
Abstract
Older persons with serious illnesses living in rural communities are an underserved population. They often live with heavy symptom burden and poor quality of life with limited access to resources. Nav-CARE (Navigation: Connecting Accessing Resourcing and Engaging) was developed to specially train and mentor volunteer navigators who help connect older persons with serious illness to the resources and information they need.
Aims:
This mixed methods longitudinal study evaluated Nav-CARE for feasibility, acceptability, ease of use, and satisfaction by older persons and volunteers.
Methods:
Nine volunteer navigators visited 23 older persons with serious illness every 3 to 4 weeks for 1 year. Data were collected from volunteer navigators, and older person participants at baseline, during the year- long implementation and post implementation.
Results:
Volunteer navigators and older persons reported Nav-CARE was easy to use, feasible and acceptable. The majority of older persons agreed or strongly agreed that they were satisfied with the navigation services (100%; 8/8), that navigation services were important to them (87%; 7/8), that they would recommend the program to someone else (87%; 7/8), and would participate in the program again (75%; 6/8). Similarly, volunteer navigators reported 100% (9/9) satisfaction with the program, 100% (9/9) would recommend it to others, and 67% (6/8) would participate again.
Conclusions:
Nav-CARE appears to be a feasible, acceptable, and satisfactory program for older persons with serious illness and volunteer navigators.
Background
In North America, many older persons live in rural communities and experience poor health 1 with little support when transitioning from chronic illness management to palliative care. 2,3 These older persons often live with heavy symptom burden 4,5 and are at risk for social isolation. They have critical needs for support, navigation, advocacy, and assistance with decision-making. 4 As well, they may not know of the health or social services available in their community. 6 As such there is a critical need for navigators in rural areas. 7
Although several models of navigation exist in the literature, 8 -10 they do not appear to reflect the unique issues of rural communities and of older persons with chronic illness. 7 However, volunteers can help overcome challenges faced by older persons with chronic illness in accessing resources. 11 -13 Volunteers have long been an integral part of the interdisciplinary team in rural communities, however, their focus is often with end of life care, not early palliative care and usually lack the necessary training to be in an advocacy role required for successful navigation. 14,15 In a systematic review of community health navigator interventions, the authors concluded that training of navigators was key to the success of these interventions. 16 As such, a program with specially trained volunteer navigators may address the gap of access to resources and services needed for rural older persons with serious illnesses before they transition to end of life
A program of specially trained volunteer navigators entitled Nav-CARE (Navigation: Connecting, Accessing, Resourcing and Engaging) was conceptualized in 2016 in Western Canada 10 with the goal improving the quality of life of older persons with serious illness living in rural communities. It was further developed and successfully pilot tested in three rural Canadian communities located in a coastal/mountain geographic region. 11
The aim of the current study is to determine if Nav-CARE is feasible and acceptable in two rural prairie communities. In implementing community programs assessing feasibility is an important step to illustrate the program can be delivered as intended. 17 Acceptability, often included in definitions of feasibility, is the extent to which those delivering and receiving the intervention find it appropriate and satisfying. 18 Feasibility and acceptability of Nav-CARE is important for the sustainability of this program.
Methods
Study Design
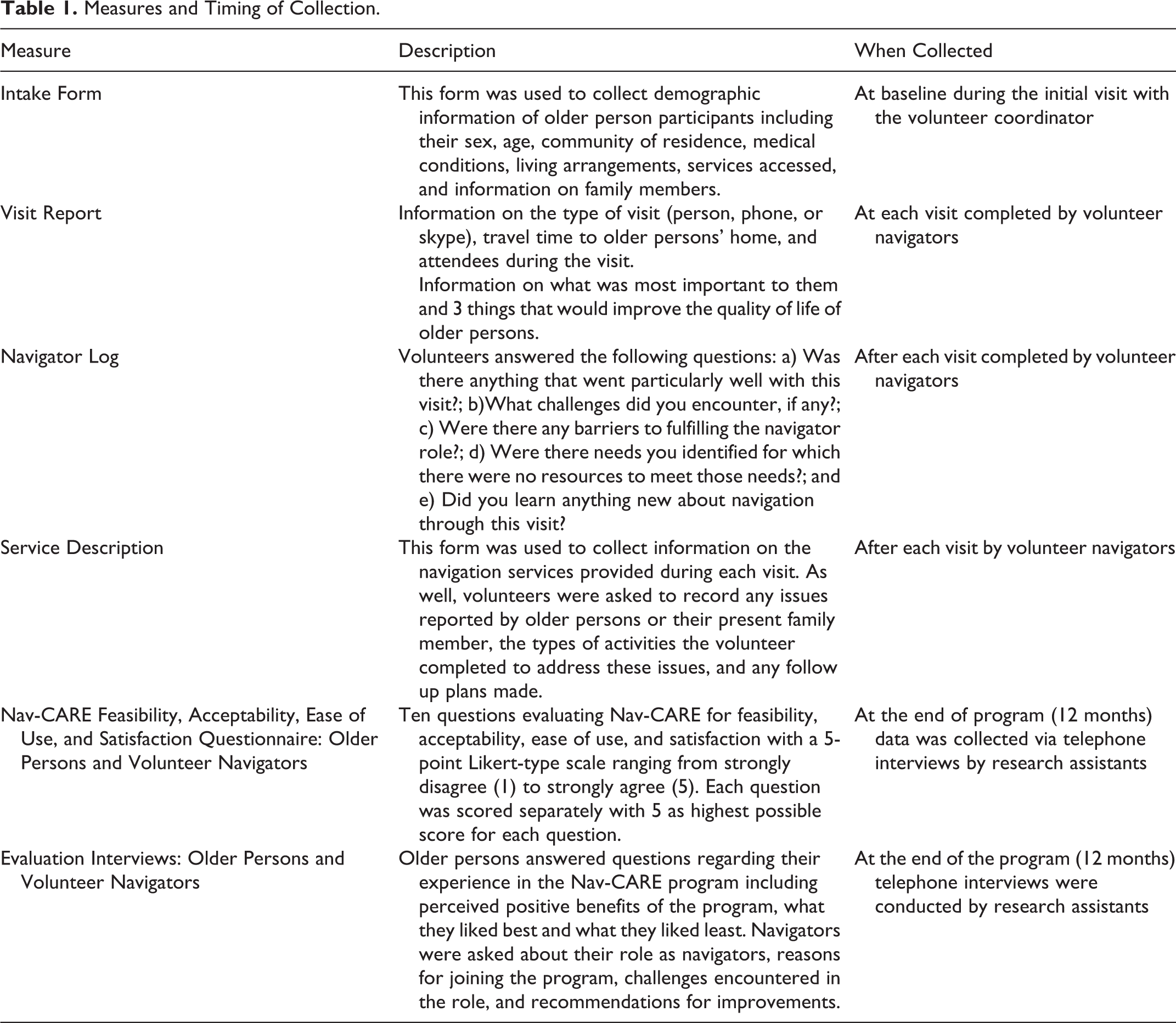
Using a mixed methods longitudinal feasibility study design, Nav-CARE was implemented and evaluated in two rural communities for one year. Qualitative and quantitative data were collected from volunteer navigators, and older persons (see Table 1 for data collection timeline and measures). All data were integrated in the results section for a more comprehensive evaluation and understanding of the impact of Nav-CARE.
Measures and Timing of Collection.
Setting
Two rural western Canadian communities (rural was defined as populations less than 10,000) 19 that were 70 kilometers away from each other participated in this study. Because of their proximity multiple organizations served both communities. Community Advisory Boards for the hospital in the larger community and the health center in the smaller community agreed to support the implementation of Nav-CARE in their communities.
Participants
Volunteer navigators
Volunteer navigators needed a minimum of one-year experience as a volunteer visiting older persons in the home and be willing to commit two to four hours per week of volunteering for one year. The time commitment includes visits, as well as meetings with the volunteer coordinator, debriefing sessions, documentation and searching for resources. Volunteers were recruited by the volunteer coordinator through community organizations where they volunteered.
Older persons
Inclusion criteria for older persons were: a) age 55 years and older, b) living in one of two rural communities, and c) living with a serious illness. Recruitment was ongoing throughout the course of the study when attrition occurred. Participants could self-refer or be referred by a healthcare provider. In addition, the volunteer coordinator provided information about Nav-CARE through in-person presentations to the community and healthcare organizations. Posters and brochures provided information on the Nav-CARE program and encouraged older persons to contact a toll-free number if they were interested in participating.
Procedure
Nav-CARE consists of three main components: a) training of a volunteer coordinator and volunteers, b) ongoing support for volunteer navigators by the volunteer coordinator, and c) ongoing visits to older persons by volunteer navigators. Figure 1 outlines the specific procedures for the study. All measures were developed and pilot tested in a previous Nav-CARE study. 11
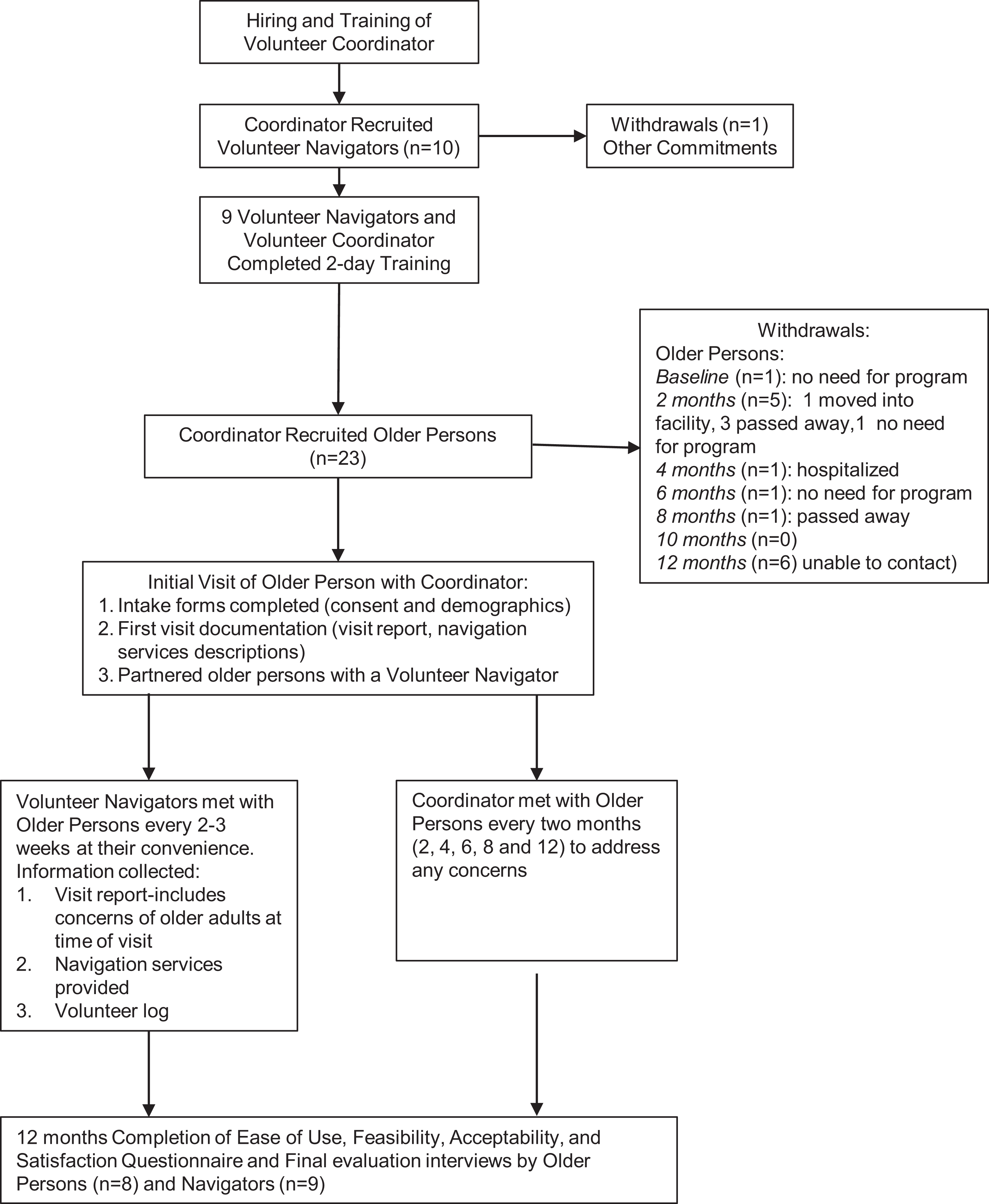
Study Procedures.
The volunteer coordinator was hired through recommendations of the community advisory board and once the program commenced, this coordinator provided ongoing support to volunteers. The 9 volunteer navigators completed a 2-day training in September 2016 which focused on understanding the navigator role, screening for quality of life concerns, advocating for clients, facilitating community connections, coordinating access to services and resources and promoting active engagement. Specific details of the training and its evaluation has been reported elsewhere. 20 At the beginning of the workshop written informed consent was obtained by the Principle Investigator.
After obtaining written informed consent the volunteer coordinator obtained older person participants’ demographic information using an intake form. Following the initial visit, the coordinator assigned a volunteer navigator to visit the older person. Nav-CARE volunteers completed visits with older persons every three to four weeks over the course of a year. Every six weeks the volunteers met with the volunteer coordinator and research coordinator in a de-briefing session designed to support the work of the volunteer navigators.
Data Analysis
All quantitative data from the Nav-CARE Feasibility, Acceptability, Ease of Use, and Satisfaction Questionnaire were statistical analyzed using SPSS version 24 software. 21 Descriptive statistics were used to calculate frequencies and proportions for categorical variables. Means, and standard deviations were reported for continuous variables.
Qualitative data from the visit reports, navigation logs, service description form and evaluation interviews were transcribed verbatim by an experienced transcriptionist and analyzed using content analysis 22 to identify common themes. Trustworthiness of the data was maintained by using participants own words and keeping an audit trail of analytic decisions. Qualitative and quantitative data were integrated in the results section.
Ethics Approval
This project received Ethical approval from the University of Alberta Health Research Ethics Board (Pro00059300). In addition, it received Operational/Administrative Approval for the St. Mary’s Hospital in Camrose and Killam Health Center from the Covenant Health Research Center (CHRC).
Results
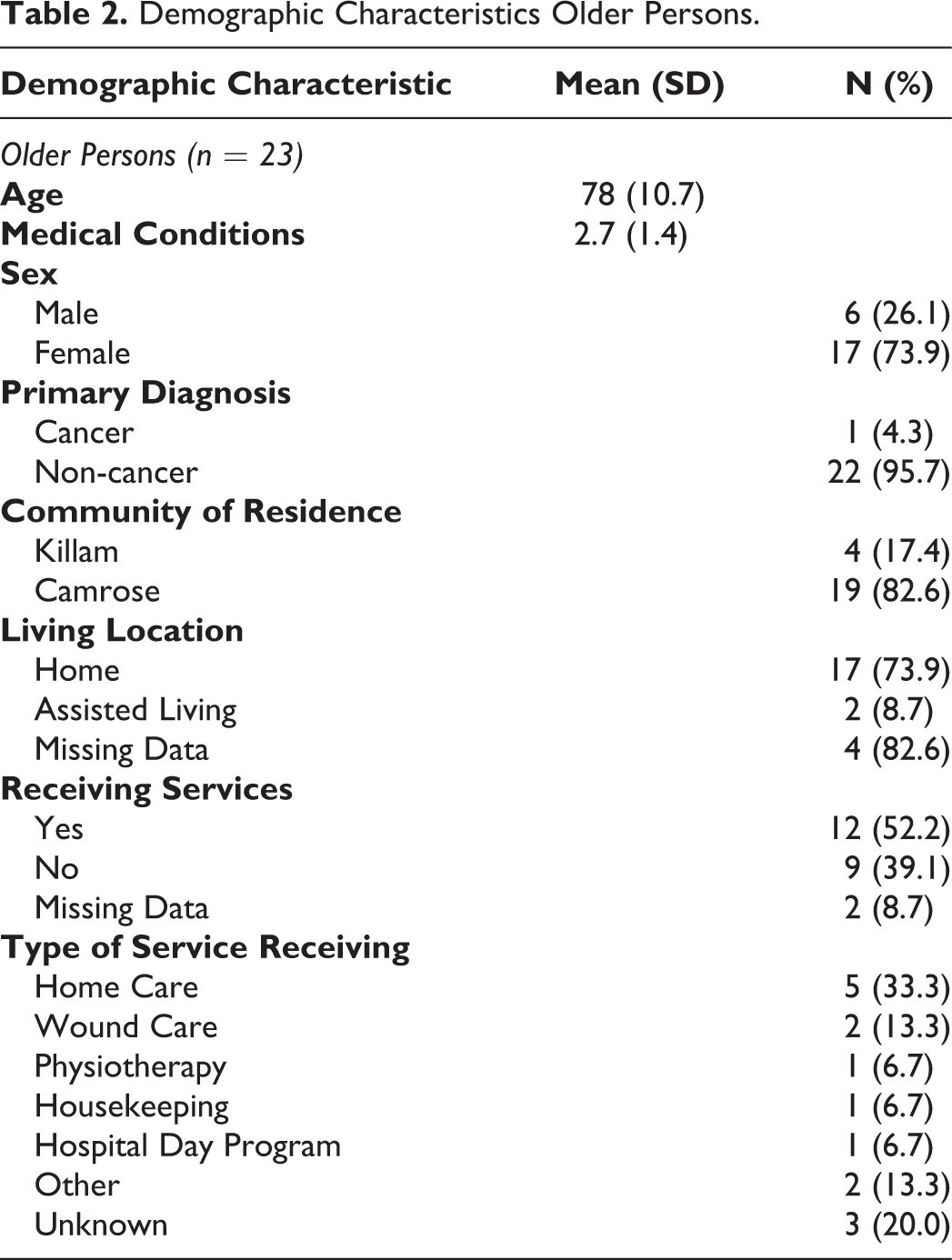
With only two volunteers and three older person participants in the smaller community the data were combined with the larger community and reported together. Volunteer navigators had a mean age of 60.7 years (38-79), and on average 2 years of experience volunteering and working with older persons. Demographic characteristics for older persons are described in Table 2. Twenty-three older persons participated in the implementation phase of the Nav-CARE program from October 2016 to October 2017. They were on average 78.0 (SD = 10.7) years of age; most were female (74%; 17/23), lived alone (57%; 13/23) and were receiving services (such as home care) (52%; 12/23). The majority (22/23) of older person participants had a non-cancer diagnosis and on average had 2.7 medical conditions (SD = 1.4). Fifteen withdrew during implementation of Nav-CARE for a variety of reasons (Figure 1). In the 15 that withdrew three withdrew as they felt they no longer needed the program. Their perception of no longer needing the program included an improvement in their health, subsequently being connected to the resources needed and 1 older person was reconnected by the volunteer navigator to their family. Four died during the study timeline, 1 was hospitalized and 1 was admitted to a long-term care facility. Six did not participate in the final evaluation interviews as the RA’s were unable to contact them. Unfortunately, as they were not contacted their reasons for withdrawal were not captured.
Demographic Characteristics Older Persons.
Visits
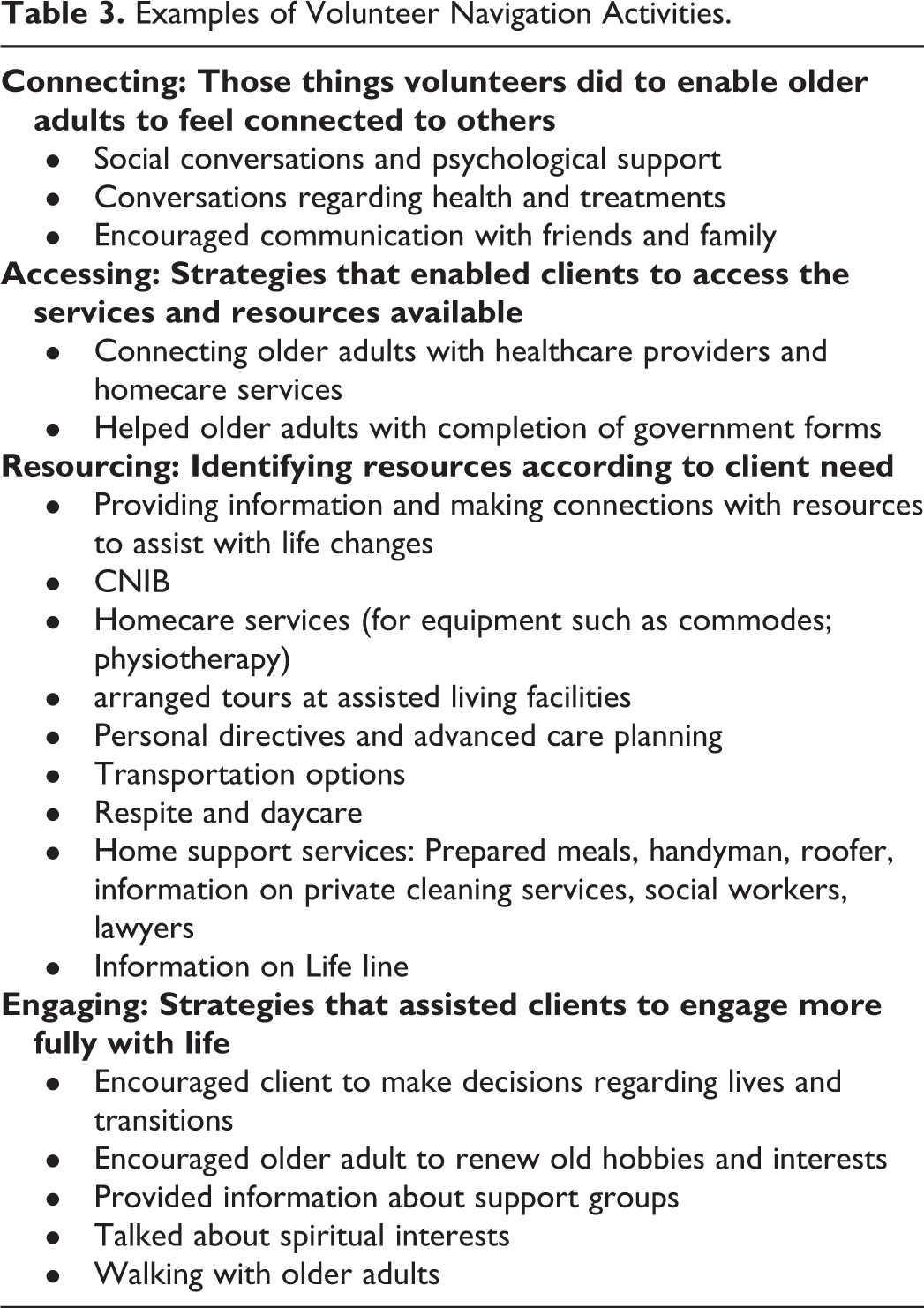
Volunteers completed 220 visits with older persons over one year. One volunteer was assigned initially to visit two older persons. Table 3 provides examples of the volunteer navigator activities during the visits. The visits ranged from 5 to 210 minutes with an average of 28.6 minutes per visit (SD = 17.9). The majority of the visits were scheduled [87.7% (193/220)] and 17.3% (38/220) were unscheduled. Most visits occurred at home [79.5% (167/220)]. When visits were not in the home they were in the hospital [1.8% (4/220)], residential facilities [8.1% (18/220)] or other locations such as cafes [13.6% (30/220)]. The majority were in person [87.7% (193/220)] and the rest by phone [10.9% (24/220)] (missing data from 3 visits).
Examples of Volunteer Navigation Activities.
Feasibility, Acceptability, Ease of Use, and Satisfaction With Nav-CARE
Volunteer navigators
Table 4 presents the data from the feasibility, acceptability, ease of use and satisfaction questionnaire. Volunteer navigators reported Nav-CARE to be easy to use (questions 1 and 2). One-hundred percent of volunteer navigators (9/9) agreed or strongly agreed that they were able to perform their navigation services without difficulties, and 78% (7/9) agreed or strongly agreed that they were sure about what they were expected to do in their role as navigators.
Ease of Use, Feasibility, Acceptability Volunteer Navigators.
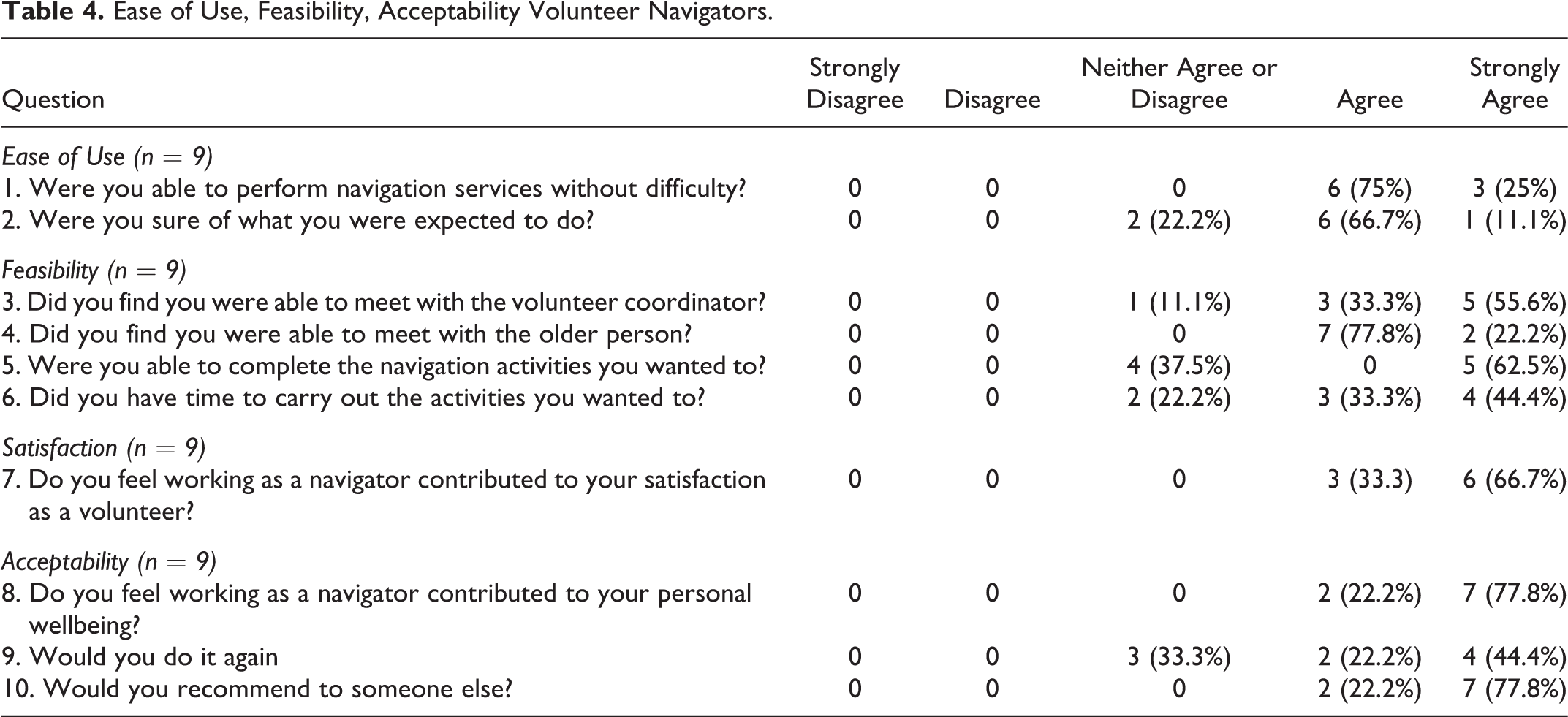
Nav-CARE was reported by the volunteer navigators to be feasible (questions 3-6). The majority (88%; 8/9) reported being able to meet with the volunteer coordinator for support. They also reported being able to meet with the older person (100%; 9/9). The majority (62.5%; 5/9) strongly agreed that they were able to complete the navigation activities they wanted to and had the time to carry out these activities (7/9; 77.7%).
The volunteer navigators also reported being satisfied with their role as navigators (question 7). One hundred percent (9/9) of the volunteers agreed or strongly agreed that working as a volunteer navigator had contributed to their satisfaction as a volunteer.
Nav-CARE was acceptable to the volunteer navigators (questions 8-10) as 100% (9/9) agreed or strongly agreed that working as a navigator contributed to their well-being. As well, 67% (6/9) of volunteers agreed or strongly agreed that they would do the role again with 100% (9/9) agreeing or strongly agreeing that they would recommend the role to someone else. This finding was supported in the qualitative evaluation interviews where volunteers felt that being in the volunteer navigator role was not only beneficial for the older persons, but for the volunteer as well. For example one participant said that they learned a lot themselves; “Yes, definitely. It certainly—it’s like a self-education as well when you’re finding out this information. I’m certainly a senior myself, and so it has helped me.” (P02)
The positive experience of being a volunteer navigator was also described by volunteers during the evaluation interviews. For example one participant said: “It’s a wonderful role, very rewarding, not monetary-wise, but rewarding in the terms of there’s a sense of satisfaction to know that you have assisted in even if it’s in a small little way by just listening to someone. It means a whole lot” (P06).
When asked what they enjoyed most about being a Nav-CARE volunteer, volunteers said that they enjoyed visiting with the older persons: as one participant said: “I guess what I liked most was being able to get out there and help the people any way I could. It was just enjoyable to be visiting with them. Even when they didn’t need that much, it seemed like just being there and talking to them made them feel better” (P10).Some volunteers described being able to connect their older person with resources was what they enjoyed most. For example, one participant said: “So that’s what I was really pleased about being a part of and being maybe able to offer them some resources that are out there” (P04).
The volunteer navigators also described what they liked least. Volunteers felt that their role was to provide older persons with resources in the community. Volunteers would help older persons identify their quality of life concerns and attempt to connect the older persons with resources, however sometimes this didn’t happen. For example, one participant said:
When I’d get all this information and they wouldn’t follow through on it: the next time I’d go, they’d say, “Oh, I totally forgot about that.” So you learn to step back and say, “I did what I could, and it’s up to them to follow through.” So that’s probably—it’s not maybe least liked, but probably the most frustrating of what it was. There was very little about it that I least liked about doing this (P07).
Two volunteer participants described feeling guilty at times was the thing they liked the least. As one participant suggested: “Probably, and this is, like I say, it’s self-imposed, but the self-imposed guilt I felt about maybe not being able to connect with my people maybe perhaps when they needed it, or maybe my availability didn’t work for them. So just that little bit gnawing sense of “Am I doing enough?” (P01).
Older Persons
At the end of the program, eight older persons completed the feasibility, acceptability, ease of use, and satisfaction questionnaire (see Table 5). Older persons reported that Nav- CARE was easy to use (questions 1 and 2), as 100% (8/8) agreed to strongly agreed that they were able to access the navigator without difficulty. The majority of participants (75%; 6/8) were sure of what they were expected to do; 2/9 (25%) were not sure of what they were expected to do.
Ease of Use, Feasibility, Acceptability Older Persons.
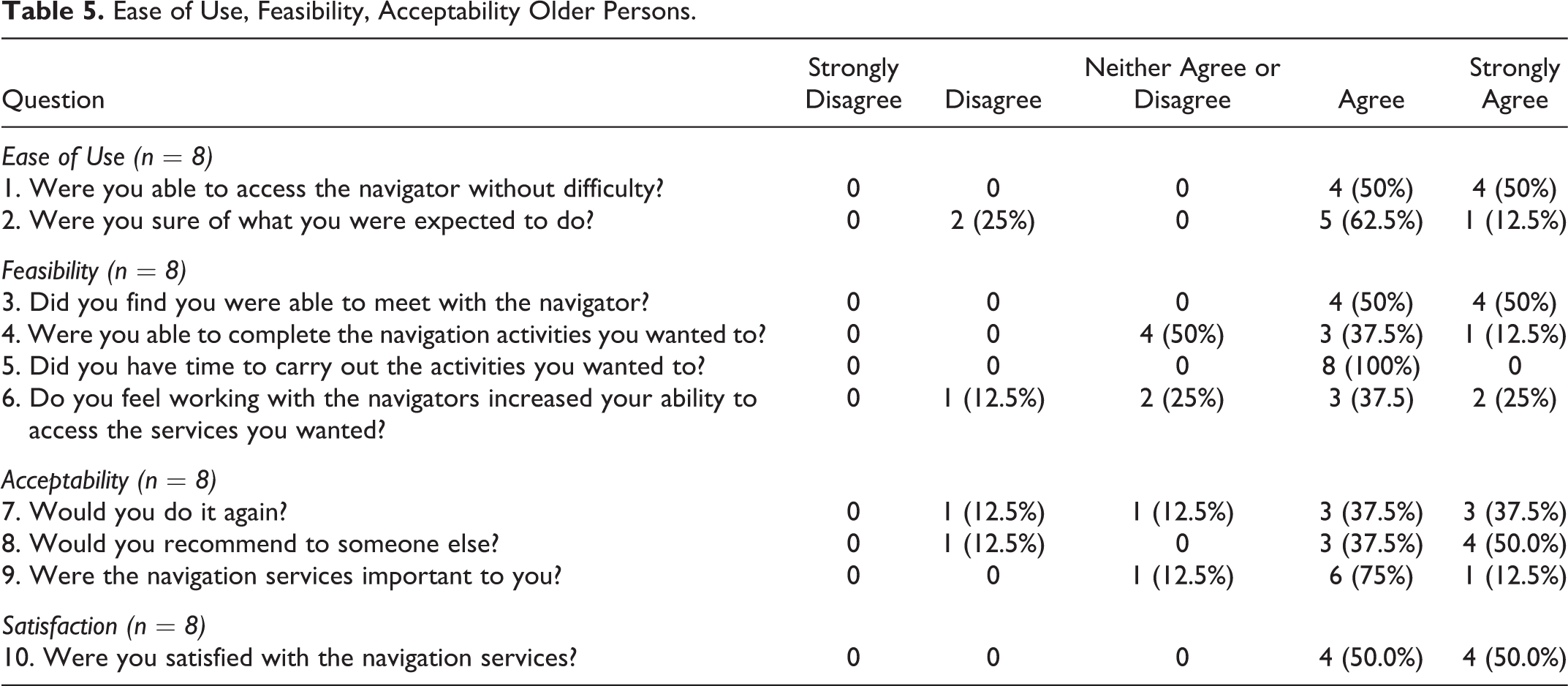
In regard to feasibility (questions 3-6), 100% (8/8) were able to meet with the navigator and had time to carry out navigation activities (8/8). The majority (62.5%;5/8) reported working with the navigators increased their ability to access wanted services. Fifty percent (4/8) reported they were able to complete the navigation activities they wanted to.
The majority of older persons reported acceptability of Nav-CARE (questions 7-9). For example 88% (7/8) agreed or strongly agreed that they would recommend the program to someone else with 75% (6/8) agreeing or strongly agreeing that they would do the program again. As well, 88% (7/8) of participants agreed or strongly agreed that the navigation services were important to them. One hundred percent (8/8) agreed or strongly agreed that they were satisfied (question 10) with the navigation services they received.
The positive evaluation of Nav-CARE by older persons were also found in the evaluation interview data. For example, a participant said: “Oh, the positives: helped me work on getting all these things, putting me in the right direction” (P006). Another participant said: “Everybody deserves to have that kind of program in their life. I think it would be beneficial to many others” (P022).
Discussion
The results from this study suggested that Nav-CARE is an easy to use, feasible, acceptable and highly valued program as reported by older persons and volunteer navigators. Both older persons and volunteer navigators reported satisfaction with Nav-CARE. These findings build on the evidence from the first pilot study in BC, 11 that suggested Nav-CARE showed promise as a beneficial program for rural communities. The 2 communities for this current study were geographically located in a prairie setting, compared to the first pilot which was geographically located in a costal/mountain region. A feature of Nav-CARE is that it can be easily adapted to different communities and this study supports that perception. This may be because Nav-CARE focuses on individual quality of life concerns and response to these concerns.
The results also indicated that Nav-CARE may benefit volunteers, not only by increasing their satisfaction with the volunteer roles and improving their own well-being, but as an opportunity for self-education. The program served to promote self-education for volunteers as they were able to learn about existing community resources that they themselves could access in the future. Satisfaction of Nav-CARE volunteer navigators was also reported in our previous pilot study, 11 but qualitative findings of the benefit of self-education was not reported. In a scoping review of navigation programs, although satisfaction of clients was an frequent outcome measure, 12 the satisfaction of the navigators did not appear to have been a consideration. Future research with volunteer navigators should measure satisfaction and qualitatively explore why volunteers are satisfied, to determine whether self-education should be enhanced as part of supporting volunteers. Education and mentoring has been considered best practice in supporting volunteers. 23
Only 50% of older persons reported they were able to complete the navigation activities they wanted to. This maybe the result of the participants’ serious illness. Volunteers also struggled at times with the tension of recommending resources to older person and older persons not following through with their recommendations. A major principle of Nav-CARE is “working with” older persons in a way that honors the decision making of older persons. The tension experienced by volunteers in our study suggested that the volunteer education training program and mentoring needs to prepare volunteers for this situation. However future research should explore why older persons reported not being able to complete the navigation activities they wanted.
Limitations
One limitation to the study was the sample attrition that occurred over the year-long study for a variety of reasons, resulting in only eight older persons participating in the final evaluation. Similar to the first pilot, 11 this attrition is potentially the result of a year-long study and the participant’s chronic illnesses. However, using a mixed method study, there were multiple data points and with the qualitative interviews there was rich in-depth data to support the findings of this study.
Another limitation is the inclusion of two communities which were in close proximity together, but very diverse in terms of characteristics. With only two volunteers and three older person participants in the smaller community the data was combined with the larger community. With such a small sample size it was difficult to determine if there were any differences because of size of the community. There is a need for future research to determine if the size of the community has an impact on the positive outcomes from Nav-CARE.
Conclusions
Nav-CARE continues to show promise in improving the quality of life of older persons with serious illness and provides a satisfying meaningful role for volunteer navigators in diverse rural communities. .However more research is required to evaluate Nav-CARE in additional communities. Continuous evaluation of navigation programs is important for scale up and spread of these innovations. 12 This feasibility study may be of use in planning for evaluation of other navigation programs in the palliative context and is a foundation for future research.
Footnotes
Acknowledgments
This project received financial support from the Covenant Health Network of Excellence in Seniors’ Health and Wellness. Thanks you to the research assistants who contributed to this work (Kaitlyn Muse, Marina Riccio, Vanessa Ritcher), Wanita Toews (study volunteer coordinator) and the study participants. A Feasibility Study of a Volunteer Navigation Program in the Palliative Context.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received financial support from the Covenant Health Network of Excellence in Seniors’ Health and Wellness Innovation Grant.