
Abstract
Purpose:
Health and social care professionals report it challenging to have conversations with families when an important adult in the life of a child is at end of life, often feeling this aspect of care is the responsibility of other colleagues. This study aimed to understand professionals’ perceived role in family-centered conversations as part of routine care at end of life, and how to promote this element of care in clinical practice.
Methods:
An audit was completed with 116 professionals who work in palliative care including doctors and nurses that attended a 2-day virtual congress.
Results:
Professionals (73.2%) felt confident about starting a conversation with adult patients at end of life about important children. However, enquiring about relationships with children was largely dependent on the age of the patient. 64.7% of respondents reported signposting families to websites and services that provide family support. Most professionals (76.7%) wanted training to equip them with the skills and confidence to having family-centered conversations at end of life, with videos demonstrating how to provide these elements of care the most preferred option.
Conclusions:
Short training resources should be developed to equip professionals with the necessary skills toward having conversations about children with patients and relatives in clinical appointments. There is a need for professionals to ask every patient about important relationships with children.
Keywords
Introduction
Global evidence has shown that effective communication with children about parental illness is essential for long term psychological wellbeing and family functioning. 1 Health and social care professionals (hereafter referred to as professionals) are central to providing psychosocial support to families when an important adult in the lives of their children (<18 years old) is at end of life.2-4 Professionals often feel ill-equipped to have conversations with patients and their families about children; frequently reporting family-centered care to be the role of other colleagues within the multidisciplinary team.2,5 In reality, parents have reported a lack of supportive guidance from professionals about sharing information with their children about a significant adult’s illness, even when death is imminent.6-8 Professionals have reported a desire to develop their skills and confidence to have conversations in routine care with patients and their families about children from diagnosis through to end of life.2,5,9,10
One of the reported obstacles to conversations with patients about their children is professionals’ own discomfort with raising these sensitive topics.2,3 Professionals working in palliative care have extensive training, skills and experience talking with patients about illness, death and dying. The authors wanted to understand the extent to which these skills were used to consider the needs of children within the family. An audit was conducted with palliative care professionals to better understand: (1) professionals perceived role in having family-centered conversations with patients and families at end of life, and (2) clinicians’ views about support that would facilitate their provision of this psychological care to families about children in routine clinical practice.
Methods
The audit consisted of an online open survey. This study is reported following the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) criteria. 11
Audit Development
The audit was developed using JISC Online Survey software and tested by the research team. The questions were informed by a qualitative systematic review 3 and 2 qualitative studies exploring professionals’ role in supporting families when a parent of dependent children is at end of life.2,5 The authors, who developed the audit, have a wealth of research and clinical experience in palliative care and communication with children regarding illness. The audit consisted of questions exploring professionals’ views about their role, confidence, and training needs to having family-centered conversations with families about important relationships with children. Professionals were also asked to state their professional role and years’ working in clinical as well as palliative care practice. The questions were not randomized, each question was presented on a new page, and respondents were unable to review and change their answers (e.g., through a “Back” button or a “Review” step at the end of survey) as this could have resulted in biased responses from respondents.
Audit Pre-Testing
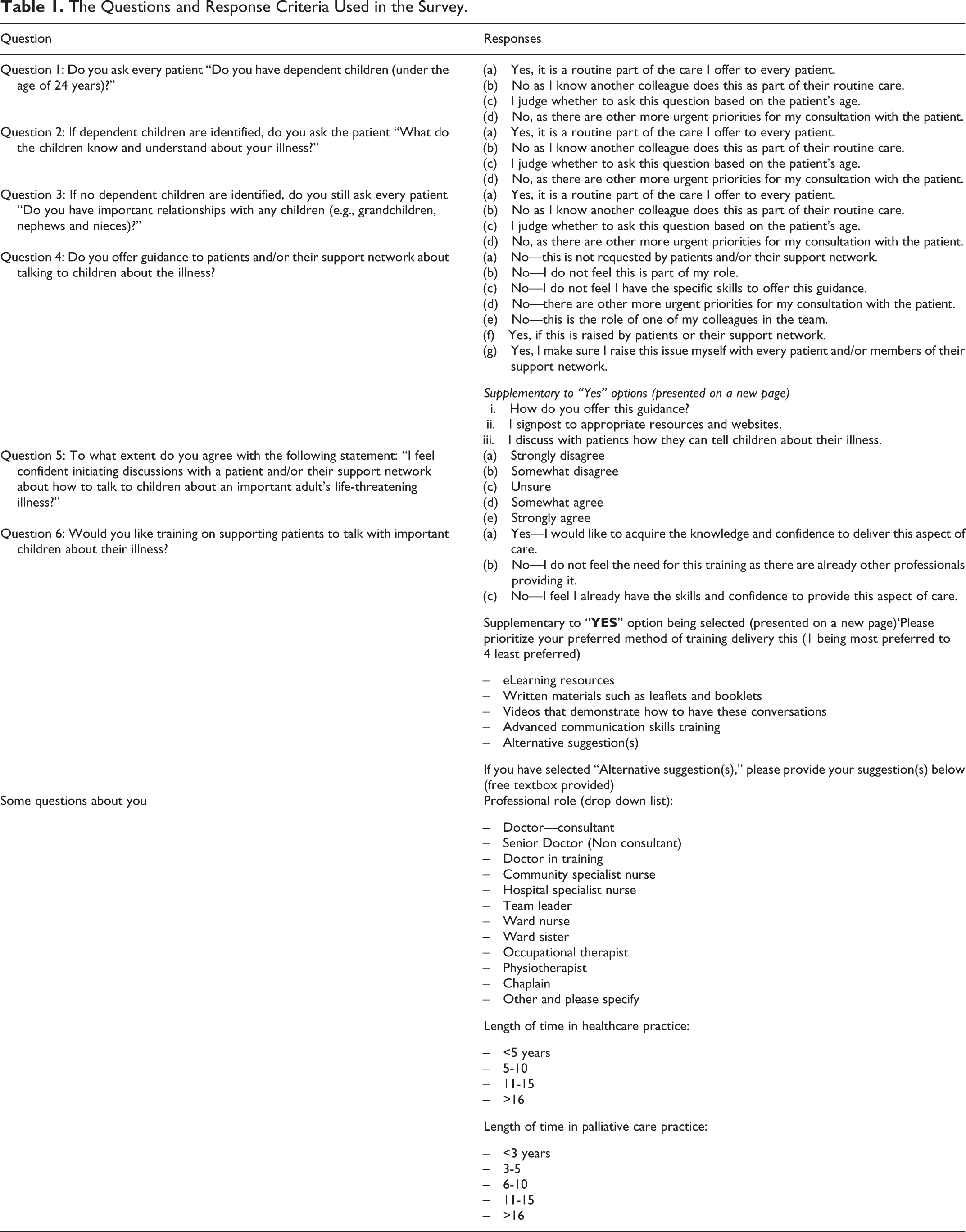
The audit was pre-tested with palliative care registrars, a palliative care nurse, and a palliative care consultant to check for its appropriateness, language, and understanding. Piloting the audit resulted in the rewording of some questions, the inclusion of additional criteria in the suggested responses, and the reordering of 2 questions. The decision was also made to highlight the questions as mandatory to complete the survey; the aim of the research was to have a better understanding of current practice and answering the 6 questions in the audit was considered necessary to enable this appreciation. The questions and response scale for each is reported in Table 1.
The Questions and Response Criteria Used in the Survey.
Sample
The audit was distributed at the 2-day Palliative Care Congress virtual conference (host city; Edinburgh, United Kingdom) in March 2021. Individuals were considered eligible to complete the questions if they provide end of life care as part of their routine workload.
Audit Administration
Individuals completed the audit by accessing the link in the research team’s exhibition stand. Prior to completing the questions, delegates were provided with information in the research team’s exhibition area about the purpose of the study, what their involvement would be, an estimate of how long the survey may take (up to 3 minutes), and the research team’s contact details to ask any questions. To encourage completion, delegates were informed they would be invited to enter a prize draw at the end of the audit, by clicking through to an unlinked form to provide their email address.
Data Analysis
Data were analyzed by JRH using SPSS v.27 to provide details of the sample characteristics, and the frequencies and percentages of responses.
Ethical Considerations
Delegates attending the virtual conference were not coerced to complete the audit. A member of the research team was “available” at the exhibition stand area during the 2-day conference to answer any queries or concerns of the delegates. Data protection procedures were observed. The research team provided a resource pack for all interested and participating respondents providing them with information about the purpose of the audit, information of organizations that provide family or professional support, the authors contact details, and links to psychoeducational resources designed for clinicians on how to support families in relation to dependent children about a parental life-threatening illness. Following consultation with the Joint Research Classification Group at University of Oxford, ethical approval was not required.
Results
Response Rate
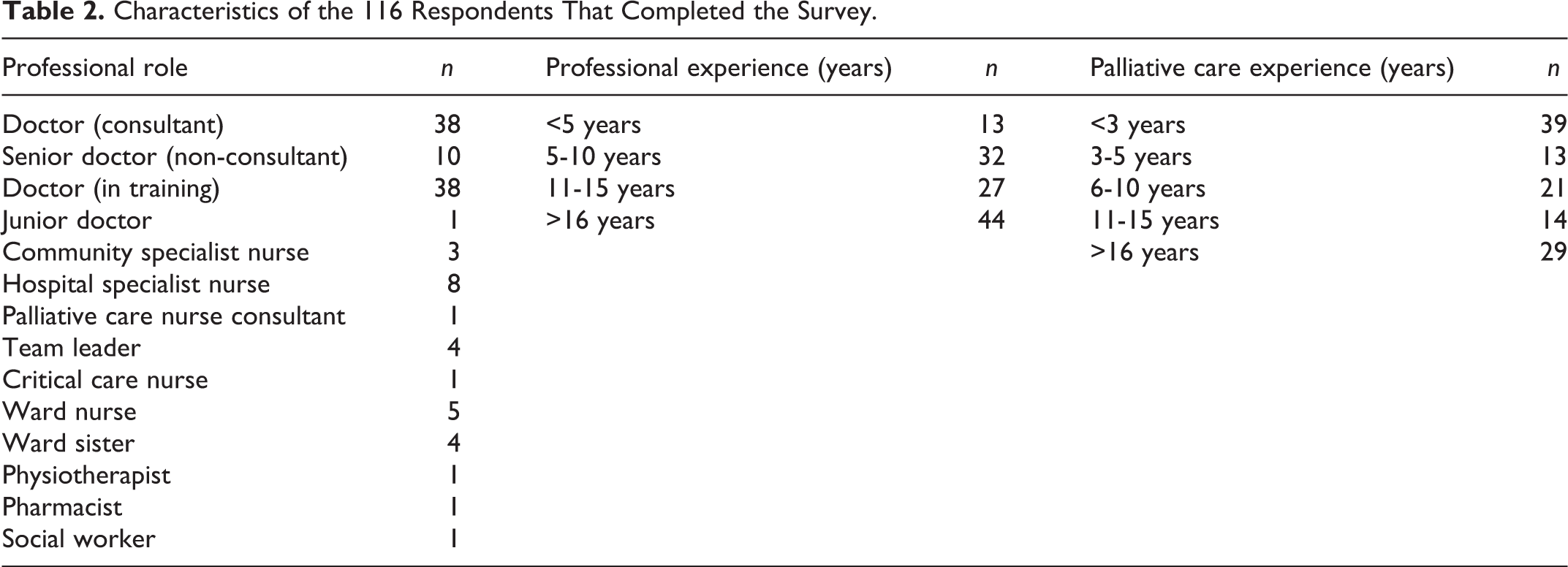
The conference was attended by 588 professionals. Of these, 158 delegates visited the exhibition stand over the 2-day period. A total of 116 professionals entered and completed the survey, including doctors (n = 87) and nurses (n = 26), as well as a physiotherapist, pharmacist, and social worker. 88.7% of the sample had 5 or more years’ experience working in healthcare; 55.1% of the sample had at least 5 years working in palliative care. Professionals were based in the United Kingdom and Ireland. Sample characteristics are reported in Table 2.
Characteristics of the 116 Respondents That Completed the Survey.
Identifying Important Relationships With Children
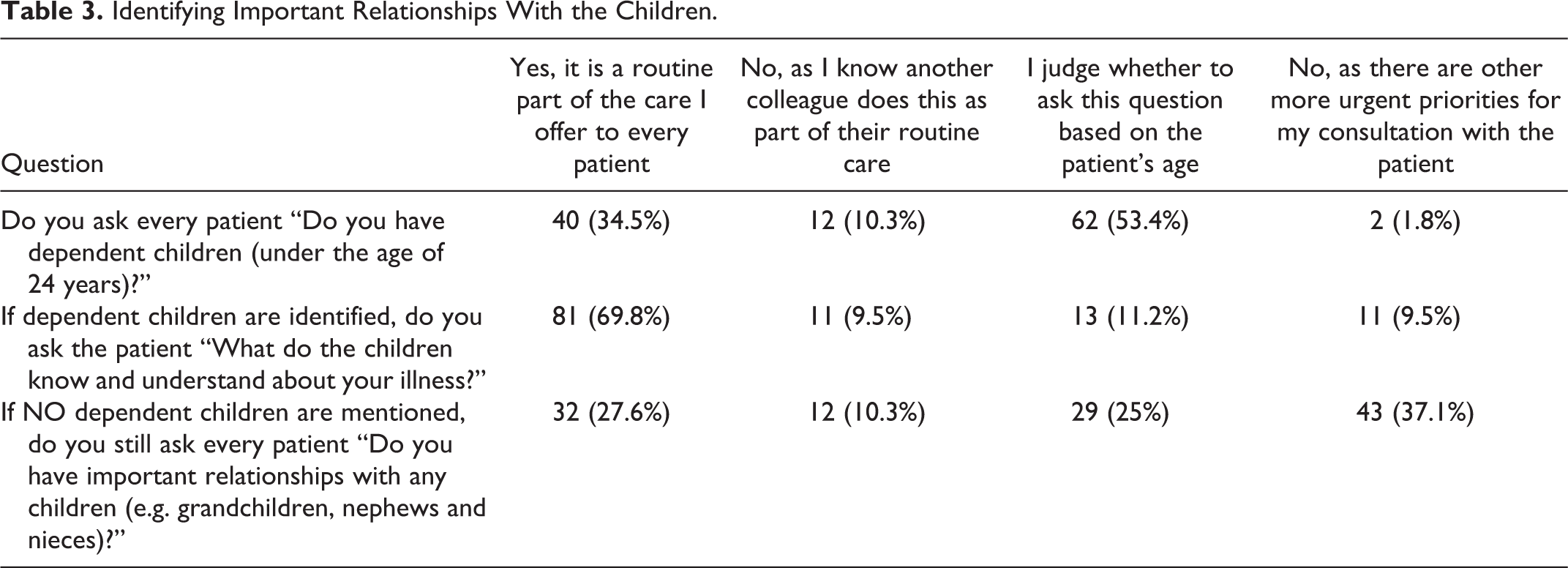
Over a third of respondents (40/116) reported it is a routine part of their practice to ask patients if they have dependent children. This contrasts with over 50% of the sample (62/116) that decide to ask a patient if they have dependent children based on the patient’s age. When no dependent children are mentioned by patients, most professionals (84/116) stated they do not ask the patient about any other important relationships with children (Table 3).
Identifying Important Relationships With the Children.
Providing Psychosocial Care to Families About the Children
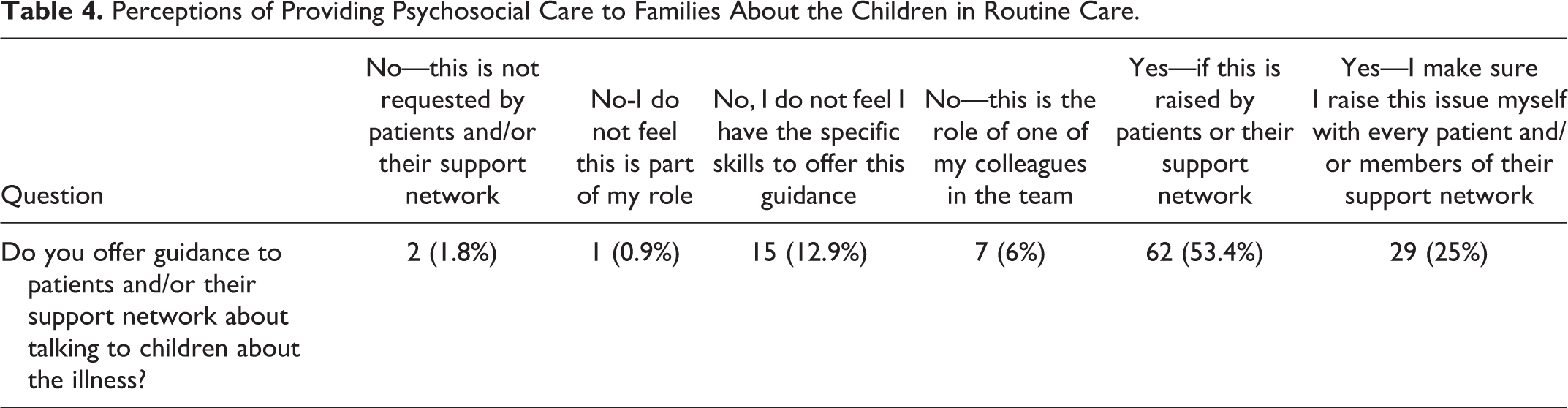
Less than a quarter of professionals (29/116) stated they raise the issue of how to talk to the children with every patient or a member of the family. Most respondents (62/116) reported that when the issue has been raised by the patients or their support network, they provide guidance to patients and/or their support networks about talking to their children about the illness (Table 4). Many respondents (64.7%) considered it to be their role to signpost patients and their support networks to appropriate resources and websites that provide family support, advice, and guidance on telling children about an illness.
Perceptions of Providing Psychosocial Care to Families About the Children in Routine Care.
Confidence and Skills to Deliver Family-Centered Care
While the majority of the professionals (73.2%) somewhat or strongly agreed they are confident initiating discussions about children (Table 5), 76.7% of respondents still reported a desire for training to deliver this aspect of care (Table 6). Professionals reported their preferred method of training would be videos demonstrating how to have conversations with patients about children (74/116; 63.8%), followed by classroom-based advanced communication skills training (67/116; 57.8%). Written materials such as leaflets and booklets were the least preferred choice for the provision of training (9/116; 7.8%).
Professionals’ Confidence in Initiating Discussions With Patients About the Children.

Professionals’ Views on Training About How to Support Patients to Talk to Children About Their Illness.

Discussion
There remains a critical gap in the provision of psychological care to families at end of life regarding the important relationships a patient has with children. Strikingly, the majority of professionals make a decision about whether to ask patients at end of life about relationships with children based on their age. This potentially overlooks children (e.g., grandchildren, nieces, nephews) who have a significant relationship with patients and may need support to understand their loved-one’s illness and death.
Most respondents felt confident about initiating conversations with patients at end of life about children, and described their involvement as signposting patients and families to websites and services that provide family support. A similar finding had been reported in the literature.2,3,7,10 However, the majority of professionals reported they want training to equip them with the skills and confidence to provide families with psychosocial support at end of life about children. Although evidence-based guidelines to scaffold raising these topics with patients are available,1,12 participants rated videos demonstrating how to deliver this aspect of care as their most preferred option for training (63.8%) followed by classroom-based courses (57.8%). There is a need to develop these specific resources, which would also be relevant to professionals working in many different medical specialties, with evidence indicating the benefits of raising these issues with patients earlier in their illness trajectory.2,7
Implications for Practice
One of the greatest challenges faced by families is how best to prepare and support their children for the death of an important adult.6,7,13,14 Parents’ need support and guidance from professionals on how to: (1) tell children someone important to them has a serious illness and is going to die, and (2) prepare children for the actual death.15,16 Children who are prepared for a death are reported to cope and adjust better in bereavement with less input from psychological services, compared to children who are unprepared for a death of an important adult.17,18 Alongside this, children want to be informed of the reality of an important adult’s illness and involved in the end of life experience.4,19 Healthcare teams are removed from the emotional tension within the family which places them in a position to encourage parents to “start the conversation” with the children about the reality of a patient’s illness.2,15 Talking about important relationships with children in clinical appointments offers families the permission to put children on the agenda.
Psychosocial support in relation to dependent children should be incorporated into all routine appointments in adult services, highlighting family-centered care is the clinical responsibility of all professionals, similar to that of Scandinavian countries. 19 To promote family-centered conversations in routine practice, it is important for professionals to ask all patients “do you have important relationships with children?” 9 Professionals should be reassured that while conversations about children can be upsetting for families and for clinicians themselves, bereaved relatives have reflected it would have been if the healthcare team had initiated a discussion about children’s needs before the death happened and encouraged families to involve the children in the end of life experience.7,9,20 Additionally, bereaved families describe the limitations of leaflets and websites about how to talk to children about illness and death. Rather, families want professionals to start the conversation with them (the patient /partner) about how to navigate the end of life experience with their children. 7 Professionals should be reassured that family-centered conversations do not need to be arduous or time consuming; short training resources such as video tutorials could equip clinicians with the skills to support the provision of family-centered care in practice.
Strengths and Limitations of the Study
While it may be argued a biased sample of professionals were included in this audit (respondents were attending a palliative care conference), findings highlight a need for training to support clinicians’ provision of family-centered care in routine practice. Findings represent a range of professionals providing end of life care throughout the United Kingdom and Ireland. The survey did not ask specific questions about professionals’ role in providing psychosocial support to families from minoritised groups; this should be investigated through future research.
Conclusion
Despite palliative care professionals’ advanced communication skills training, there remains a desire for further training to support and guide staff in talking to patients about the effect of the illness on children in their family. Professionals feels these skills would be best developed through specific video resources.
Footnotes
Authors’ Note
All authors were involved in the design and conduct of this study. Data analysis and manuscript preparation were completed by JRH. All authors have approved this version. The data that supports the findings of this study are available at the University of Oxford repository and available on request from the first author.
Acknowledgments
The authors would like to express their sincere thanks to the professionals who piloted the survey. We extend our gratitude to the 116 professionals that took the time to complete the questionnaire.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There was no direct funding award for conducting this study. Data analysis and manuscript preparation was supported by funding from the Westminster Foundation awarded to University of Oxford.