
Abstract
Aim:
To describe healthcare professionals’ and volunteers’ experiences of a pathway for movement on a hospice ward.
Method:
This was a qualitative study with an inductive approach. Data were collected in a hospice setting through 4 focus group interviews with healthcare professionals and volunteers (n = 12). The focus group participants varied in age, profession, and length of experience in palliative care. The interviews were audio recorded, transcribed and analyzed with qualitative content analysis.
Results:
Dignity through movement at the end of life was the main theme, complemented by 4 sub-themes. Two descriptive sub-themes: “A practical tool to facilitate physical activity” and “Companionship and goals give meaning to the day,” and 2 interpretative sub-themes: “Regaining control and having a choice” and “Feeling normal and alive” based on participants’ views of patient experiences.
Significance of Results:
Indications are that the pathway for movement addresses a wide range of experiences related to different aspects of being human in a difficult situation. Experiences of movement and physical activity can promote wellbeing, dignity, and a sense of feeling “at home” for patients within hospice care. The pathway for movement is simple to set up, offers access to appropriate physical activity and seems to benefit patients both in the early and later phases of palliative care.
Introduction
Palliative care is based on a holistic view of humankind, in which the physical, psychological, social, spiritual and existential dimensions are interwoven.1-3 The World Health Organization’s definition of palliative care affirms quality of life and dignity, in helping patients “live as actively as possible until death.” 4 Dignity is a multifaceted concept involving human value, a person’s social position, ethical actions and personal identity within a larger group. 5 Symptom distress, ability to preserve their core identity and roles as well as level of autonomy contribute to patients’ perceptions of dignity at the end of life, in effect promoting courage to live despite existential pain. 6 Palliative care has developed significantly during the past 30 years, resulting in a longer palliative phase of illness, 7 and repeated periods of inpatient care. Without the possibility to be physically active while in hospital, there is a risk that patients will lose their independence.
The human body is built for movement and goal-oriented activity activities, as well as being the medium through which we experience and communicate with the world.8,9 In normal functioning, the body is perceived as invisible and unnoticed, all its different parts automatically integrated 10 but in sickness the body demands attention and becomes an object for treatment. Merleau-Ponty identified dualistic positivisms separation of the person into body and mind as a problem, and believed that in order to understand the whole person, one must also understand their context. The “Lived body” theory describes all aspects of human existence, body, mind and the present situation, as woven together in a constant interplay creating meaning. The unpredictable and failing body disturbs this interplay and can cause feelings of alienation and homelessness, with a person neither feeling at home in their body nor in their social relationships.11,12 There is a strong link between patients’ perceptions of dignity and the body’s deterioration, because all aspects of daily life are affected by the loss of the previous “taken for granted” body.6,13 Lawton 14 describes the extreme situation of “fragmentation” in which the patient retreats inwards and closes off due to overwhelming feelings of helplessness and despair.
Physical activity and exercise training have shown positive effects on fatigue, daily function and mood in patients with advanced cancer.15-17 However research regarding the experience of movement with focus on body awareness is scarce, and whether movement positively affects wellbeing for weaker patients in the later phases of palliative care warrants exploration. The aim of this study was to describe healthcare professionals’ (HCP) and volunteers’ experiences, observations, and reflections over a pathway for movement on a specialized palliative care unit.
Methods
The was a qualitative interview study with an inductive approach.
Setting
One of the authors is a registered physiotherapist working in a hospice with 20 single rooms in an urban area in Sweden. During 2019, 388 patients were cared for, 70% of whom died there, with the remaining 30% discharged, often to “Hospice at Home” or other care. The average length of stay in 2019 was 17 days. Patients’ functional levels varied from being confined to bed to being mobile, occasionally even to climbing stairs.
The Body Awareness Movement Pathway (BAMP) was prepared January – May 2019 and started in June 2019 with 4 stations (armchair cycling, sitting-standing, pulling therapy band, mindfulness breathing) and a 60 m walk, see Appendix 1.
Participants
All HCPs or volunteers in hospice during May-June 2019 were informed about the BAMP at a staff meeting and through email. Written information and a map were posted in the unit. Each station had a picture and written instructions.
Data Collection
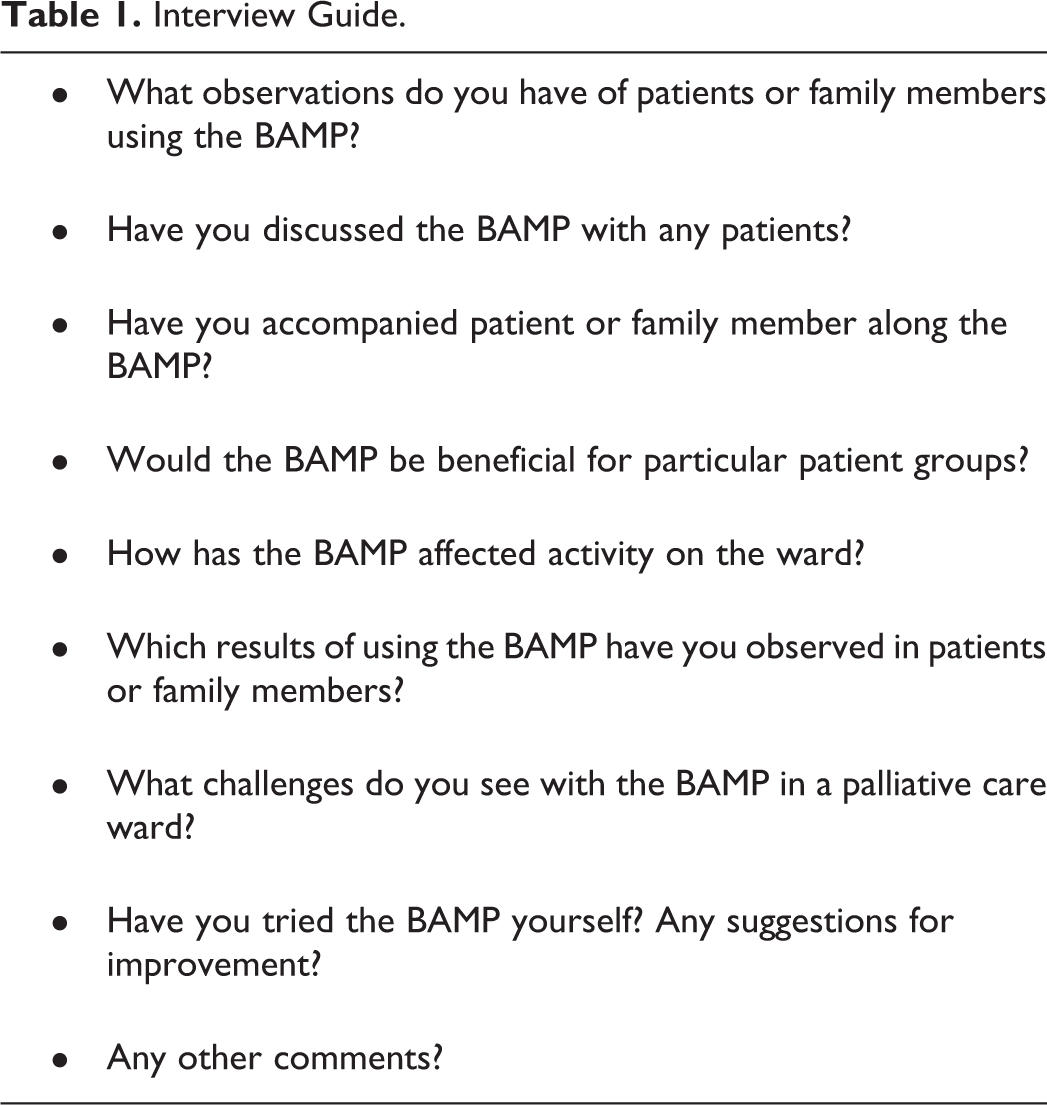
Data were collected through focus group interviews with HCPs and volunteers. 18 The unit manager invited all staff to participate and informed that it was voluntary. Four focus group interviews of 45-60 minutes were conducted, with 2 to 6 participants in each (n = 12). Nine of the interviewees were clinical staff. Authors AJ and AK facilitated all interviews. A list of questions was used to initiate discussion, with probes for elaboration, see Table 1.
Interview Guide.
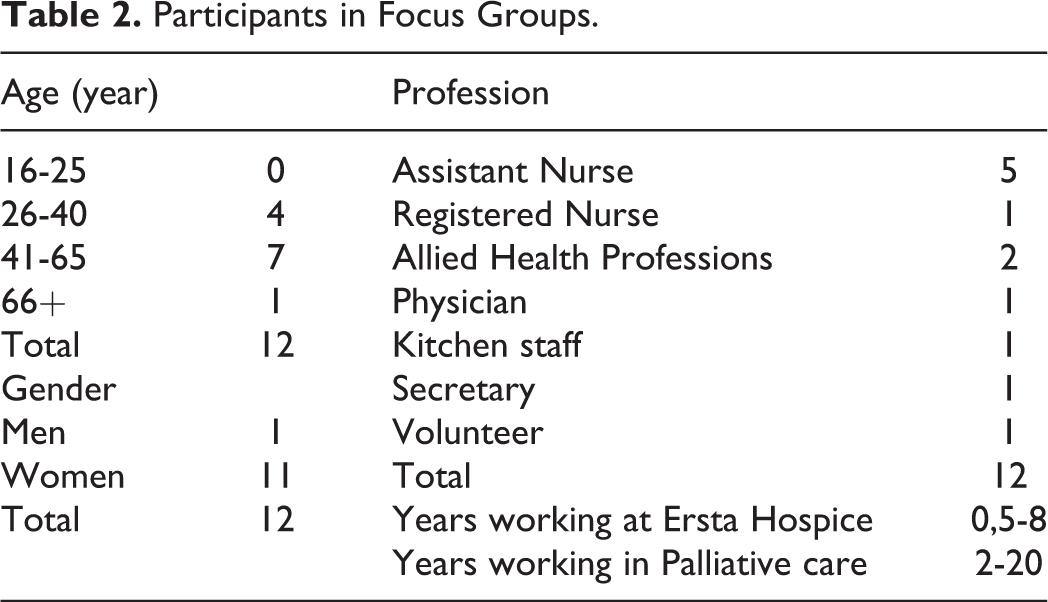
Written informed consent was explained and collected at the start of each interview. Demographic data are shown in Table 2. Interviews were audio recorded and transcribed verbatim.
Participants in Focus Groups.
Data Analysis
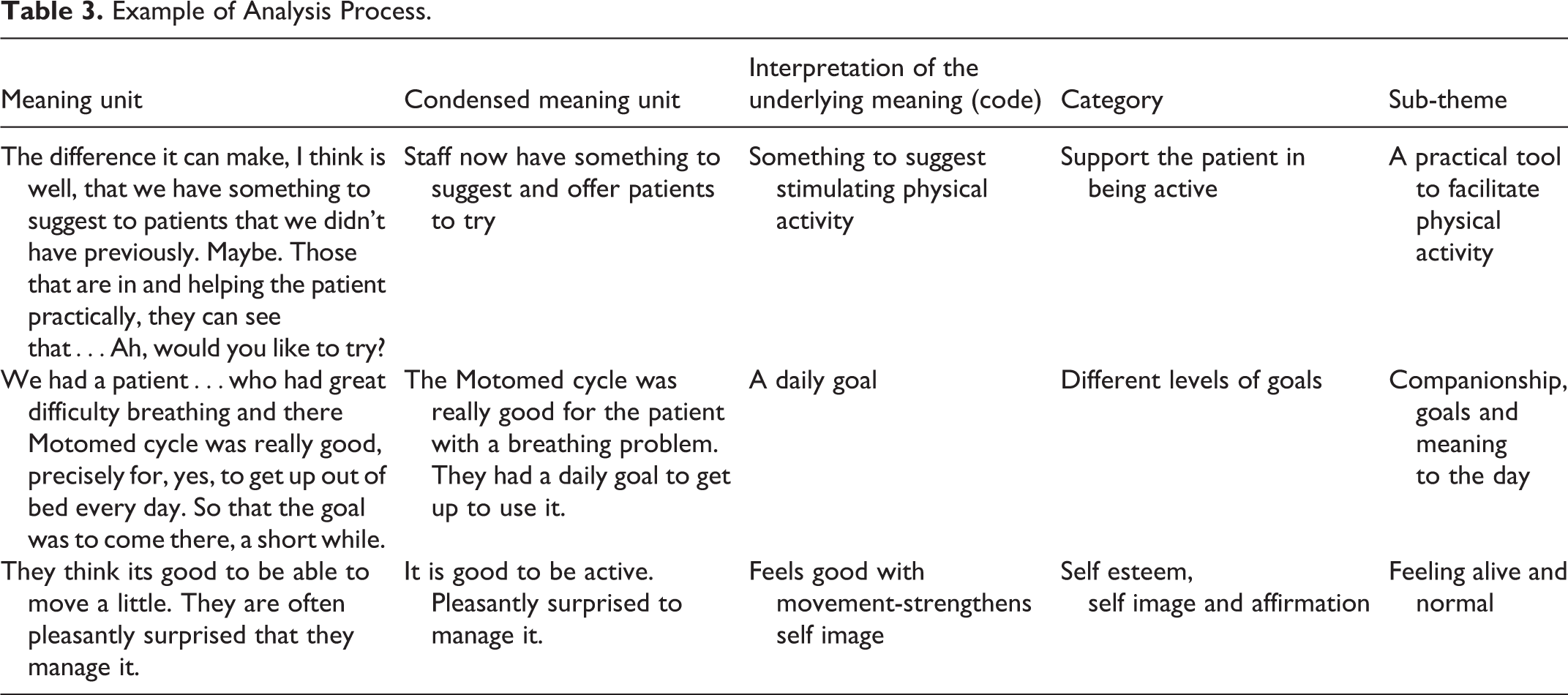
All data were analyzed with qualitative content analysis.19,20 Each interview was read through several times, before being divided into meaning units. These were condensed whilst preserving the meaning. All codes were manually organized in mind maps (using the software application ´Simple Mind´), one for each interview. Similarities and differences were then compared and clustered in varying combinations to eventually form categories. In the final stage of the process, authors brainstormed together to reach consensus in connections between the categories, thus forming four sub themes and one main theme, see Table 3.
Example of Analysis Process.
The research protocol for the study was reviewed and ethical approval granted by Ersta Sköndal Bräcke University College, number 1908-A, see Appendix 2 [in Swedish].
Results
The first two sub themes: “A practical tool to facilitate physical activity” and “Companionship and goals give meaning to the day” were descriptive, based on the participants’ observations and experiences. The other two sub themes: “Regaining control and having a choice” and “Feeling normal and alive” were more abstract and addressed underlying nuances. The four sub themes were gathered under the main theme: “Dignity through movement at the end of life.”
A Practical Tool to Facilitate Physical Activity
Participants described the BAMP as an asset, something structured and positive to offer patients, as well as to inform relatives and visitors about. HCPs who enjoyed being active themselves, saw a particular value in movement and were glad to see patients using the pathway. “…it is a great step forwards, but I would never be able to say it to her…because then she would directly close herself off, but it is really..., anyway, it is lovely to see.” (Focus group 4) “…it is a constant dilemma, you can see people…that you could motivate, but we have so many other very sick patients…there is the wish to help. It is anyway a problem for us.” (Focus group 4)
Companionship and Goals Bring Meaning to the Day
The stations became meeting places for family and visitors around the patient. This provided opportunity for relaxed companionship and a place to socialize. Patients and HCPs also experienced companionship when the BAMP became the focus for a conversation. Sometimes the patient initiated this with a request for help or to report that they were “off to cycle,” later proudly reporting BAMP use. At other times HCPs initiated conversation with patients. “I remember a short spontaneous exchange of words there…I know that getting encouragement myself like…” Are you sitting here? Wow, well done, you’re doing great”…I know myself that it is motivating.” (Focus group 4) “That you can have some control over your body and…process thoughts and feelings and sometimes it is also positive to come out from the patient’s room a few minutes, collect yourself…get a little energy from breathing different air for 5 minutes.” (Focus group 1) “She had a goal ‘no, I have to become well…I am not ready to die!’ and so I think that you, sort of, in that state get power like, when you have a goal, then you get…more energy from being able to train and the body coping with it.” (Focus group 2)
Regaining Control and Having a Choice
The participants supposed that having control over the body in movement could be a way for patients to work through thoughts about loss and death. Patients became more aware of how different parts of the body were still able to function, and this led to a feeling of control and independence that seemed to calm confusion and restlessness. “Because some patients say: ‘Oh wonderful that I feel where my legs are…that I can pedal, I can lift them. I’m not just lying in bed like…a package, but I can move’.” (Focus group 2) “But I think that you always have a group of patients who maybe struggle a little more with loss and…the thought of dying. And these patients…are…also those…that have the greatest need of getting control over something, when you no longer can control all the losses you have had.” (Focus group 1) “I avoid disturbing the patients I see using the pathway for movement. Because I think that it is theirs, their pathway and not mine, in fact.” (Focus group 1) “Sometimes I hear ‘No, I can’t do that now because in half an hour I’m going to do the BAMP and I need to gather strength for that’.” (Focus group 1)
Feeling Normal and Alive
Patients often felt good after doing the BAMP and were eager to tell others of their accomplishments. They frequently related feedback from the Motomed cycle about the distance traveled or the level of resistance as a testimony to their efforts. “But also maybe a feeling that you can do something…you lie in bed for 23 hours of the day…and then you pull yourself out of bed and cycle…5 minutes and maybe that’s that, yes, but I did it and that maybe is more than just a good feeling…I understand that there is more of a deeper meaning.” (Focus group 4) “You could also think that the BAMP helps people to work through their feelings so that when their abilities diminish and they can no longer follow the Pathway, then they have accepted their situation.” (Focus group 1) “I believe that it has increased the quality of life in some way you could say. Made that last time…of life much more,…valuable.” (Focus group 2) “There is a delightful feeling I think of being able to relax because of tiredness…that you have exerted yourself or you’re just tired because you’re sick. That’s a difference that I have seen a few times.” (Focus group 1)
Discussion
The results indicated that the BAMP stimulated a variety of experiences related to being human with severe life limiting illness. Impressions were that using the BAMP contributed to promoting well-being and dignity through a holistic experience of the body as well as supporting social relationships and roles.
Studies have shown positive experiences related to physical activity in patients with advanced cancer, such as reduced fatigue, increased hope, 21 coping and psychological well-being, 15 as well as improved mood and quality of life. 16 However, in these studies physical strength and fitness, rather than the experience of movement, have been the focus. Results from this study indicate positive outcomes from directing awareness to the body during movement. Participants described that even a relatively short period of movement seemed to be enjoyable for patients, a comfortable feeling of being alive and able to do something with the body, despite having little energy. These are important factors for quality of life.4,22
Merleau-Pontys’ theory of the “lived body” is particularly relevant in understanding the complex phenomenon, in which the usually friction free relationship between all the aspects of being human, can become strained due to sickness and suffering. 10 Movement has potential to create meaningful interactions within the lived body and its current situation, for example even awareness of small movements during breathing has shown benefit for relaxation and anxiety relief. 23 Furthermore, increased contact with, and awareness of the body as it presents with life threatening illness, may create a foundation from which patients are willing to accept change, create new meaning and find the feeling of being “at home” in the body again. 9
Within caring sciences, researchers have suggested that a focus of care should be promoting meaning, control and helping patients find their way back to being “at home” in their body.9,12 Participants in this study described how patients’ ability to decide if, and when, they would follow the BAMP was significant. For seriously ill patients, the possibility of making individual decisions has been described as strengthening self-determination, creating normality and thus conferring dignity.6,24 Gulde et al 21 similarly reported that patients who had been physically active before illness, experienced that the possibility to continue moving, supported their identity, and created a feeling of control. The sense of being independent and having control have been suggested as two of the most important aspects during the end of life.25,26
Even though the instructions at the BAMP stations encouraged awareness of the movement in the body, many patients seemed focused on physical exercise, reporting their achievements with pride. This can be understood as a human trait, giving attention to the body as an object for care when it ceases to function as normal and thereby becomes visible. The object and its parts become the focus for strength and fitness training, and this overshadows the body as a subject, the experiencer of life. 9 This leaning toward physical training may however give positive consequences (albeit temporary) including increased strength, balance and consequently independence in moving, which in turn builds self-image and autonomy, important aspects of dignity.6,22,27
The study was implemented at first author’s place of work, and she was involved in developing and setting up the BAMP, as well as giving information about the project and its goals on the unit. Consequently, there was a risk of bias, although measures were taken to reduce this risk. Using a BAMP in palliative and hospice care is feasible, however further feasibility and pilot testing with elements of randomization are recommended to validate the model. The main limitation of the study is the lack of direct input from patients. Future studies may remedy this by investigating patients’ perspectives.
Clinical Implications
Present research supports the use of training and other rehabilitation methods to reduce fatigue, dyspnea, and pain as well as improving mood for patients within palliative care. Designing a BAMP for bed bound patients would increase the possibility for those in the last stages of palliative care to be physically active.
Conclusion
This study addressed the understanding of the experience of movement in a structured pathway for patients in a hospice context. The physical, psychological, social, and existential aspects of being the “lived body,” a person in a difficult situation, emerged in the results. Performing bodily movements in the end of life may support patients’ identity and autonomy, thereby promoting their wellbeing and dignity. The pathway for movement can also be a useful instrument for facilitating physical activity as well as stimulating community for patients in hospice.
Supplemental Material
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211017876 - Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211017876 for Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals by Fiona Cameron, Anna Janze and Anna Klarare in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material, sj-pdf-2-ajh-10.1177_10499091211017876 - Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals
Supplemental Material, sj-pdf-2-ajh-10.1177_10499091211017876 for Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals by Fiona Cameron, Anna Janze and Anna Klarare in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material, sj-pdf-3-ajh-10.1177_10499091211017876 - Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals
Supplemental Material, sj-pdf-3-ajh-10.1177_10499091211017876 for Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals by Fiona Cameron, Anna Janze and Anna Klarare in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material, sj-pdf-4-ajh-10.1177_10499091211017876 - Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals
Supplemental Material, sj-pdf-4-ajh-10.1177_10499091211017876 for Homecoming—Dignity Through Movement at the End of Life: A Qualitative Interview Study With Healthcare Professionals by Fiona Cameron, Anna Janze and Anna Klarare in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
Great thanks to healthcare professionals and volunteers at Ersta Hospice for their involvement and support during this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.