
Abstract
Purpose:
Patients with hematological malignancies (HM) have more unpredictable disease trajectories compared to patients with advanced solid tumors (STs) and miss opportunities for a palliative care approach. They often undergo intensive disease-directed treatments until the end of life with frequent emergency department (ED) visits and in-hospital deaths. Insight into end-of-life trajectories and quality of end-of-life care can support arranging appropriate care according to patients’ wishes.
Method:
Mortality follow-back study to compare of end-of-life trajectories of HM and ST patients who died <3 months after their ED visit. Five indicators based on Earle et al. for quality of end-of-life care were assessed: intensive anticancer treatment <3 months, ED visits <6 months, in-hospital death, death in the intensive care unit (ICU), and in-hospice death.
Results:
We included 78 HM patients and 420 ST patients, with a median age of 63 years; 35% had Eastern Cooperative Oncology Group performance status 3-4. At the ED, common symptoms were dyspnea (22%), pain (18%), and fever (11%). After ED visit, 91% of HM patients versus 76% of ST patients were hospitalized (P = .001). Median survival was 17 days (95% confidence interval [CI]: 15-19): 15 days in HM patients (95% CI: 10-20) versus 18 days in ST patients (95% CI: 15-21), P = .028. Compared to ST patients, HM patients more often died in hospital (68% vs 30%, P < .0001) and in the ICU or ED (30% vs 3%, P < .0001).
Conclusion:
Because end-of-life care is more aggressive in HM patients compared to ST patients, a proactive integrated care approach with early start of palliative care alongside curative care is warranted. Timely discussions with patients and family about advance care planning and end-of-life choices can avoid inappropriate care at the end of life.
Keywords
Introduction
The disease trajectories of patients with a hematological malignancy (HM) are diverse, from diseases with an acute manifestation and poor survival to those with a chronic nature. Treatments for HMs, even in patients with a poor clinical condition, are often intensive and are associated with a high risk of severe toxicity (such as graft-versus-host disease), infection, and even death. 1 Because disease trajectories of patients with HM are unpredictable and life threatening, recognition of those who could benefit from a palliative care approach is complicated. 2 -6 As a consequence, patients with HM are seldom referred to palliative care consultation teams (PCCTs) or hospices, and if they are referred, they often die within days or weeks. 2,7,8 It is known that palliative care needs of patients with HM are often unmet. 9 According to the definition of the World Health Organization, the aim of a palliative care approach is to improve quality of life of both patients and family; in addition, it can concur with curative systemic treatment along the disease trajectory. 10 This approach includes conversations about the end of life, supportive care, symptom management, and psychosocial support. 9 Insight into the end-of-life trajectory of patients with HM may help identifying cues for initiation of a palliative care approach.
With the occurrence of disease progression or metastases, the palliative phase in patients with a solid tumor (ST) is easier to identify. 6,7,11 According to Murray, their physical decline is stable and predictable until a steep and short period of decline before death. During the stable phase, health-care providers can proactively assess and support palliative care needs at the end of life. 12 A palliative care approach has been shown to be effective in a various populations of patients with ST in improving quality of life, symptom burden, and even survival. 13 -15 In patients with HM, palliative care can improve the quality of life after hematopoietic stem cell transplantation already after 2 weeks, as a randomized controlled study by El-Jawahri et al. showed. 16 However, literature indicates that patients with HM need a different proactive approach for early palliative care than the disease trajectory of patients with advanced ST. Conceptual models of integrated palliative care for patients with HM depict palliative care as concurrent with curative care to aim for both cure and care. 17 -19 So-called trigger events can help identifying patients with HM with palliative care needs to arrange appropriate care. 20 An ED visit is shown to be a potential trigger. 21
Many patients with HM are urged to visit the emergency department (ED) with uncontrollable symptoms or a high symptom burden at home. Consecutively, they are often admitted to the hospital or even to an intensive care unit (ICU), where many of them die. 2,22,23 These situations can diminish the quality of the end of life of patients with HM and their families. 24 To measure the quality of end-of-life care provided to patients with incurable diseases, Earle et al. constructed the following indicators: receiving chemotherapy in the last 14 days of life, starting a new chemotherapy in the last 30 days of life, >1 ED visit in the last month of life; >1 hospitalization in the last month of life; ICU admission in the last month of life; death in an acute care hospital; lack of hospice admission; and admission to hospice <3 days before death. 24,25
The primary objective of this study was to provide insight into the end-of-life trajectory of patients with HM visiting the ED during the last 3 months of life and to compare them with patients with ST. Secondary objective was to compare the quality of end-of-life care in patients with HM and ST.
Patients and Methods
Setting
This mortality follow-back study was conducted at Leiden University Medical Center (LUMC) in Leiden, the Netherlands. The LUMC’s ED is open 24 hours a day, 7 days a week. On average, 80 patients visit the ED every day and about 30 000 patients are evaluated every year. Since 2011, LUMC has a PCCT, which is available to all departments of our center for consultation after patients are referred by their health care provider. This study was part of a larger study on end-of-life trajectories of all patients visiting the ED between 2011 and 2013, approved by LUMC’s Committee of Medical Ethics on May 27, 2013. Written consent was not required according to Dutch Law (WGBO, article 458) and European Law (General Data Protection Regulation).
Patients
All adult patients with HM who died within 3 months after their last ED visit were included. They were compared to patients with ST having advanced cancer, which was defined as not having any curative options or receiving anticancer treatment not aimed at curation. Detailed analysis of patients with ST is published elsewhere. 26 The period of 3 months was chosen because in the Netherlands, an estimated life expectancy of <3 months justifies referral to intensive palliative care at home, in nursing homes, and in hospices. Data collection occurred from May 2011 to January 2013.
Data Collection
For transparent and solid data collection, a code book was designed by 2 members of our PCCT, which contained inclusion and exclusion criteria and description and coding of all variables.
27
Characteristics of disease, referral, ED visit, and follow-up from ED arrival until death were extracted from electronic patient records (EPRs) of eligible patients by 4 trained research assistants. One expert of the PCCT checked for interrater agreement. Electronic patient records were searched for any correspondence with general practitioners (GPs) or PCCT consultations during the 3 months before the ED visit and proactive symptom management plans in files or letters up to 6 weeks before the ED visit. Limitations on life-sustaining treatments (LSTs) were orders on no resuscitation, no ventilation and no admission to the ICU. Discussions on LST did not occur routinely and notes about LSTs were collected by the research assistants. Arrival at the hospital within office hours was defined as from Monday to Friday between 8
Statistics
Characteristics of patients, referrals, ED visits, and follow-up were analyzed using descriptive statistics. To test differences between patients with HM and ST, we performed χ2 tests for nominal variables, Mann-Whitney U tests for non-normally distributed continuous or ordinal variables, and Fisher-Freeman-Halton tests for variables with 3 or more categories. Kaplan-Meier’s methodology was used to estimate survival from the ED visit, and survival between patients with HM and ST was tested using a log-rank test. Complete case analyses were performed, using SPSS 23.0 software, and a 2-sided P value <.05 was considered statistically significant.
Results
Patient and Disease Characteristics
Seventy-eight patients with HM and 420 patients with ST died within 3 months after their ED visit (Table 1); more men were in the HM group (67.9% vs 54.5% of patients with ST, P = .026); median age was 63 years (range: 22-94 years). Eastern Cooperative Oncology Group performance score did not differ between patients with HM and ST. Acute myeloid leukemia and multiple myeloma were the most common HM types (26% and 17%, respectively); most STs were located in the digestive tract (27.6%) and in the lung (16.0%; Online Appendix 1). Before the ED visit, limitations on LSTs were discussed with 171 patients (34.3%): with 13 (16.7%) patients with HM and 158 (37.6%) patients with ST (P < .0001). Four (5.1%) patients with HM and 142 patients with ST (33.8%) had documented limitations; “no limitations” were documented in 9 (11.5%) patients with HM and 16 (3.8%) patients with ST (P < .0001). Up to 3 months before the ED visit, the PCCT was consulted in 27 patients (1 patient with HM and 26 patients with ST, P = .10). Communication via letters, telephone, and transfers between medical specialists and the patient’s GP had occurred in 67 (85.9%) patients with HM and 332 (79.0%) patients with ST (P = .15). Proactive care plans were documented for 13 (16.7%) patients with HM and 66 (15.7%) patients with ST (P = .83).
Characteristics of 78 Patients With a Hematological Malignancy and 420 Patients With a Solid Tumor Visiting the Emergency Department.
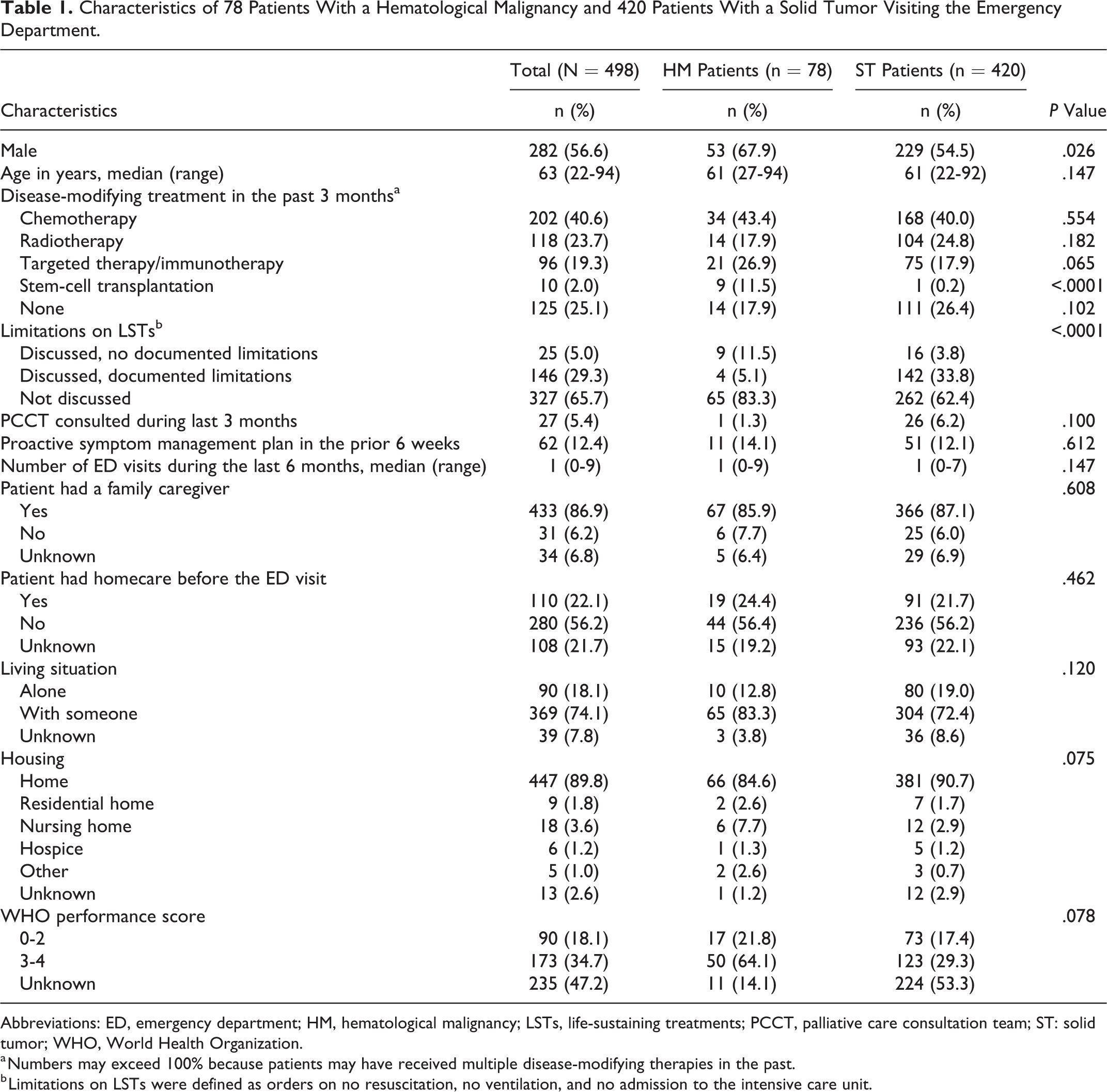
Abbreviations: ED, emergency department; HM, hematological malignancy; LSTs, life-sustaining treatments; PCCT, palliative care consultation team; ST: solid tumor; WHO, World Health Organization.
a Numbers may exceed 100% because patients may have received multiple disease-modifying therapies in the past.
b Limitations on LSTs were defined as orders on no resuscitation, no ventilation, and no admission to the intensive care unit.
Referral Characteristics
Patients or their family initiated the ED visit in 37.3% (Table 2). Two hundred fifty-eight (51.8%) came outside office hours. Most common main symptoms were dyspnea (22.1%), pain (17.5%) and fever (11.2%). Patients with HM more often presented with fever (23.1% vs 9.0% of the patients with ST, P = .001); patients with ST more often presented with nausea or vomiting (9.3% vs 2.6% of the patients with HM). Patients had a median of 2 symptoms.
Emergency Department-Referral Characteristics of 78 Patients With a Hematological Malignancy and 420 Patients With a Solid Tumor.
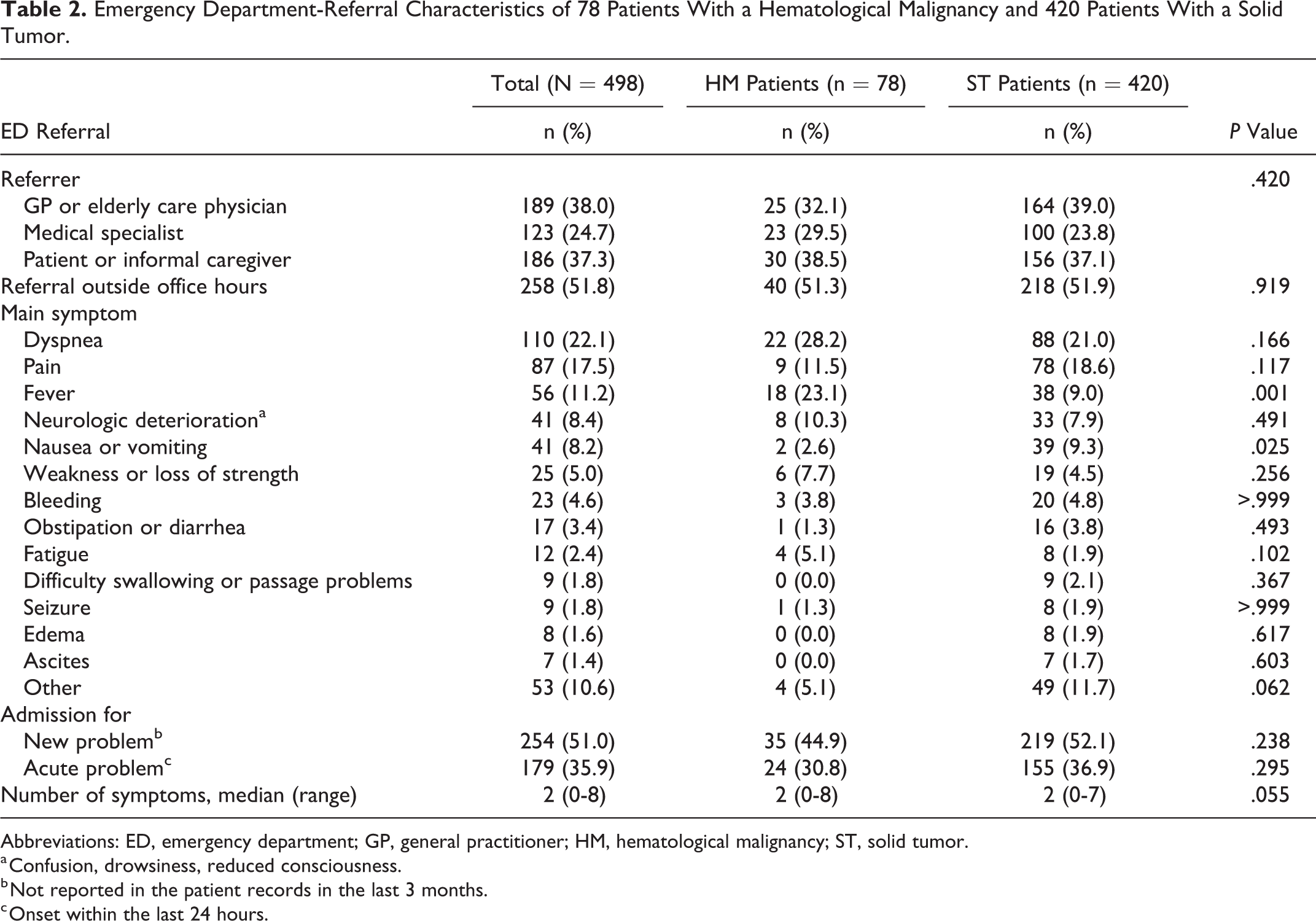
Abbreviations: ED, emergency department; GP, general practitioner; HM, hematological malignancy; ST, solid tumor.
a Confusion, drowsiness, reduced consciousness.
b Not reported in the patient records in the last 3 months.
c Onset within the last 24 hours.
Visit and Follow-Up Characteristics
Patients underwent diagnostic imaging in 64.1% and laboratory tests in 84.1% (Table 3). Most patients were diagnosed with infection or fever (24.5%), bronchopulmonary insufficiency (14.3%), or renal insufficiency (11.8%). In patients with HM, treatment for their main symptoms was initiated at the ED more often than in patients with ST (69.2% vs 54.8%, P = .010). After their ED visit, more patients with HM were hospitalized than in patients with ST (91.0% vs 76.0%, P = .001). The ED visit triggered discussions about LSTs in both patients with HM and ST. After the ED visit, LSTs were documented for 41 (52.6%) patients with HM and 307 (73.1%) patients with ST (P < .0001). Among these patients, 39 (95.1%) patients with HM and 297 (96.7%) patients with ST had limitations on LSTs (P = .64). Median survival from the ED visit was 17 days (95% confidence interval: 15-19) and was significantly shorter in patients with HM (15 days vs 18 days, P = .028). In-hospital death occurred in 67.9% of the patients with HM versus 29.5% of the patients with ST; patients with HM died at home in 15.4% versus 38.3% of the patients with ST (P < .0001). In patients with HM, causes of death were disease progression (46.2%), treatment toxicity (39.7%), or both (9.0%).
Emergency Department Visit and Follow-Up Characteristics of 78 Patients With a Hematological Malignancy and 420 Patients With a Solid Tumor.
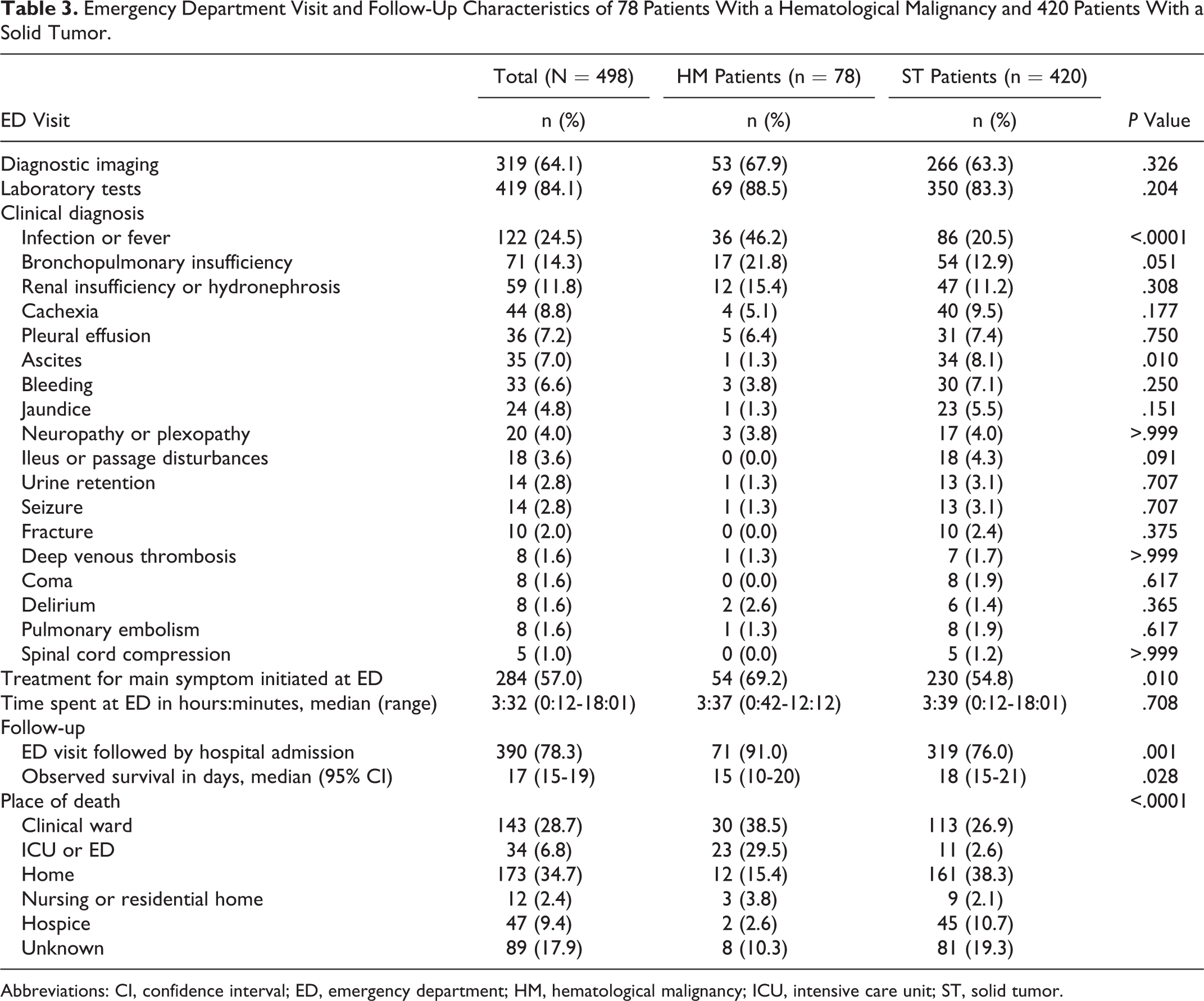
Abbreviations: CI, confidence interval; ED, emergency department; HM, hematological malignancy; ICU, intensive care unit; ST, solid tumor.
Quality of End-of-Life Care
Quality of end-of-life care in patients with HM and ST is shown in Table 4. Intensive anticancer treatment was administered to 375 (72.4%) of all patients up to 6 months before the ED visit, to 75.6% of the patients with HM versus 71.8% of the patients with ST, P = .48. Patients with HM died more often in hospital compared to patients with ST (67.9% vs 29.5%, P < .0001), in an acute hospital setting (29.5% vs 2.7%, P < .0001), and less often in a hospice (2.6% vs 10.5%, P = .011).
Comparison of Indicators of Quality of End-of-Life Care Between 78 Patients With a Hematological Malignancy and 420 Patients With a Solid Tumor.
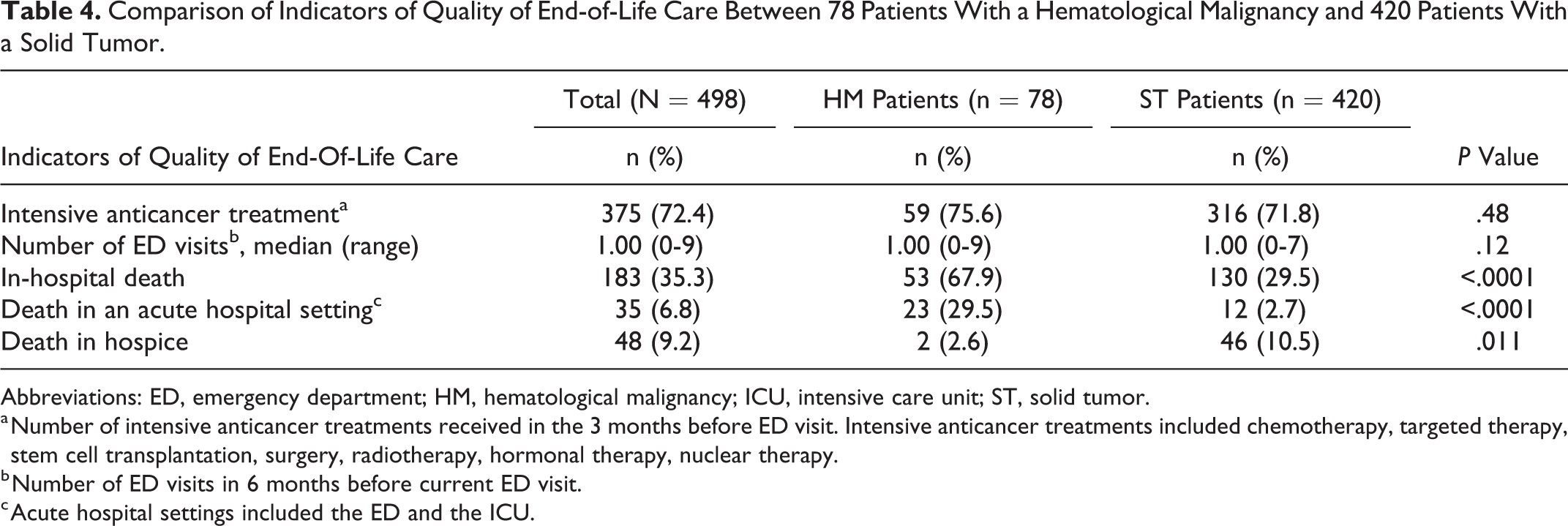
Abbreviations: ED, emergency department; HM, hematological malignancy; ICU, intensive care unit; ST, solid tumor.
a Number of intensive anticancer treatments received in the 3 months before ED visit. Intensive anticancer treatments included chemotherapy, targeted therapy, stem cell transplantation, surgery, radiotherapy, hormonal therapy, nuclear therapy.
b Number of ED visits in 6 months before current ED visit.
c Acute hospital settings included the ED and the ICU.
Discussion
This study gives insight into the disease trajectory of patients with HM and into the differences compared to the disease trajectory of patients with an ST visiting the ED in the last 3 months of their lives. Limitations on LSTs were often not discussed in patients with HM before their ED visit, and if these were discussed, patients often had no limitations on LSTs. End-of-life care was considerably more aggressive in patients with HM compared to patients with ST. Patients with HM had a worse survival than patients with ST and more often died in-hospital and in the ICU and seldom in a hospice.
Our results implicate that end-of-life care is aggressive in patients with HM: they scored poorly on 5 of the indicators of quality of end-of-life care by Earle. 24 Our findings are in accordance with international literature reporting that patients with HM receive intensive treatments until death. In a study by Hui et al., patients with HM received significantly more chemotherapy (21%) and targeted therapy (17%) than patients with ST (6% and 5%, respectively). 2 Other studies report that patients with HM often received granulocyte-colony stimulating factor, blood transfusions, and antibiotics and underwent diagnostic imaging, blood sampling, endoscopy, and bone marrow examination in the last 7 days of life. 23,29 A French study in patients who died of metastatic lung cancer showed that end-of-life care was less aggressive the earlier palliative care needs were reported in their EPRs: patients sooner stopped with anticancer treatment and they underwent less often invasive ventilation. 30 In patients with pancreatic cancer in the last 30 days of life who were referred to a palliative care service, those with an early referral to a palliative care team visited the ED less often and were less often hospitalized. 31 It thus seems that when palliative care is integrated into oncology care, patients with ST are at a lower risk of aggressive end-of-life care. In our study, limitations on LSTs were seldom discussed with patients with HM, and remarkably, if it was discussed, it was often explicitly stated in their EPRs that there were no limitations on LSTs. A recent integrative systematic review provided more insight into the aspects of this “curative mind-set”: hematologists feel uncomfortable with hospice referrals and discussing approaching death with patients and family; disease progression is considered as personal failure; and they are concerned that mentioning palliative care early in the disease trajectory might scare patients and their relatives. 6 A qualitative study by Prod’homme et al. showed that end-of-life discussions are avoided by hematologists as long as cure is possible; these discussions are perceived to damage the doctor–patient relationship, especially when the patient’s prognosis is uncertain. 32 In addition, hematologists interpret palliative care more often as end-of-life care than medical oncologists do and are less used to involve a palliative care specialist than medical oncologists. 33 It is known that if patients with HM are referred to palliative care, it generally occurs very late in their disease trajectory. 3,7,11 Although a curative care approach toward patients with HM could be appropriate, the way it is currently practiced discourages timely initiation of a palliative care approach and conversations about the end of life. El-Jawahri et al. reported that 27% of the hospital admissions in acute myeoloid leukemia patients could have been avoided. 34 Reasons were: being discharged too soon after the previous admission, visits for problems that would have been manageable at home, and the lack of timely outpatient follow-up appointments. These reasons are starting points for initiating a palliative care approach to avoid possible aggressive and harmful treatments in vulnerable patients.
Our study suggests that in many patients the ED visit marked deterioration and a transition in disease trajectory and often even the start of the dying phase. After the ED visit or following hospital admission, limitations on LSTs were discussed and documented in 73% of the patients with ST and 53% of the patients with HM. Although efforts were made to discuss these LSTs, still 36% of the patients with HM were subsequently transferred to the ICU. This is in line with literature demonstrating that patients with HM are frequently and more often admitted to ICUs than patients with ST (39% and 8%, respectively). 2 Failure to recognize patients in the end-of-life phase makes them at risk of receiving aggressive treatments in the hospital and may even result in death: in our study, 33% of the patients with HM died in the ICU, compared to 4% of the patients with ST (P < .0001). 2 Sixty-nine percent of our patients with HM died in the hospital and 40% died as a result of treatment toxicity. Howell et al. showed that, compared to patients with ST, patients with HM had a twice higher risk to die in the hospital. 22 Our findings confirm that patients with HM have unpredictable disease trajectories that can suddenly change from curative to dying: most of our patients died shortly after the ED visit with a median survival of only 15 days. Reasons for difficulties to predict survival and to recognize the transition to the end-of-life trajectory are possibly reversible conditions such as infections, increasing availability of systemic therapies that stimulate continuance of active treatment and increase the risk of lethal complications. 1,35 Long-lasting physician–patient relationships are also known to hamper accurate recognition of deterioration. 6 The combination of these factors makes it difficult for physicians to recognize approaching death in patients with HM and to timely prepare them for their approaching death.
A Proactive Integrated Care Approach
We advocate, as Zimmermann, Bruera, LeBlanc, El-Jawahri, Chung, and Button do, the use of an integrated care approach with 2 concurrent tracks: a curative approach and palliative care approach (Figure 1). 16 -19,36,37 Integrated care should be initiated early in the disease trajectory if the disease is potentially life threatening (which can be at diagnosis). The first track consists of conventional disease treatment aimed at cure. The second track consists of supportive care following the 4-dimensional principles of palliative care: physical, psychological, social, and spiritual. Importantly, the second track also includes discussions about future problems, treatment choices, hospital admissions, LSTs, and place of death. The palliative care approach has shown to benefit symptom control 37 and quality of life, 38 to decrease ED visits, hospital and ICU admissions and in-hospital deaths, 39,40 and might even prolong survival. 41 In the integrated care approach, multidisciplinary discussions and communication across specializations within and outside the medical field are crucial to satisfy care needs. The randomized clinical trial by El-Jawahri et al. demonstrated that inpatient palliative care improved the quality of life of patients with HM already within 2 weeks after hematopoietic stem cell transplantation had taken place. 16
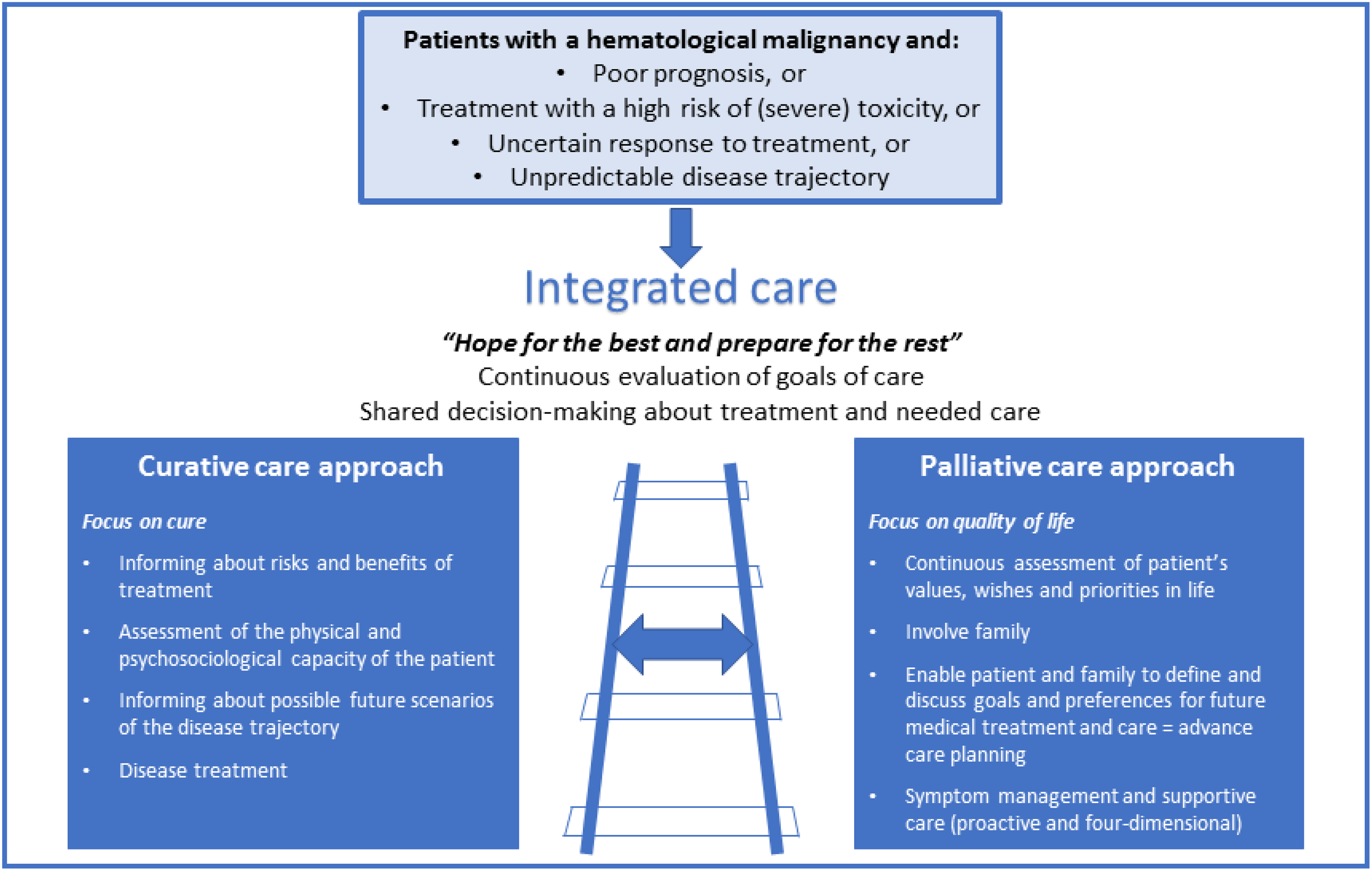
A proactive integrated care approach for patients with a hematological malignancy: a curative and a supportive track.
Our pragmatic study provides insight into the care for patients with HM visiting the ED in their end-of-life trajectory and compared it with the disease trajectory of patients with ST. The inclusion of only those patients who died within 3 months after the ED visit is inherent to the mortality follow-back design of this study, but it has introduced selection bias. Although data were collected from 2011 to 2013, they are still relevant since new life-prolonging systemic treatments only further emphasize the need for an integrated care approach. Further research should be directed to identifying the specific palliative care needs of patients with HM and their families and developing interventions to address to those.
We would like to thank Leanne Smit, Tobias Wieles, Mathijs Kruizinga, Iris Groeneveld, Lotte van der Stap, and our colleagues at the Center of Expertise Palliative Care of the LUMC.
Conclusions
Patients with HM who visited the ED in the last 3 months of life are more often hospitalized and die in hospital compared to patients with ST. To improve care during the end-of-life trajectory, especially for patients with HM, palliative care should be timely integrated in standard oncological care.
Supplemental Material
Supplemental Material, Appendix_1 - End-of-Life Trajectories of Patients With Hematological Malignancies and Patients With Advanced Solid Tumors Visiting the Emergency Department: The Need for a Proactive Integrated Care Approach
Supplemental Material, Appendix_1 for End-of-Life Trajectories of Patients With Hematological Malignancies and Patients With Advanced Solid Tumors Visiting the Emergency Department: The Need for a Proactive Integrated Care Approach by Mary-Joanne Verhoef, Ellen J. M. de Nijs, Claudia S. Ootjers, Marta Fiocco, Anne J. Fogteloo, Christian Heringhaus, Corrie A. M. Marijnen, Nanda Horeweg and Yvette M. van der Linden in American Journal of Hospice and Palliative Medicine®
Footnotes
Authors’ Note
As approved by the Medical Ethics Committee of the LUMC and according to Dutch and European law, informed consent from patients was not necessary because of the retrospective design of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.