
Abstract
Background: The purpose of this study was to clarify how the Regional Referral Clinical Pathway for Home-based Palliative Care (RRCP-HPC) and an outreach program by a palliative care team (PCT) lead to an improvement in the outcome. Design and Methods: We conducted questionnaire surveys using the mailing method involving the regional medical staff involved in cancer patients introduced to the PCT of a single hospital, as well as bereaved families. The questionnaire was prepared through interviews with the medical staff and bereaved families. Subsequently, factor analysis was performed to identify factor structures and calculate the correlation coefficient with each outcome. Results: For the questionnaire survey involving the medical staff, responses were collected from 119 regional medical institutions and 84 regional medical staff. The response rate per institution was 51.3%. Similarly, for the questionnaire survey involving bereaved families, the response rate was 42.4%. For the survey involving the medical staff, 6 factors, such as “improved awareness of an interdisciplinary team,” were extracted. For the survey involving the bereaved families, 4 factors, such as “improvement of communications between patients and healthcare professionals,” were extracted. There were significant (≥moderate) correlations between these factors and all outcomes. Conclusion: In this study, we clarified the process of achieving palliative care until death at home without difficulties using the outreach program and RRCP-HPC. The results suggest the importance of improving communications. The outreach program and RRCP-HPC may have contributed to palliative care at home without difficulties through an improvement in communications.
Keywords
Introduction
The number of patients who wish to receive home-based palliative care is latently large.1,2 According to national surveys in Japan, approximately 50% of terminal cancer patients wished to receive medical treatment at home,3,4 and approximately 30% wished home death.2,5-7 However, many persons do not consider home death realistic in Japan, where there is no general practitioner (GP) system.7,8 Therefore, a home-based palliative care-related increase in the number of deaths at home meets patients’ wishes, raising an issue regarding home-based palliative care in Japan. 2
However, affiliations by the medical staff involved in home-based palliative care, such as GP, community nurses, and community pharmacists, vary, and occupations to be needed, functions, and palliative care-skilled regional medical staff are insufficient in many areas. The following 3 interventions were implemented to overcome these concerns: (1) an educational program for medical staff who do not have a specialization in palliative care, including everything from using medications to communication skills (Palliative Care Emphasis Program on Symptom Management and Assessment for Continuous Medical Education: PEACE); (2) a new information-sharing tool (introduction of the Regional Referral Clinical Pathway for Home-Based Palliative Care [RRCP-HPC]) to increase the participation rate of GPs, patients’ families, and patients in sharing information, which is a common concern, and to enhance information sharing 9 ; and (3) a team of palliative care specialists in the hospital visited the area at the same time and date with local medical staff, including GPs, to complement the insufficient functions (an outreach program). 10 These interventions allowed us to provide almost the same intensity of medical care at home as available in a hospital. These interventions increased the rate of deaths at home. 10 However, while the effectiveness of the PEACE has been verified, 10 the process by which the other 2 interventions increased the number of deaths at home was unclear.
Therefore, this study surveyed the medical staff providing these interventions and the bereaved families to determine why the 2 interventions increased the outcome, that is, home deaths.
Methods
This study consisted of 2 questionnaire surveys involving the medical staff and bereaved families, respectively. The contents of questions differed between the 2 surveys.
Questionnaire Survey Involving the Medical Staff
Preparation of the questionnaire
The interview data of 8 bereaved families obtained from a previous study 9 was examined using content analysis focusing on the RRCP-HPC and outreach program to prepare each item pool. Based on this, a questionnaire consisting of 28 items under 6 subscales about the outreach program, and another questionnaire consisting of 15 items under 3 subscales about the RRCP-HPC was prepared.
Participants
Participants included the regional medical staff who were non-specialized palliative care healthcare professionals, visited the patients at home on a daily basis (physicians, nurses, pharmacists, and care managers), and had been involved with the cancer patients introduced to the palliative care team (PCT) of a hospital in Japan between October 2006 and September 2013.
A questionnaire was sent by mail to medical institutions to which the participants belonged. An answer sheet was delivered to each participant. The participants responded to the items on a 5-point Likert scale (1: don’t think so and 5: think so). Similarly, the following outcomes, including the global usefulness of the outreach program and the RRCP-HPC and their usefulness for improving communication/the sense of security, complementing knowledge/techniques, devising care strategies, promoting/providing home-based palliative care, and achieving home death without difficulties, were investigated using the 5-point Likert scale (1: not useful and 5: very useful). Unsigned answer sheets were collected in each institution, and sent to us.
Outcome and its assessment
Responses were obtained with respect to the domains that had been assumed as expert opinions by palliative care physicians and researchers in the field of palliative care. Furthermore, factor structures were confirmed using factor analysis, and Cronbach’s α and intraclass correlation coefficients were calculated/used as indices of reliability. Subsequently, the mean score per domain was calculated, and the correlation coefficient with each outcome was calculated.
Questionnaire Survey Involving Bereaved Families
Preparation of a questionnaire
Of the bereaved families (patients who died at home) who had experienced an outreach program, those with a shorter interval from patients’ deaths were initially recruited. The participants were interviewed individually for approximately 45 to 60 minutes using a semi-structured method and their freely spoken speech was recorded verbatim using a voice recorder. A clinical research coordinator was the interviewer. The interview guide involved questions, such as “global impression of outreach,” “usefulness,” “necessity (and its reasons),” and “problems in clinical practice.” Subsequently, content analysis was performed using the interview data obtained to prepare an item pool. An interview was started, targeting 10 persons. However, there was no new category for the contents at the completion of interviews with 8 persons, and the survey was completed. Eight of the interviewed bereaved families were excluded from the questionnaire survey. Based on this, a questionnaire consisting of 17 items involving 4 subscales regarding outreach was prepared.
Participants
The participants were the bereaved families of cancer patients who were treated in a single hospital (cancer treatment regional cooperation center hospital) belonging to the Takaoka medical care zone between October 2006 and September 2013, and introduced to the PCT. The medical staff was surveyed using the mailing method. The usefulness of outreach was investigated using a 5-point Likert scale (1: not useful and 5: very useful). Similarly, the following outcomes, including the global usefulness of the outreach program and the RRCP-HPC and their usefulness for improving communication/the sense of security, complementing knowledge/techniques, and devising care strategies, were examined using a 5-point Likert scale (1: not useful and 5: very useful).
Outcome and its assessment
Responses were obtained with respect to the domains that had been assumed as expert opinions by palliative care physicians and researchers in the field of palliative care. Furthermore, factor structures were confirmed using factor analysis, and Cronbach’s α and intraclass correlation coefficients were calculated/used as indices of reliability. Subsequently, the mean score per domain was calculated, and the correlation coefficient with each outcome was calculated.
Analysis
Statistical analysis
To compare the results between 2 groups, the t-test, Mann–Whitney U-test, chi-square test, and Fisher’s exact test were used in accordance with the type of data.
To extract factors on factor analysis, the maximum likelihood method was used. For axial rotation, the promax method was adopted. A threshold factor load was established as .4. Several factor structures that can be interpreted were calculated in reference to the number of assumed factors, eigenvalues, and results of scree plotting.
A P-value of .05 was regarded as significant. As an effect size, Cramer’s V, Pearson’s correlation coefficient, or Cohen’s d was calculated. An effect size of <.2 was regarded as ineffective, that of .2 to .39 as minimally effective, that of .4 to .59 as moderately effective, and that of ≥.6 as very effective.
For statistical analysis, we used SPSS version 22 software (IBM Japan, Ltd., Tokyo).
Content analysis
Content analysis was performed based on Krippendorff’s methodology. 11 Krippendorff states that content analysis is the objective clarification of an event by analyzing, categorizing, and naming record units based on data (descriptive data) obtained through a survey. 11 The implication of the usefulness of the RRCP-HPC/outreach program or problems regarding the regional widespread use of these programs for bereaved families and medical staff was extracted as 1 unit. According to the similarity of extracted implications, inductive classifications/generalizations were conducted. Two investigators independently performed categorization. When preparing categories, they were discussed until a mutual agreement between the 2 investigators was reached, and the final categories were determined.
Ethical Consideration
Prior to this study, its protocol was approved by the Ethics Review Board of Saiseikai Takaoka Hospital. All subjects (the medical staff and bereaved families) were adults who do not require any legal representative. Before interview surveys, the purpose of this study, anonymity, and study participation based on free will were explained verbally and using documents, and written informed consent regarding study participation was obtained. Prior to questionnaire surveys, a questionnaire with an explanatory document was sent to each subject by mail, and responders to the questionnaire were regarded as consenting to study participation.
Results
Collection Rate on the Questionnaire Surveys
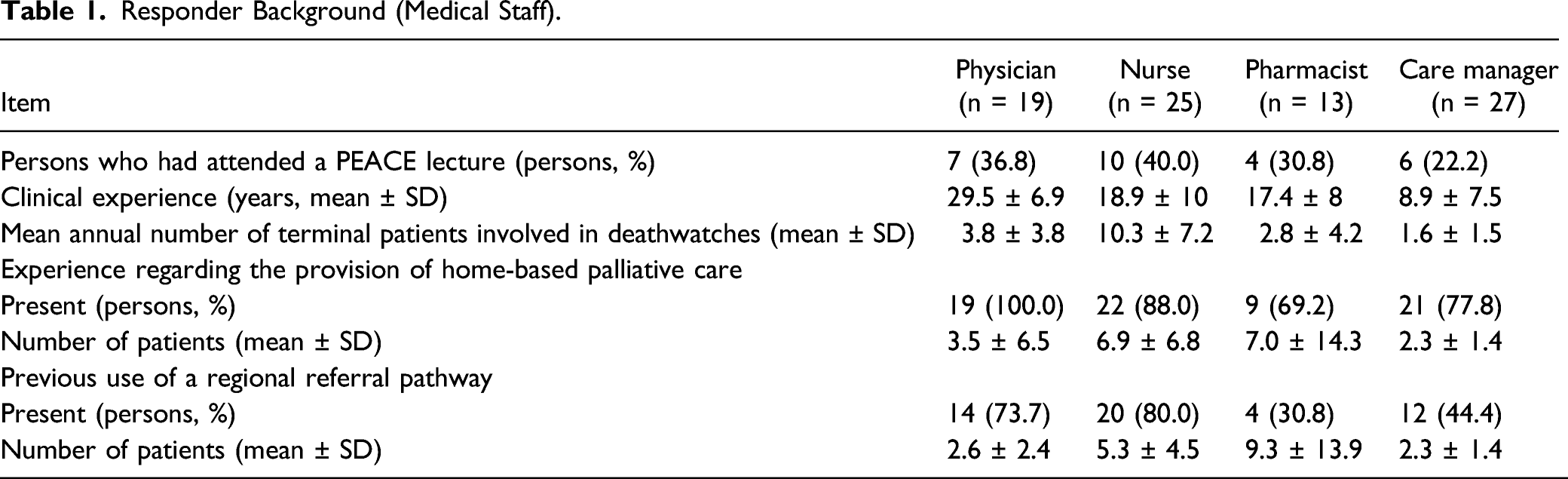
Responder Background (Medical Staff).
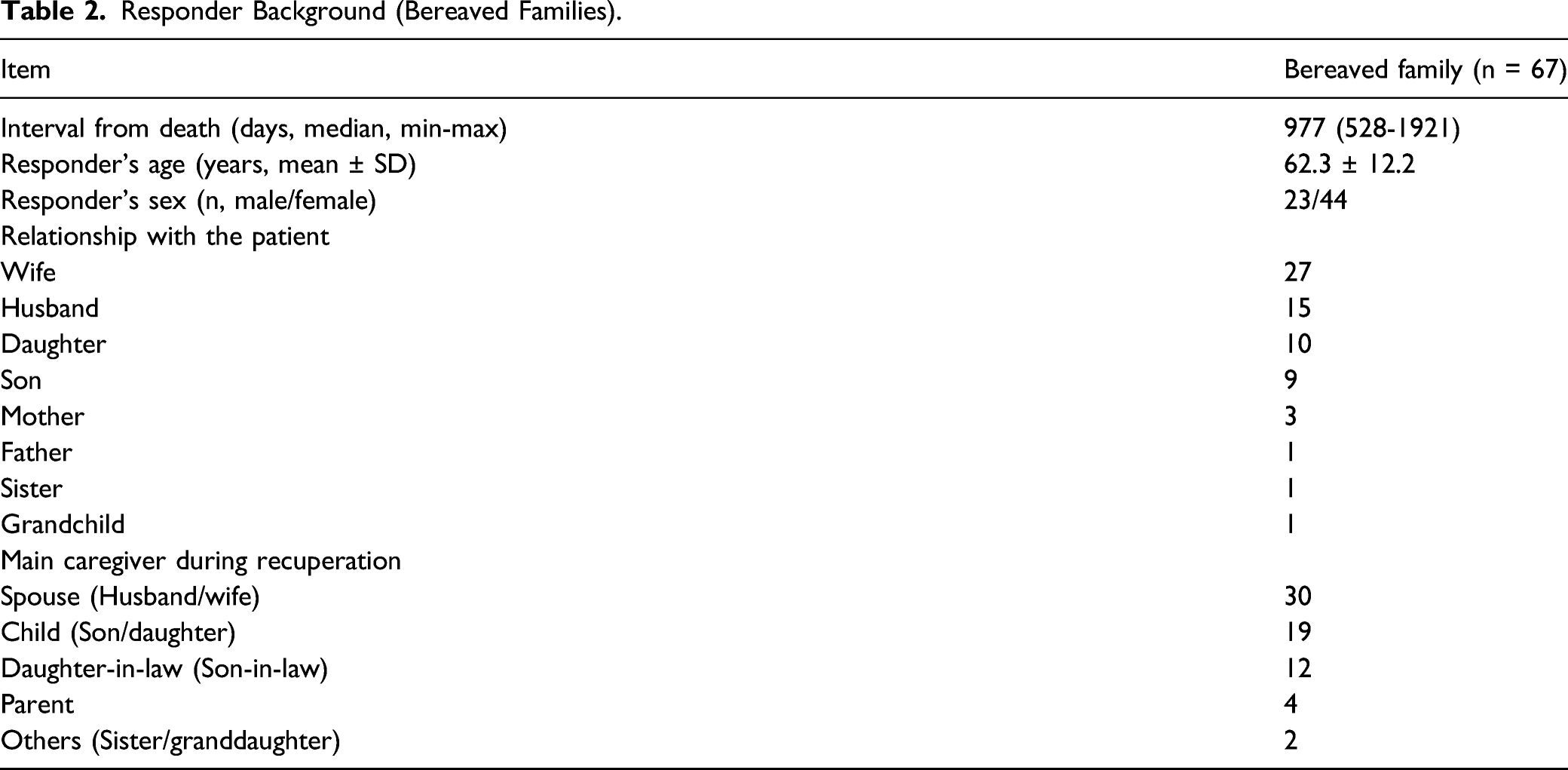
Responder Background (Bereaved Families).
Reasons for the Usefulness of Intervention (Factor Analysis)
Factor Analysis (Questionnaire Survey Involving the Medical Staff).
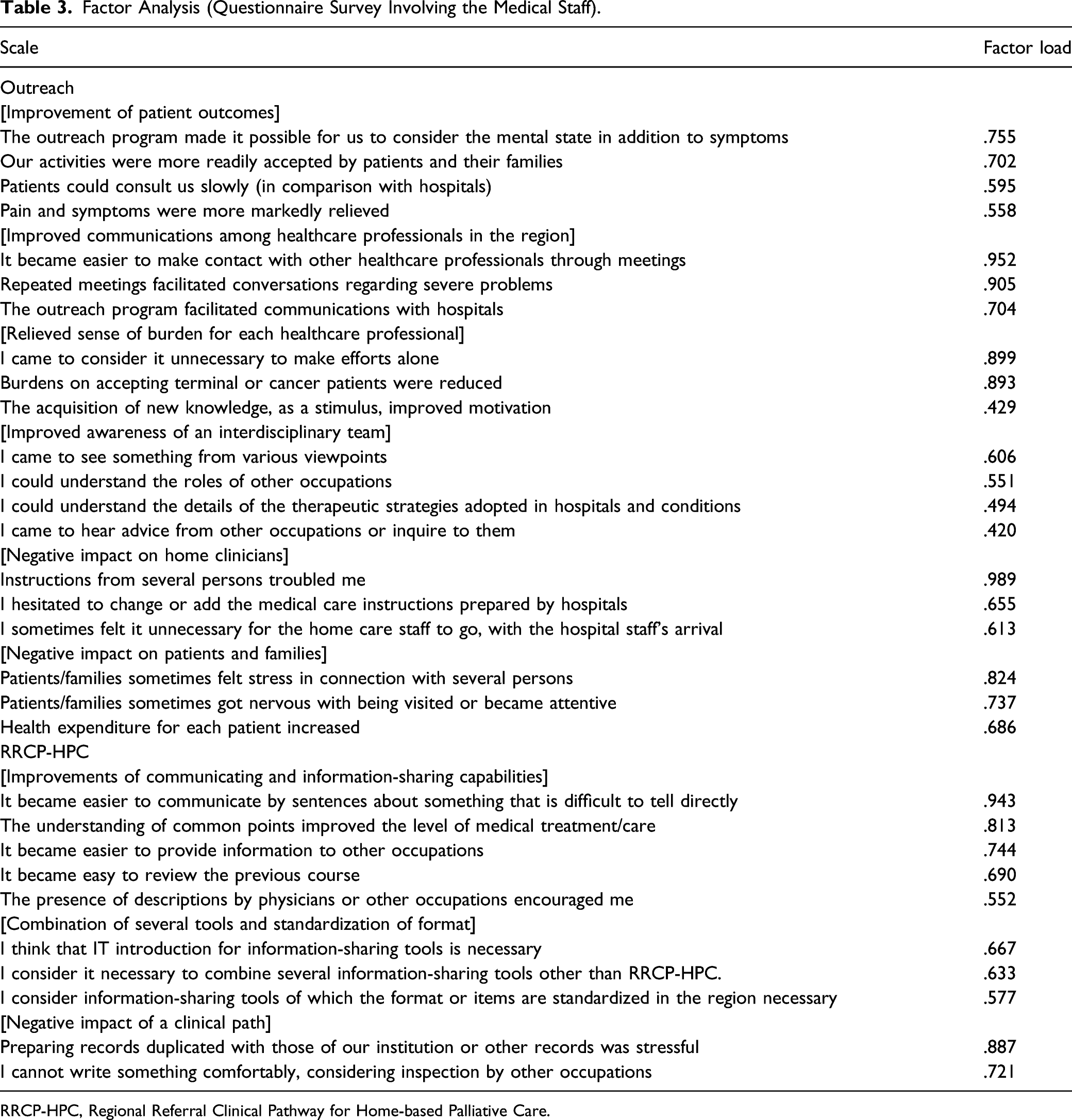
RRCP-HPC, Regional Referral Clinical Pathway for Home-based Palliative Care.
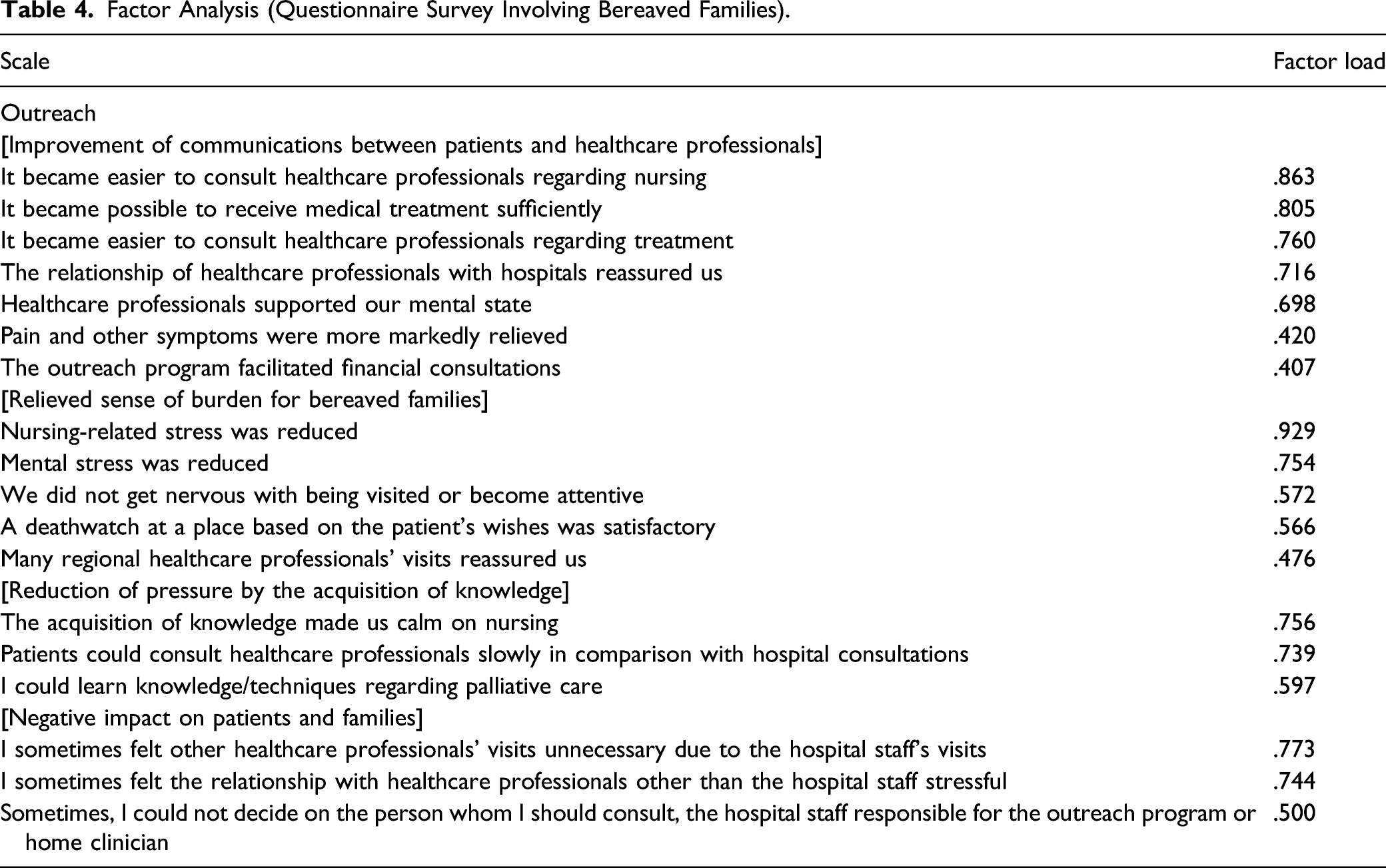
Factor Analysis (Questionnaire Survey Involving Bereaved Families).
Evaluation of Validity.
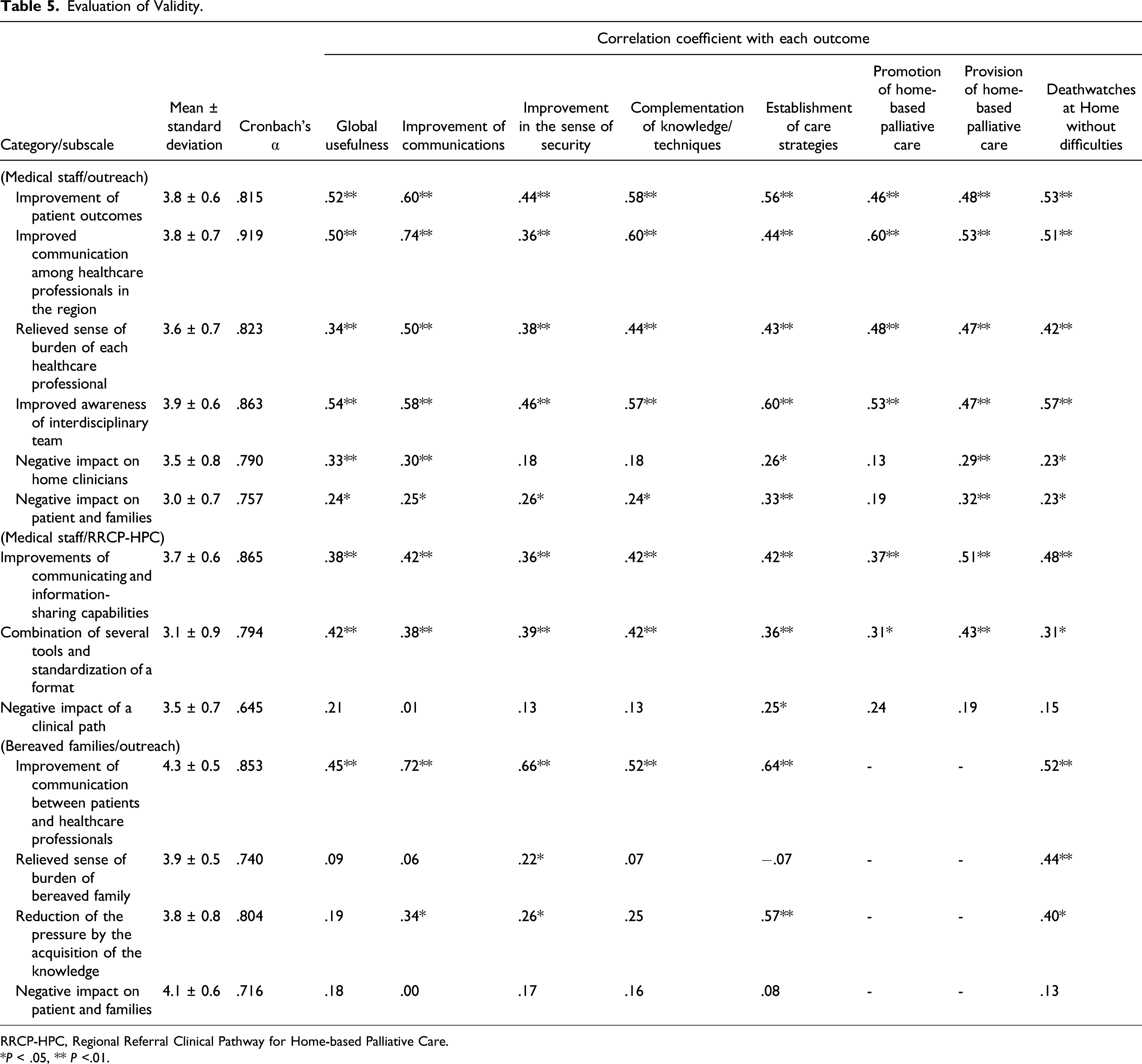
RRCP-HPC, Regional Referral Clinical Pathway for Home-based Palliative Care.
*P < .05, ** P <.01.
Concerning the outreach program, the factor loadings were high for items related to communication and reducing the care burden, such as “it became easier to make contact with other healthcare professionals through meetings,” “repeated meetings facilitated conversations regarding severe problems,” “I came to consider it unnecessary to make efforts alone,” “burdens on accepting terminal or cancer patients were reduced” (Table 3), and “nursing-related stress was reduced” (Table 4).
Correlations Between the Extracted Factors and Outcomes
The correlation coefficients between 6 evaluation factors for the outreach program and 8 outcomes were calculated based on the medial staff’s responses. “Improvement of patient outcomes” and “improved awareness of an interdisciplinary team” were moderately or strongly correlated with all outcomes. “Improved communications among healthcare professionals in the region” was moderately or strongly correlated with 7 outcomes, excluding “improvement in the sense of security.” “Relieved sense of burden for each healthcare professional” was moderately correlated with 6 outcomes, excluding “global usefulness” and “improvement in the sense of security.” There was no moderate or marked correlation of “negative impact on home clinicians” or “negative impact on patients and families” with any outcome.
The correlation coefficients between 6 evaluation factors for RRCP-HPC and 8 outcomes were calculated based on the medial staff’s responses. “Improvements of communicating and information-sharing capabilities” was moderately correlated with “improvement of communications,” “complementation of knowledge/techniques,” “planning of care strategies,” “provision of home-based palliative care,” and “home death without difficulties.” “Combination of several tools and standardization of a format” was moderately correlated with “global usefulness,” “complementation of knowledge/techniques,” and “provision of home-based palliative care.” There was no moderate or marked correlation of “negative impact of RRCP-HPC” with any outcome.
In addition, the correlation coefficients between 4 evaluation factors for the outreach program and 5 outcomes were calculated based on the bereaved families’ responses. “Improvement of communications between patients and healthcare professionals” was moderately correlated with all outcomes. There was a moderate correlation between “relieved sense of burden for bereaved families” and “home death without difficulties.” “Reduction of pressure by the acquisition of knowledge” was moderately correlated with “planning of care strategies” and “home death without difficulties.” There was no moderate or marked correlation of “negative impact on patients and families” with any outcome.
Most of the factors, except for negative impact, had significantly high correlations with one of the outcomes, “improvement of communications between patients and healthcare professionals,” validating the importance of communication. Notably, there are many moderately significant correlations with the “promotion of home-based palliative care” outcome.
Discussion
This study clarified the process by which the outreach program and RRCP-HPC achieve home death without difficulties. As the most important point, factors moderately or strongly correlated with “home death without difficulties” were clarified. In particular, this is the first study involving outreach assessment by bereaved families. Both the medical staff and bereaved families recognized the importance of improving communications; the outreach program may achieve home death without difficulties through the improvement of communications. Similarly, concerning RRCP-HPC, communication-related factors were correlated with “home death without difficulties,” suggesting that communications are the most important. Previous studies reported that the improvement of communications in a medical team led to many merits, such as an increase in awareness, a complementary role among members, a favorable access to medical resources in the region, and an improvement in the quality of life.12,13 In this study, the importance of communicating capability, which leads to home death without difficulties, was clarified from patient families’ viewpoints, suggesting its necessity for increasing the home death rate.
As the second most important point, 4 factors related to “promotion of home-based palliative care” were clarified. There was a strong correlation between “promotion of home-based palliative care” and “improvement of communications.” Insufficient communications with patients and among the medical staff are known factors that inhibit the continuation of home-based palliative care.” 14 Once patients are admitted, discharge may be difficult,15-17 leading to hospital death. The widespread regional application of home-based palliative care contributes to an increase in the home death rate; the factors that were found to be highly related to “promotion of home-based palliative care” may have important implications.
Furthermore, as the reason why the outreach program is useful for promoting home death without difficulties, the results suggest that it reduces the medical staff’s and bereaved families’ burdens. Nursing is a factor important for achieving home death. 18 Heavy burdens for nursing are stressful for patients and their families, resulting in the consideration of euthanasia or physician-assisted suicide 19 ; therefore, it may be important to reduce them.
In Japan, even large hospitals have free access and very often, GPs are not assigned. When such patients are transferred from hospital care to home care for the first time, they are given a piece of paper called a “referral letter” to see a GP. Furthermore, GP have to see terminally ill cancer patients for the first time, and in many cases, end-of-life care is required before a trusting relationship could be established leading to miscommunications. Given this background, it is possible that the interventions we provided were particularly sensitive to creating a “face-to-face” (i.e., understanding the other person’s personality) relationship in communication.
This study has some limitations. Initially, a single institution provided the outreach program, and this was a relatively small-scale study. Therefore, the results may not completely reflect the state of the test region. To evaluate the reproducibility and potential generalization, it is necessary to conduct a multicenter cooperative study involving several supporting hospitals in other areas. However, the hospital that offered the outreach program is the only hospital that offers home palliative care within the target medical region, and has been assigned most cases which need the outreach. Therefore, it is suggested the study result has the certain generalizability. Furthermore, since the number of providers belonging to each institution varied and the number of providers was unknown, a fixed number of about 15 copies per institution were uniformly sent out and each person was asked to answer 1 copy. Theoretically, this could lead to selection bias on the part of the provider institutions. However, they assured us that there was no selection bias and we have no choice but to trust them. Furthermore, this was a clinical study, and various complex interventions other than the outreach program and RRCP-HPC were performed in accordance with patients’ conditions, recall bias, and learning bias due to differences in the number of interventions. Therefore, we cannot rule out the possibility that the results of this study may have been influenced by other interventions. In addition, outcomes were obtained as the results of representative assessment by the bereaved families and medical staff. The patients were dead, and it was impossible to obtain the results of assessment from themselves. However, the use of representative assessment should be considered. Although this study has these limitations, we clarified the process (or reasons) from interventions, such as the application of the outreach program and RRCP-HPC, to home death without difficulties. This may provide findings important for determining strategies to increase the number of home death. Furthermore, in this study, we clarified the process based on the bereaved families’ viewpoint for the first time. This may suggest the necessity of communications between healthcare professionals responsible for an outreach program and bereaved families or matters to be considered.
Conclusion
We clarified the process of home death achievement by the outreach program/RRCP-HPC. The results obtained from both the medical staff and bereaved families suggest the importance of improving communications. The evaluation of the outreach program and RRCP-HPC revealed that “home death without difficulties” through the improvement of communications was achieved by providing a place for practice in a situation where direct guidance from a palliative care specialist could be received, and as a matter of concern between medical professionals and between medical professionals and patients/families. This may give suggestions important for establishing strategies to increase the number of home death.
Supplemental Material
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211055901 - Process Evaluation of the Regional Referral Clinical Pathway for Home-Based Palliative Care and Outreach Program: A Questionnaire Survey of the Medical Staff and Bereaved Families
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211055901 for Process Evaluation of the Regional Referral Clinical Pathway for Home-Based Palliative Care and Outreach Program: A Questionnaire Survey of the Medical Staff and Bereaved Families by Nozomu Murakami, Kouichi Tanabe, Tatsuya Morita, Yasunaga Fujikawa, Shiro Koseki, Shinya Kajiura, Kazunori Nakajima and Ryuji Hayashi in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material, sj-pdf-2-ajh-10.1177_10499091211055901 - Process Evaluation of the Regional Referral Clinical Pathway for Home-Based Palliative Care and Outreach Program: A Questionnaire Survey of the Medical Staff and Bereaved Families
Supplemental Material, sj-pdf-2-ajh-10.1177_10499091211055901 for Process Evaluation of the Regional Referral Clinical Pathway for Home-Based Palliative Care and Outreach Program: A Questionnaire Survey of the Medical Staff and Bereaved Families by Nozomu Murakami, Kouichi Tanabe, Tatsuya Morita, Yasunaga Fujikawa, Shiro Koseki, Shinya Kajiura, Kazunori Nakajima and Ryuji Hayashi in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant [25460892] from the Japan Society for the Promotion of Science.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.