
Abstract
Introduction:
Advance care planning is recommended in chronic respiratory diseases, including Idiopathic Pulmonary Fibrosis. In practice, uptake remains low due to patient, physician and system-related factors, including lack of time, training and guidance on timing, components and content of conversations. Our aim was to explore perspectives, experiences and needs to inform a framework.
Methods:
We conducted a qualitative study in western Canada, using semi-structured interviews and inductive analysis. Patient, caregiver and health care professional participants described advance care planning experiences with Idiopathic Pulmonary Fibrosis.
Results:
Twenty participants were interviewed individually: 5 patients, 5 caregivers, 5 home care and 5 acute care health care professionals. Two categories, perceptions and recommendations, were identified with themes and subthemes. Participant perceptions were insufficient information and conversations occur late. Recommendations were: have earlier conversations; have open conversations; provide detailed information; and plan for end-of-life. Patients and caregivers wanted honesty, openness and clarity. Professionals related delayed timing to poor end-of-life care and distressing deaths. Home care professionals described comfort with and an engaged approach to advance care planning. Acute care professionals perceived lack of clarity of roles and described personal, patient and caregiver distress.
Interpretation:
Analysis of diverse experiences provided further understanding of advance care planning in Idiopathic Pulmonary Fibrosis. Advance care planning is desired by patients and caregivers early in their illness experience. Health care professionals described a need to clarify role, scope and responsibility. Practical guidance and training must be available to care providers to improve competency and confidence in these conversations.
Keywords
Advance care planning (ACP) is the ongoing communication process for individuals to consider their goals and preferences for medical care, discuss them with family and health care providers, and document and review them regularly. ACP conversations are foundational to patient-centered care in life-limiting illnesses, including Idiopathic Pulmonary Fibrosis (IPF), an incurable fibrotic lung disease with a mortality of 2 to 3 years after diagnosis. 1 IPF patients and caregivers suffer a poor quality of life marked by frustration and hopelessness, often magnified at end-of-life. 2,3 Evidence suggests ACP may improve quality of care and life by eliciting and addressing what matters most to patients and families, 4 and positively affect end-of-life care. 5 Unfortunately, ACP is inconsistently implemented in IPF despite multiple stakeholder recommendations. 2,6 -11 For example, Lindell et al reported 13.7% of IPF patients received a palliative care consultation. 12 Lack of ACP discussions is a known patient-clinician communication gap in IPF. 13 Identified barriers are health care professional (HCP) reluctance, an unpredictable disease trajectory, insufficient communication training, prioritization, and patient readiness. 2,8,14
In our provincial health system, ACP includes personal directives and medical goals of care orders (GOCs). Personal directives express preferences and name an agent if there is loss of decision making capacity; GOCs encompass wishes with medical decisions and location of care, including resuscitation, transfer to hospital, and comfort care. We sought to explore perspectives of IPF patients, family caregivers, and healthcare professionals on ACP-related experiences to understand and inform an ACP framework to guide clinicians and facilitate early, meaningful conversations.
Methods
Study Design and Population
We conducted a qualitative study and used the COnsolidated Criteria for REporting Qualitative Research (COREQ) guideline for reporting. Patients with IPF and family caregivers (PFCs) were recruited through the local Pulmonary Fibrosis Association and IPF specialists with convenience and snowball sampling. HCPs were recruited through email invitation letters to home care (HC) and acute care (AC). No incentives were provided.
Interviews
A semi-structured interview guide was developed from the literature and expert clinician input (see supplemental file), 6,15 -18 which included preferences on content, delivery format and settings for ACP conversations. Interviews were conducted after informed consent obtained by SO, research assistant trained by first author, MK. SO had no relationship to the participants or the Multidisciplinary Collaborative Interstitial Lung Disease (MDC-ILD) Clinic. PFCs were interviewed at the university (5), at home (2) or by phone (3). HCPs were interviewed in work settings.
Qualitative Analysis
Data were systematically analyzed with inductive content analysis, 19 led by CP, PhD trained and experienced qualitative researcher and conducted by CP, MK, and SO. Research procedures for anonymity, rigor, validity and reliability included: verbatim transcriptions; de-identification; content analysis of keywords, phrases and patterns; ongoing team discussion; consensus of descriptions; and final agreement on categories and themes. Data analysis was managed with Word© documents on a protected shared drive, with independent and shared analysis to minimize predetermined coding and anticipation of findings. Extensive personal experiences were shared with rich data across participant groups. Meaningful saturation was evident in emerging categories and repeating themes across and within responses. 20
Ethics Approval and Funding
The study was approved by the University of Alberta Health Research Ethics Board (HREB; #Pro00066208).
Results
Twenty participants were interviewed between July 20 and August 16, 2016 (Table 1). No participants withdrew. Detailed and rich descriptions of ACP perspectives and experiences were analyzed. Two categories, perceptions and recommendations, were identified with themes (Figure 1). Quotes were selected to exemplify findings and diversity of participant perspectives (Table 2).
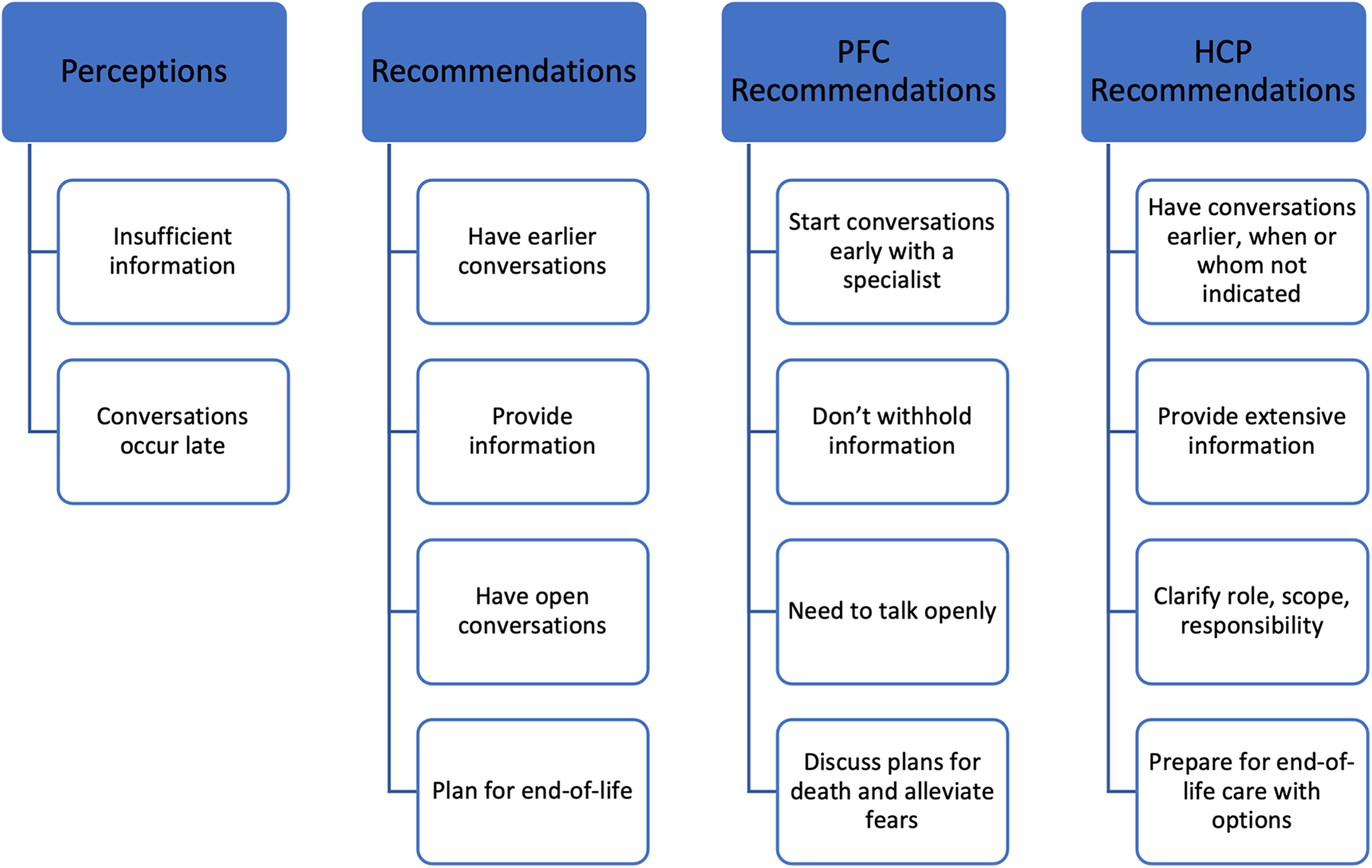
Categories, themes and subthemes identified from participant responses. PFC, patient and family caregiver participants; HCP, health care professional participants.
Participant Demographics and Interviews.
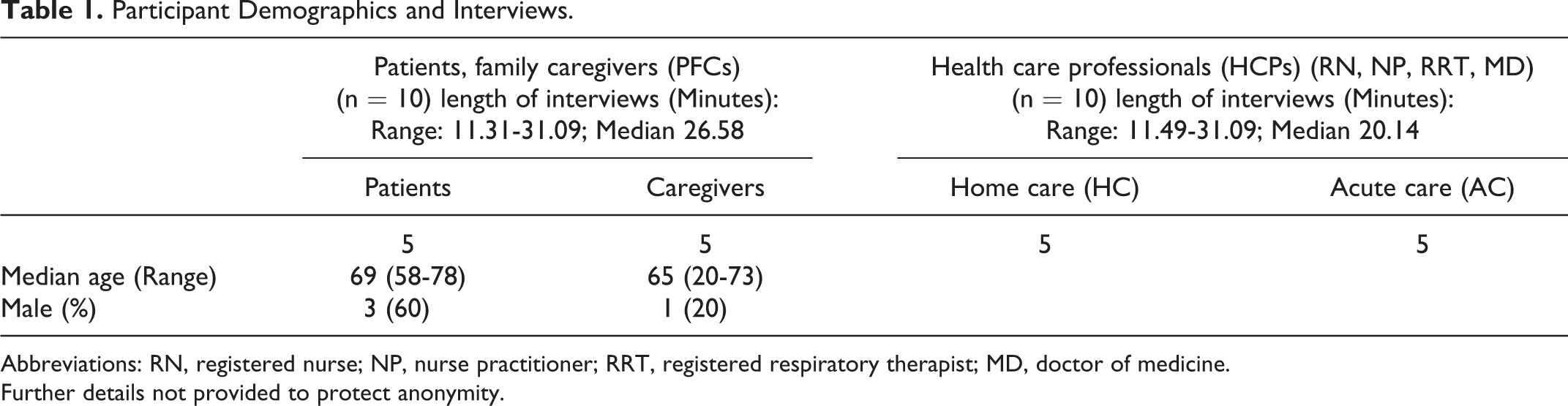
Abbreviations: RN, registered nurse; NP, nurse practitioner; RRT, registered respiratory therapist; MD, doctor of medicine.
Further details not provided to protect anonymity.
Quotes That Exemplify the Findings.
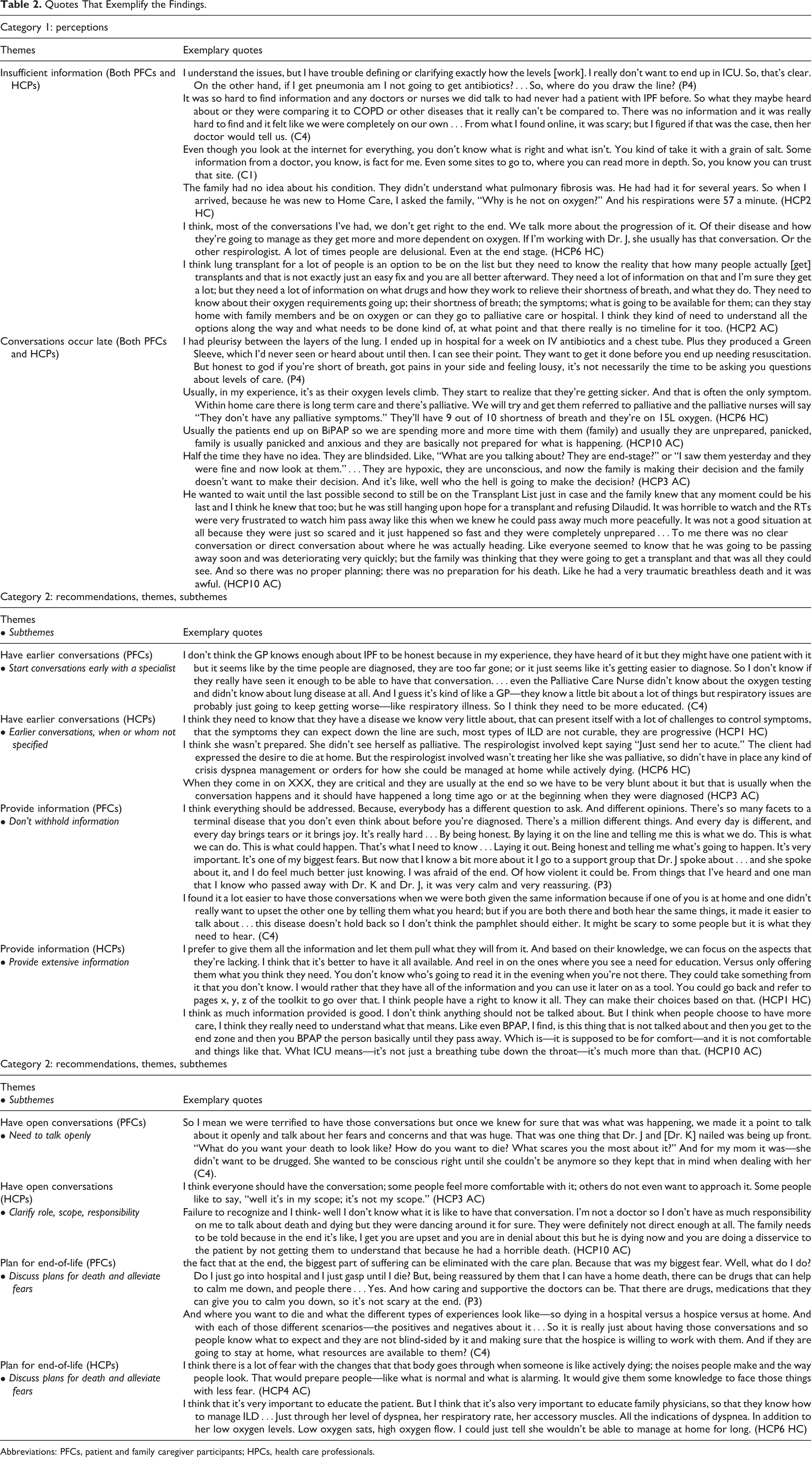
Abbreviations: PFCs, patient and family caregiver participants; HPCs, health care professionals.
Perceptions
Both groups shared the themes in this category: “insufficient information” and “conversations occur late”.
Insufficient information
Patient and family caregiver participants (PFCs) had challenges in obtaining and understanding ACP information. Some understood they had to do something but did not know what to do or how to prepare. One stated, “My wife did a lot of digging on her own to find it” (C3). PFCs indicated they had poor overall understanding of choices. One caregiver with previous experience indicated she understood most issues.
PFCs also found it challenging to find or trust resources, even when directed to the internet: “My wife keeps looking on the internet and we were advised to get as much information as possible off the web. And there’s loads of information. They’re not sure exactly what it is, but one thing they are sure, it’s fatal.” (P1). A few described the internet as bad or scary, and most were uncertain about the accuracy of information: “I actually didn’t find it reliable” (P4).
HCPs perceived PFCs did not have sufficient information about the disease or its trajectory. They agreed many HCPs do not have the conversations. One suggested patients were afraid or did not know how to ask questions, especially near end-of-life.
Conversations occur late
HCPs from all disciplines and both settings perceived ACP conversations occurred “quite late in the trajectory of their illness” (HCP8 HC). Even when the disease was rapidly progressing, the severity was not necessarily recognized. At times, conversations and goals of care orders (GOCs) were just in time to support patient wishes. One NP went to see a client “right away because I was afraid he would pass away” (HCP2 HC). It was positive when conversations were in time: “I had a lengthy conversation with her the first day I met her, because I knew she would not last long.” (HCP1 HC)
HCPs were concerned when near-death events occurred without patient or family caregiver readiness. “Usually they are unprepared, panicked, family is usually panicked and anxious and they are basically not prepared for what is happening.” (HCP10 AC). Rapid deterioration with no plan for complicated symptom management and end-of-life care was distressing for patients, family and HCPs.
Recommendations
There was overlap and variation of themes in this category: “have earlier conversations”; “have open conversations”; “provide detailed information”; and “plan for end-of-life.”
Have Earlier Conversations
All participants recommended initiating ACP conversations earlier. PFCs were more specific as to when and with whom conversations should occur.
Start conversations early with a specialist
PFCs recommended conversations be initiated early in the disease, “I think at diagnosis, obviously, you need to be told that this is not curable and it’s progressive and it will end your life.”(P4). Four patient and two caregiver participants indicated professional expertise and knowledge was important: “A general practitioner is not up on it, it’s not their specialty” (P1). Diverse disciplines were recommended: “An IPF specialist, maybe a nurse practitioner in IPF. Or a respiratory therapist who focuses only on IPF, or it’s in her role. Someone who’s really knowledgeable about it.” (P4).
Earlier conversations, when or whom not specified.
HCPs also recommended having conversations earlier, and debated who should have the conversations and when they should start. They focused on challenges when conversations did not occur earlier.
Provide Information
The second theme was provision of information. PFCs recommended information not be withheld, whereas HCPs recommended extensive information be actively provided.
Don’t withhold information
PFCs sought information about their disease, quality of life, care options, symptom self-management, and alleviation of fears. They emphasized the importance of information and perceived HCPs withheld it. Caregivers emphasized the significance of knowing, not “holding back” (C4), even when dwelling on the finality of the disease. C5 described “the necessity for ACP” and how “important this planning is.” Some caregivers indicated they needed more information, or more often, than the patient to plan, “so no, don’t hold back” (C1).
Provide extensive information
HCPs recommended providing extensive information, then letting patients determine what they need to know more about. They noted specific questions may be challenging, primarily about fears and symptoms. Examples of “main questions” patients asked were: “Am I going to suffocate to death?”; “Is my breathing ever going to get better?”; “How am I going to be comfortable?” (HCP7 HC). No HCPs reported PFCs asking about intubation or resuscitation although AC HCPs noted the importance of discussing these, including non-invasive ventilation.
Have Open Conversations
The third theme described the context and processes that enable or challenge conversations.
Need to talk openly
PFCs recognized the uncertainty of the disease and their situations, and did not expect specifics. ACP conversations were reassuring, enabled planning and alleviated fears. Desired information included: “What’s likely to happen. I realize things can’t be black and white, but they can be a little bit more defined” (P4). Most perceived physicians and nurses would initiate conversations.
Clarify role, scope, responsibility
HCPs agreed with earlier and ongoing ACP, however, there was uncertainty about who was to initiate conversations. They indicated conversations should occur “continuously” with various professionals as the disease progressed (HCP4 AC). One recommended “specialists should explain it to them and the nurse, the home care nurse and kind of in that order.” (HCP9 HC)
Roles, scope, and responsibilities were unclear and challenging among acute care HCPs. Several suggested family physicians should lead conversations, because they know the patients, but then acknowledged, physicians say “specialists should be having these conversations.” Subsequently, conversations may occur “unfortunately for many patients, in the middle of a crisis in the Emergency Department” or “at the very, very end.” (HCP5 AC) Even when confident to have conversations, acute care professionals suggested physicians should initiate them, and expressed uncertainty about their roles, “I do feel confident; but in my place for it to be appropriate for me to talk about it. I don’t really know where I fit in to be honest.” (HCP10 AC) Although most professionals in acute care had had conversations, all perceived they occurred late or in a crisis: “It is usually when they are too critical and it’s at the end.” (HCP3 AC)
Home care HCPs discussed having a relationship with the person, “building trust” (HCP2 HC) and having rapport. Most thought conversations should not “fall on one person.” One expressed that all involved in the client’s care “has a responsibility to assess the level of knowledge and to assess their level of preparedness.” (HCP1 HC).
Plan for End-of-life
Although ACP is broader than end-of-life, all participants had recommendations for this aspect.
Discuss plans for death and alleviate fears
All PFCs recognized IPF as a terminal disease. They sought information to understand and prepare for disease progression. Information provided hope, encouragement and quality of life: “I want to know what to expect, what’s coming down the line. To me, I think that is something that should be at the beginning” (C5). P3’s home death care plan alleviated his fears and he did not “want to go into a hospital and have them do something totally different.” Caregivers recommended information be provided about different scenarios and options for end-of-life, resources, access and contacts, and how to “navigate the system” (C5).
Prepare for end-of-life care with options
HCPs recognized the value and importance of end-of-life conversations including symptom management, preferred place-of-death, and available resources. Options and “all of the alternatives to hospitals are not really brought forward as much as they could be” (HCP10 AC). If a home death is preferred, people need to be prepared: “it will take some work and it will take some preparation” and “not everybody can die at home” (HCP2 HC). Several HCPs recommended specialized knowledge for this population to support conversations, including quality of dying and end-of-life care. They noted that family physicians needed to be prepared and educated.
Discussion
PFCs in our study desired open, honest communication, and expected HCPs to initiate conversations early. Similar to other studies, these PFCs lacked understanding of care choices 8,21 and described insufficient ACP information and resources. 21,22 They preferred to engage with knowledgeable and experienced professionals, which also aligns with previous findings. 23 -25 In contrast, some HCPs perceived patients and caregivers were afraid to ask questions, unsure or hesitant to engage in ACP conversations. This contradiction is described in the literature, where patients and professionals perceive the other as reluctant and expect the other to initiate ACP conversations. 14,26 Both groups agreed on ACP topics, in contrast to Rozenberg et al who reported health professionals ranked IPF drug therapy as an important information topic whereas patients and caregivers ranked end-of-life care as important. 27 Clinicians need to recognize the benefits of discussing ACP and consciously engage in early conversations. 28,29 Overall recommendations for ACP topics, timing, and context align with previous studies. 17,30,31 Similar to You et al, prognosis, identifying values, addressing fears or concerns and end-of-life care preferences were included. 32 Desired end-of-life topics included symptom management, non-invasive ventilation and place of care options. Some caregivers identified they wanted or needed additional information for planning, thus caregivers may require tailored information at different times. 4
All participants recommended providing detailed and extensive information, although not their experiences. Most patient participants expressed wanting to learn about end-of-life, signifying the importance of this topic, regardless of the severity of IPF. Many patients may ask about timelines but expect information on the dying process, care options, dyspnea management, and want hope and support for themselves and their families. When conversations extend beyond do-not-resuscitate orders to address fears, elicit goals, values and preferences, and provide reassurance that symptoms may be managed, they facilitate planning, enable a shift to focusing on making memories and accomplishing goals, and bringing meaning and dignity when living and dying with IPF. 4 Kylmä et al reported that providing honest information about the patient’s illness can contribute to patient hope; death and dying conversations give patients a sense of control and lessen their fears. 33 Learning about end-of-life options may enable patients to make informed choices and decrease risk of acute or critical care deaths. Most ILD patients prefer home or hospice deaths, thus planning for symptom self-management, home care support and knowledge of preferred place of death is essential. 34 Knowledge of end-of-life home or hospice care options, competency in refractory breathlessness management, and collaboration between physicians and community teams are paramount to providing patient-centered care and good quality of death and dying in IPF.
With limited treatment options and an unpredictable trajectory, IPF patients may feel more confident about their plans and worry less about future symptoms when informative and wholesome conversations are held early, so they can focus on living life in the time they have left. 26,35 Of importance, HCPs relayed distress at death, similar to Bajwah et al. 8 Lack of ACP is a missed opportunity and failure for this patient population globally. 10 -12
There were notable differences in HCP perceptions between care settings; home care HCPs engaged in conversations independently and confidently within their roles. Acute care HCPs indicated confusion of roles and responsibilities that impeded engagement in ACP conversations. Lack of role clarity has been described as an important barrier to ACP. 36 Al Hamayel and colleagues suggested older patients may require time to conceptualize their wishes before documenting them or engaging with others. 37 Introducing concepts earlier in primary care may be a useful strategy for IPF patients who are referred to specialty clinics, home care or transplant programs where conversations are continued.
PFCs recommended formal training which aligns with other recommendations. 38 Communication skills can be learned as any other clinical skills, with numerous programs ranging from seminars to workshops and online learning platforms, such as the Serious Illness Conversation Guide (SICG) and The Conversation Project. 39 SICG includes exploring the patient’s understanding of their illness, then their wishes, priorities, fears, strengths and prognosis. Other evidence-based models of patient-clinician communication emphasize prioritizing ACP conversations, making time to establish a rapport, eliciting patient perspectives, concerns, and wishes, explicitly demonstrating empathy and engaging in shared decision-making. 40,41 The SPIKES approach recommends setting up the conversation, assessing patient perception, obtaining patient invitation to engage in discussion, providing individualized information and knowledge, addressing emotion with empathy, and ending with providing a strategy and summary that is easily understood. 42 From the literature and these findings, we propose a framework for ACP discussions in IPF to guide clinicians in implementing early, meaningful conversations (Figure 2; Table 3). ACP conversations are prioritized, fears regarding death openly addressed; patients and families empowered through self-management strategies and information; and connections to support groups and home care facilitated. Caregivers are engaged at each and every step through invitation to attend clinics and participate in decision-making. This approach includes the core components highlighted in the National Cancer Institute’s commissioned monograph on patient-centered communication in cancer. 43
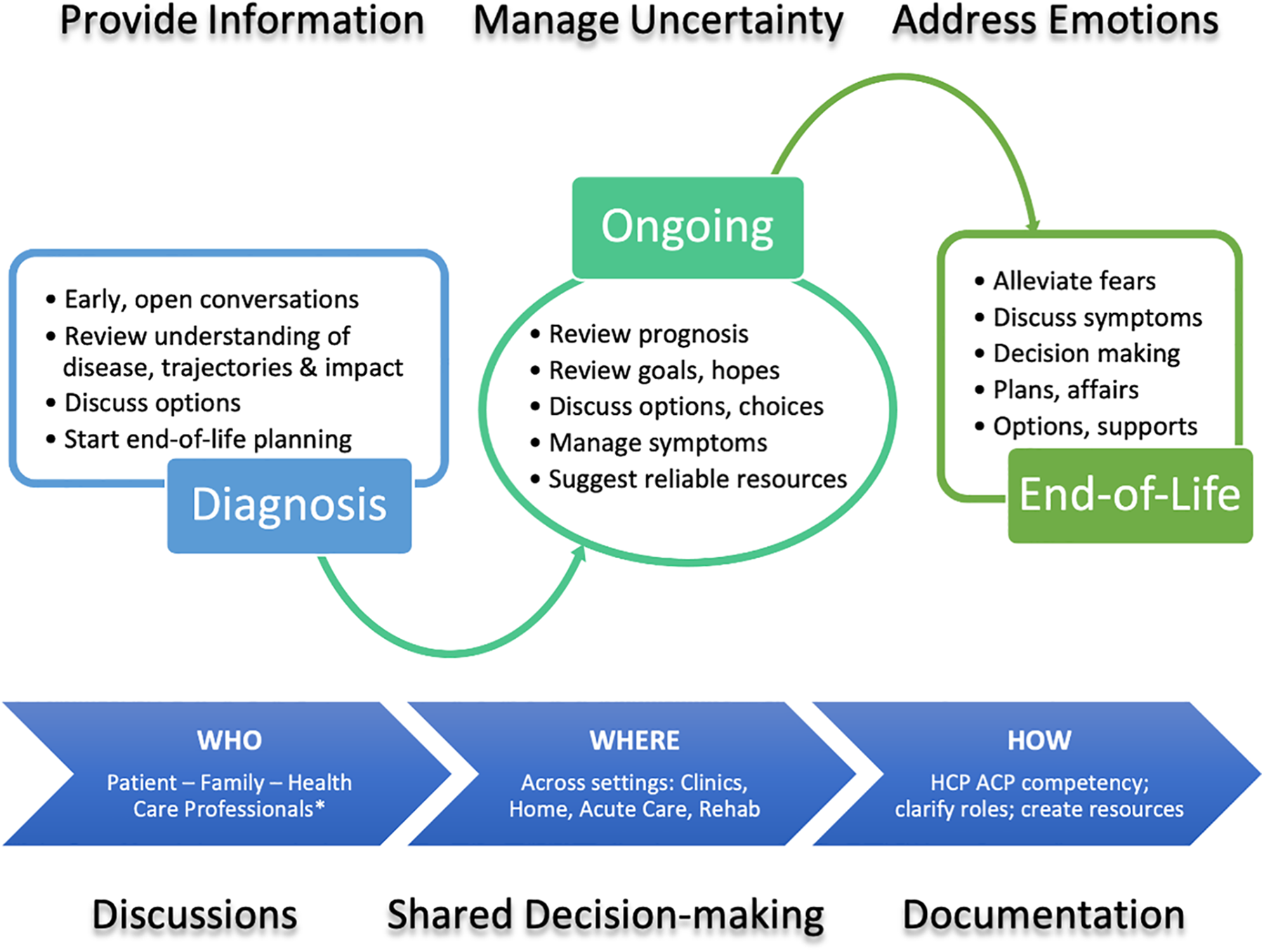
Framework for ACP discussions in IPF. HCP, health care professional participants; ACP, advance care planning. * Specialist and primary care physicians, nurses, nurse practitioners, allied health.
Framework: Individualized Advance Care Planning Conversations With IPF Patients and Caregivers.
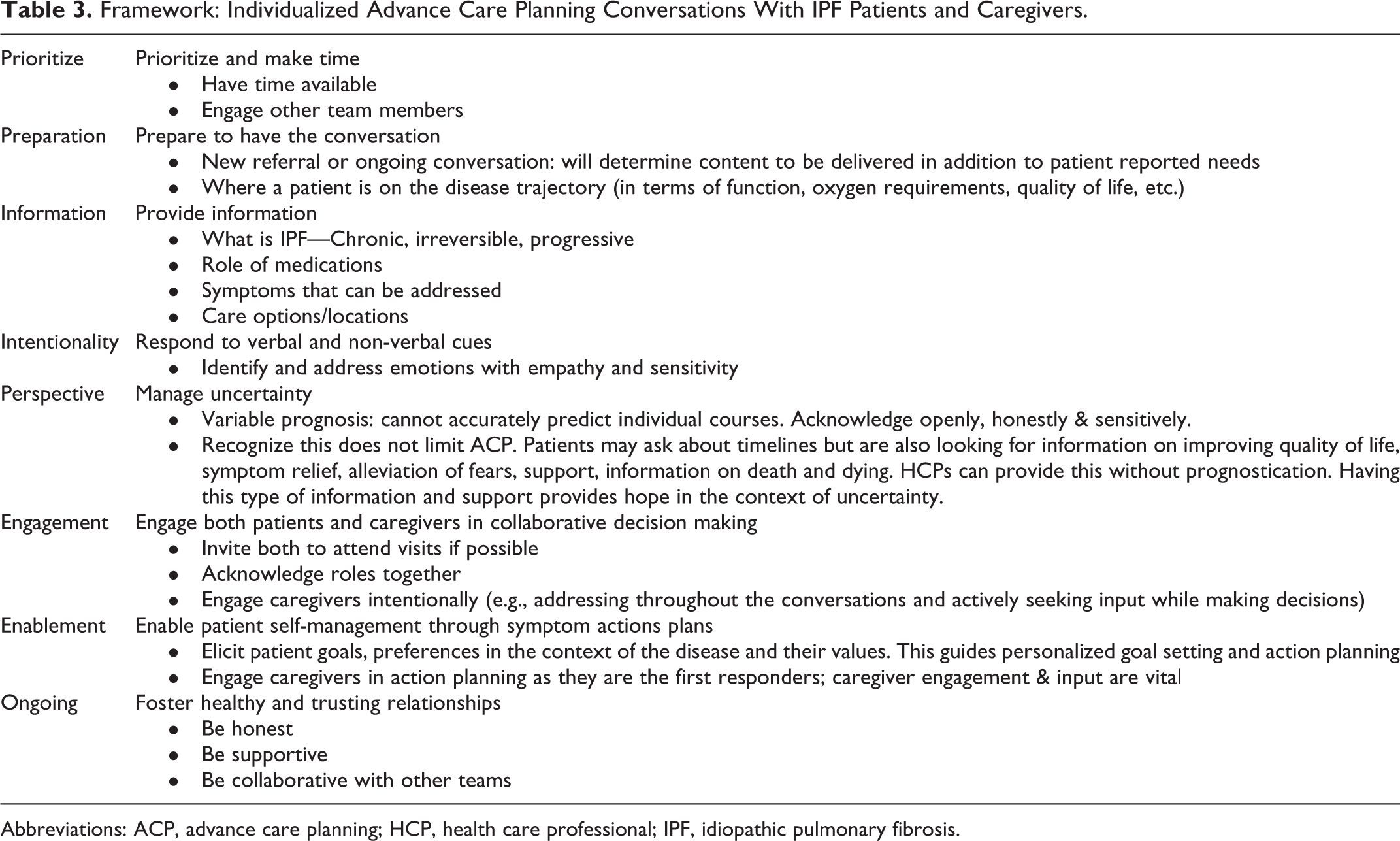
Abbreviations: ACP, advance care planning; HCP, health care professional; IPF, idiopathic pulmonary fibrosis.
Strengths and Limitations
Ethnic and cultural diversity were unintentionally limited in both participant groups; the majority were Caucasian. Some HCPs had previous training and support from specialists in an integrated palliative approach for IPF, and therefore expected to have more confidence and experience in ACP conversations. Strengths include the rich descriptions from perspectives of PFCs and HCPs from both acute and community settings. This is the first known study that revealed the distress and burden experienced by HCP in hospital settings where HCPs perceived palliative needs were neither identified nor openly discussed, and indicated the opportunity for ACP to improve end-of-life care.
Conclusion
Advance care planning is desired by patients and caregivers living with IPF, encouraged by HCPs, although numerous challenges and barriers exist. Potential for distress at end-of-life emphasizes the need for early ACP conversations. HCPs should discuss available end-of-life options, including home and hospice. Recognition by HCPs that ACP is more than do not attempt resuscitation orders, but a holistic communication process that addresses symptoms, psychosocial and emotional needs, relieves fears, promotes hope and elicits engagement, may in turn address HCP concerns of taking away patient hope. Practical guidance and training to improve HCP competency and confidence in ACP are needed, in addition to clarity within organizations as to scope, policy and responsibilities.
Supplemental Material
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211041724 - Advance Care Planning Needs in Idiopathic Pulmonary Fibrosis: A Qualitative Study
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211041724 for Advance Care Planning Needs in Idiopathic Pulmonary Fibrosis: A Qualitative Study by Meena Kalluri, Sara Orenstein, Nathan Archibald and Charlotte Pooler in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material, sj-pdf-2-ajh-10.1177_10499091211041724 - Advance Care Planning Needs in Idiopathic Pulmonary Fibrosis: A Qualitative Study
Supplemental Material, sj-pdf-2-ajh-10.1177_10499091211041724 for Advance Care Planning Needs in Idiopathic Pulmonary Fibrosis: A Qualitative Study by Meena Kalluri, Sara Orenstein, Nathan Archibald and Charlotte Pooler in American Journal of Hospice and Palliative Medicine®
Footnotes
Authors’ Note
CP, SO and MK contributed to the study design. SO collected the data. CP, SO and MK analyzed the data. All authors contributed to data interpretation, drafted, revised and approved the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the University of Calgary 2016 Summer Studentship of the Health Professions Education Grant Program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.