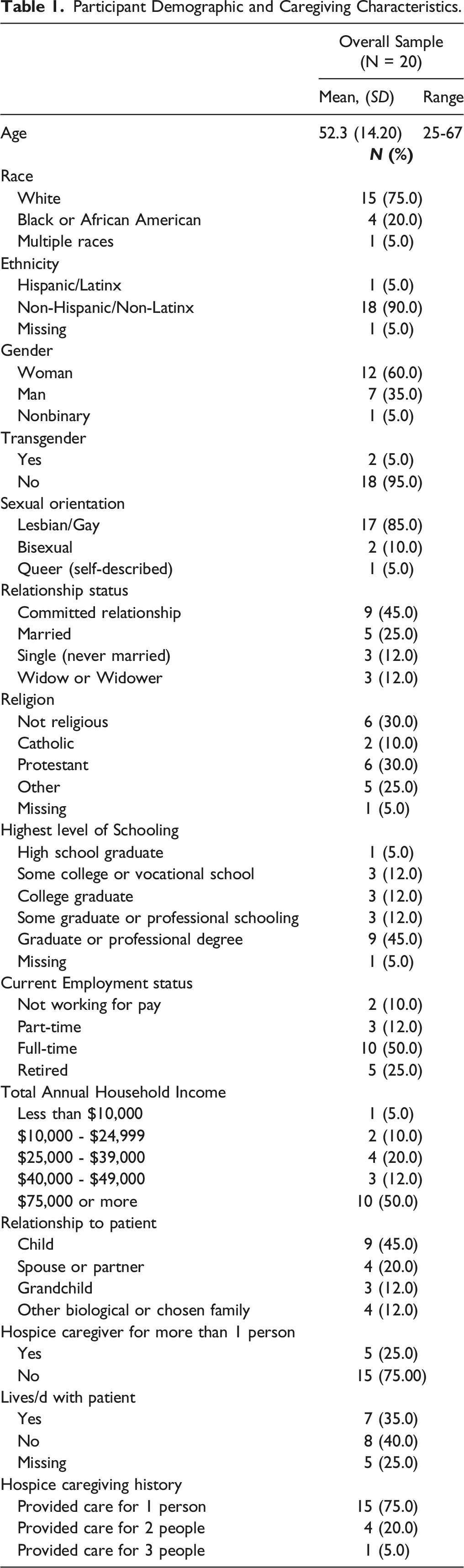
Participants (60%) were currently caregiving at the time of the interview. Eight (40%) had provided care in the past, ranging from 2 weeks to 25 years ago (M = 4.81 years, SD = 8.35 years). Five participants (25%) had cared for more than 1 person receiving home hospice services.
Thematic Analysis: The Burden of Having to Wonder
Participants described a level of uncertainty as to whether being LGBTQ + factored into their experiences with providers. One woman who cared for her long-term partner said: “I’m sure if I were married and had kids and my husband was dying, it would have been a different experience. But we don’t know that for sure.” Other participants described wondering whether to attribute difficult interactions to anti-LGBTQ + bias, to their age or gender, to complications in patient care, to providers’ moods or stress levels, or something else.
I think even now, there are times when I’m careful, and I don’t introduce [wife] as my wife. The fear is that somebody will treat you differently because you don’t know their proclivities and the inclinations associated with how they’re feeling about gay people.
This prevented some caregivers from being as open with hospice providers as they wanted to be and from seeking and receiving the support they needed. One woman who was an adult child caregiver stated, “It would have been nice to have someone be a little more personal, just to be able to talk to someone and cry with them. I didn’t do that with [the nurse]. I didn’t expand on my personal stuff. It would have been nice."
They’ll refuse because he’s gay. They don’t want to touch him and I get upset because even though he’s my dad and I don’t mind doing it. It’s just the fact that sometimes it makes me uncomfortable because I’m touching a man that’s related to me and I don’t do that. But the reason I do it is because I try to keep him clean and I try to make sure he’s okay because I’m responsible for him and nobody else ain’t going to do nothing but me.
We had one hospice care worker that came in, it felt was a little more dismissive of me. He would, I don’t know, it just felt like he kind of like bossed me around a little bit. At first, I thought he mistook me, even though he shouldn’t have treated anybody like this, like I was a [hospice aide] because I was the only one there. I’m like “No, we’re in this together. [My partner] wants me to be part of these decisions,” and I just felt there was a little bit of misogyny there too.
A young adult man caring for an older adult relative said the care and services they received were supportive with effective communication, yet he also felt that a nurse he interacted with made “off-color” comments about the way he provided direct care but felt uncertain as to why or whether it was intentional: That’s just one of those little microaggressions, I guess, that we’re just so used to. Just like a little maybe skepticism or misunderstanding or fear because [the nurse] doesn’t know what to expect, I’m probably the first gay man she’s ever met.
I have to be careful about it because I’d have to find somebody else or I couldn’t go to work. I had to find somebody else and make sure she wasn’t in physical danger but like [nurses and aides] were giving her attitude about that and giving me attitude and then, just not feeling that safe psychologically or physically sometimes too.
Further, she felt that the hospice providers sensed and resented her reluctance to leave the patient alone with them and believed that this diminished the quality of communication and care.
Navigating EOL Universalities vs Minority Realities
More than half of the caregivers interviewed made at least 1 statement about having the same needs as non-LGBTQ + hospice caregivers while they also recounted specific instances when they felt that being LGBTQ + made their situation different. Participants saw this as especially challenging when they thought providers were making normative assumptions that did not align with the caregivers’ reality. This spouse caregiver wondered whether nurses and aides saw her and her spouse as a family and whether this affected providers’ ability to communicate with them: Maybe [providers] do talk more to people who are--— if they’re like them. Maybe they can have more stories to share and that type of thing because they’re familiar with it. Maybe they think there’s something different with us and there isn’t, but you know what I mean? We didn’t have a [biological] family. We didn’t have anything like that.
An older man explained: “I feel like the first nurse could not believe that I had a difficult time with my mother, that—because I’m gay. I mean, that just wasn’t something she could understand, that my mother did not approve of me being gay.”
Sometimes, the problem is that heterosexual people are trying almost too hard on some level, and they aren’t attuned to things. They aren’t attentive to know what’s going on, because they’re working through their own fears or uncomfortableness. So it’s just kind of back to feeling like, okay, I don’t want to be the one to have to make you comfortable with this, you know? If I’m in for my routine physical, maybe I can be your project. Not now.
I could tell they did not like that we were a lesbian couple. Some [hospice aides] would ask directly [about being a couple] then others would read the Bible to me, and they’d like preach to me, and they’d ask me if I’ve been baptized and I would say to them “You cannot do this.”
Participants also raised the impact of a lack of structural protections for chosen families not legally codified or recognized. An unmarried woman caring for her life partner within their own home recounted how the failure of the hospice agency or local authorities to recognize or affirm the legitimacy of their years-long relationship impacted her experience at the time of her partner’s death: The rude awakening for me was when [she] died at home, and my power of attorney ended. When the ambulance came, they were like “We need a family member here to take the body away.” So, the police had to come until I could get her daughter to come from two hours away. I was angry. I was upset. The police officer that was there to guard the body, after about 15 minutes, he’s like “How about if I go sit outside in my squad car?” Like yeah, that’s a good idea.
Discussion: Minority Stress and Home Hospice Caregiving
Our findings suggest that minority stress impacts the home hospice experiences of LGBTQ + caregivers and patients. The burden of having to wonder whether being LGBTQ + affected the quality of EOL care manifested as a persistent underlying level of uncertainty, caution, and concern. Navigating assumptions about universal and minority-specific experiences layered additional LGBTQ + -specific anxiety and stress over the everyday EOL caregiving stressors. Even when these structural and institutional risks were not immediate concerns for participants, associations and memories remained in the background and were part of the context within which they interpreted their hospice caregiving experience.
Minority stress theory, first developed to explain the impact of systematic and structural discrimination and stigma on the mental health of sexual minority groups, 32 has been defined as chronic, cumulative, and ongoing stress that is specific to the experience of living as a member of a minoritized and stigmatized group in relation to a marginalizing dominant culture. Minority stress affects LGBTQ + people across their lifespans and has been associated with disparities in treatment and care outcomes across multiple conditions and healthcare settings.33-35 Sources of minority stress are described as both proximal (eg self-doubt, anticipated rejection, struggles with concealment vs disclosure) and distal (eg experiences of bias and discrimination related to structural discrimination and inequities.) 36 Proximal and distal stressors are often linked, and their effects interact over time to shape individuals’ life-course experiences along the continuum of health and aging, including EOL. 37
The effects of minority stress in health care settings are increasingly well-documented. 34 Despite this, hospice providers may believe that patients’ or caregivers’ LGBTQ + identity is irrelevant to EOL care, or that providers treat all patients and caregivers the same.21,38 How minority stress may impact the experience of EOL care remains under-examined, and accounts of LGBTQ + caregivers and patients are underrepresented in the literature. 10
Moreover, the complexity of delivering EOL care within patients’ and caregivers’ homes and personal spaces—and the many new intimacies and intrusions associated with EOL caregiving—may intensify the effects of minority stress. 39 More than 1 participant called the home they shared with their spouse or partner a “safe” space; an older gay male caregiver described the home as “a place where if you’re—especially if you’re in a closeted relationship—that’s the 1 place where you can be yourself.” For others, home hospice caregiving for biological relatives may exacerbate burdens associated with both EOL caregiving and minority stress, especially if the caregiver or patient has experienced rejection, psychological abuse, or trauma by those who provide care or with whom they must interact.
Study Limitations
Our sample does not fully represent the diversity of LGBTQ + hospice caregivers. We recruited only 1 transgender and 1 gender nonbinary participant, and only a quarter of our sample identified as Black or African American and mixed-race. Future research should explore these topics in a broader range of EOL caregivers from an intersectional perspective, including sources of stress that are particularly impactful for people with differing experiences and support needs. 40
Conclusion
A complex set of factors shapes EOL outcomes for LGBTQ + family caregivers and patients who may face a disproportionate risk of caregiver burden while having unmet support needs related to acknowledgement, safety, and trust. Hospice and EOL healthcare providers and researchers can understand these factors as manifestations of minority stress that span intrapersonal, interpersonal, and structural levels of influence. Understanding how minority stress dynamics shape the EOL care context for LGBTQ + family caregivers and their hospice care providers, and developing strategies to directly address these issues, is essential for promoting equitable and optimal hospice family caregiver and patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research (NIH NR016249; T32NR013456).