
Abstract
Background:
Whole person care is appropriate for seriously ill persons. The current framework of palliative care domains in the National Consensus Project (NCP) Guidelines for Quality Palliative Care offers an opportunity to reassess the domains of care delivered at home, earlier in the course of illness.
Objective:
This qualitative study was used to test the applicability of a proposed, expanded set of domains. The results were used to inform a home-based, upstream model of supportive care for serious illness.
Methods:
Quotes relating to the experience of late-life serious illness were derived from transcripts of 12 semi-structured group interviews conducted with patients, family, and professionals. Quotes originally coded to the NCP domains of palliative care were then coded to the proposed domain set, which included new categories of family/caregiver, legal/financial, and legacy/bereavement domains.
Results:
A total of 489 quotes were assigned to the proposed expanded set of domains. One hundred one (19%) coded to the family/caregiver domain, 28 (5%) to the legacy/bereavement domain, and 27 (5%) to the legal/financial domain. Ninety-seven (87%) of the 111 quotes coded to family/caregiver had been initially coded to the NCP social aspects of care. Family/caregiver themes included challenges, rewards, insights, and family growth.
Conclusion:
The preponderance of family-related issues suggests that including the family domain may promote recognition and support of family caregivers and the services they provide. Although this study provides some support for including the legacy/bereavement and legal/financial domains, additional research is needed to determine whether there is a basis for including them in the domain structure.
Introduction
Whole person care has been proposed as a new paradigm for the care of serious illness. 1 –3 The discipline of palliative care extends holistic features of primary care 4 and geriatrics 5 into a coherent practice that acknowledges the nonmedical facets of suffering. 6 Beginning in 2006, the National Consensus Project (NCP) for Quality Palliative Care developed guidelines defining deliverables of palliative care and providing benchmarks for quality improvement. 7 –9 These guidelines were arrayed within a framework of domains such as social, spiritual, or physical aspects of care. The domain structure was developed using patient/family surveys, existing recommendations, and statements of principle. 10 –14
This domain construct supports performance metrics intended to reflect the interdisciplinary nature of palliative care programs. Although obvious in one sense, this orientation to measurement draws us away from the source of holism—the person herself or himself. As palliative care enters earlier in disease, are there opportunities to enhance the person-centered aspects of the NCP domain framework?
Four aspects of the framework deserve mention. The social aspects of care domain is broad, encompassing interpersonal relationships, finances, work, sexual intimacy, caregiver stress, and social networks. 9 Understanding the depth of the social aspects of care domain could guide training and practical implementation for workers in the field.
A second reality of the current domain framework is its orientation to the activities of professional disciplines. In the example of social aspects of care, implementation has been described in the context of social workers operating in health-care settings. 15 Revisiting the domains provides an opportunity to position their implementation upstream in the course illness and across disciplines.
Third, the inherent limitations of biopsychosocial assessment tools argue for robust representation of whole person within the domain structure. The NCP guidelines reference the Edmonton Symptom Assessment System (ESAS), commonly used in palliative research and practice for assessing medical and emotional symptoms. 16 When applied to patients with severe heart failure, ESAS symptom scores exhibit poor correlation with validated measures of social functioning and self-efficacy, attributes that independently mediate drivers of effective self-care. 17,18 Studies of persons with advanced lung cancer or heart failure reveal they suffer distress from impending mortality, functional loss, and social isolation. 19 Even when emotional distress is identified, it may be a marker for suffering in other, unarticulated domains. 20 As Cassel points out, we are known and suffer as unitary beings, not as the sum of whole person components. 21 Without balanced exploration of the broader psychosocial and spiritual experience of illness, even multidimensional assessment tools could result in a reductive and inadvertently medicalized approach to the complexity of individuals.
Finally, delivering palliative care earlier in the course of illness may raise previously unidentified issues in distinct aspects of personhood. Key issues in nonmedical domains may be better appreciated if the work is approached from an intentionally holistic perspective.
Owing to the breadth of the NCP social domain, the professional orientation of guidelines, and the limitations of clinical assessments, the framework of domains offers opportunity for refinement.
The current study explores the applicability of an expanded palliative care domain set to patient and family experiences of serious illness. This analysis will explore evidence for expanding the current NCP domains to include the additional domains of family/caregiver, financial/legal, and legacy/bereavement.
Methods
This analysis is part of a late-life supportive care research study begun in 2012 for patients with serious illness potentially in their last 3 years of life. The intervention is designed to systematically support whole person care. The clinical intervention uses trained lay health-care workers to meet with patients and families in their homes. These workers, called care guides, provide whole person support and linkage to medical and nonmedical resources. 22 Successful implementation of care guides for managing chronic conditions in the clinic led the researchers to propose a trained lay person working in the community as part of the health-care team. 23
The supportive care approach used in this research was developed with inputs from caregivers, patients, and providers. The clinical team also provided insights in the pilot phase. Based on these inputs, the NCP domain framework was expanded early in the approach. Three expanded domains were proposed: family/caregiver, financial/legal, and legacy/bereavement.
Participants and Procedures
Twelve semi-structured focus interviews were conducted with groups of 2 to 8 participants between March 3, 2012, and June 30, 2012. Participants who had experience with a variety of chronic medical conditions were recruited from senior living communities, faith communities, provider organizations, and disease advocacy associations (see Table 1). Of 73 individuals, 23 were patients, 29 were family, and 19 were professionals. Of the professionals interviewed, 4 were palliative-trained clinicians: 2 physicians, 1 social worker, and 1 chaplain. The remainder included physician/advance practice nurse providers (5), nurses (2), chaplains (6), social workers (2), occupational therapist (1), and administrator (1). Eight of the professionals related personal experiences caring for loved ones, and it was these quotes that were included in the data set; professionals’ comments on patients or on care they provided were not included. Diagnoses relevant to the patients and caregivers were dementia (28), cancer (16), chronic respiratory disease (11), heart failure (5), and other (3). Participants received no compensation. Interviews were facilitated by a family physician and lasted 90 to 120 minutes. Questions were selected by the facilitator from a question set to stimulate discussion within the group. Not all questions were asked of each group (Appendix A).
Interview Participants.
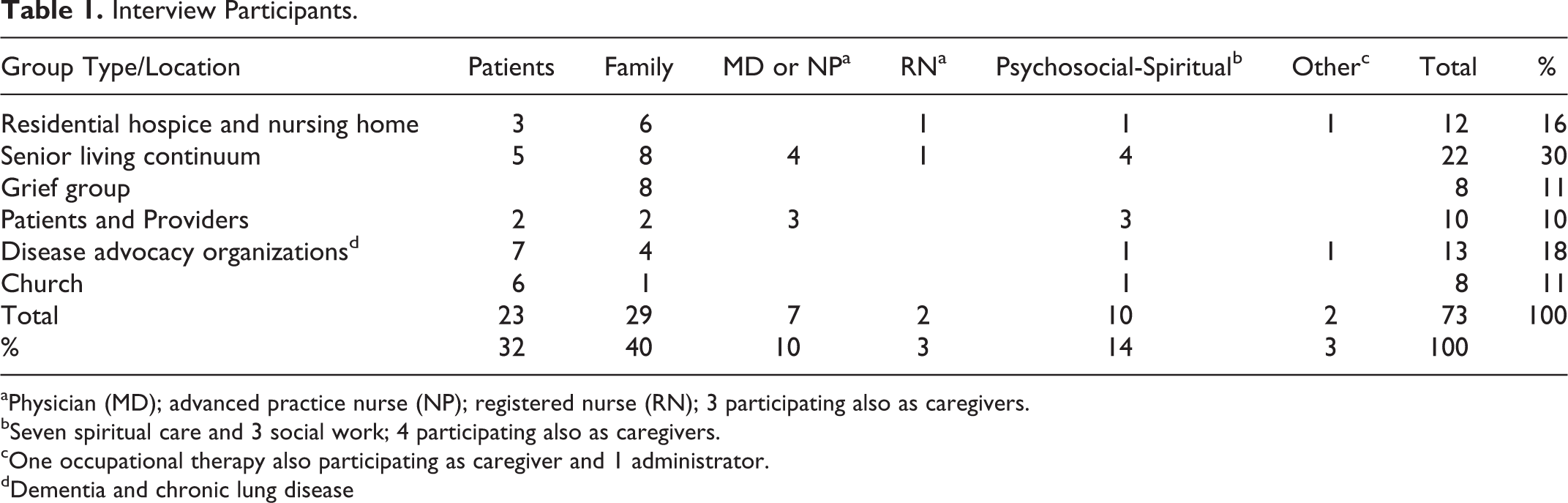
aPhysician (MD); advanced practice nurse (NP); registered nurse (RN); 3 participating also as caregivers.
bSeven spiritual care and 3 social work; 4 participating also as caregivers.
cOne occupational therapy also participating as caregiver and 1 administrator.
dDementia and chronic lung disease
A public television crew filmed the sessions. Unrelated content was edited out, and dialogue was transcribed by a researcher. These transcripts provided the data for analysis. Quorum Review Institutional Review Board (IRB) granted approval for use of the transcripts.
Analysis
Qualitative method
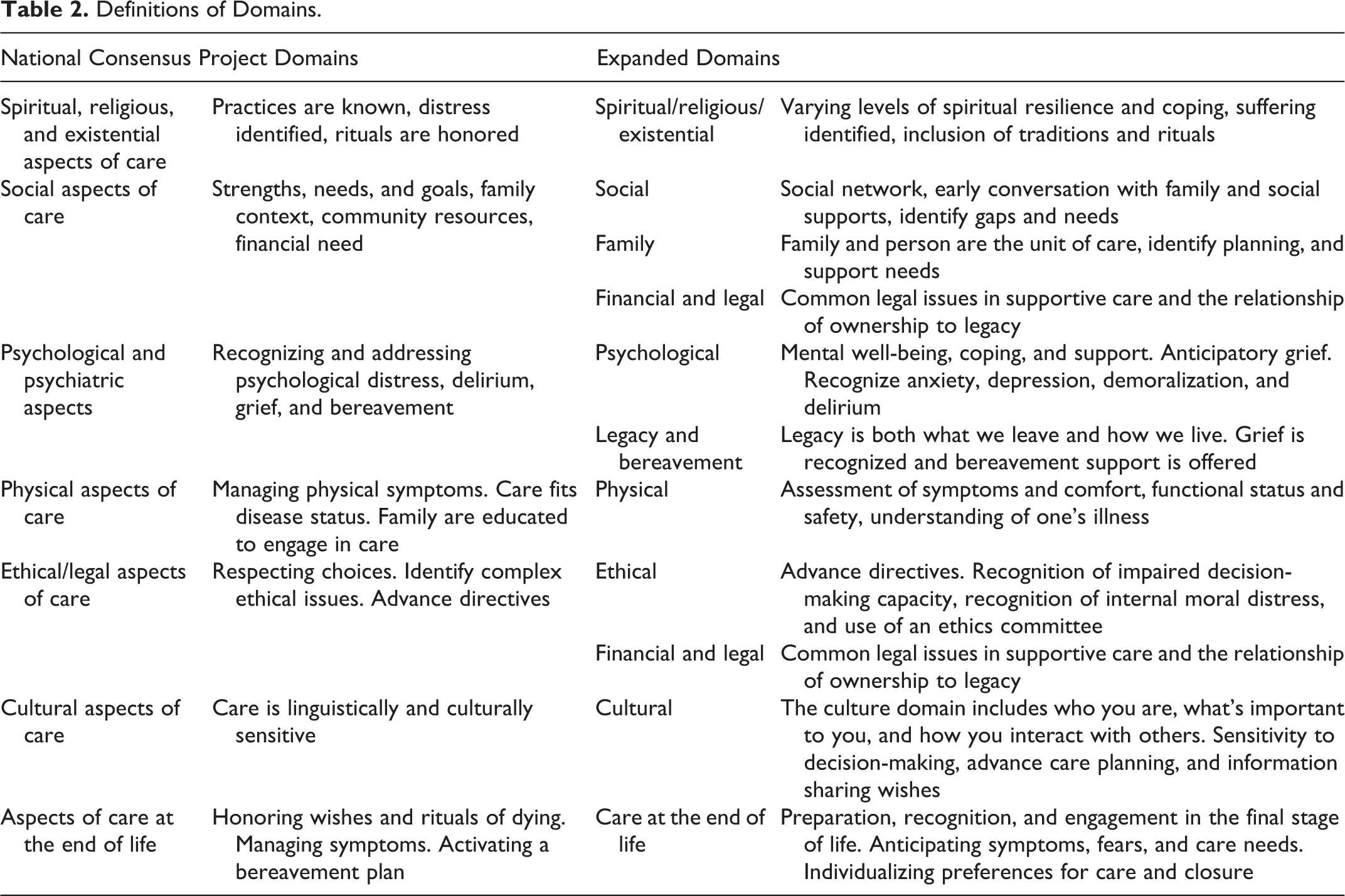
A 3-step approach was used to assign quotes to domains. Two researchers (E.W.A., M.S.F.) deductively double coded 25% of transcripts to assign quotes to the 8 existing NCP domains. 9 Coding rules for the NCP guideline domains were established using an iterative process (see Table 2). 9,24 Coding agreement was 95.0%. This set of quotes was then coded to the proposed expanded domain set. Twenty-five percent of interviews were coded by both researchers, with 99.0% agreement. The remaining transcripts were coded by 1 researcher (E.W.A.). Thematic analysis was conducted as a third step within the second cycle. NVivo 10.0 software was used for data management. 25 Simultaneous coding was used, applying quotes to more than 1 domain. 24 The data were numerically represented by enumerating the one-to-many relationships between quotes and domains. 26 Deidentified transcripts and coding assignments are available from the authors.
Definitions of Domains.
Results
Four hundred eighty-nine quotes were coded a total of 591 times to the NCP domains (see Table 3). The left side of Table 3 shows results of first cycle coding to the NCP domains, and the right side shows results of second cycle coding to the expanded domains. The proposed domains of family/caregiver, legacy/bereavement, and financial/legal accounted for 168 (29%) of all quotes. Of the 111 items coded to the family/caregiver domain, 97 had been coded originally to the NCP social aspects of care domain. The remaining 13 were split between ethical–legal, psychological, and spiritual, with a single quote from the physical domain. The main sources of quotes for the financial legal domain were originally coded to NCP ethical (13) and social (11) aspects of care. The proposed legacy/bereavement domain was composed largely of quotes from the NCP psychological (15), social (5), and spiritual (4) aspects of care.
Distribution of Serious Illness Interview Content to Domains.
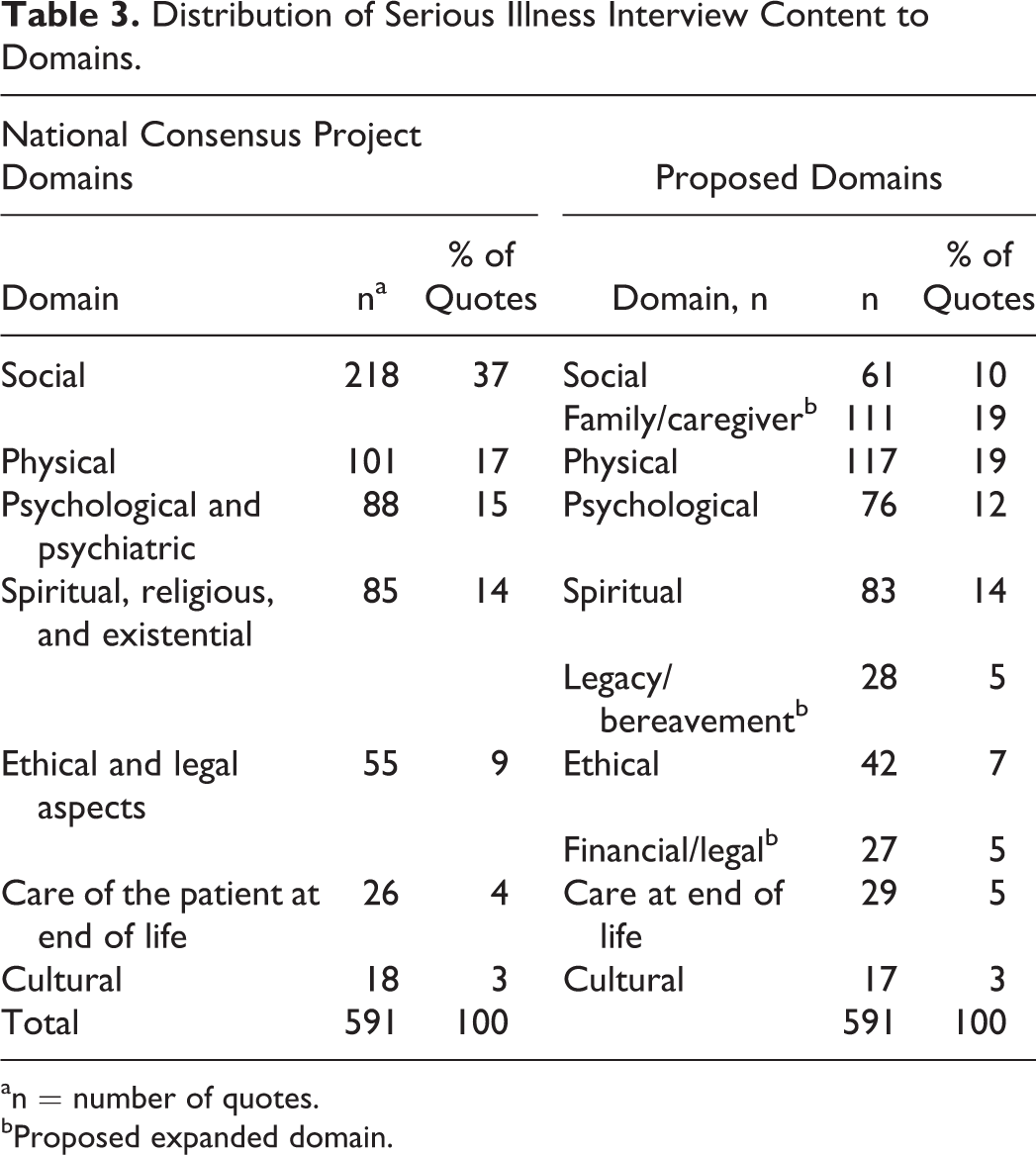
an = number of quotes.
bProposed expanded domain.
Thematic Analysis of Family/Caregiver Quotes.
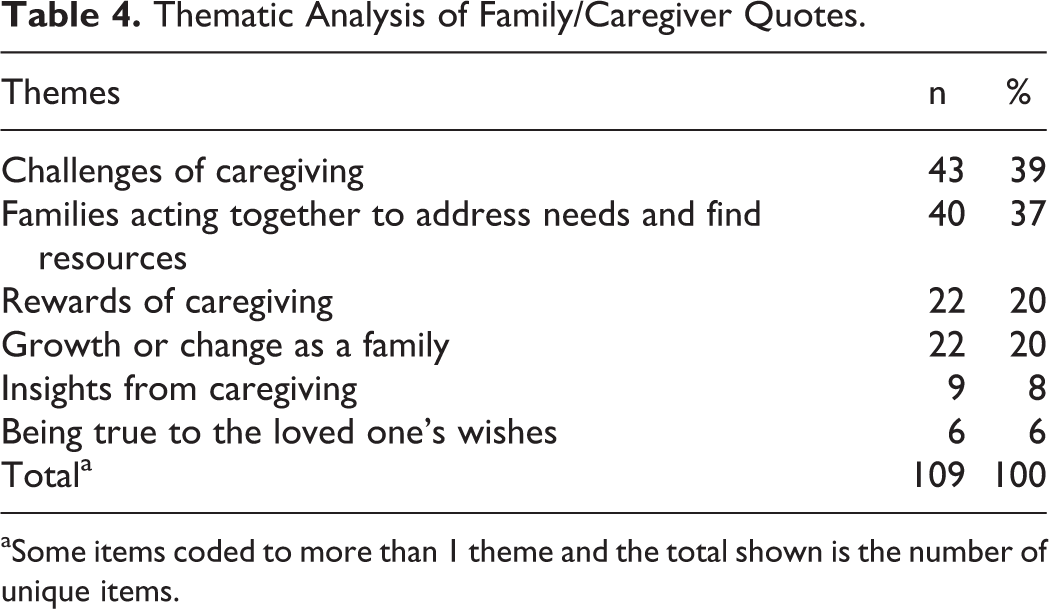
aSome items coded to more than 1 theme and the total shown is the number of unique items.
Thematic Analysis of the Proposed Domains
Family/caregiver domain
Six broad subthemes emerged, describing challenges, collective family actions, rewards, family growth, insights from experience, and honoring wishes of the person in care (Table 4). Participants voiced many challenges of caregiving. Family members struggled with obligations to parents, spouses, and children, while needing more than their families could sometimes provide.
My siblings have been good with support. I don’t think they all get it.…But my circle of friends—people who have been through it—have just been an incredible source of information and support.
Struggles with gender roles are reflected in a man’s discomfort at buying incontinence diapers (Table 5) and on comments by female caregivers about their role carrying the emotional burden, (“I think women kind of take on the emotional piece”). Finally, participants described the irremediable weight of caregiving, the “plodding, endless trek.”
Exemplars of Themes in the Family/Caregiver Domain.
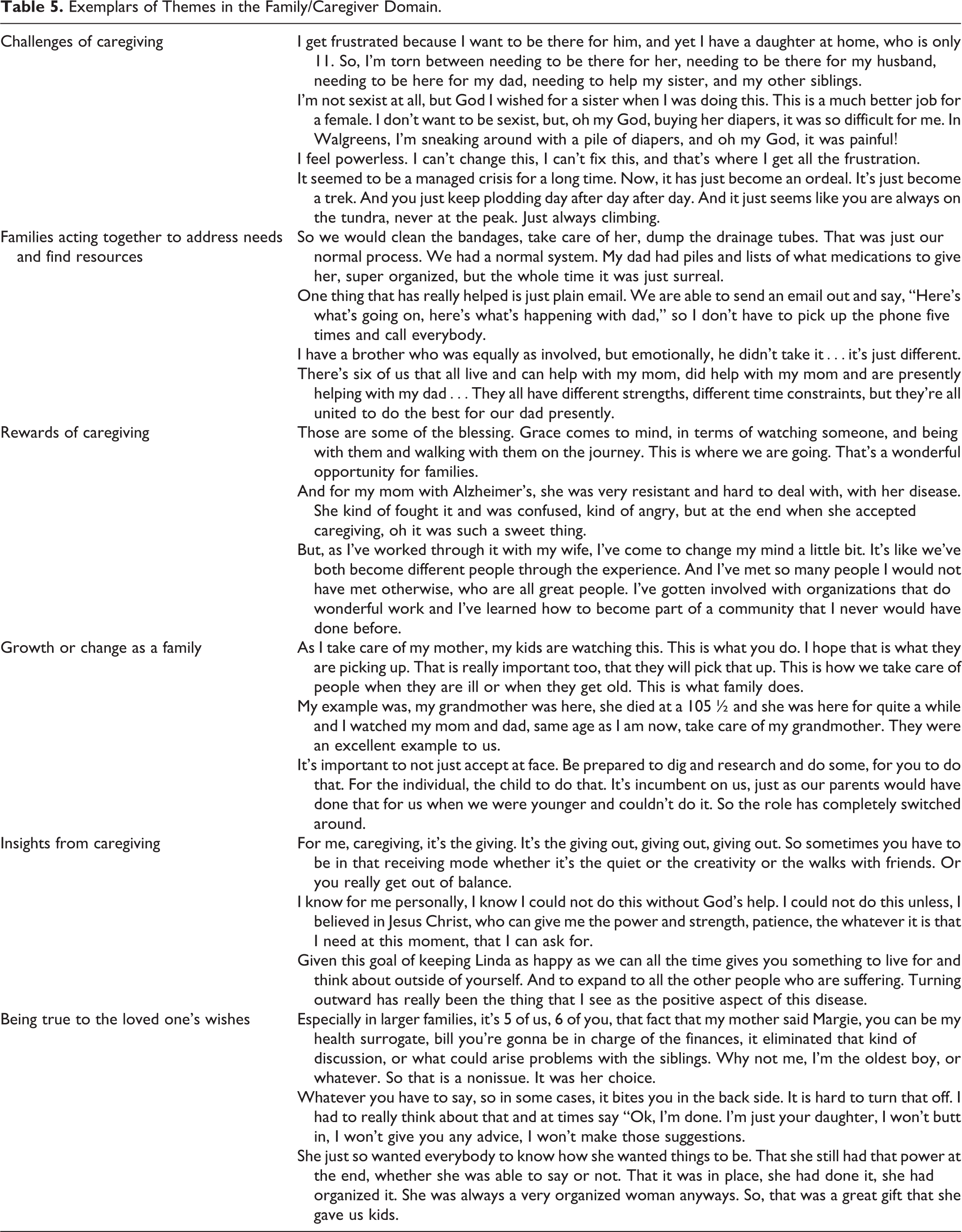
Amidst these challenges, families acted together to address needs and find resources. Families organized and managed complex care, often with little outside direction. Although participants commented on temperamental differences in the family, most expressed gratitude for teamwork.
Participants also described rewards of caregiving, such as having time with their loved one, feeling changed for the better by the experience, entering new communities and relationships, and receiving gifts of grace from their loved one. (“I was only able to do [his caregiving] because…of the type of person he was. He was just a wonderful, wonderful, wonderful man.”)
According to participants, families experienced growth and change. Adult children accepted the challenge of role reversal, while trying to support their parents’ autonomy. Several participants spoke of modeling caregiving for future generations. (“This is how we take care of people…This is what family does.”)
Participants also shared personal insights gained from caregiving. Quotes revealed learnings about setting limits, finding balance in life, and accepting spirituality.
Finally, the theme of honoring the loved one’s wishes was expressed in 2 ways. When the ill person articulated his or her wishes, it relieved family of the potential for conflict. When wishes were unclear, families routinely spoke of the struggle to make decisions. (“She had Parkinson’s, and by the time it progressed she couldn’t tell us [what she wanted]…So that was very difficult.”)
Financial/legal domain
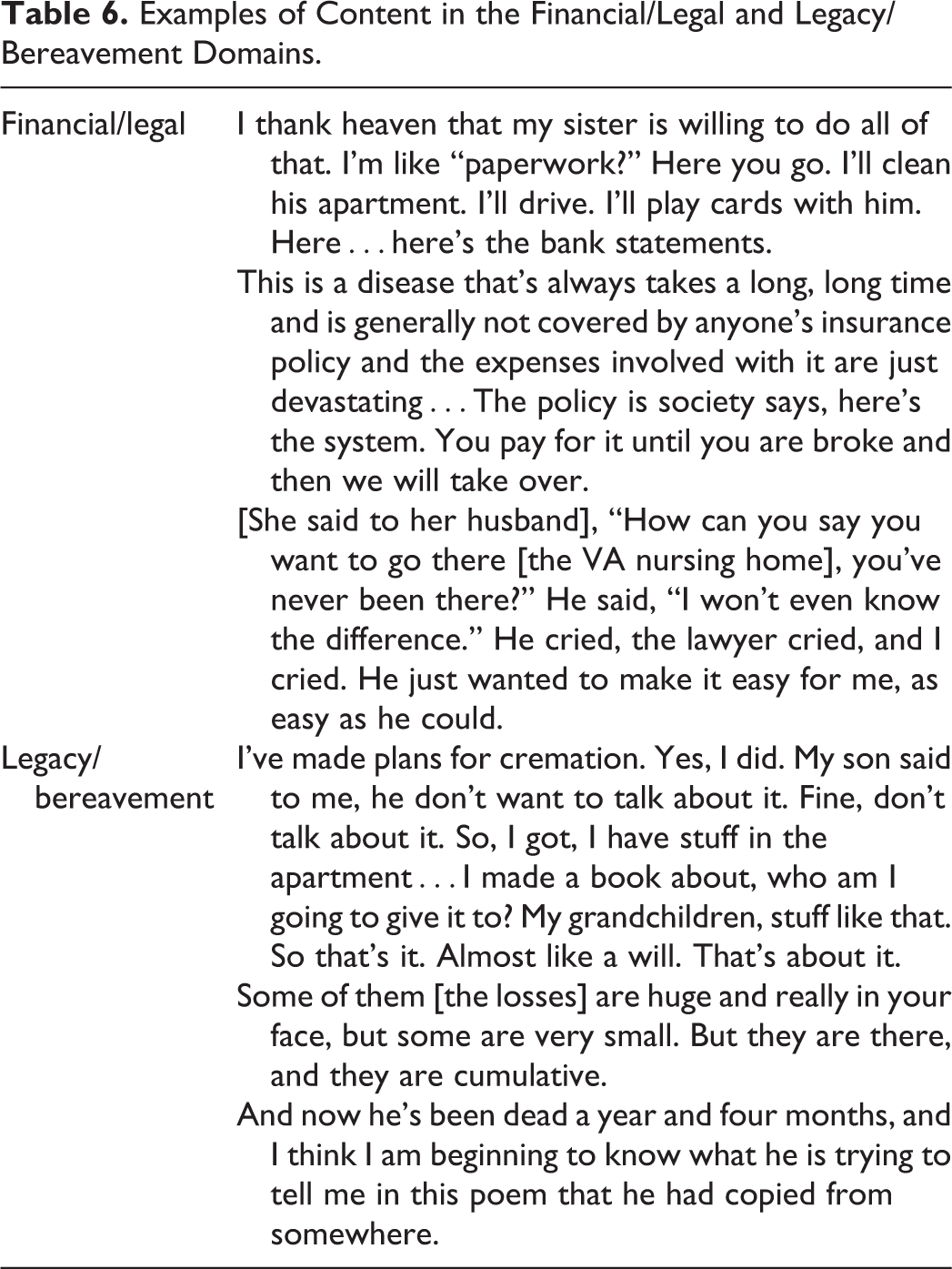
Quotes shown in Table 6 demonstrate a range of issues in this domain. Paperwork, lawyers, wills, and insurance were topics of concern in the interviews. Families feared losing assets to pay for care, and they found legal and financial paperwork daunting. Other quotes dealt with the cost of care for a protracted illness, overshadowed by the threat of impoverishment. Legal and financial decisions often were the substrate from which intense interpersonal experiences emerged, exemplified by the final quote in the legal/financial section of Table 6.
Examples of Content in the Financial/Legal and Legacy/Bereavement Domains.
Legacy/bereavement domain
In this proposed domain, patients spoke of the continued search for meaning, despite their impending mortality. (“We are in a position where people are helping us now. It is nice not to always be helped. It is nice to be helping.”) Both patients and family spoke of actions taken before death that would affect how they would remember or be remembered (Table 6). Patients and families commented on each other’s reactions to discussions of legacy. For some family members, it was an uncomfortable reminder of their loved one’s mortality. (“My son said to me, he don’t want to talk about it.”) For others, it was affirmation of the qualities they admired in their seriously ill family member. (“My mother wrote her own obit, she planned her funeral. She took care of everything.”) Family caregivers acknowledged the accumulating burden of losses that precede death, and they shared the grief of multiple losses. (“I’ve lost 2 people—my wife and my son, in less than a year.”) Survivors reflected on how their loved one constructed their legacy and continued to value it as a connection to the deceased.
Discussion
The intervention informed by these focus groups was intended to address the needs of patients and their families during the last 2 to 3 years of life with serious illness. During this time, when patients continue to receive aggressive medical support from their regular care teams and hospice is a future consideration, the interviews provided an opportunity to explore palliative needs long before end of life. These needs were most clearly identified in the proposed family/caregiver domain.
In shear breadth, the NCP social aspects of care domain is expansive, accounting for 37% of all domain coding in this study. The social domain touches many facets of personhood including caregiving, social networks, family, work life, and financial–legal concerns. Using the proposed domain set, strong empirical support was found for identifying a distinct family/caregiver domain. Caregivers, in this study, described well-documented challenges including gender roles, managing difficult behaviors, caregiving at a distance, the time and physical burdens of caregiving, performing complex medical tasks, helplessness in the face suffering, feelings of depression, and disregard for self-care. 27 –41 Counterbalancing these, they described rewards of a close relationship, personal growth, a sense of mastery, and self-esteem. 35,39,42,43
For most caregivers, these experiences unfolded within a family system. Caregivers described family support, adaptability, and self-efficacy, all of which improve clinical outcomes or caregiver health in serious illness. 44 –48 Families transferred values, for example, by engaging in caregiving as a cherished transgenerational activity. 49,50
In addition to its substantive presence in serious illness, the family/caregiver domain is important to consider because it highlights tractable barriers to optimal care. Caregivers in this and other studies have described feeling invisible or ignored by the health-care system; this can even arise with home-based services when providers focus on the patient to the perceived exclusion of family. 51,52 When caregivers feel their needs for practical or emotional support go unmet, they experience distress that is not related to objective measures of caregiver burden. 53 It is not surprising therefore that caregivers request practical support, active listening, better 2-way communication, and a more navigable, less complex health system. 54,55
Conjoined financial and legal concerns expressed in the interviews led to proposing a financial/legal domain. During the course of serious illness, families provide most of the support to loved ones, while medical costs headline the story of personal bankruptcy. 56,57 Perceived or real financial constraints can lead to social isolation for caregivers, when they forego needed social services. 58
The third of the proposed domains, legacy/bereavement, identified issues spanning individual lives and extending across generations. Although legacy is typically seen as work of the patient, and bereavement as work of the survivor, the quotes reveal some interdependence. Patients constructed their legacy as both patient and family began grieving cumulative losses. Caregiving itself was passed down as a legacy of example. 49
There are limitations to this study. It is a secondary analysis of interviews conducted to gain insights for a new clinical model. General questions related to caregiving were asked, for example, “What are your joys and your challenges in being a caregiver?,” but there were no specific questions on legal matters, financial concerns, legacy, or bereavement. Proposals for these smaller domains should be viewed as preliminary until further research can be done. Although the clinical intervention broadly defines family from the patient’s perspective, the sample of patients and families interviewed came from traditional family settings.
Conclusions
This study was used to explore the applicability of an expanded domain set to the serious illness experiences of individuals. Results of this study highlight the particular importance of a family/caregiver domain. Families reflected on their roles as care managers and importantly also on their own family and personal transformations. Two additional proposed domains—financial/legal and legacy/bereavement—reflect experiential groupings of concerns around preservation of assets and life transitions, respectively. Both the applicability of these proposed domains and a parallel analysis of the whole person perspective of families’ experiences deserve further study.
Expanding the NCP social aspects of care domain by adding the newly described family/caregiver domain more fully describes the day-to-day experiences of patients and families. This understanding supports efforts to deliver whole person care by focusing on key facets of the broad social/family landscape. Honoring the central role of caregivers will set the stage for effective partnerships with patients and families in the consuming work of living with serious illness.
Footnotes
Appendix A
Acknowledgments
The authors wish to thank William Spinelli, MD, for conducting the interviews, and Heather Britt, PhD, for helping articulate the expanded domains and providing manuscript review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a grant from the Robina Foundation.