
Abstract
Objectives
Compared to urban family caregivers (FCG), rural FCG experience greater burdens accessing coordinated care for their loved ones during and after hospitalization. The impact of technology-enhanced transitional palliative care (TPC) on caregiver outcomes is currently being evaluated in a randomized control trial. This study evaluates resource use and health system costs of this FCG-focused TPC intervention and potential Medicare reimbursement mechanisms.
Methods
Rural caregivers of hospitalized patients were randomized into an 8-week intervention consisting of video visits conducted by a registered nurse certified in palliative care, supplemented with phone calls and texts (n = 215), or attentional control. Labor costs were estimated for a registered nurse and compared to scenario analyses using a nurse practitioner or social worker wages. Medicare reimbursement scenarios included Transitional Care Management (TCM) and Chronic Care Management (CCM) CPT codes.
Results
In the base case, TPC cost was $395 per FCG facilitated by a registered nurse, compared to $337 and $585 if facilitated by a social worker or nurse practitioner, respectively. Mean Medicare reimbursement in the TCM-only scenario was $322 and $260 for high or moderate complexity patients, respectively. Reimbursement in the CCM only scenario was $348 and $274 for complex and non-complex patients, respectively. Reimbursement in the TCM+CCM scenario was $496 and $397, for high/complex and moderate/non-complex patients, respectively.
Conclusion
TPC is a feasible, low cost and sustainable strategy to enhance FCG support in rural areas. Potential reimbursement mechanisms are available to offset the costs to the health system for providing transitional palliative care to caregivers of patients recently hospitalized.
Introduction
Family caregivers (FCG) play a critical and often under-recognized role in the health care system. 1 Compared to urban caregivers, rural caregivers experience greater burdens accessing coordinated care for their loved ones during and after hospital discharge.2-4 Interventions grounded in palliative care have been found to improve caregivers’ quality of life and psychosocial outcomes.5,6 The impact of technology-enhanced transitional palliative care (TPC) on patient and family caregiver outcomes is currently being evaluated in a randomized control trial. This paper assesses the feasibility and sustainability of the FCG-focused TPC intervention when potentially embedded in a health care system.
Caregiving can have significant negative psychosocial impacts on caregivers, hindering sleep quality, increasing social and economic strain, and in some cases manifesting as chronic stress and/or depression.7,8 The caregiving role is multifaceted, with FCG of patients often being called to facilitate conversations between providers and patients, maintain medical records, advocate for patients, and execute physical caregiving tasks, among other demands.9,10 FCG living in rural areas specifically face challenges that may compound existing caregiving burdens. Rural communities generally experience greater geographic distance from care, lower access to specialists, lower levels of education and income, and greater financial barriers.2-4 Despite high need for caregiving and palliative supports, low knowledge of palliative care compounds access issues in rural areas.3,11
To expand access to care, use of interventions delivered remotely using video platforms or phone calls has increased during the COVID-19 pandemic. Telehealth interventions differ in technological modalities, the duration of service provided, and the type of clinician offering the support. 12 The potential for technology-enhanced FCG interventions is supported by Holland and Vanderboom 2014’s assessment of the efficiency and effectiveness of technology-assisted transitional care support. 13 However, the evidence testing remote delivery and for non-cancer patients’ caregivers is nascent.12,14 The evidence for virtual caregiver interventions are mixed,15,16 with some reductions in burden and depressive symptoms. 17 While telehealth interventions have potential for increasing accessibility, evidence for the acceptability and feasibility of implementing telehealth interventions is limited, particularly in rural areas. 18
Especially in rural areas, limited resources to support inpatient and outpatient palliative care at a loss could hamper access to extending services to include caregiver supports. Despite potential benefit to caregivers, inpatient palliative care interventions are often provided at a financial loss to the health system, with hospitals covering half of palliative care program funding. 19 Lack of reimbursement options are a key obstacle to implementation of palliative care in rural communities. 20 One promising trend is that the COVID-19 pandemic has motivated the introduction of a greater range of telehealth-specific reimbursement mechanisms that may provide new avenues for remote palliative care. 21
This paper uses a budget impact analysis to assess the feasibility and sustainability of the FCG-focused TPC intervention from a cost perspective. We compared health system costs from the perspective of the provider and potential Medicare reimbursement mechanisms. This budget impact analysis is intended to support the implementation and dissemination of the transitional palliative care (TPC) for FCG. We apply a health care system perspective to provide practical information about resources, costs, and reimbursement that administrators of rural health facilities could use to build a business case for TPC to support FCG.
Methods
We conducted a budget impact analysis of a TPC intervention as implemented in a randomized clinical trial using the health care provider perspective which consists of a large health care system with hospital facility and outpatient network. We also evaluated potential revenue streams to assess sustainability in the short term (<1 yr) to support adoption and implementation decisions. We evaluated TPC intervention resource use using intervention data from the trial and then estimated delivery costs using mean national wage rates from the United States Bureau for Labor Statistics (BLS). We also estimated the costs in scenarios where the intervention was facilitated by a social worker or nurse practitioner. Estimated program costs were compared to potential Medicare reimbursement mechanisms in 3 scenarios: Transitional Care Management (TCM) only, Chronic Care Management (CCM) only, and TCM+CCM.
Intervention Delivery and Costs
As a part of the randomized control trial, community-dwelling rural caregivers of hospitalized patients with a serious life-limiting illness and receiving palliative care during hospitalization in Minnesota, Wisconsin, and Iowa were randomized into an attention control condition or to an 8-week TPC intervention consisting of video visits, conducted by a registered nurse, supplemented with phone calls and texts (n = 215). For those in the intervention group, interventionists—registered nurses certified in palliative care--met with caregivers prior to hospital discharge, and after discharge they met twice a week for 4 weeks and then once a week for another 4 weeks. Calls consisted of teaching, guidance and counseling for caregivers. Those in the attention control condition received a phone call once a month to collect data on costs or if they reported high rates of depression on any study survey, they received a supportive phone call from a palliative care social worker. 13 This trial and study activities were registered at Clinicaltrials.gov (NCT03339271 Protocol version: 11) and were approved by the health care system’s Institutional Review Board (IRB# 17-005188).
The primary resource needed to implement the intervention is the workforce with the skills and time to conduct the intervention. We did not include overhead or capital investment costs in this budget impact analysis because palliative care interventions are typically implemented in settings where the fixed costs are supported by other revenue streams. We excluded time spent on research activities by the study team. In the trial, the intervention was facilitated by a registered nurse certified in palliative care. Labor costs were estimated using the BLS median hourly rate for a registered nurse and compared to a scenario analysis using a nurse practitioner or social worker wages.
Most visits were conducted using a video platform on the caregiver’s chosen electronic device, and when necessary, by phone, so we did not assess travel costs for our estimates to reflect remote implementation. A one-way sensitivity analysis estimated resource use over a range of visits per FCG and time per visit.
Reimbursement
Medicare reimbursement scenarios included CPT codes for TCM and CCM.22,23 We specifically selected CPT billing codes that allowed for 1) caregiver education and engagement, 2) remote, telehealth services in an outpatient setting, and 3) non-physician, auxiliary staff time. Other codes considered included the Cognitive Assessment and Care Plan (99 483, 99 484) for dementia patients and Outpatient Palliative care/Advance care Planning (99 497, 99 498). After review of CMS documentation, discussion with the study team and external experts, we decided these did not reflect the intervention services as delivered in the trial as well as the TCM and CCM codes. Of course, physicians and administrators will need to assess which billing codes appropriately reflect any services they provide after consulting Center for Medicare and Medicaid Services (CMS) regulatory documents.
We simulated 3 scenarios for reimbursement using the National Payment amount from the CMS Physician Fee Schedule:
The TCM billing code would only be appropriate for services provided in the 30 days following hospital discharge, assuming CMS minimum service requirements are met. TCM (99 496 or 99 495) may be billed 1 time, and the billing code for additional services in the same 30-day period (99 439) may be billed up to 2 times. However, in the trial, the intervention included visits preceding and following hospital discharge, so any inpatient visits prior to discharge would not be billable in this scenario. TCM requires a face-to-face meeting within 14 days (or 7 for high need) of hospital discharge, however this can be provided as a telemedicine service if the patient and caregiver agree. TCM billing codes require a nurse practitioner or physician conduct the initial visit, and this initial visit is expected to be combined with non-face-to-face services that may be delivered by another qualified health professional. TCM would not be available to provide reimbursement for visits after the first 30 days following hospital discharge.
We used the national payment amount for each CPT code from the 2022 Medicare physician fee schedule to estimate reimbursement for staff time (appendix). To be conservative, we calculated reimbursement as 85% of the physician staff time to allow for the potential of non-physician staff, such as nurse practitioners, billing these services. Intervention cost and potential reimbursement are reported in 2022 US Dollars. No discount rate is applied due to the short time horizon. All data were evaluated in Stata Version 16.
Results
The majority of caregivers in this study (215 intervention, 214 control) were under 65 years old (60%), women (71%), white (92%), not Hispanic or LatinX (99%), married or in a relationship (75%), the spouse to the care recipient (66%), and had some college (57%). All lived in rural or underserved areas. The majority of care recipients were over 65 years old (62%), men (57%), white (97%), not Hispanic or LatinX (99%), married or in a relationship (70%), and had either some high school or had completed high school (56%).
TPC Intervention Activities Over the 8-Week Study Period by Study Arm.
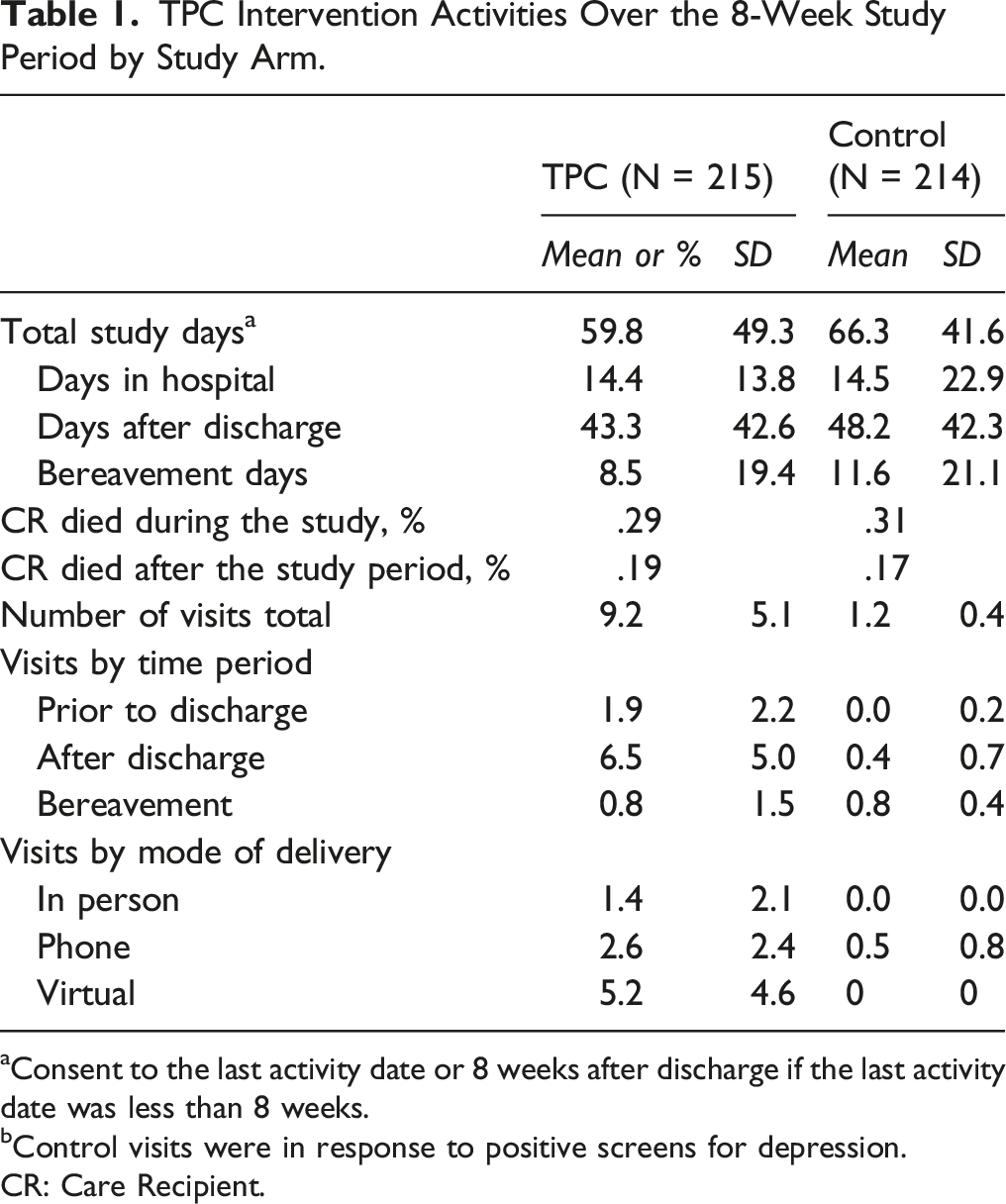
aConsent to the last activity date or 8 weeks after discharge if the last activity date was less than 8 weeks.
bControl visits were in response to positive screens for depression.
CR: Care Recipient.
Using study data documented by the nurse interventionist, we estimated registered nurse (RN) time to deliver the intervention included activities such as 1) scheduling visits, 2) conducting the visits, and 3) documenting patient and caregiver information (Table 1). The nurse spent an average of 10 minutes per visit to schedule the visit, for a total of about 1.5 hours per caregiver over the study period. The nurse spent .7 (about 45 minutes) hours per visit conducting the visit, for a total of 6.3 hours per caregiver over the study period. The nurse spent about 3.1 hours documenting information into the chart for each caregiver over the study period. Nurses spent a total of 8.9 hours across all activities per caregiver over the study period.
Input Parameters for Estimating Cost of TPC Implementation.
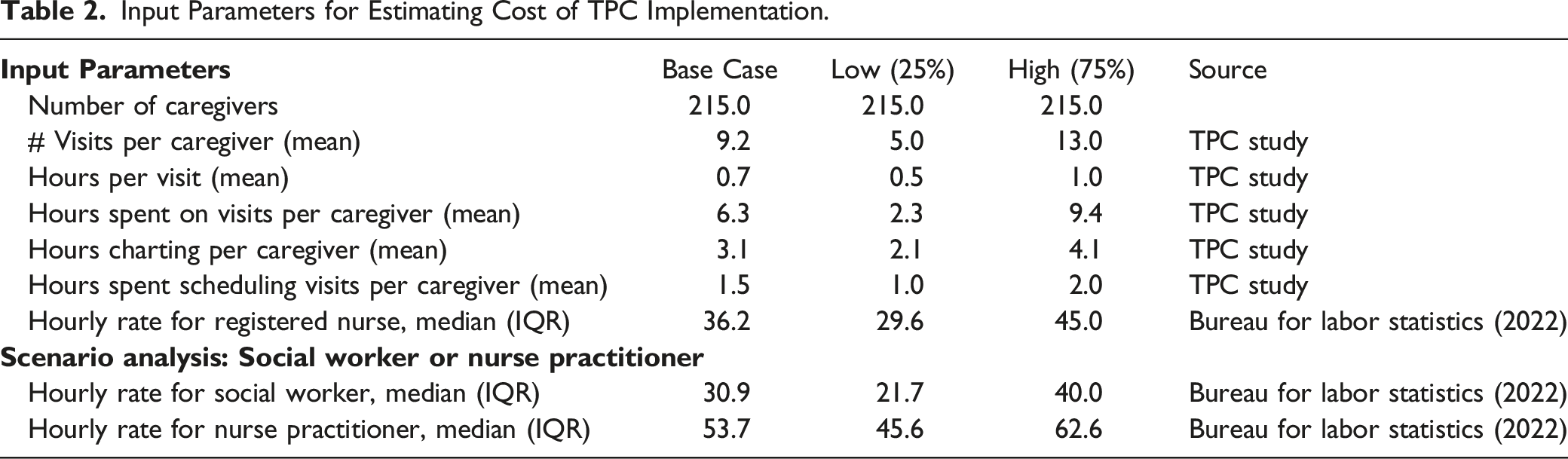
In the base case, TPC cost was $395 per caregiver if facilitated by a registered nurse, compared to $337 and $585 if facilitated by a social worker or nurse practitioner, respectively. A one-way sensitivity analysis accounting for variation in hourly rates for each type of professional as well as number of visits and hours spent revealed that potential costs per caregiver may be significantly more or less than this base case estimate depending on how the intervention is implemented (Figure 1). One Way Sensitivity Analysis: Change in Cost per Caregiver at the 25th and 75th percentile for each parameter compared to the base case (2022 USD).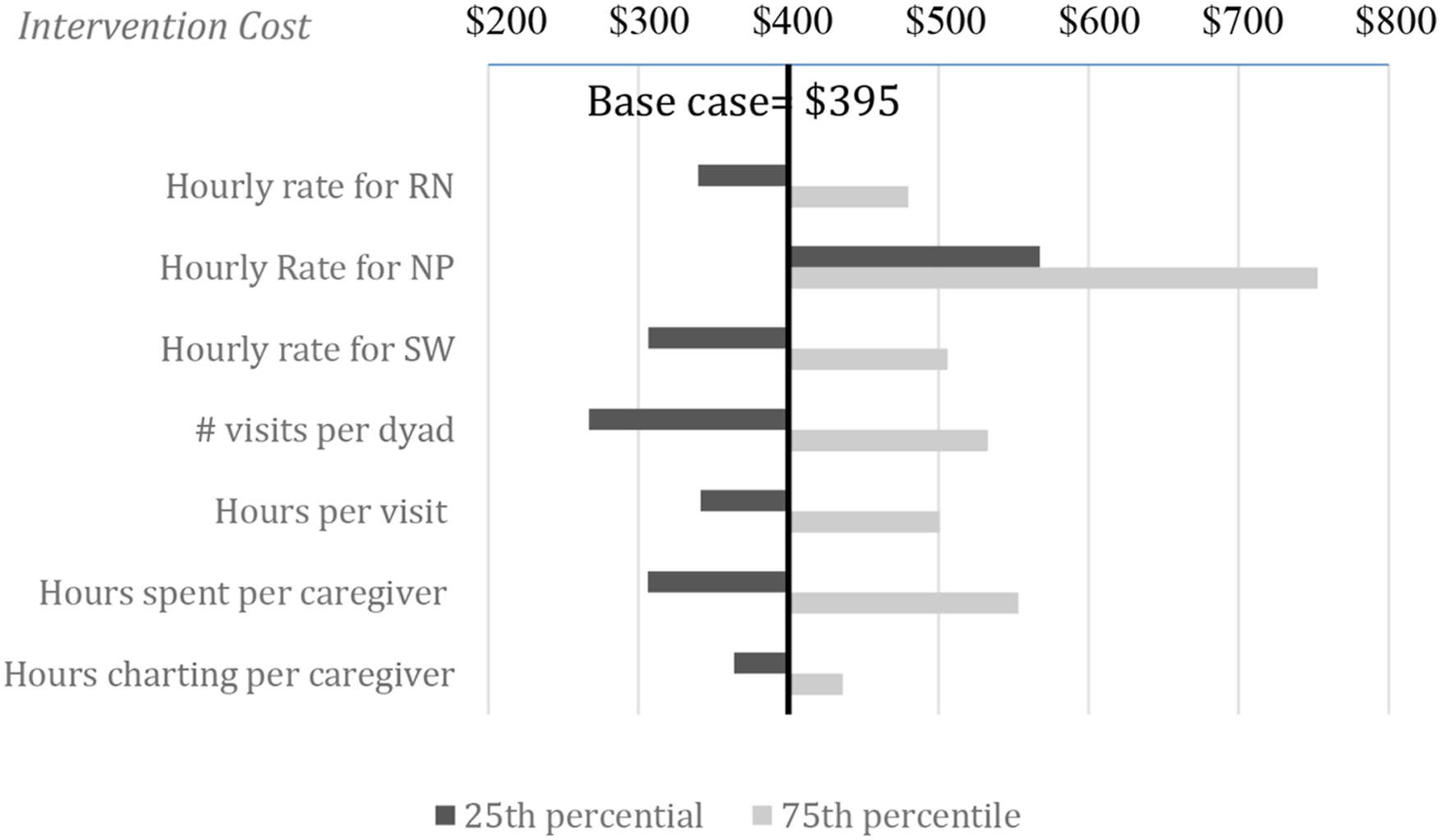
Of all the potential factors affecting the estimate, number of visits had the greatest influence on total costs of the intervention (low of $291, high of $488) (Figure 1). Variation nationally in hourly rates for registered nurses or social workers also impacted total cost. Utilization of a nurse practitioner even at the 25th percentile of hourly rate increased the total cost estimate relative to a registered nurse (Figure 1).
Potential CMS Reimbursement
Reimbursement amounts were higher than the base case cost of $395 for the TCM+CCM scenario, for both complex and non-complex patients. Reimbursement in the TCM+CCM scenario (60 days post-discharge) was $495 and $396, for high/complex and moderate/non-complex patients, respectively.
CMS Reimbursement Codes and Revenue for Transitional Care Management and Chronic Care Management Services (2022 USD).
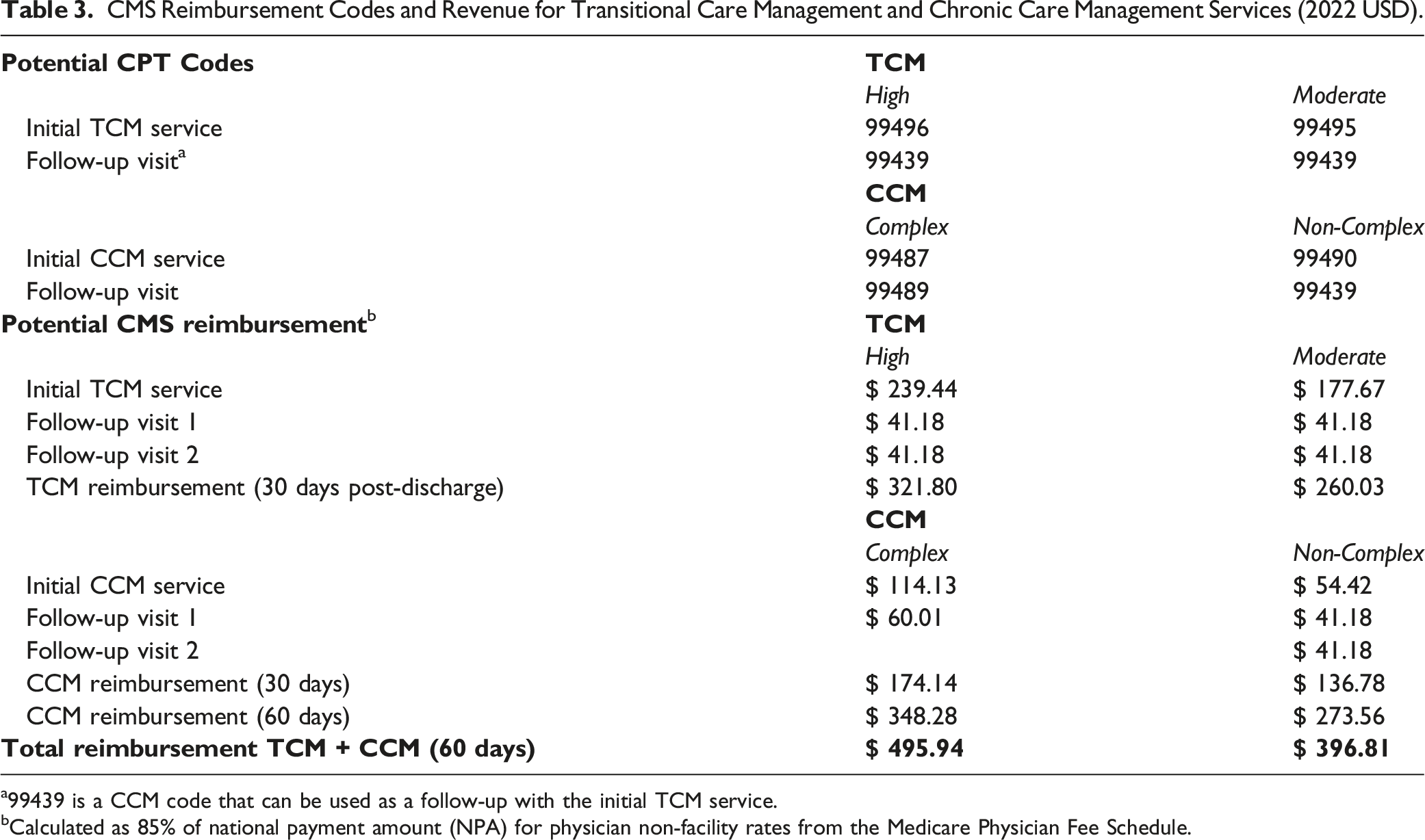
a99439 is a CCM code that can be used as a follow-up with the initial TCM service.
bCalculated as 85% of national payment amount (NPA) for physician non-facility rates from the Medicare Physician Fee Schedule.
Discussion
TPC provides palliative care supports to family caregivers using telehealth, and we found TPC is a feasible, low-cost and sustainable strategy to enhance caregiver support in rural areas. Potential reimbursement mechanisms are available to offset the costs to the health system for providing transitional palliative care to support caregivers of patients recently hospitalized. However, to offset the total costs of the intervention, health systems must ensure that both the TCM and CCM criteria are met. Use of TCM or CCM billing mechanisms alone is not sufficient to cover the average cost of the intervention.
In the trial, the intervention was facilitated by 2 registered nurses specialized in palliative care, and both intervention nurses had years of palliative care experience. In other contexts, similar interventions have been facilitated by social workers, registered nurses, or licensed practical nurses. 24 A systematic review of 9 telehealth palliative care interventions demonstrates overall caregiver satisfaction and reported improvement of quality of life. 12 The review reported the average duration of a telehealth call to be 12 minutes, whereas the video visits in our intervention averaged about 45 minutes. There were other variabilities (eg, patient age, diagnosis, immediate vs schedule calls) between the programs evaluated in the review and our intervention that would impact resource use.
Use of appropriate billing codes available through CMS on average reimburses most of the direct labor expenses needed for delivery of the intervention. However, substantial variation in the time to deliver the intervention results in scenarios where reimbursement is not sufficient to cover the costs of the intervention. For example, if the duration of visits is longer than the average case at the 75 percentile, the intervention would cost close to $500 with only $495 available in maximum CMS reimbursement using the TCM+CCM approach. While number of visits per caregiver was dictated by the study team, length of call was driven by caregiver needs. Most of the time longer calls indicated more issues, but sometimes shorter calls indicated an overwhelmed caregiver with little time to spare.
We present scenarios for use of advanced practice and limited scope practitioners because the TPC intervention should be tailored to meet the needs of the FCG and care recipient. Although the NP may cost more, they generally can prescribe medications and diagnostic services that the RN may only recommend. In the trial, the FCGs were typically caring for patients with complex care needs that required a palliative care trained nurse. In other contexts, a higher level of practice such as NP may be needed for complex medical decision-making or a lower level of practice such as a social worker may be sufficient for non-complex chronic care management. The high/moderate and complex/non-complex designations for TCM and CCM should take into consideration CMS definitions, including the amount of time/resources used by the provider to support the patient and their caregiver with medical decision-making and care management.
In addition to considering the budget impact to health systems, it is also important to consider the cost to the patient/family. CMS allows providers to charge patients a cost-sharing fee. In the case of TCM and CCM, the allowable fee is usually less than $10. However, in this intervention, a $10 co-pay for each visit would add up over time and create a substantial burden on some caregivers. Even if CMS reimburses the provider costs of providing the intervention, cost sharing with the caregiver and patient may limit the acceptability and feasibility of scaling the TPC intervention.
Health systems implementing TPC and similar supports for complex patients and caregivers may also benefit from participating in shared-savings contracts with insurers. The Medicare Shared Savings Program for Accountable Care Organizations allows health systems to share in any savings from prevented hospitalizations and other health care use.
This study fills an important gap in the evidence for the sustainability of telehealth, transitional palliative care interventions. To be conservative in estimating potential revenue, we did not include reimbursement for inpatient visits, however these might be billable in some situations. We also estimated reimbursement at 85% of the National Payment Amount because this is the rate allowed for non-physician practitioners, though in some cases 100% of the NPA reimbursement may be appropriate. In the trial, some visits occurred during the bereavement period, and these would not be reimbursable in the scenarios presented in this paper. To improve generalizability to different contexts, all costs were estimated using national data. However, local wage rates and workforce availability will impact whether this intervention is sustainable for individual health systems.
Family caregivers may benefit from transitional palliative care following hospital discharge to the community, and sustainable reimbursement is necessary for scaling TPC and similar telehealth interventions. This study demonstrates that TPC is a low-cost, and potentially budget-neutral intervention when using CMS reimbursement for transitional care and care management as is appropriate. Further research into cost and reimbursement strategies in value-based payment models is needed to promote implementation and scaling of caregiver support programs.
Supplemental Material
Supplemental Material - Implementation Costs of Technology-Enhanced Transitional Palliative Care for Rural Caregivers
Implementation Costs of Technology-Enhanced Transitional Palliative Care for Rural Caregivers by Brystana G. Kaufman, Diane E. Holland, Catherine E. Vanderboom, Cory Ingram, Ellen M. Wild, Ann Marie Dose, Carole Stiles, Allison M. Gustavson, Alice Chun, Erica Langan, Henry A. Baer-Benson, Jay Mandrekar, and Joan M. Griffin in American Journal of Hospice and Palliative Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Gustavson was supported for this work by the Agency for Healthcare Research and Quality (AHRQ) and Patient-Centered Outcomes Research Institute (PCORI) grant K12HS026379; the National Institutes of Health’s National Center for Advancing Translational Sciences, grant KL2TR002492; and the Minneapolis Veterans Affairs Center of Innovation, Center for Care Delivery and Outcomes Research (CIN 13-406). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government, AHRQ, PCORI, or Minnesota Learning Health System Mentored Career Development Program (MN-LHS).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health, National Institute of Nursing Research - NIH-NINR R01NR016433.
Competing Interests
Clinicaltrials.gov # is NCT03339271. Registered on 13 November 2017. Protocol version: 11.
Key Points
This paper evaluates resource use and health system costs of this family caregiver-focused Technology-Enhanced Transitional Palliative Care intervention and potential Medicare reimbursement mechanisms. Potential reimbursement mechanisms are available to offset the costs to health systems for providing transitional palliative care to support caregivers of patients recently hospitalized.
Compliance with Ethical Standards
Data Availability
Study data is available on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.