
Abstract
Background:
It is estimated that in 2050 one quarter of the population in Europe will be aged 65 years and older. Although the added value of a palliative care team is emphasized in the literature, the impact of the palliative care team on the symptom burden in older non-cancer patients is not yet well established.
Objectives:
To structurally measure symptoms and to investigate whether proactive consultation with a palliative care team results in improvement of symptoms.
Design:
This study has a prospective comparative design.
Setting/Participants:
Older patients, admitted to a Dutch University Medical Centre for who a health care professional had a negative response to the Surprise Question, were selected.
Measurements, Results:
In period one, 59 patients completed the Utrecht Symptom Diary (USD) at day one of admission and after 7 days. In period 2 (n = 60), the same procedure was followed; additionally, the palliative care team was consulted for patients with high USD-scores. Significant improvement on the USD Total Distress Score (TSDS) was observed in both groups without a difference between the 2 periods. This study showed an association between consultation of the palliative care team and improvement on USD TSDS (adjusted odds ratio: 4.9; 95% confidence interval: 1.816-13.198), despite low follow-up rate of advices (approximately 50%).
Conclusions:
This study emphasizes the importance of creating awareness for consulting the palliative care team. Further research should focus on assessing the reason behind the low follow-up rate of the advice given and understanding the specific advices contributing to symptom improvement.
Introduction
In 2050, it is estimated that one quarter of the population in Europe will be aged 65 years and older, due to the aging population and increasing life expectancy. 1 Subsequently, more health-related issues will become prominent in people, especially, in the last years of life. In this phase, patients could benefit from palliative care. 2,3 The World Health Organization (WHO) defines palliative care as the prevention and relief of suffering of adult and pediatric patients and their families facing the problems associated with life-threatening illnesses. These problems include physical, psychological, social, and spiritual suffering of patients and psychological, social, and spiritual suffering of family members. In the past, palliative care was often restricted to terminal (cancer) patients. 4 Renewed insights show that palliative care can be provided, when appropriate, at any point in the trajectory of a life-limiting illness as it could be beneficial alongside disease-oriented therapies. 5 Palliative care should also be integrated into management of chronic diseases. 6 The growing needs of the elderly impose the need for adequate policies for the elderly and adequate involvement of palliative care (services), which could improve their quality of life. 5 Early referral to a palliative care team is associated with better long-term outcomes including preservation of (instrumental) activities of daily living independency. 7 It is also believed to be economically beneficial for the patient, as it would shorten the length of hospital stay. 7 Despite these advantages, only 14% of the people who could benefit from palliative care receive the appropriate palliative care worldwide. 8 Although the added value of a palliative care team was emphasized in the literature, the impact of the palliative care team on the total symptom burden in non-cancer patients is not yet well established. 9 -11
Early identification of patients who might benefit from palliative care is a challenge. 12,13 The surprise question (SQ), “Would it surprise you if this patient died within the next 12 months?”, is a simple, feasible and currently one of the most used screening tools to identify the start of the palliative phase in the Netherlands. 14 However, a negative answer to the SQ does not necessarily indicate a need for palliative care. 15,16 When a negative answer to the SQ has been given, the symptom burden should be assessed. To assess the symptom burden in the palliative care setting, different instruments have been developed, including the Utrecht Symptom Diary (USD), which is the edited Dutch version of the Edmonton Symptom Assessment Scale. 17 The outcome of the USD can be used to trigger clinicians to take action, including referral to a palliative care team. 17 In the Netherlands, palliative care is considered to be a basic skill and every doctor and nurse should be able to deliver basic palliative care to patients in need. Specialized palliative care teams are available for consultation 24/7 in every setting. However, most hospital teams have an advisory role only and are led by specialized nurses.
Patients who could benefit from palliative care are not structurally identified In Dutch hospitals. Subsequently, screening tools, including the USD are infrequently used. 18,19 Lack of structural symptom assessment can result in an underestimation of the actual symptom burden.
Thus, the aims of this study are the following: To investigate whether consultation of the palliative care team in response to a high symptom burden results in more symptom reduction in identified palliative care patients compared to standard care. To investigate whether consultation of the palliative care team is associated with an improvement of the symptom burden.
Methods
Design, Setting and Participants
This prospective comparative study, concerning 2 periods of 3 months each, took place from October 2018 to March 2019 at the Maastricht University Medical Centre. Individuals over 60 years were identified as patients who could benefit from palliative care (SQ). They were admitted to the departments of internal medicine and were included if they understood the Dutch language and provided informed consent. Patients were excluded if they suffered from a delirium (delirium observation scale > 3), if their life expectancy was < 1 week, or when the palliative care team was already involved with the patient’s wellbeing. Patients with cognitive impairment were not excluded when the attending physician estimated that they were competent to fill out the USD.
Ethical Considerations
The study was conducted in accordance with principles of the Declaration of Helsinki and was approved by the local Medical Ethics Committee of Maastricht (METC 2018-0844). Informed consent was obtained before the commencement of the study.
Instruments
The SQ, to mark the palliative phase, has moderate predictive values (sensitivity of 67.0%, specificity of 80.2%, positive predictive value of 37.1% and a negative predictive value of 93.1% for death at 6 to 18 months). 10 In this study, the SQ was asked to both the physician and the unit nurse. Patients were identified when at least one answer to the SQ was negative.
The USD (Online Appendix I), 20 the Dutch version of the Edmonton Symptom Assessment Scale, is a validated standardized self-report tool, which assesses 13 prevalent symptoms on a numeric eleven-point rating scale. 17 The total symptom distress score (TSDS) is the sum score of the 13 individual items resulting in a score between 0 and 130 points. A significant improvement was suggested to be 6 points on the TSDS, an extrapolated value of the 5 points used in the study of Follwell. 21
Procedure and Data Collection
The study procedure is depicted in Figure 1. For 6 months, hospital admissions were monitored by one researcher every working day and the SQ was asked to the unit nurses and physicians by 2 researchers. Medical data obtained were reason of admission, comorbidities, use of analgesics/opioids and amount of hospital stays in the past year. During the first 3 months (P1), eligible participants were asked to complete the USD within the first 3 days after admission (T0). The researcher filled in the USD when patients were unable to write. The researcher documented high individual USD-scores, defined as scores >4, in the electronic patient file. Seven days after inclusion (T1), patients filled out the USD again or answered the questions by phone. During the next 3 months (P2), the same procedure was followed, and, the palliative care team was consulted in patients with high symptom burden. High symptom burden was defined as one item of the USD exceeded 4 points or, in case the symptom “tiredness” was involved, 2 symptoms exceeded 4, because tiredness is a very common symptom which is hypothesized not to be a valid discriminating factor. The cut-off value was chosen based on recent literature. 22
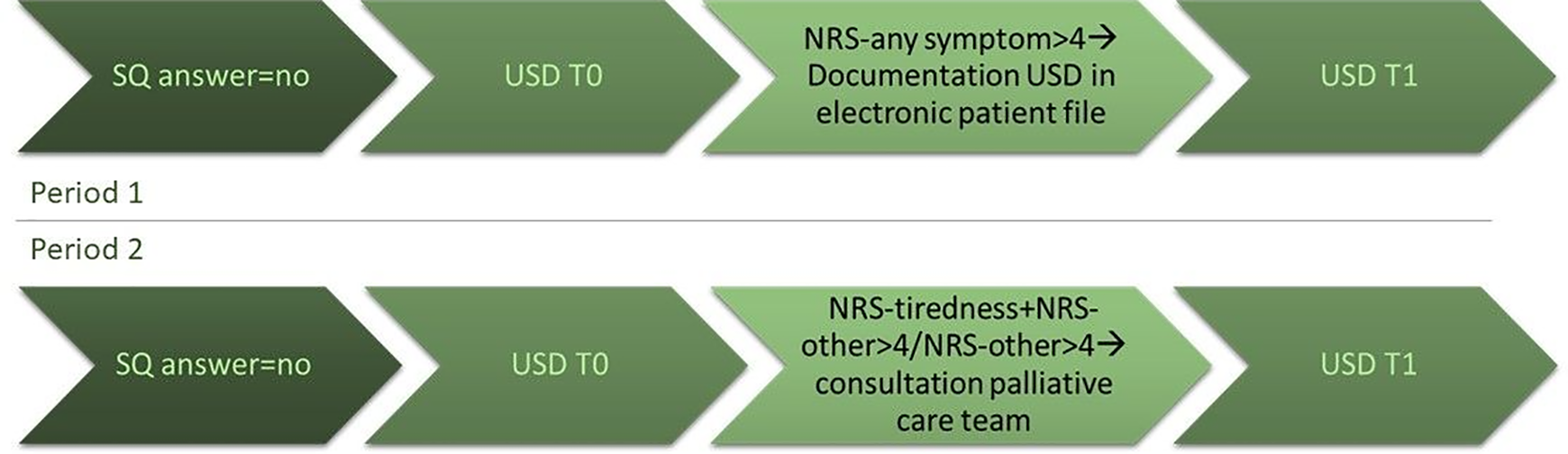
Procedure prospective comparative study. NRS: numeric rating scale; SQ, surprise question; T0, day 1-3 after admission; T1, day 7 after T0; USD: Utrecht symptom dairy.
The consultation of the palliative care team consisted of a bedside consultation of a nurse who was part of the palliative care team. Three palliative care nurses were involved in this study. In general, the palliative care team performed one bedside consultation, except when the attending physician asked for more visits. The palliative care team documented their advices in the electronic patient file using a predefined format (Online Appendix II). They did not communicate their advices to the attending physicians.
Statistical Analysis
The statistical analysis was carried out with SPSS (version 25.0). Descriptive statistics were used to show the characteristics of the study populations. Baseline patient characteristics of both study arms were compared using Chi-square tests, student’s t-tests, or Mann-Whitney U tests, as appropriate.
With 66 patients in each group, it was estimated that the study had a power of 80% to detect a 20% difference in proportion of patients who significantly improved on the USD TSDS, with a minimal clinically important difference of 6, comparing the 2 study groups, given the conservative estimate of the loss-to-follow-up of 10%. 23,24 The primary analysis was performed using a Chi-square goodness-of-fit test.
The participants of the 2 periods were combined to detect whether consultation of the palliative care team is associated with a significant improvement on the TSDS in the total study population. Furthermore, logistic regression was performed in which they was adjusted for variables that were significantly different between the 2 study arms at baseline.
Results
A total of 308 patients, aged over 60 and admitted to a department of internal medicine, were screened for eligibility (Figure 2). A total of 181 patients were considered to be eligible, of which 36 patients were not willing to participate. Main reasons for exclusion were positive answers to the SQ from the physician and nurse, delirium, and difficulties in understanding. We enrolled 145 patients of which 6 were discharged from the department before the USD was handed. In P1, 67 patients completed the USD at T0 of which 8 were lost to follow-up. In P2, 12 patients were lost to follow-up of the 72 patients who completed the USD at T0. The analyses were performed with the patients who completed USD at T0 and T1. So, 59 patients in P1 and 60 patients in P2 completed the study.
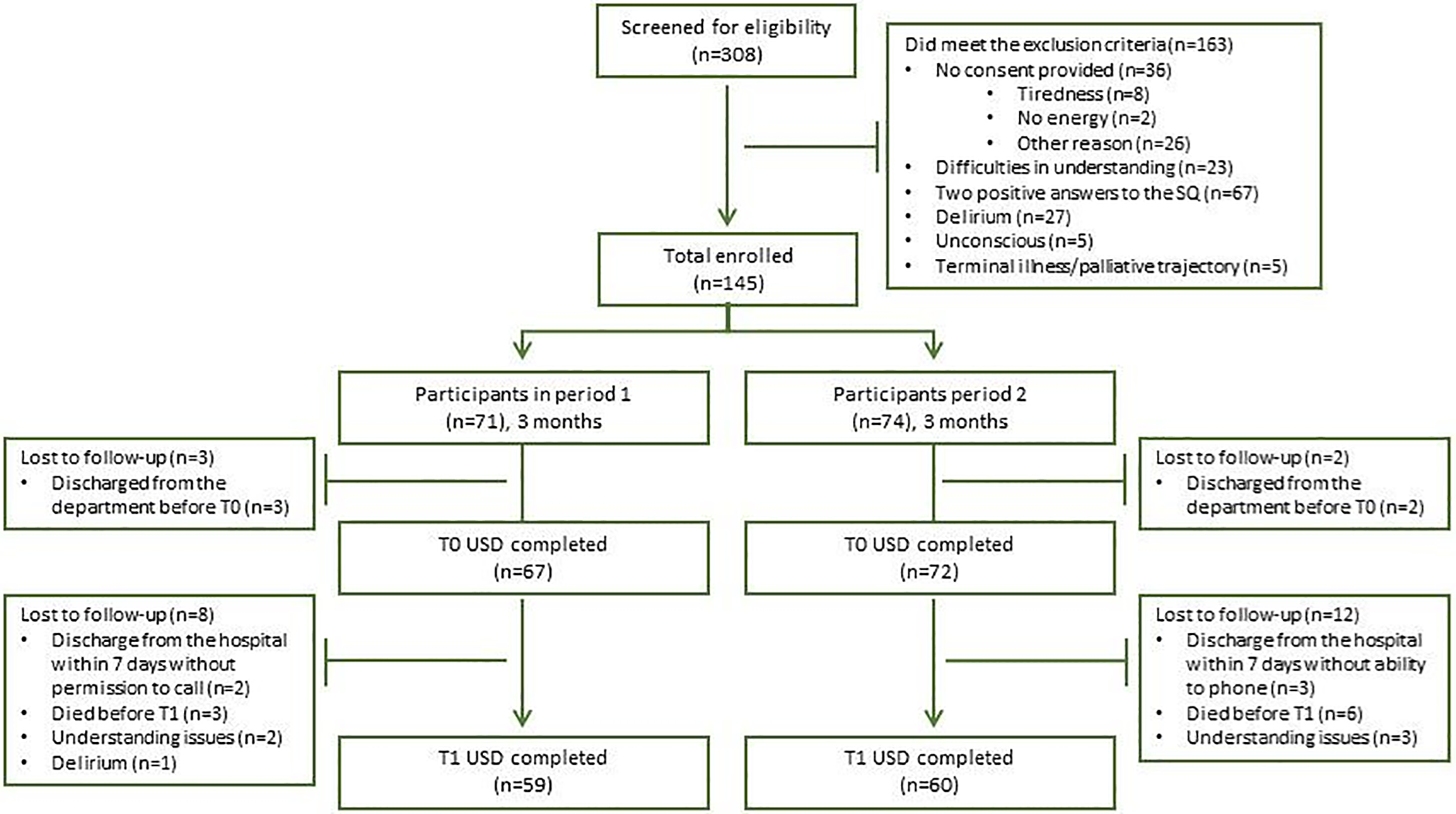
Flowchart patient enrolment process. T0: day 1-3 after admission; T1, day 7 after T0; USD, Utrecht symptom dairy.
Patient Characteristics
In this study, most patients were male (56.7% in P1, 58.3% in P2), who were admitted because of an infectious disease (55.2% in P1, 63.9% in P2), had 2 or more comorbidities (64.2% in P1, 63.9% in P2), used no analgesics at baseline (62.7% in P1, 66.7% in P2), and lived at home without partner (46.3% in P1, 41.7% in P2).
Patients in the 2 study arms differed significantly from each other in terms of a high symptom burden (95.5% in P1 vs 79.2% in P2; p: 0.004). Moreover, patients in P2 had significantly longer hospital stays compared to patients in P1 (P1: median 9 days vs P2: 13 days; p < 0.0001). A significant difference was seen in patients who had no comorbidities between the 2 periods (0% in P1 vs 6.9% in P2; p < 0.05). None of the other comorbidities differed at baseline (Online Appendix II).
USD Total Symptom Distress Score (TSDS)
The mean USD TSDS of patients in P1 did significantly decrease from baseline (T0) to follow-up (T1) (50.5 vs 42.8 points; p: 0.006). Additionally, a significant improvement was found (35.1 vs 24.0; p < 0.0001) in P2. The proportion of patients who significantly improved on the USD TSDS, did not significantly differ between the 2 periods (45.8% in P1 vs 56.7% in P2; p: 0.234).
Additionally, it was observed that in P2, significantly less patients deteriorated on the USD TSDS compared to P1 (32.2% in P1 vs 17.7% in P2; p:0.04).
Logistic regression in the total study population showed that patients with high symptom scores and proactive consultation of the palliative care team had 5 times higher chance to improve significantly on the TSDS as compared to patients who did not receive proactive consultation (adjusted odds ratio: 4.895 (95% confidence interval: 1.816-13.198; p: 0.002)), after adjustment for comorbidity, high symptom burden at T0, and T1 via telephone.
Advices of the Palliative Care Team
In P1, for one patient, the palliative care team was consulted. However, in P2 consultation of the palliative care team was conducted in 79.2% (n = 57) of the patients. Of all patients in P2, 66.7% received extra advices of the palliative care team. In over 80% of the consultations, advices for physical symptoms were given, of which 27.3% were followed. Of the total advices, 50.0%, 53.8% and 44.4% were followed for psychological, social, and spiritual advices, respectively (Figure 3).
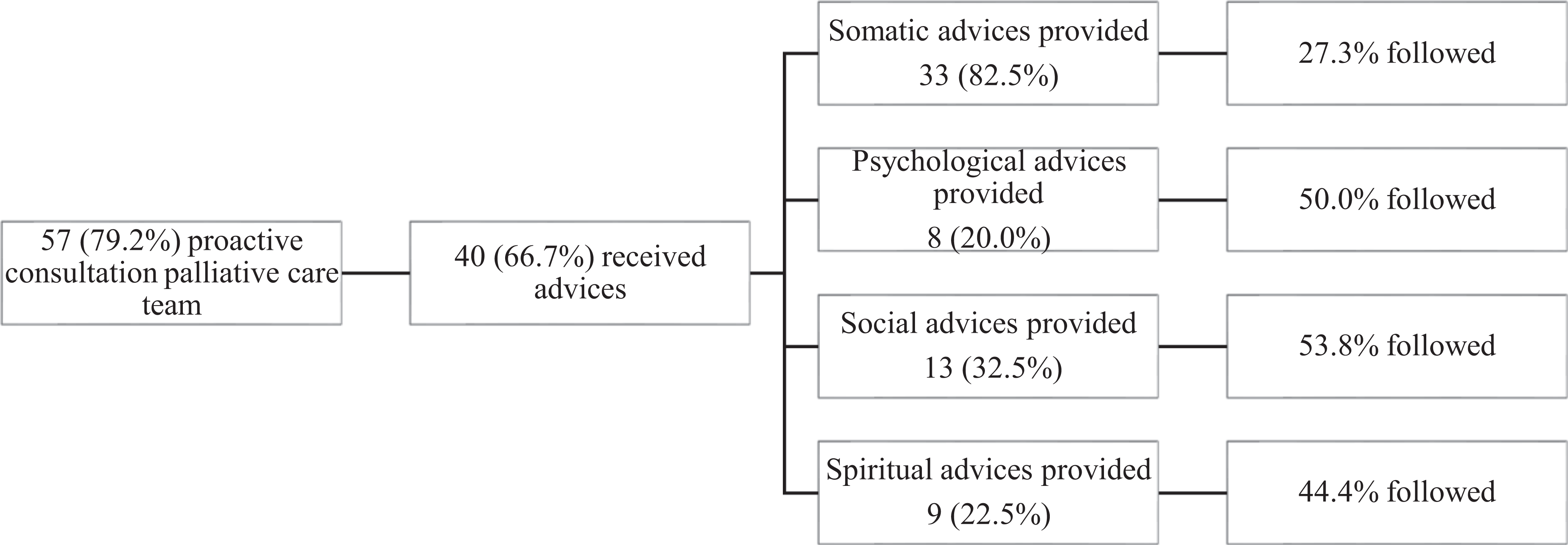
Advices palliative care team in period 2. Data is presented as number (percentage). Percentages do not add up, because one patient could receive advices on different domains.
Discussion
As measured with the USD, symptom scores improved from T0 to T1 in P1 and P2. However, no difference between P1 and P2 was found with respect to the proportion of patients who significantly improved on the USD TSDS. Interestingly, logistic regression revealed that patients with high symptom scores receiving consultation of the palliative care team had a chance 5 times higher to improve significantly on the TSDS as compared to patients who did not receive consultation. This finding implicates that early involvement of an inpatient palliative care team for patients with a high symptom burden has added value.
During the first week after admission, approximately 50% of patients showed a significant improvement of their symptom burden, irrespective of the intensity of involvement with the palliative care team. This finding resonates with the study of Hanks et al. 25 which showed that hospitals provide a high level of care for palliative patients. Over the last decades, palliative care, in especially cancer patients, has evolved. However, identification of palliative care needs is not routinely implemented in current treatment of elderly patients. The first step, identification of the palliative phase is, mostly by a negative answer to the surprise question, is widely described for patients with cancer, COPD, chronic heart and kidney failure but rarely in the elderly. 15 Several instruments have been described for the identification of palliative care needs such as SPICT, NECPAL, RADPAC, PALLI, eFI, and i-Harp, all mainly used in the research setting. 26,27 This pilot study suggests that, in this tertiary hospital, palliative care is embedded in standard care regarding older patients admitted to a department of internal medicine. However, a firm statement cannot be made as no control group was part of the study design. It would be helpful to assess the usefulness and applicability of the USD in qualitative research. Health care professionals could be asked whether the SQ and the USD could be implemented in clinical practice.
This study showed no significant difference between the periods with respect to the proportion of patients who significantly improved on the USD TSDS. Patients in P2 had a lower symptom burden at baseline than in P1, which will be further elaborated upon in the limitations section. As a result, only 66.7% of the patients in P2 needed advice of the palliative care team. It is proposed that the added value of the palliative care team would be more pronounced when in P2 more patients suffered from a high symptom burden. Many studies comparing standard care with additional consultations 28 -33 showed that involvement of the palliative care team was often not better in reducing the severity of individual symptoms. 33,34 However, it is difficult to draw firm conclusions because of heterogeneity of the studies, methodological challenges, and different interventions and outcomes. 28 Studies concluded that the added value of a palliative care team was mainly based on improvement of patient and caregiver satisfaction, costs, and quality of life. 28,29 This study added that with consultation, patients seem to have a 5 times higher chance to improve on the TSDS.
To our surprise, only up to 50% of the advices from the palliative care team were followed. To the best of our knowledge, this is the first study describing the poor follow-up rate of the advices of the palliative care team. It is hypothesized that this could be partly attributed to the fact that the advices of the palliative care team were only mentioned in the electronic patient file, but not orally discussed with the attending physicians. In line with this hypothesis, a deliberately asked consultation of the palliative care team might have more impact compared to consultation based on high USD-scores. Especially because our definition of high symptom burden is chosen with a relatively low threshold. However, as the palliative care team was consulted only in one case in P1, it is not possible to compare the asked advices with the unasked advices. This phenomenon also illustrates the importance of creating awareness concerning the possibility to consult the palliative care team. As Friedrichsen et al. 34 emphasized in their research, investigating the effect of palliative care consultation teams on acute wards, and collaboration between the health care teams is of pivotal importance and can be improved when each team recognizes and supports each other’s expertise. For future studies it would be interesting to explore the reason behind the poor follow-up rate with qualitative research and to find out which advices of a palliative care team contribute to improvement of the symptom burden.
Strengths and Limitations
A strength of this study is the prospective comparative study design with a moderate sample size. Research in the field of early integrative palliative care is mainly focused on patients with cancer or those with chronic diseases. 28 This study has a unique character as it focuses on the elderly, admitted to a department of internal medicine.
This study, however, has several limitations. First, at baseline, patients in P2 had a lower symptom burden than in P1. Randomization could have prevented this issue, but contamination could have occurred when randomization was applied. The reason behind the difference could not be traced back. The possibility exists that more patients suffered from a viral infection in P2, as it took place during the flu season. It is hypothesized that patients with a viral infection have less symptoms compared to patients with another reason of admission.
Second, this study was performed in a single-center tertiary hospital in which the SQ was used to identify patients. Those factors contribute to diminished generalizability. As mentioned before, the SQ has moderate predictive values. The discriminative factor of the SQ is even worse in patients with chronic diseases compared to patients with cancer. 15 However, to date, the SQ is the best available tool 15 to identify patients. Weijers et al. 33 showed that adding a second surprise question, “Would I be surprised if this patient is still alive after 12 months,” might improve the specificity, and suggested that this would be a helpful tool to initiate advance care planning. It could be argued whether prognostication is of great significance as identified patients are likely to benefit from a palliative approach, irrespective whether they survive the following year.
Third, it can be discussed whether 6-points improvement on the USD TSDS, is a clinically relevant outcome measure to evaluate the effectiveness of a palliative care team as our population deviates from the population in the study of Follwell. 21 Follwell et al. 21 focused on the effectiveness of outpatient palliative care in patients with metastatic cancer, and it is a matter of debate whether the cut-off value of our study is properly chosen. Moreover, the literature emphasizes that the ESAS is appropriate for routine symptom assessment, but adequate cut-off points have been proven difficult to obtain. 17 No other study investigated cut-off values of USD TSDS in elderly. Moreover, Hui and Bruera 17 explained that a meaningful difference could be different for different patients as some patients might consider 6/10 points to be agonizing whereas others do not. Personalized symptom goals might be more adequate. Thus, the study did not fully reach the inclusion as deemed necessary in the power analysis.
Conclusions
This study showed that patients with a high symptom burden and palliative care consultation were 5 times more likely to improve on the TSDS compared to patients who did not receive consultation, despite the low follow-up rate of the advices. Therefore, physicians should not deviate from consulting a palliative care team. It would be interesting to assess the reason behind the low follow-up rate of advices of the palliative care team and subsequently develop tactics to improve this phenomenon. Furthermore, this study emphasizes the need for research focused on understanding the advices of the palliative care team that attribute to improvement of the symptom burden. Following this, adequate referring criteria should be identified, and implementation strategies could be further explored.
Supplemental Material
Supplemental Material, sj-pdf-1-ajh-10.1177_1049909120982606 - Added Value of Early Consultation of an Inpatient Palliative Care Team in Hospitalized Older Patients With High Symptom Burden: A Prospective Comparative Study
Supplemental Material, sj-pdf-1-ajh-10.1177_1049909120982606 for Added Value of Early Consultation of an Inpatient Palliative Care Team in Hospitalized Older Patients With High Symptom Burden: A Prospective Comparative Study by Myrthe W. Naaktgeboren, Fabienne J. H. Magdelijns, Daisy J. A. Janssen and Marieke H. J. van den Beuken-van Everdingen in American Journal of Hospice and Palliative Medicine®
Footnotes
Authors’ Note
All authors fulfill the authorship requirements as defined by International Committee of Medical Journal Editors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.