
Abstract
Background
Despite the general preference to die at home, many deaths occur in institutionalized settings. While biomedical interventions to ameliorate end-of-life (EoL) suffering have advanced, the end-of-life care (EoLC) environment is less understood as a means of palliative support.
Objective
This exploratory study considered the implications of clinical EoLC environments (facility buildings and their adjacent areas), aiming to understand how these designed spaces may be improved to better support experiences for patients, families, and staff.
Methods
Using an ethnography-driven approach, field observations (including participant commentaries) were captured at a standalone hospice and a palliative care ward at a general hospital. These were supplemented with semi-structured interviews. Content and thematic analyses were performed based on an interpretive-descriptive paradigm. Finally, informed by a review of field literature, analyses of all data were inter-related, and an interpretation was built to highlight key design considerations.
Results
Through the analysis, 6 socio-spatial dimensions of EoLC facilities were identified (locational contexts; service administration & management; common spaces; private spaces; in-between spaces; and nature-integrated spaces) as guiding concepts to appraise and improve such settings.
Conclusion
Physical, emotional, and social wellbeing at the end of life is coalesced in and made visible by the designed environment. Therefore, evidence-based design serves as an important non-clinical intervention in such settings; however, patient involvement in such research remains difficult. Future scholarly research, new building schemes, and renovation projects should further examine the socio-spatial functions of clinical EoLC environments and investigate the challenges surrounding patient engagement within this domain.
Keywords
Introduction
The relationship between built space and public health is a long-established and well-studied one.1-4 In this context, the field of evidence-based design has attempted to “carefully observe, quantify and analyze the way people use buildings” 5 in order to understand its implications for health quality outcomes. Much of this enquiry has focused on patient experiences of wayfinding in healthcare spaces, 6 not only highlighting the topical relevance of design in clinical sites but also indicating critical knowledge gaps. One commonly overlooked realm is the end-of-life care (EoLC) setting, which may include hospital-based palliative wards, residential hospices, and—although not primarily intended for EoLC—long-term care (LTC) facilities and other types of care homes where death may occur outside the home.
The design of residential and in-patient care units has been explored over several decades, generating various practice standards and guidelines for facility design.7,8 Yet, the implementation and further advancement of this knowledge is far from universal. Moreover, there has been little scholarly research—outside of isolated design projects—on how EoLC facilities align with patient, caregiver, staff, and community needs and expectations, many of which are non-clinical in nature. Over the last two decades, only two major texts have consolidated and presented developments in EoLC design; namely: Verderber and Refuerzo’s (2003) Innovations in Hospice Architecture 9 and Worpole’s (2009) Modern Hospice Design. 10 Recent research continues to suggest that social and spatial elements are pertinent (and often, interdependent) within EoLC facilities; however, the evidence base on these aspects is far from comprehensive.11,12
Moreover, cultures of death and dying have shifted considerably over time, 13 as have the places where people spend their last days, with many deaths occurring in different EoLC settings. 14 Despite the common preference for and upward trend towards dying at home in the United States (30.7%), a substantial proportion of deaths still occur in institutions such as hospitals (29.8%); nursing facilities (20.8%); and hospice facilities (8.3%). 15 In Canada, over 60% 16 and in the United Kingdom, over 41% 17 of deaths still occur in hospitals. While hospital deaths may decline in future with the increased utilization of home-based hospice care, other institutional settings like nursing homes, hospices, LTCs, other care homes, and dementia-friendly residences may become increasingly common locations of death.18,19 In some cases, patients with comorbidities and complex care needs may find it more comfortable, or otherwise desirable, to spend their last days at a facility, 20 and often, professional care provided at such sites may help ease family caregivers' burdens. 21 Overall, the need for specialized EoLC settings and services is expected to rise steadily over the next 50 years. 22 Accordingly, it is essential to develop evidence-based design responses and strategies to better support the communities and individuals who use these sites.
The objective of this study was to examine the designed (and designable) characteristics of EoLC settings and draw out socio-spatial implications for EoLC experiences for patients, families, staff, and broader communities who interact with these locations. The terminologies for categorizing and describing diverse EoLC settings differ with geography and culture (for e.g., the word ‘hospice’ may indicate a type of care rather than a physical setting in some countries). While field sites used for data collection will be described shortly, the terms EoLC environment/setting/facility are used in the paper to indicate the diverse settings to which this discussion may be extended.
Methods
Conceptual Approach/Methodological Framework
This study utilized an exploratory-observational approach, which is an interpretive descriptive form of qualitative enquiry. As an inductive analytical methodology, it is used increasingly in health research to answer experience-based questions of interest to clinical research and practice. 23 It aims to generate “a coherent conceptual description that taps thematic patterns and commonalities believed to characterize the phenomenon that is being studied and also accounts for the inevitable individual variations within them.” 24 Given the inductive nature of this approach, the key elements that shape the EoLC environment are intended to be derived from the dataset, as opposed to deductive approaches where a more rigid framework of terms may be pre-determined to capture or eliminate certain data. However, recognizing the need to form an observational and interview strategy, some open-ended concepts were identified from field literature (for e.g., room arrangements; light and fresh air; exterior and interior materials; differential use of space by patients, caregivers, and staff; navigability of layout; domesticity and comfort; sensorial needs; grieving; privacy; etc.). These served as broad sensitizing ideas, with the expectation that many elements may be expanded upon or modified as new issues of interest become apparent over the course of the study.
Depending on the topic of investigation, data collection and analysis tools may vary within interpretive description. In this study, rapid cycle or focused ethnographic methods were employed; these primarily involve field observations that can be completed in a very short time-frame, which may be supplemented with different methods, such as interviews, document analysis, and others.25,26 Rapid/focused ethnographies have been found particularly suitable in certain situations where the subject of interest is narrow, the setting being studied is highly specialized or small in scale, the groups/individuals being observed are very few, or resources are insufficient for an extensive investigation. Such situations are certainly not limited to, but frequently seen in, highly safeguarded zones with restricted access where other types of research could be ethically or practically unfeasible, unsafe, or uncomfortable for the researchers or the participants 27 (for e.g., in high conflict zones, 28 among marginalized or stigmatized groups, 29 and in contexts of severe or critical illness 30 ). Thus, given the heightened vulnerability of patients and families in the last days of life and the modest scope of this study, a short observation cycle was found most appropriate.
Data Collection
Given the complex safeguards around research activity in medicalized settings, 31 particularly in sensitive locations like EoLC facilities, a convenience sampling strategy was used to select study sites and recruit interview participants. The observational phase of the study was conducted at two sites in Alberta in Canada: a small, standalone hospice in a suburban area and the palliative ward of a large general hospital in an urban centre. Rapid ethnographic observations—which need a shorter duration of fieldwork and afford the methodological flexibility required in specialized environments 32 —were conducted over 3-5 days at both sites. For gathering comprehensive data and ensuring transferability, extensive field notes and photographic records were generated, enabling a “thick description” 33 of the study sites. These data were supplemented with 60-90 minute semi-structured interviews, conducted with onsite staff (n = 4), a healthcare manager (n = 1), and a provincial health system decisionmaker (n = 1). Field observations additionally captured comments from the residents (patients and families) as well as staff, whenever communication was initiated by them (unprompted).
Data Analysis
As noted earlier, some open-ended concepts were derived in advance from a preliminary review of relevant literature on death and dying, evidence-based design, and palliative care to guide data collection. During the first stage of analysis, these were used as initial codes to organize, describe, and sort the data. Content analyses were performed on observational field notes and photographic materials, with further codes and themes derived inductively from the dataset. Dependability and reflexivity were ensured by maintaining decision trails and memos. 33 Audio recordings of interviews were transcribed verbatim and thematic analyses were performed through an iterative process of coding to identify recurrent concepts and categories. The coding process and final interpretations were checked by another researcher who was not involved in data collection or extensive analysis, with differences resolved through discussion and consensus. Lastly, using insights from field literature (discussed in a conceptual paper published elsewhere), 34 analyses of all gathered data were interpreted together. In particular, three sources of literature9,10,35 guided the inter-relational interpretive phase to formulate key considerations for EoLC facility design.
Findings and Discussion
Illustrative Quotes — Socio-Spatial Considerations for End-of-Life Care Facility Design.
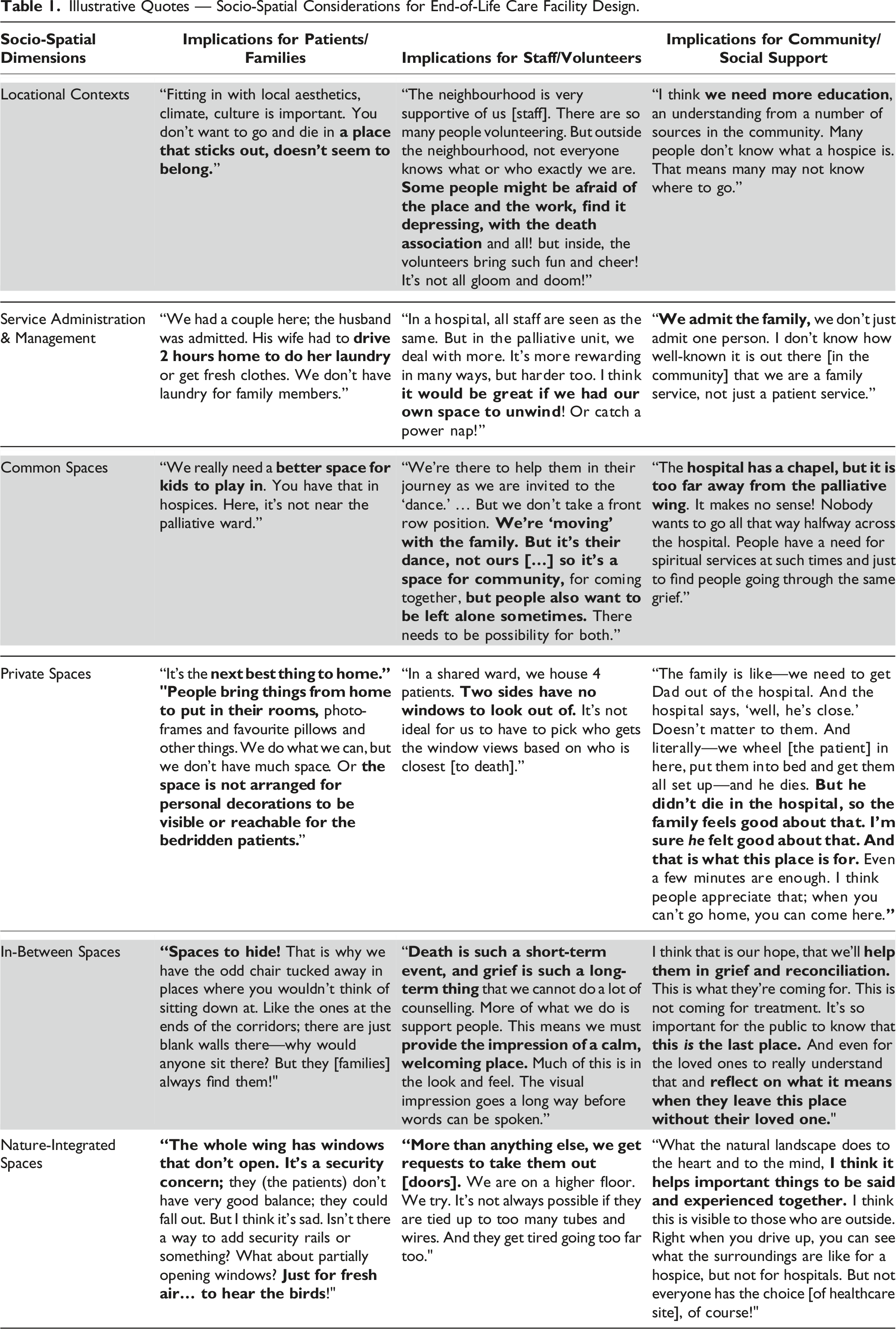
Overall, the findings indicated that EoLC facilities are complex spaces requiring careful consideration of how socio-spatial dimensions affect EoL experiences, and importantly, interact with each other. While it may not be realistic or necessary to address all dimensions at every EoLC setting, these findings are relevant for designing future EoLC facilities that better support the communities and individuals they serve. A detailed analysis was performed on field data to better understand the implications for EoLC facility design, pulling together and building upon prior research,
9,
10,
35
and resulting in the development of 6 socio-spatial dimensions. These may be regarded as guiding concepts to alert and sensitize communities, healthcare providers, EoLC researchers, and facility designers towards the relationship between the EoLC setting, death-related experiences, and perceptions of supportive care delivered and received within. Each of these dimensions are discussed briefly below, with a view to generating widely applicable overarching themes. (i) Locational Contexts: Architectural congruence with surrounding areas and the public identity of the EoLC facility emerged as important factors affecting community knowledge, acceptability, and support in this dataset. Given the vast cultural, demographic, socioeconomic, and logistical differences across sites, advance and ongoing consultations with stakeholders can help determine and monitor local needs, challenges, acceptability, and overall community support for the EoLC setting. Furthermore, hospices in rural and semi-urban residential areas are found to face challenges in accessing allied medical resources, major transport networks, and recreational or commercial establishments. While palliative wards within large general hospitals in urban areas often enjoy better social connectivity, they may face other challenges relating to noise from adjacent settings, crowdedness, and less access to the natural landscape. The use of sound buffers, climate-appropriate building materials, and small-scale intuitively navigable layouts may help break unpleasant associations with clinical settings that often use complex wayfinding and signage systems. (ii) Service Administration and Management: The front reception—serving as the central hub connected to all other parts of the facility—is important for streamlining administrative tasks. Nurse stations should, therefore, be situated close to the reception, while balancing the need to remain accessible from patient rooms. Additionally, field data indicated that despite regular bedsheet and gown changes occurring in EoLC facilities, hospital-based palliative wards—in contrast to standalone hospices—may not have their own laundry and linen room, instead sending their laundry out to the main site for cleaning. The provision of family laundry rooms may help ameliorate undue stress for those staying onsite with the patient for several days or weeks. Another overlooked area is the need for designing staff respite areas for spending time away from the bedside, eating meals with colleagues, or enjoying quiet moments; these are crucial to help protect against emotional and physical burnout. Similarly, well-organized spaces should be allocated for community volunteers to afford visibility to these highly valued and frequently under-appreciated workers. (iii) Common Spaces: The reception desk and waiting area form the first points of contact between patients and healthcare facilities, helping establish trust and reassurance. While this initial impression is even more important in an EoLC setting, it was found that hospital-based palliative ward receptions may reflect a cold and detached appearance, compared to the approachability of a standalone hospice. In contrast, hospice settings often use murals, tapestries, sculptures, and paintings to instil warmth, disrupt visual monotony, and animate an otherwise tedious clinical realm. It was also found that donations form an important part of community support, with gestures of thanks and remembrance seen in the form of donor walls, outdoor name plaques, and commissioned art. Spatial layouts should, therefore, anticipate these needs and be able to accommodate tokens of remembrance and gratitude. In this study, the standalone hospice site incorporated child-safe play areas as well as friendly gathering spaces for grieving adults, while hospital palliative wards conspicuously lacked these. Similarly, preparing and sharing meals was identified as crucial for strengthening emotional connections and triggering social interaction. Eating areas should thus be designed to offer flexible levels of privacy, with provision for both individual as well as communal cooking and dining spots. Some residents and family members also voiced requests for a reading room with internet-enabled computers and printing and scanning facilities, while others mentioned undesirable restrictions on bringing in pets to visit the patient. In times of trauma and vulnerability, animal therapy may restore emotional wellness in human beings; hence, designated pet visitation areas close to patient rooms could help offset hygiene, noise, and safety concerns, while allowing patients and families much valued emotional support from animals. (iv) Private Spaces: Space and budget permitting, each patient should have their own room, conceived using culturally neutral and universal design vocabulary—although this remains challenging in high population density areas served primarily by hospitals that have few palliative beds. In this study, secure windows (with fall protection features) that overlook garden spaces and let in sunlight emerged as the most common need in patient rooms, followed by enough storage space for families who often spend uncertain lengths of time onsite. Patients also noted problems staying asleep due to the grating sounds of pushcarts and wheelbeds caused by the absence of seamless floor tiles outside their rooms. In shared patient rooms, privacy was reported to be of substantial concern. Where shared rooms are unavoidable, it is suggested that partitions employ sturdy, non-translucent, and noise-minimizing materials. No individual patient sections in a shared room should be completely cut off from the windows; unfortunately, windowless patient areas were a key concern discovered during field observations. In addition, bathrooms affect patient perceptions of dignity and autonomy, and may inadvertently signify physical inadequacy and loss of control to terminal patients. Accordingly, mirror features should be discreet and not occupy too much space, as witnessing a continual decline in one’s bodily appearance with every bathroom visit could prove distressing. A basin placed at wheelchair height (in addition to a regular-height sink for family members) should be considered if there is enough space. Some family members noted the added burdens of driving home to shower or do laundry (often for long distances) and feeling concerned about missing the moment of their loved one’s death while away. This indicates that shower and laundry facilities for use by family members staying overnight are essential, given the precarious condition of the patients they accompany. Finally, nurses noted that a cleaning space with a hand-held water jet, separate from the patient bathing and showering areas, should be designed to rinse soiled linen and bedpans; for example, a dishwasher-equipped anteroom constructed near patient rooms could aid in facilitating these tasks with optimum hygiene and minimal discomfort. (v) In-Between Spaces: Narrow passages that take a long time to traverse are disorienting and reinforce the idea of large, institutionalized spaces. Corridors are not entirely avoidable in every type of building, but their limitations can be overcome by making them shorter and wider, with visual and tactile interest generated on the walls through art, plants, lighting, and textures. Natural materials such as wood and stone should be used to create intimate, personable, and homely environments wherever possible—especially in hospital palliative wards. In this dataset, a pertinent need was identified for spaces to retreat to and reflect in away from caregiving duties, both in privacy as well as to seek social connection with others. Such spaces are noticeably missing in typical hospital designs; for example, the chapel in the hospital-based field site was found to be located too far from the palliative ward. Non-denominational, accessibly designed meditative spaces—ideally with views, if not access to—the natural landscape appear to be much needed. Strategic spatial interventions, such as a discreetly placed chair in an unfrequented spot, can further grant the user a temporary escape from the continuum of stressful events. Lastly, rooms devoted to grief counselling should ensure privacy and security by visually and acoustically separating them from high activity zones, thus ensuring that people feel safe to cry, express anger, or remain silent in vulnerable moments. (vi) Nature-Integrated Spaces: Air quality and circulation are key considerations for terminally ill patients who may suffer from nausea and dizziness due to medication, sanitizing agents, or simply as a result of debilitating illness. Yet, patient rooms observed in this study did not necessarily have windows if located in a hospital ward, and where present, windows were often designed as fixed/picture windows to prevent falls. With many modern advancements in universal design, anti-fall security mechanisms for windows should be tested and integrated within EoLC facilities to improve natural ventilation and reduce the feeling of confinement. Given the therapeutic effects of nature, indoor landscaping with strategic exit points to go outdoors should be located at regular intervals across the facility. Relatedly, water has long held an enduring place in human consciousness and is associated with palliative benefits for the mind and the body. If open ground is available, landscaping could incorporate outdoor ponds and waterfalls. If space is limited, as in a hospital-based palliative setting, indoor aquariums or fountains can be used to create a peaceful, self-contained oasis. Comfortable seating and wheelchair accessibility should be provided near as many of these as possible. Being able to physically access nature and natural elements was found to be the most commonly expressed, and surprisingly, the least addressed need at study sites.
Limitations
This study has several limitations to report. The sampling strategy and exploratory methods did not allow for data saturation; however, triangulation was achieved by combining several types of ethnographic data: (1) field notes; i.e., observations and commentary; (2) photographic records; (3) in-depth interviews. In addition, concepts from the broader literature were applied throughout the preparatory and interpretive phases of the study. Further, given increased vulnerability in their final days, interviewing patients/families directly was unfeasible; therefore, the findings do not necessarily represent the experiential needs of all individuals. This limitation was partially addressed through field notes—which captured interactions between patients, families, and staff—and through unprompted, informal conversation initiated by onsite individuals. Lastly, recognizing the vast variations in the form and organization of diverse EoLC facilities, the findings are not expected to be applicable to every setting. To account for this, after preliminary data analyses, the 6 emergent dimensions were further refined using knowledge from evidence-based design literature concerning a range of EoLC setting-types and best design practices in the field. It remains possible, however, that some aspects of socio-spatiality in EoLC facilities may have been missed.
Conclusion
Overall, this study indicates that the designed environment is a fundamental, but frequently overlooked, area for situating non-clinical interventions that support patient, family, and staff experiences at the end of life. Spatial and social elements appear to be heavily entangled, and the experiences of diverse groups (patients, caregivers, and staff) are found to shape each other. Managing the vulnerability of patients/families remains difficult in conducting evidence-based design research in EoLC spaces. While the severity and type of illness is likely variable across patients and some may have longer to live than others, it is not ethically or practically possible to regard certain individuals as less vulnerable and selectively subject them to more intrusive investigations or intensive involvement activities that are typical within design practice. Larger-scale and longer-duration studies are necessary to reveal how such challenges can best be overcome while respecting patient privacy and organizational regulations relating to restricted access.
To summarize, further evidence is needed to better understand how socio-spatial functions manifest in various EoLC environments and the ways in which they affect experiences of death and care for those within. Examining ethical and methodological complexities in conducting such studies is necessary for developing and evaluating context-appropriate and adaptable research methods in this domain. Finally, community engagement throughout the design process should be explored more deeply to generate rich contextual knowledge about local needs and perspectives; encourage community involvement in and social ownership of EoLC facilities; and increase the cultural visibility of death and dying.
Footnotes
Acknowledgements
The author thanks Prof. Aidan Rowe (Department of Art & Design, University of Alberta) for aiding in the coding process and providing overall guidance during the conceptual and interpretive stages of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
This study received ethics approval from the University of Alberta Health Research Ethics Board (Approval ID Pro00068687).