
Abstract
Purpose
The purpose of this study is to determine which element of advance care planning (ACP) - an advance directives (AD) document or an end-of-life discussion between patient and family (DwF), if any—improves the likelihood of cancer patients’ attaining their preferences regarding treatments in the last month of life and dying in the place they prefer.
Methods
First-degree relatives of deceased cancer patients, interviewed by telephone, were asked if the treatments the patients received in their last month of life and their place of death corresponded to the patients’ preferences. Nominal logistic regression analyses were conducted in search of significant association between having an AD document and/or conducting a DwF and patients’ treatment and place of death in accordance with their preferences.
Results
491 deceased patients were included in the study. Their average age was 68; 52% were women. According to 32% of the relatives, the patients’ treatment in the last month of life was aligned with their preferences and 55% said the patients had died in their preferred place. Only 16.5% had an AD document, 58.5% only discussed their treatment preferences with relatives, and 25% did neither. DwF and ability to speak until last week of life were significantly related to receiving treatment consistent with patients’ preferences. Dying where the patient prefers is significantly associated with having an AD and a DwF, with an AD yielding higher odds.
Conclusion
A multifaceted interconnection exists between the two elements of ACP in attaining cancer patients’ wishes and abetting better end of life care.
Introduction
The debate over medical decision-making at end of life (EOL) has been on the medical, legal, ethical, and public agenda for almost half a century.1-3 Although advance care planning (ACP) has long been thought to improve compliance with patients’ preferences at EOL, innumerable studies and projects indicate that the issue has not yet been settled.4-6 Advance care planning is an ongoing process that helps individuals share their preferences regarding future medical care.7,8 Its first element is a legal advance directives (AD) document (a living will) that specifies individuals’ care preferences if they can no longer express them. The second is the designation of a surrogate decision-maker (granting of power of attorney); the third is a discussion between patients and family members as to the preferences of the former (Discussion with Family—DwF),9,10 as family members often attend cancer consultations together with patients 11 and most cancer patients prefer to have their families participate in the decision-making process.12-15 In many counties, the designation of a surrogate is included in the AD document.
Advance care planning may be especially important for cancer patients because numerous complex caregiving decisions are made during their illness. Advance care planning is found to be associated with improved quality of EOL, less use of aggressive treatments at EOL, and a better chance of receiving EOL care consistent with patients’ preferences.16-23 However, the impact of ACP is usually studied and understood en bloc, bundling the discussion with the documentation of goals and preferences for future medical treatment and care. Therefore, the outcomes of care are attributed to the entire ACP process rather than to each of its elements separately. 17
The attainment of patients’ treatment preferences is key to quality patient-centered EOL care. 24 The alignment of care with individuals’ preferences, including those relating to place of death, is one of the most common indicators of such care.16,25,26 Thus, the purpose of this study is to determine which element of ACP -AD or DwF, if any -improves the likelihood of cancer patients’ attaining their preferences regarding treatment in their last month of life and dying in the place that they prefer.
Methods
Research Population
The target population of this retrospective cross-sectional study is comprised of Israeli citizens aged 23+ who died from cancer three to 6 months before the study. The consecutive names of 1000 cancer patients who had received care at large 4 university medical centers in Israel, including details of their primary first-degree relatives, were retrieved from the centers’ medical records. The actual research population was composed of these relatives. The relatives were contacted by telephone, advised about the aims of the study, and asked for their consent to be interviewed by telephone. Of the 1,000 contacted, 491 (49% of the study target population) agreed to participate. More than half of those who refused (28% of those contacted) said that it was too difficult for them to speak about the last period of their loved one’s life, whereas 23% said that their loved one’s condition had deteriorated so quickly that they remembered few details.
Methodology
Telephone interviews using a closed-ended structured questionnaire were conducted by skilled interviewers who received half a day of detailed training from the investigators, exercised a simulation of the questionnaire, and were under the investigators’ continuous guidance and supervision. Before each interview began, the interviewers read out the consent document and the participants reconfirmed their consent to be interviewed. The study was approved by the 4 medical centers’ institutional review boards (Helsinki committees).
Research Variables
The dependent variables in this study were two: Did the care the decedent patients received in their last month of life correspond to their preferences? and did the patients die in the place that they preferred? The primary independent variables were also two: Did the decedent patients have an AD document and had they discussed with the interviewee the care they wished to receive at EOL? The answers for both were yes or no.
Data Analysis
The data were input to IBM SPSS (Version 25). Descriptive statistical indicators were analyzed first; a bivariate analysis followed. Nominal logistic regression analyses were used to estimate the odds ratios of each of the two dependent variables with the two primary independent variables. This is the most appropriate method for use in comparing a three-point dependent variable. 27 Receiving the preferred treatment was defined with three categories (yes, partly, and no) and dying in the preferred place was defined with two categories (yes, no). The covariates were age (a continuous variable), gender, years of education, economic capacity (the household’s ability to make ends meet: with great difficulty, with some difficulty, fairly easily, and easily), and the ability to speak until the last week of life. The independent variables were assessed for the presence of significant multicollinearity; none was found.
Results
The average age of the deceased cancer patients was 68 (SD (14.3, 52% were women, about half had 13 years of education or more, and 51% of their households made ends meet fairly easily or easily. About 43% of the patients were totally or almost totally dependent on assistance in Activities of Daily Living. 31% of the patients died at home, 54% in hospital, and 15% in an inpatient hospice.
The family members’ average age was 55 (SD 14.4). 59% were women, 40% were patients’ spouses, 40% were offspring, and the rest were other. About 32% of relatives said that the treatment patients received in their last month of life matched their preference, 26% said it did so partly, 17% said that it did not, and 25% could not answer. More than half (55%) said that the patients had died in the place of their preference, 24% answered in the negative, and 21% could not answer.
Only 16.5% of the patients (81 people) had an AD document and 58.5% had none but discussed their care preferences with their family. Most of those who had ADs (77 individuals) also discussed their preferences with family, meaning that 75% either had an AD document or held a discussion or both. The others did neither.
Characteristics of deceased cancer patients by outcome indicators (percent), N = 491.
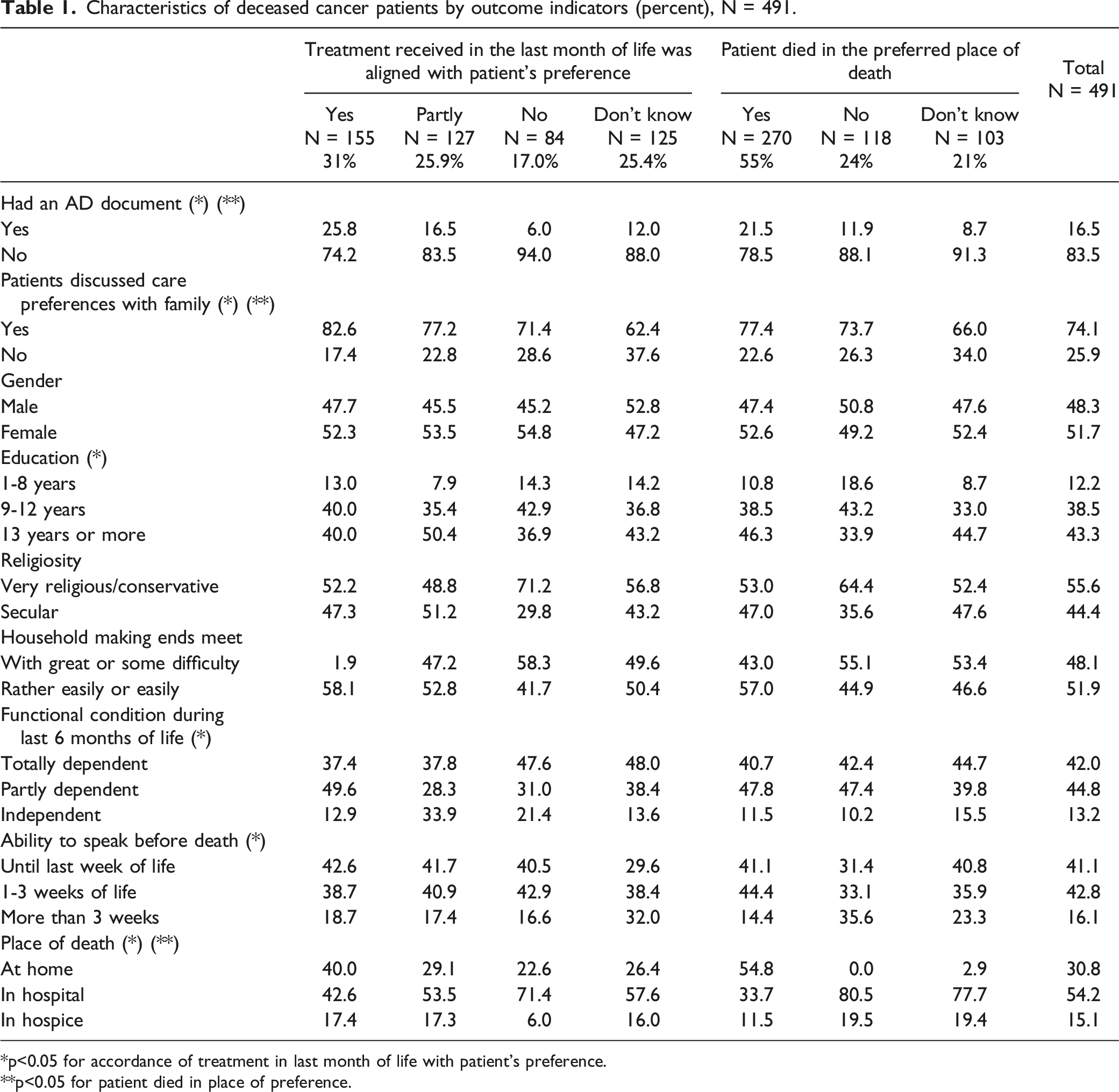
*p<0.05 for accordance of treatment in last month of life with patient’s preference.
**p<0.05 for patient died in place of preference.
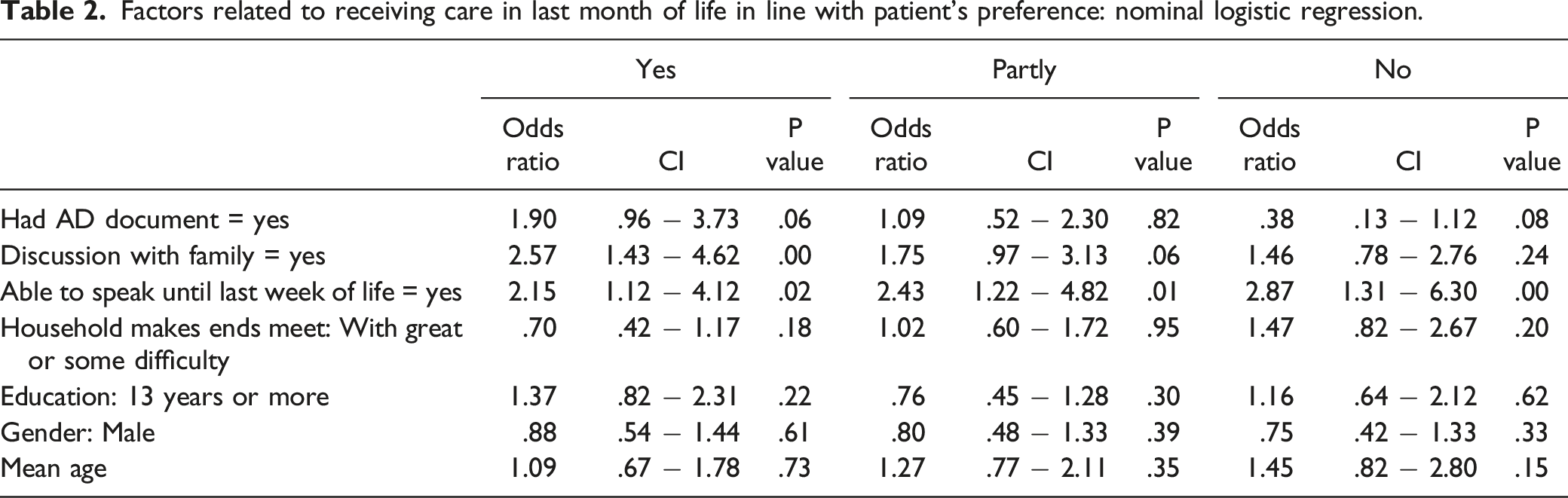
Factors related to receiving care in last month of life in line with patient’s preference: nominal logistic regression.
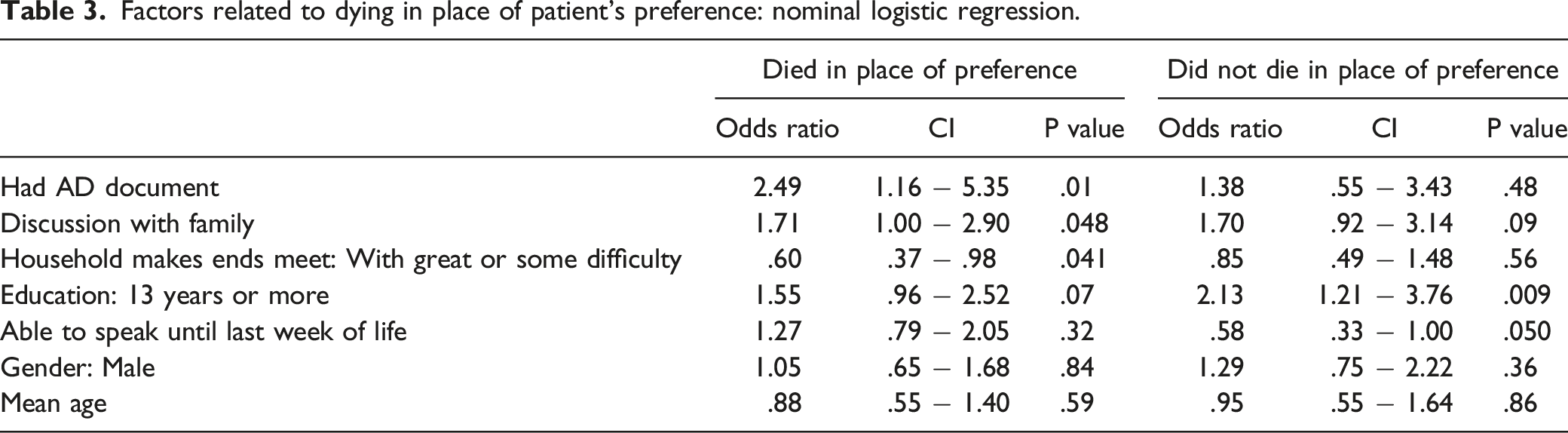
The odds of dying in the place of patient’s preferences were found to be significantly related to having an AD document, holding a DwF, and the household’s being strongly able to make ends meet. These odds, however, are higher when an AD document exists than when a DwF is held. Only higher education and patient’s ability to speak until the last week of life are related to not dying in the preferred place. Age, gender, and education were not found independently associated with dying in the preferred place.
Discussion
Factors related to dying in place of patient’s preference: nominal logistic regression.
In view of this complex reality, we found that receiving EOL treatment consistent with patients’ preferences is significantly related to DwF but not to having an AD document, and to their ability to speak until the last month of life. Indeed, cancer patients report that the most important element among their EOL wishes is to discuss them with family2,16,34 and a recent study in Israel found that the main enabling factors in completing ACP is open communication with family members. 35 In a systematic review of the relationship between EOL discussions about care planning, evidence was found that an EOL discussion is associated with less aggressive or intensive care as EOL approaches, 36 and it was concluded in another study that patients and caregivers who prepare for EOL by carrying out comprehensive ACP have the potential of improving EOL outcomes. 37 In other studies, it is found that while both elements improve the odds of receiving care in accordance with patients’ preferences, having EOL discussions, rather than AD documents, is the key predictor of higher-quality EOL care as perceived by bereaved families.38,39 This finding reinforces a systematic review that found extensive ACP interventions possibly more effective than written documents alone. 13 In another systematic review, it is suggested that ACP derives its value from being undertaken more as a family-centered and social process than as a personal directive. 21 Namely, ACP is not simply the manifestation of patients’ choice but the result of complex and dynamic interaction between patients and their close environment, including family and healthcare providers.
The picture as to dying in the preferred place of death is somewhat similar to that regarding the honoring of care preferences. Both AD documents and DwF are associated with dying in place of preference, but here the odds of this outcome are greater with ADs. Perhaps dying in the preferred place is less susceptible to variations than are treatment preferences because the burden of symptoms, interrupted by worsening, is much more contingent upon fluctuations in the illness trajectory at EOL. In a systematic review of the stability of patients’ preferences for dying at home, it was found that most patients do not reconsider this as their illness progresses. 30 In another systematic review, it was found that more seriously ill patients and those with ACP most commonly have stable preferences for future care. 40
It is especially noteworthy that one-fifth to one-fourth of family members were unable to state whether their loved ones had received the care they desired and died in their preferred place of death. We did not ask why this was so, but the fact that two-thirds of them discussed care preferences with their loved ones may hint at the families’ frustration over being unable to honor their loved ones’ preferences even though they knew about them.
This study has several limitations that deserve consideration. First, due to institutional review-board regulations, information about those who did not consent to participate in the study could not be collected. Therefore, we could not assess whether consenting family members differed significantly from those who did not consent. Second, although family members were interviewed close to the patients’ death and information from proxies abounds in EOL research, memory problems may create recall bias, social-desirability bias, and potentially misunderstanding. Thus, when family members said they could not answer a question, many reasons for this may have been in play. Even though family members of cancer patients may try to do the right thing, the emotional distress that they face may plunge them into anxiety that persists long after the death of their loved one. In addition, cultural, racial, and spiritual needs and values may influence family members’ responses. 41 However, interviewing bereaved families in order to explore the quality of care up to the last stages of life is common in research40,42-44 and it was found in a systematic review that two-thirds of next-of-kin surrogates accurately knew patients’ EOL care preferences. 45 Third, we had insufficient information on patients’ clinical characteristics such as types of cancer, the speed of disease deterioration at EOL, and family members’ characteristics that may have influenced the honoring of patients’ preferences. Future research should focus on disease-trajectory factors that may affect the honoring of patients’ preferences and quality of death. Finally, although the study was performed on a large national sample, the results are limited to cancer patients in Israel. Future research should continue to examine the concordance of the different elements of ACP and the attainment of preferred care outcomes in order to generalize the results to cancer patients in other countries and in different cultural contexts.
In conclusion, this study adds to the recognized evidence of the importance of ACP in cancer patients’ EOL as a process that improves the attainment of their care preferences. It also shows that although even one element of ACP is better than none, DwF has a stronger impact on attaining EOL care preferences than does an AD document alone. Also illuminated in this study are the multifaceted interconnections of the different elements of ACP, indicating that the realization of all elements abets better EOL care for cancer patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Israel National Institute For Health Policy Research (R/42/2017) and Minerva Center for Interdisciplinary Studies of the End of Life from Tel Aviv University.