
Abstract
• Palliative care is known to decrease the cost of inpatient hospitalization • Early initiation of a palliative consult can impact overall utilization of high-level care in the inpatient setting
• It adds a process to influence physician referral timing to achieve an earlier palliative care consult and associated cost and LOS reductions
• The tactics used for this pilot could easily be scaled to reach additional physician groups, hospital sites, or other medical specialtiesWhat is Already Known about this Topic?
What does this Paper Add?
Implications for Practice, Theory, or Policy?
Introduction
Palliative care has been shown to improve pain and symptom control and reduce hospital cost by aligning the treatment plan with patient goals, thereby eliminating unnecessary diagnostic tests and medications, and reducing readmission rates. Palliative care also positively impacts health outcomes and patient and family satisfaction and supports decision-making. Palliative care programs can initiate advance care planning along with communication strategies that can facilitate the decision-making process for patients and families at the end of life. Moreover, palliative care programs have demonstrated the ability to lower the overall cost of care, particularly if provided early in a hospital admission.1,2 Kupensky et al reported early palliative care consults (<72 h post trauma) for geriatric trauma patients reduced tracheostomy and Percutaneous Endoscopic Gastrostomy (PEG) procedures and hospital stays. 3
An analysis of palliative care 2018 data at Advocate Aurora Health, (over 6000 patients at 9 Illinois hospitals) showed that patients who had a palliative care referral by day 3 of admission had lower overall costs. Although this early referral for palliative care consult demonstrated cost savings benefits, examples in the literature of how to operationalize this were limited. In the inpatient setting, there is no clear standard for the initiation of a palliative care consult, despite evidence that palliative care intervention can reduce cost of care. 4 In fact, palliative care is often initiated late in a sizable proportion of terminally ill patients, resulting in increased use of high-level care in the hospital setting. 5 These findings were the impetus for us to design a process for an expedited palliative consult referral.
Aim
We explored whether operationalizing an early palliative care consult could decrease hospital length of stay (LOS) and increase cost savings. We also explored tactics to develop a process to change the timing of palliative care consult. This encourages physicians to avoid the usual pattern of delaying palliative care consult requests until after the workup is complete or the patient is closer to discharge.
Methods
Design
We completed a descriptive retrospective cohort study, using de-identified data from Advocate Aurora 2018 palliative care new consults (over 6000 patients at 9 acute care sites in Illinois). This data was originally captured for a system-wide initiative. The analysis revealed a decrease in cost of care when patients were referred for palliative care consult by day 3 of hospitalization. This outcome was the catalyst to complete a pilot to determine if we could operationalize decreasing the pre-consult LOS by educating providers on the benefit of an early palliative care consult.
A 3-month pilot was run from December 2019 through February 2020. All hospitalists employed by Advocate Medical Group (hospitalists) were selected as the pilot group because they are a consistent referral source with a large patient volume and share Key Result Areas (KRAs). All other physicians referring to palliative care during the pilot period (non-hospitalists) served as the control group. The pilot data was also compared to a baseline of all palliative care patients at the site referred during the 3 months prior to the pilot (September 2019–November 2019). The baseline was used to gain an understanding of how our institution was performing prior to the pilot. The intent of this pilot was to demonstrate that standardizing an early referral process would result in cost savings. The pilot group received a 30-minute education on the results of the 2018 retrospective data analysis, benefits of an early referral and the expectation of an early palliative care referral. They were encouraged to refer patients earlier, preferably by day 3 of admission. The mantra was “If you think your patient may require a palliative care consult, don’t wait. Refer for consult before day 3 of the hospitalization.” “Don’t delay, refer today!” This education was also reiterated and reinforced throughout the 3-month pilot period by both the hospitalists leaders and palliative teams as patients were reviewed during the daily hospitalists huddle. The control physician group did not receive the education and continued with their normal referral patterns.
Participants
Participants included all patients referred to palliative care over a 3-month period (December 2019–February 2020). Patients referred in the 3 months leading up to the pilot served as the baseline period (September 2019–November 2019).
All patients receiving palliative care at the site were included in this pilot. These patients had multiple chronic and acute serious illnesses requiring palliative care interventions. These conditions include, but are not limited to cancer, cardiac disorders, complex chronic conditions/failure to thrive, dementia, infections, neurologic/stroke/neurodegenerative disorders, pulmonary disorders, vascular disorders, and trauma. Since it was believed that the diagnosis and severity of the patient’s illness could affect LOS, it was decided not to restrict the patient population to any specific diagnosis. The focus remained on the timing of the palliative consult referral rather than the diagnosis or condition of the patient.
Setting
Advocate Aurora Health, located in Illinois and Wisconsin, is one of the 12 largest not-for-profit, integrated health systems in the United States. It includes 9 acute care hospitals in Illinois, all of which have inpatient palliative care teams. This initiative was piloted at Advocate Lutheran General Hospital, a 645-bed, level 1 trauma center located in north suburban Chicago. This site performs over 5000 inpatient palliative visits/year and has a stable and experienced palliative team. Additionally, this project aligned with the hospital’s strategic plan.
Research Team
The research team included Director of Strategy for the system, Inpatient Director of Palliative Care, Palliative Care Medical Director, Vice President of Hospice and Palliative Care, Hospitalist Medical Directors, and a Patient-Centered Outcomes Research Coordinator.
Recruitment
This study used de-identified existing data. No active recruitment was done.
Data Collection and Analysis
The pilot used data previously collected for a system-wide initiative to reduce patient hospital costs utilizing palliative care services. All data was de-identified and the study was determined to be non-human research. Patient characteristics are presented with means for continuous variables, and as proportions and absolute numbers for categorical variables. To represent timing of palliative consult, we measured the pre-consult LOS, defined as the number of days from admission to the palliative care consult. Post-consult length of stay is defined as the number of days from the palliative care consult to discharge. Cost savings data was represented by direct cost which included the full cost of care for a patient, including staffing, building and associated equipment costs along with patient testing, and supplies.
Ethical Considerations
This was determined to be non-human subjects research by the institutions IRB as this was secondary use of de-identified data and Office for Human Research Protections (OHRP) considers secondary use of de-identified data as non-HSR.
Results

Figure 1 shows that average direct cost at baseline ($18,849 ± $26,201) was comparable to the control group ($18,669 ± $26,944) while the pilot group ($13,800 ± $13,435; P = .05) saw reductions in direct costs. Average patient cost prior to and during the pilot program. Direct cost analysis includes the full cost of care for a patient, including staffing, building and associated equipment costs along with patient testing, supplies, staffing, etc.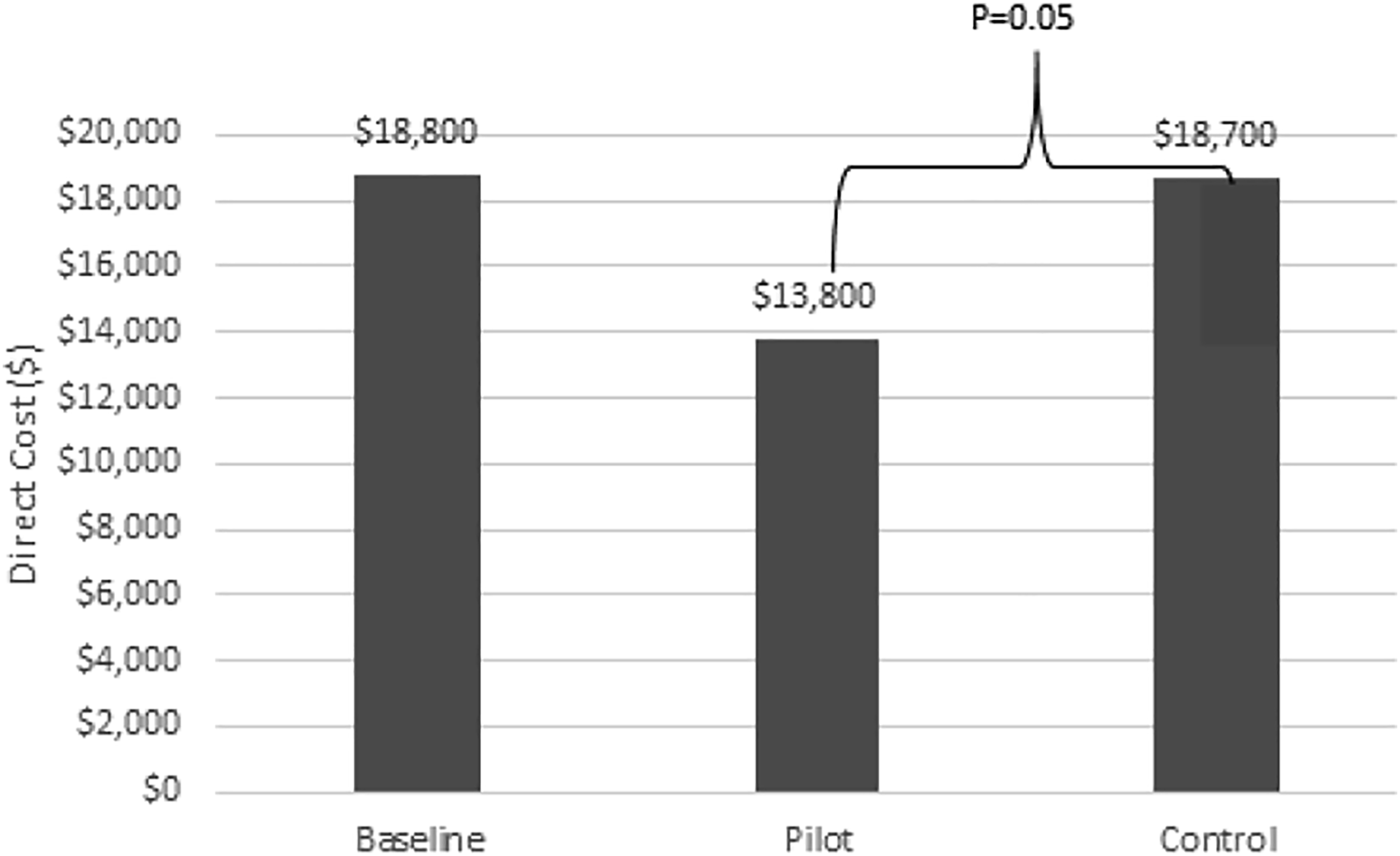
Type of Diagnosis.

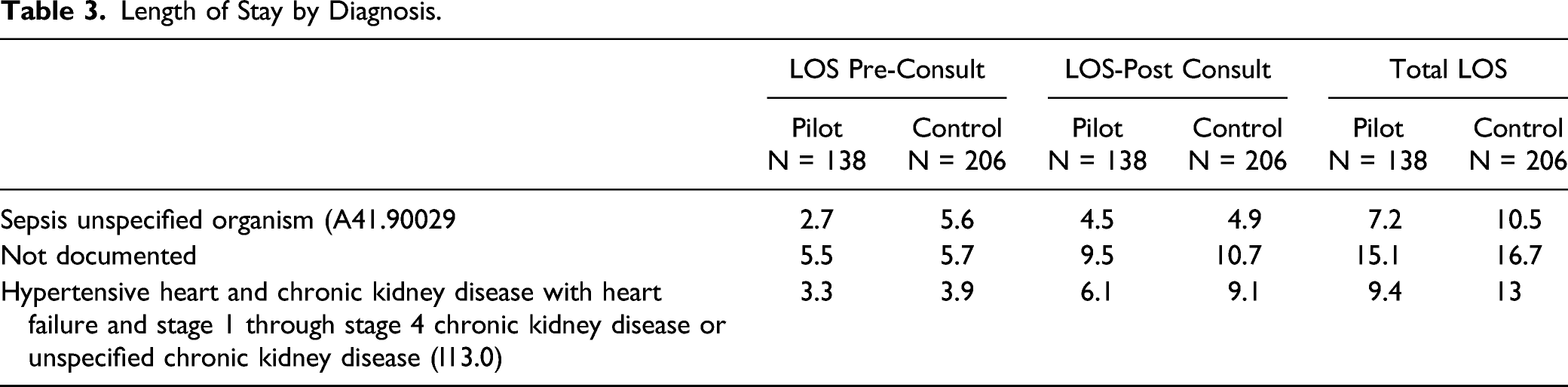
Length of Stay by Diagnosis.
Discussion
A retrospective analysis of Advocate Aurora Health’s 2018 palliative care new consult data (over 6000 patients at 9 acute care sites in IL) revealed a decrease in cost of care when patients were referred for palliative care consult by day 3 of hospitalization. This correlation between timing of consult and a decrease in total cost of care represented an opportunity to increase cost savings if we were able to operationalize a process to standardize palliative care referral by day 3 of admission. This was the impetus for our pilot.
To impact physician referral timing, we believed that additional education and reinforcement of the benefits of an earlier palliative care consult was needed. Simplicity of the process design was paramount as the hospitalists already have a busy practice and adding additional work would not be well received. To gain buy-in from the hospitalist teams, we involved the hospitalists’ medical directors to assist in the initial design of the pilot. This ensured that the process developed would be something that the hospitalists could easily incorporate into their current workflow. Additionally, the hospitalists’ medical directors were highly motivated, as this pilot would contribute to their ability to meet their LOS reduction goals.
The process developed to influence timing of referral for palliative care consult was focused on impacting the pre-consult LOS. It was hypothesized that if we could decrease the timing of admission to referral for palliative care consult, it would positively impact the overall LOS. While we did see a decrease in pre-consult LOS and overall LOS, we were not surprised that the post-consult LOS did not differ between the two groups. There was no intervention focus on post-consult LOS and post-palliative care consult the care plans remained the same. The earlier palliative care was consulted, the sooner goals and treatment preferences of the patient and families could be aligned with the care team, resulting in earlier discharge. Any earlier discharge could be attributed to a palliative care plan being put in place earlier.
Prior to the pilot, the palliative care team expressed concern that this new process would lead to increased consult volume that the current team would not be able to service. During the education for the hospitalists, it was stressed that we were not looking to trigger any new patients or diagnoses that they had not previously referred to palliative care; rather, our intention was for them to refer the same patients they would have normally referred, just earlier in their admission (preferably before day 3 of hospitalization). This tactic proved to be successful as we did not see an increase inpatient volume during the pilot compared to the baseline.
The pilot was introduced to the hospitalist teams at two separate onsite meetings to educate both teams. The analysis of the existing 2018 palliative care data showing earlier palliative care consult resulting in decreased LOS and cost savings was shared with the hospitalists. We focused on the potential LOS reduction in these education sessions as we felt that would have a greater appeal to physicians than cost savings. We shared our standard list of “Indicators for Palliative Care,” along with the suggestion that they refer any patient whom they believed may qualify for a consult by day 3 of hospitalization. Additionally, we posted simple signs in their offices stating, “If you are thinking your patient might benefit from Palliative Care, enter consult before day 3 of hospitalization. DON’T DELAY Consult Today!” These educational sessions were well received by the hospitalist groups. Additionally, for the 3-month pilot period, a member of the palliative care team attended the daily hospitalists huddle 1–2 times per week to reiterate the request for a palliative care consult by day 3 of admission. The control group of non-hospitalist physicians were not given any education and continued with their normal referral patterns. It is possible that the hospitalists pilot group spoke with the non-hospitalists about the value of an early palliative care referral, however, the education sessions as well as follow up meetings were only offered to the pilot group.
Only actual palliative patient data was included in this pilot. If a patient was referred for palliative care but refused or was not seen for any reason, the data would not be included. The pilot data was analyzed using patient level direct cost analysis which included the full cost of care for a patient, including staffing, building and associated equipment costs along with patient testing, supplies, and staffing
The results of this pilot demonstrated a direct cost savings of 26% over the 3-month pilot period. Little difference in the pre-consult LOS, post-consult LOS, and total LOS in the control group was seen compared to the baseline. The pilot group showed a decrease in pre-consult LOS and post-consult LOS compared to both the baseline and control groups. Additionally, a 2-day reduction in overall LOS was demonstrated in the pilot group compared to both the baseline and control groups. The reduction in overall LOS is very encouraging. While not statistically significant, there is great clinical importance when discharging a patient 2 days earlier.
This affects our patients as palliative care was able to assist patients and their families in making decisions that would allow them to transition to the next level of care sooner. A reduction in LOS can positively impact patient satisfaction as well as improve the quality of care. The resulting cost reduction, although less impactful to patient care, allows the palliative care program to further demonstrate the value the program adds to the system goal to reduce LOS and associated costs. This is further illustrated by the > $5000 decrease in the cost of care in the pilot group as compared to the baseline and control groups. (Figure 1)
Initially, we had some discussion on whether the LOS would vary with patient diagnosis. We were able to analyze the pilot data by diagnosis. We found there was no significant difference between the pilot and control groups in the type of diagnoses seen during the pilot period. (Table 2) Additionally, although the LOS varied slightly by diagnosis, the pre-consult LOS, post-consult LOS and total LOS were all lower in the pilot group for all diagnoses when compared to the control group. (Table 3)
Recommendations for Future Practice
Incorporate education on the benefits of early palliative care consults into future presentations to all provider groups.
Strengths and Limitations
The data used for this review was not originally collected for research and the size of the sample was underpowered to show a significant difference in our main outcomes (LOS and cost). The clinically significant decrease in both cost and LOS confirmed the need to validate our results with a larger study to see if the intervention is reproducible on a larger scale and eventually in multiple hospitals.
Conclusions
This pilot demonstrated that focused education could influence provider referral behavior to order palliative care consults earlier in the hospital stay, resulting in cost savings and LOS reduction. Although we were able to demonstrate a > 1 day earlier palliative care consult during our pilot, we did not achieve an overall average of < 3 days. However, this incremental change demonstrated cost savings and a decreased overall LOS. In retrospect, a measure or comparison of patient or family satisfaction when a palliative care consult occurred earlier in the hospitalization would have been valuable. Pilot results indicated that a larger study may be needed.
The tactics employed with this pilot to influence physician referral timing can easily be transferred to additional sites as well as new physician groups to increase the overall financial impact. Additionally, we feel that this process would be highly effective if focused in other areas of the hospital like the Emergency Department or the ICU. This process could also be used for other service lines where an early consult may result in decreased LOS and cost savings.
Footnotes
Acknowledgments
The authors thank the medical directors of the hospitalists teams, Joanna Maurice MD, and Ana-Maria Nowell MD, for assisting with the development of this pilot and their dedication to continually reiterating the value of an early palliative care consult referral with their physicians. We would also like to thank Nilofer Kidiwala DO, Lead Palliative Physician at Lutheran General Hospital who assisted in the development and promotion of this pilot. Additionally, a special thank you to the palliative care team at Lutheran General Hospital: Gayle Bereskin DO, Marla Bass APRN, Cynthia Kane APRN, Amy Miner APRN, Joanna Polk LCSW, and Michael Zeniecki MPH, Practice Manager for their willingness to participate in this pilot and give us their feedback and suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Management and Sharing
Aggregate data was used from a previous system-wide initiative. Specific raw data from this pilot is not available. The corresponding authors are available to contact for further information.