
Abstract
Background
There is a research gap regarding safety concerns of patients at the end of life. The aim of this study was, therefore, to explore whether patients under specialist community palliative care feel safe at home and which factors affect the perceived safety. Furthermore, we investigated if perception of safety is associated with different aspects of subsequent care.
Methods
Using a standardized questionnaire, a cross-sectional survey was conducted among 100 specialist community palliative care patients. Logistic regression was used to examine the strength of the association between clinical and socio-demographic variables and the perception of safety. After a 6-month follow-up period, we analyzed differences in various care-related outcomes between patients with unaffected and impaired perceptions of safety.
Results
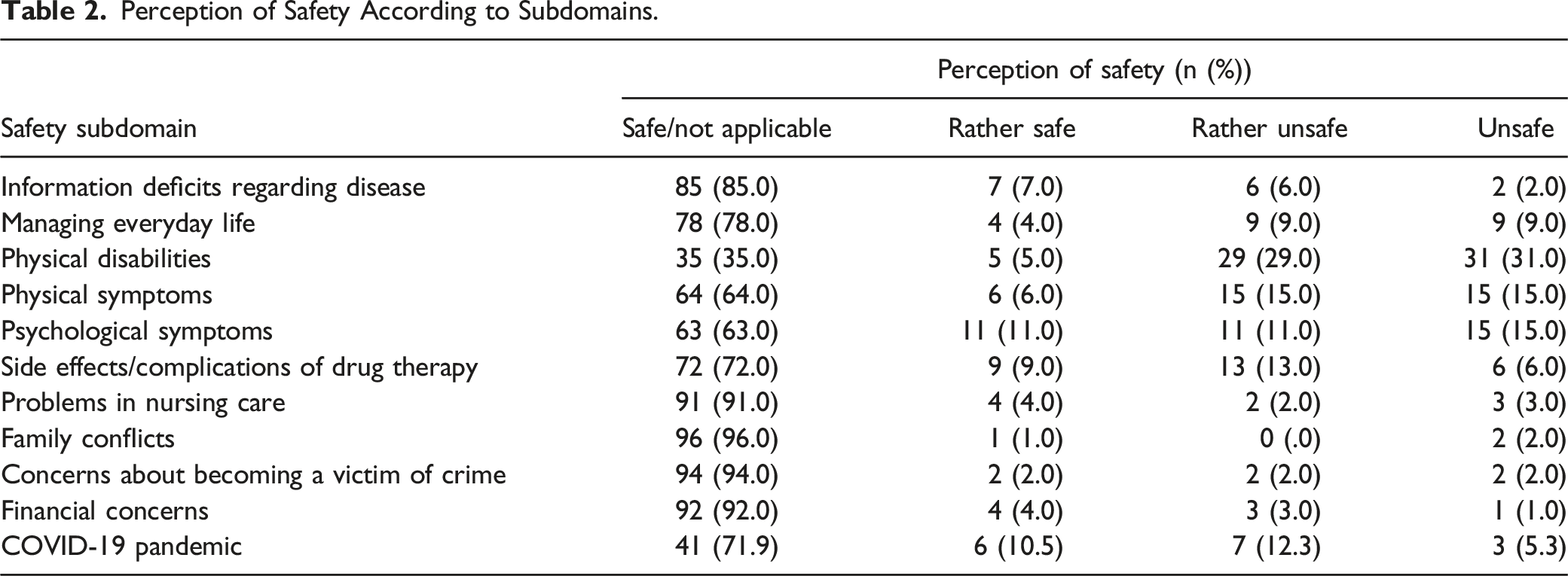
In our study, one in five patients receiving specialist community palliative care expressed safety concerns. Subdomains of safety that were reported most frequently were physical disability (60%), physical symptoms (30%), psychological symptoms (26%), and side effects/complications of drug therapy (19%). Of the participants surveyed after the initial COVID-19 lockdown, 35.1% reported that they felt their safety had been adversely affected by the pandemic. Compromised safety perception was associated with higher levels of palliative care-related problems, and proximity to death.
Conclusions
Our study uncovered relevant safety concerns of palliative care patients receiving specialist community palliative care. The insights gained into patient-reported problems may help healthcare professionals to identify situations where patients feel unsafe. Further research should address primary and secondary prevention measures to improve the quality of end-of-life care in the home environment.
Introduction
Patient safety is defined as “the absence of preventable harm to a patient during the process of health care and reduction of risk of unnecessary harm associated with health care to an acceptable minimum”. 1 Patient safety represents one of the cornerstones of high-quality healthcare 2 and, in recent years, has gained increasing attention in the palliative care literature. 3 This goes hand in hand with the realization that end-of-life interventions are particularly prone to medical errors due to prevailing intensive and complex treatment strategies as well as shortcomings in care. 4 These, in turn, may promote or prolong unnecessary suffering, shorten life and cause additional economic costs.4-7
Important integral aspects of patient safety that have already been addressed in research are that of side effects and medical errors.4,8 Nevertheless, little is known about patients’ own perception of safety at the end of life, especially in the home environment. Patients’ experience of “feeling safe” often goes far beyond the health care system’s common definition of safety focusing on malpractice. 3 First evidence suggests that in addition to the physical domain, emotional, social, and spiritual aspects are highly relevant to patients and their families when evaluating safety. 9 A differentiated and individualized approach to the assessment of safety and implementation of safety measures is therefore crucial to ultimately ensure the holistic safety of palliative care patients.
The particular relevance of patients’ perception of safety is reflected in the fact that — if compromised — it can influence the further course of the disease and thus care. Hence, the feeling of not being safe can be associated with pronounced psychological symptoms such as anxiety and depression. 10 In populations of seriously ill patients, it has been shown that safety considerations can even make the decision more likely to present in hospital.11,12 Conversely, actual or anticipated safety threats at home may lead to patients staying unnecessarily long in hospital. Given that most people wish to be cared for and die at home13-15 and that hospital admissions represent a huge economic burden for healthcare systems, 16 identifying factors that militate against a sense of safety at home could provide an opportunity to improve home care, make sensible transfer decisions and use hospital resources more efficiently.
The objective of the present study was therefore to investigate the relevance of distinct safety concerns and factors associated with impaired safety perception from the perspective of patients receiving specialist community palliative care and to clarify whether perception of safety is related to later aspects of care.
Methods
We designed a cross-sectional study to specifically examine whether patients under specialist community palliative care feel unsafe in their home environment, which subdomains of safety are mostly compromised, and which factors adversely affect the perceived safety. Closely related to this, we inquired whether the perception of safety is associated with aspects of care such as survival time, place of death as well as the number of contacts with the community palliative care team, and hospital admissions.
Study Design
Our cross-sectional survey was conducted using a questionnaire with close-ended questions to capture participants’ experience of safety. The items were developed using a two-step methodology. First, a multidisciplinary research team drafted items that were based on scientific knowledge 3 and own experiences from clinical practice through an iterative consensus procedure. During the discussions, the research team agreed on one item inquiring about the general perception of safety but also one item each relating to following safety subdomains: information deficits regarding disease, managing everyday life, physical disabilities, physical symptoms, psychological symptoms, side effects/complications of drug therapy, problems in nursing care, family conflicts, concerns about becoming a victim of crime and financial concerns. Some items were given examples for better comprehensibility, eg managing everyday life with “shopping, cooking, cleaning.” For every item, patients were asked to rate their safety perception on a four-point likert scale: “I feel safe,” “I feel rather safe,” “I feel rather unsafe,” “I feel unsafe”. For better standardization and comparability, a limited recall period for perceived safety of 7 days was chosen.
Second, prior to the final application of the questionnaire, two researchers (A.P. and A.B.) undertook cognitive interviews with five specialist community palliative care patients that helped to ensure face and content validity and to test problems in feasibility eg, comprehensibility of the questions or acceptance. Applying the two cognitive interview techniques think-aloud and verbal probing, 17 it was possible to gain insights into the thought processes of the respondents and thus uncover potential causes of problems in the questionnaire items. Minor changes in wording were made to the questionnaire according to the results obtained.
After the outbreak of the COVID-19 pandemic in Germany, we added an item inquiring about safety concerns arising from the pandemic in a second recruitment phase following the first German lockdown in 2020. This was based on the assumption that this new and thus unexplored aspect could also play a decisive role in the perception of safety.
Data Collection
During the main study, the final questionnaire was read aloud to all participants. The interviewer filled in the questionnaire manually according to the answers given. Furthermore, the respondent answered the Integrated Palliative Care Outcome Scale (IPOS), a validated instrument to assess the main symptoms and concerns of palliative care patients. 18 The researcher determined the Karnofsky performance status scale (Karnofsky index) and ECOG status. Following socio-demographic variables were collected through the questionnaire: Marital status, education level, housing situation, number of household members, housing location, and information on nursing support. The patient’s age, principal diagnosis, and length of care at the time of the survey were retrieved from the electronic care record.
In a 6-months follow-up analysis, the number of contacts between the specialist community palliative care team and patients and/or relatives (home visits and telephone contacts), number of hospital admissions (planned and unplanned), and ultimately the place of death were extracted from the electronic documentation in order to investigate whether the expressed perception of safety had an association with these care-related variables.
Study Population and Recruitment
Our study targeted patients receiving specialist community palliative care. The local specialist palliative care service has a catchment area that is characterized by an urban as well as a rural environment and is home to around 300,000 people. Specialist community palliative care in Germany serves as a complement to standard care and is aimed at people with life-limiting illnesses and their families when the intensity or complexity of the problems resulting from the course of the disease makes the involvement of a specially trained team necessary, either temporarily or permanently. The following eligibility criteria applied to our study:
Inclusion Criteria
• Adult patients who have been cared for by the local specialist community palliative care team for at least 7 days • Sufficient German language comprehension • Ability to give consent and sign a consent form
Exclusion Criteria
• Residents of inpatient hospices or residential care • Patients for whom the clinical team indicated that they were too weak and/or psychologically too stressed to participate in the study • Hearing or visual impairment of a severity that interferes with interviewing
All patients who met the eligibility criteria were registered as potential study participants and asked about their willingness to participate in the study during a regular contact. After obtaining written consent, an appointment was scheduled for the interview in the patient’s home.
In order not to further jeopardize the health of the vulnerable population during the COVID-19 pandemic, recruitment had to be interrupted several times for longer periods due to rigorous restrictions on conducting research projects. The total duration of recruitment, therefore, stretched from August 2019 to August 2021.
Analysis
Statistical analysis was performed using R Studio. Descriptive analysis was undertaken for socio-demographic and clinical variables. In addition, odds ratios were calculated using binary logistic regression to determine how strongly the individual variables were related to the perception of safety. For this purpose, independent variables were dichotomized, eg independent living situation (own household) vs. supported living situation (with children/partner/assisted living). Aware that this methodology could overestimate perception of safety, the dependent variables were combined, eg “I feel unsafe” and “I feel rather unsafe” to “perception of impaired safety.” This was defined as a safety concern for the individual sub-domains of safety. Finally, for the analysis of the follow-up results, we used Chi-squared test and Mann-Whitney U-test to test whether there were significant differences between patients that felt safe or unsafe with regard to defined aspects of care (survival time, place of death, contacts with the team, hospitalizations).
To enhance the meaningfulness of our results, we performed a power calculation that aimed at detecting small effect sizes for variables entered into the logistic regression. A sample size of 100 and estimations of small proportions of .25 at 95% confidence were assumed to provide a power of 80%.19,20
Results
Participant Characteristics at Baseline.
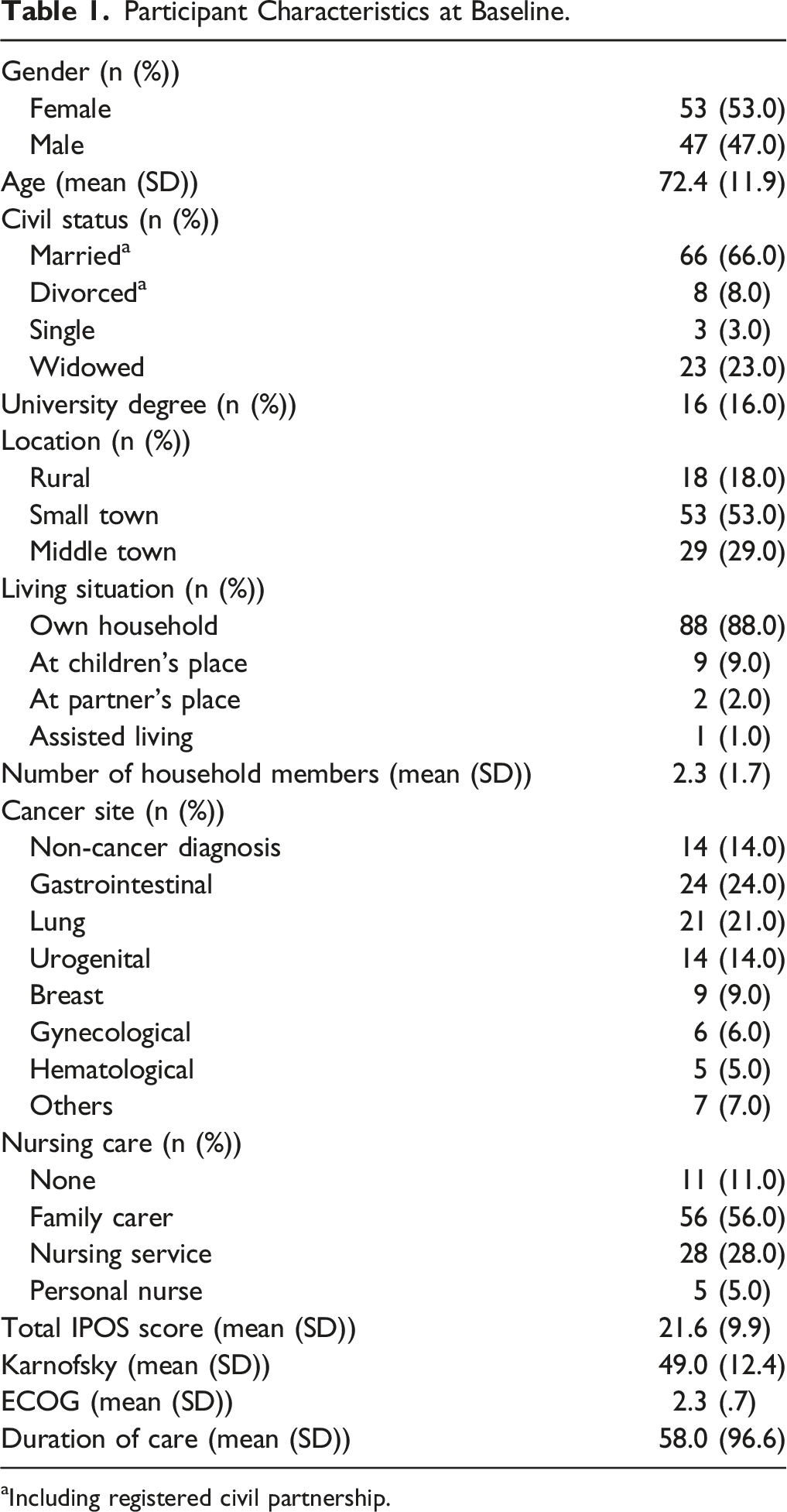
aIncluding registered civil partnership.
Perception of Safety
Perception of Safety According to Subdomains.
Associations With Perception of Safety
Sociodemographic and disease-related variables. As the total IPOS score increased, the feeling of safety decreased in the population studied (OR .88, CI 0.82–.94, P < .001). A reduced likelihood of feeling safe was found with increasing IPOS scores for weakness (OR .49, CI 0.27-.88, P < .05). Figure 1 shows detailed results for sociodemographic and disease-related variables. Patients' odds of perception of safety: patient characteristics.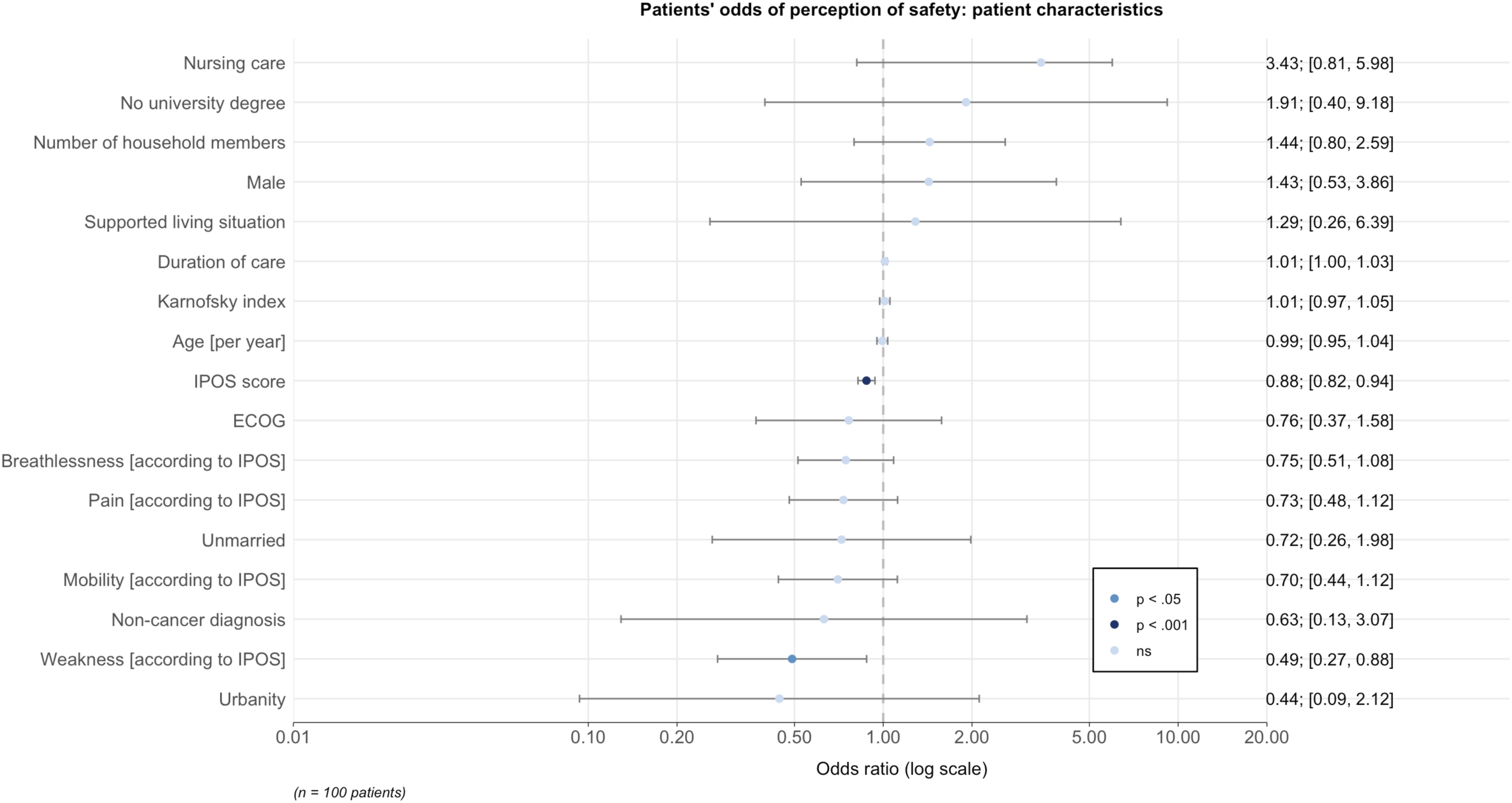
Safety subdomains. Multiple logistic regression analyses indicated that perception of safety was lower when patients felt unsafe in the subdomains of everyday life (OR .30, CI 0.10-.91, P < .05), physical symptoms (OR .19, CI 0.07-.55, P < .05) and physical disabilities (OR .21, CI 0.06-.76, P < .05), psychological symptoms (OR .13, CI 0.04-.39, P < .001), side effects or complications of drug therapy (OR .13, CI 0.04-.39, P < .001) and financial concerns (OR .07, CI 0.01-.73, P < .05). For an overview of associations of safety subdomains with perception of safety see Figure 2. Patients’ odds of perception of safety: safety concerns.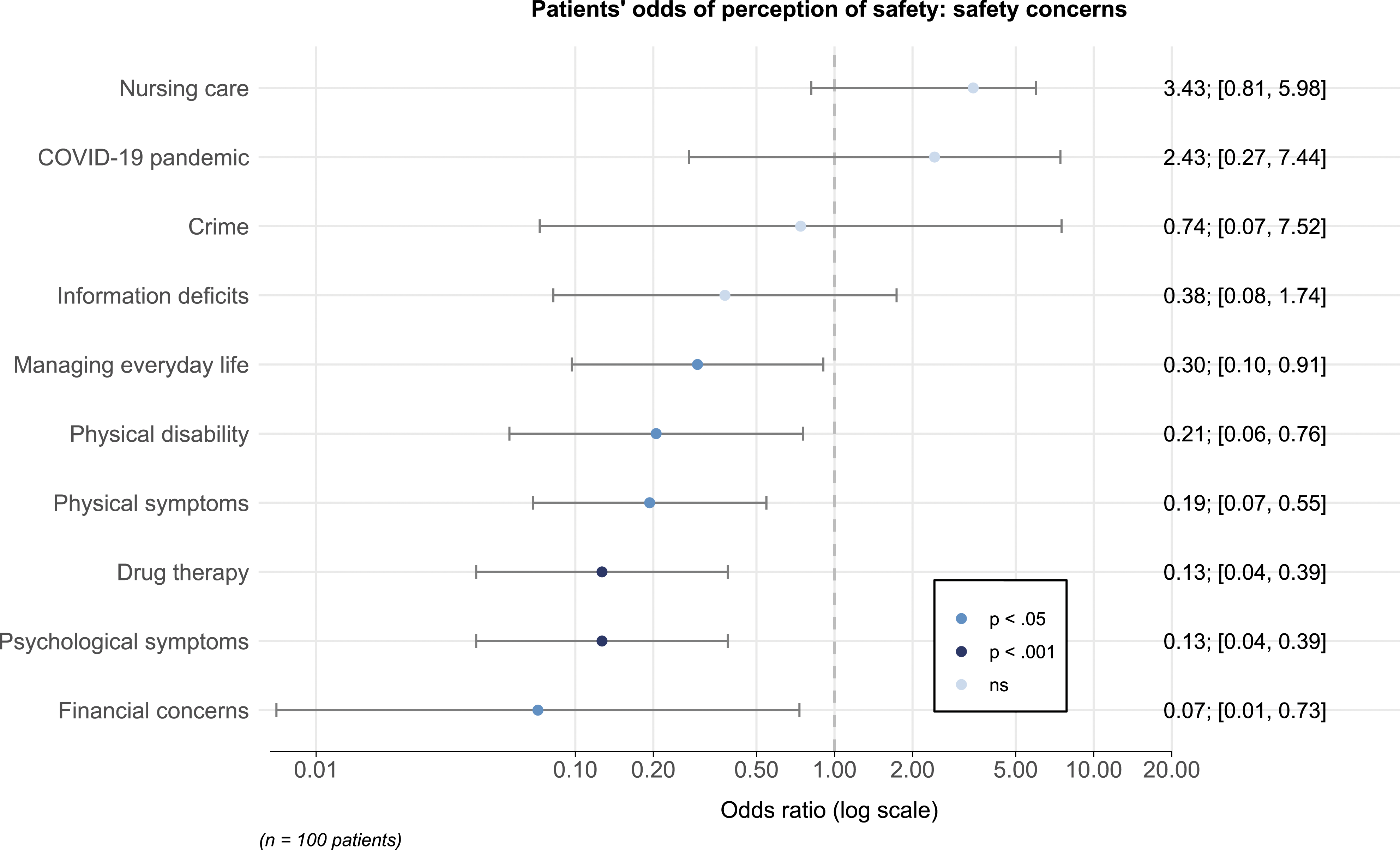
Follow-Up Analysis
Associations of Care-Related Variables with Perception of Safety.
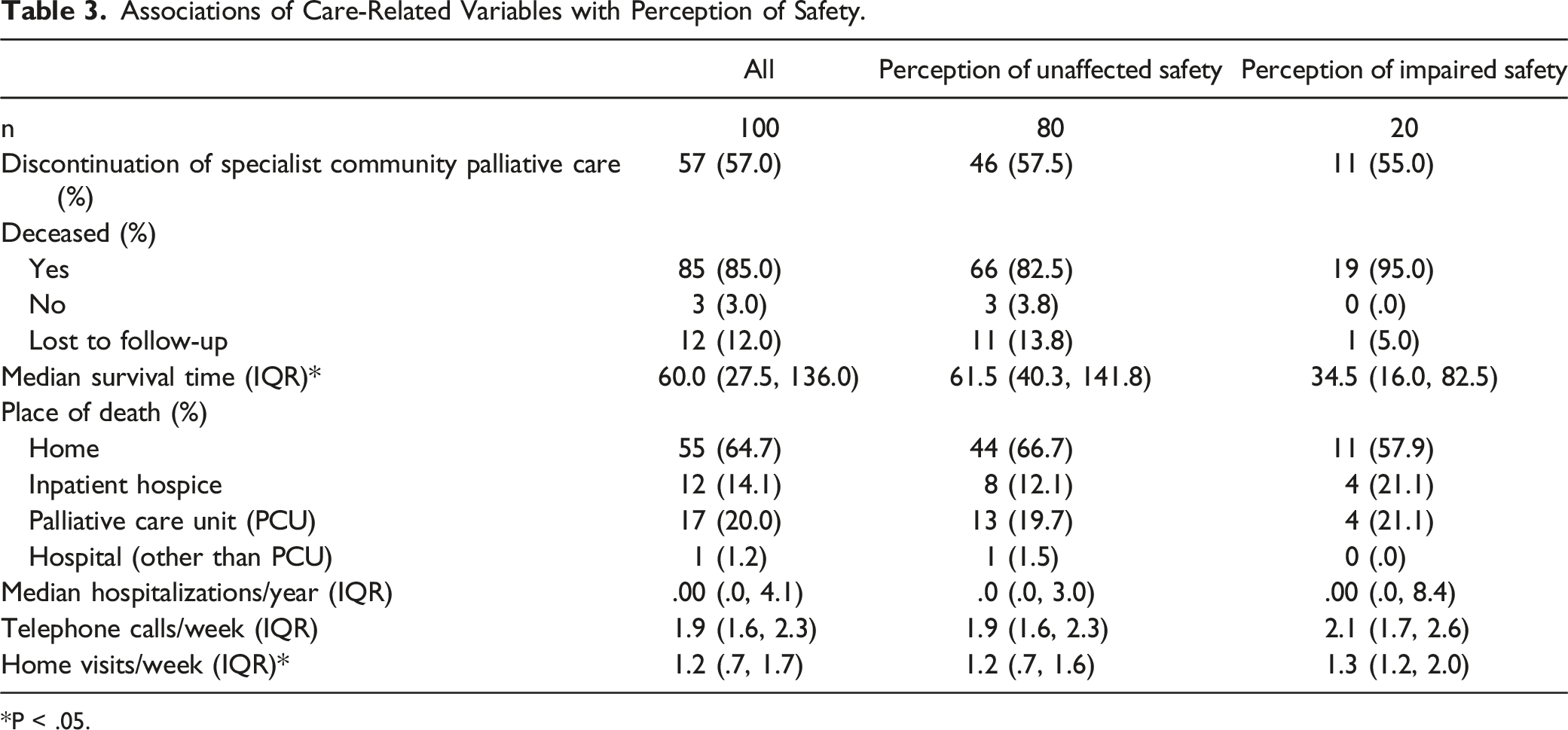
*P < .05.
Discussion
Our study provides important insights into community palliative care patients' perception of safety. Specifically, three major conclusions can be drawn from our research: (i) One in five patients under specialist community palliative care experienced relevant safety concerns and perception of compromised safety is associated with (ii) higher levels of palliative care-related problems according to IPOS sum scores and (iii) shorter survival time.
The meaning of home becomes particularly important at the end of life and is closely linked to patient safety.21,22 Perceived insecurity correlates negatively with quality of life 23 and has been shown to contribute to the vulnerability of community palliative care patients.24,25 In line with earlier research from Sweden, a substantial number of community palliative care patients reported a sense of impaired safety associated with palliative care-related problems, particularly in relation to symptom burden. 25 Our research revealed that patients felt their safety was compromised due to physical disability and symptoms. Considering that poorly controlled symptoms may result in home being perceived as unsafe fostering hospital or residential care admissions at the end of life, 26 this advocates with even more force for effective monitoring of symptoms in routine care, the treatment of which may ultimately promote safety. In addition to physical problems, assessment of psychological symptoms is imperative, given that these had a statistically highly significant effect on the perception of safety in our analysis. In view of this highlighted role of psychological problems in safety considerations and the awareness of the psychological consequences of a compromised sense of safety, 10 the work of palliative psychologists seems of utmost importance for patients’ well-being. The newly acquired knowledge about typical barriers and threats to the perception of safety in the home environment could serve as a basis for reducing possible fears and concerns through psychological interventions. 27
The present study further contributes to previous research showing that grievances in care and treatment can trigger patients' experience of unsafe practices. 28 A significant number of study participants felt unsafe as a result of their medical treatment. Given problematic polypharmacy at the end of life 29 and the growing incidence of medication harm, 30 this concern does not seem unfounded. On the one hand, the relevance of reviewing medications for interactions and side effects is obvious. It is imperative to inform patients about common complications of their treatment in order to mitigate the patient’s impression of losing self-control and to strengthen patient empowerment. On the other hand, the indication of aggressive treatments at the end of life should be thoroughly questioned. In this context, the discourse on medical ethical principles and their practical significance is becoming increasingly meaningful. All too often, decisions still seem to be made on the borderline of medical futility, while the patients themselves are not involved in decision-making processes. 31
In addition, current world events also had an influence on the perception of safety of our study participants. In the course of our study, we had to adapt to the zeitgeist and included the COVID-19 pandemic as a possible safety aspect in our questionnaire. A survey of the general public found that about half of the respondents were anxious about the impact of the COVID-19 pandemic on their lives. 32 Intriguingly, the pandemic triggered a substantial but not exceptionally high level of safety concern among our study participants, with one-third feeling unsafe. In this context, a recent German study found that cancer patients reported comparable levels of anxiety and worry in the face of the pandemic compared to healthy controls —however, cancer patients were more likely to engage in adherent safety behaviours. 33 It remains to be investigated whether the introduction of SARS-CoV2 vaccination led to a change in perspective.
Surprisingly, our study did not find any associations with factors directly related to the home environment, such as supported living situation, number of household members, and urban location—factors that could have indicated a better private and professional support network. Other sociodemographic variables also appeared to be irrelevant to perceptions of safety in our study. Indeed, our results did indicate that it is mainly the direct effects of the diseases and treatment on health that are decisive for perception of safety. Given that Germany has one of the most comprehensive social systems in the world, 34 it was hardly surprising that social aspects played a rather subordinate role among safety concerns. It can only be assumed that in countries with less developed social systems, this is precisely where there remains a significant need for support at the end of life as, for example, perceived financial insecurity was strongly associated with a lower general safety perception. Further research in other countries could be helpful to shed further light on this conjecture to identify country-specific targets for strengthening safety in palliative care.
As a complement to our cross-sectional survey, the follow-up analysis also provided interesting study results. A significant difference in the number of phone contacts most likely does not reflect clinical relevance. Nevertheless, survival time was considerably shorter in patients with a perception of impaired safety. Two opposing hypotheses could be put forward in this regard. Firstly, safety concerns could be an expression of the approaching end of life. This could be conditioned as a consequence of an increase in palliative care-related problems. Secondly, in terms of biopsychosocial models, the burden of perceived insecurity alone could lead to a shortening of life. This may be supported by existing evidence suggesting that psychological distress is associated with poorer survival of seriously ill patients. 35 Further studies to clarify causalities are warranted. In particular, it seems promising to complement the presented questionnaire approach giving predetermined answers with qualitative study designs in order to be able to capture individual patient experiences in depth.
Limitations
Our study has important limitations. First, there is a possibility of a selection bias as for one we could not recruit consecutively and particularly at the time of the pandemic, people who felt unsafe might have been inclined to refuse participation. Moreover, gatekeeping by the care team is likely considering that their assessment of patients’ physical and mental condition was fundamental for inclusion. Second, even though cognitive interviews were used to establish face and content validity, our questionnaire has not been validated and may be subject to measurement error, so conclusions cannot be drawn with absolute certainty. Third, when the individual safety subdomains were queried, there was no explicit screening for the occurrence of corresponding problems, so that this could have led to an underestimation of the influence on the perception of safety. Lastly, our study was a single service-analysis. As care practices, but also patient populations may vary between services and geographical regions, this may limit the generalizability of our findings.
Conclusion
Our study gives healthcare professionals deeper insights into patient-reported problems in establishing patient safety. Understanding what it means for patients not to feel safe and recognizing situations that raise safety concerns is an important contribution to how patients' needs should be adequately catered for at home. Further research should address primary and secondary prevention interventions to improve the quality of care at the end of life.
Footnotes
Acknowledgments
We would like to thank the specialist community palliative care team of Giessen for their valuable support in identifying eligible study participants. Special thanks to David Pedrosa for his support in the statistical analysis of the data.
Author Contributions
A.P. is responsible for the conception of the study. All authors were involved in the questionnaire design. A.P. and A.B. conducted the cognitive interviews. A.B. conducted the cross-sectional survey. A.P. carried out the analysis of the data and drafting of the manuscript. All authors were involved in the interpretation of the data and revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our study was approved by the institutional research ethics committee at the Faculty of Medicine, Justus Liebig University Giessen (AZ 136/19).