
Abstract
Background:
Informal, unpaid caregivers shoulder much of the care burden for individuals with serious illness. As part of a project to create an innovative model of supportive care for serious illness, a series of user interviews were conducted, forming the basis for this article.
Objective:
To understand both individual and interpersonal aspects of caregiving for serious illness.
Methods:
Twelve semistructured group interviews were conducted with patients, families, and professionals as part of a larger study of late-life serious illness. Transcript data were analyzed with descriptive coding, and then coded material was analyzed to elicit major themes and subthemes.
Results:
A total of 73 individuals participated in group interview sessions. Using descriptive coding, quotes were assigned to first-order codes of rewards, challenges, and a category of learnings and adaptations. Subthemes of reward included gratitude, a sense of accomplishment or mastery, and closeness in personal relationships. The most oft-cited challenges included emotional and physical stresses of caregiving and feeling unprepared or unsupported in caregiving. Reflecting on their experiences, caregivers cited new ways in which they had learned to be creative, to show assertiveness and advocacy, and to create personal balance in a demanding situation.
Conclusions:
The experience of caregiving is a life-altering journey as individuals rise to challenges and reflect on the rewards. Caregivers described intensive caregiving, often without acknowledgment or understanding of their role from the health-care system. This invisibility created its own iatrogenic caregiving challenge. The identified themes suggest avenues of meaningful caregiver support that bear further exploration.
Introduction
Informal, unpaid care for individuals with serious, chronic illness represents an escalating, seldom acknowledged investment of human resources. In 2011, 14.7 million unpaid caregivers served 7.7 million individuals living in the community without collocated services. 1 A 2015 study identified 34.2 million individuals providing care to older adults in all settings. 2 The American Time Use Survey in 2012 yielded opportunity costs of US$221 to US$642 billion annually, using the minimum wage and home health aide wages as bookends for estimates of work value. 3
Relatives are the main source of care for the seriously ill. The Institute of Medicine’s report on caregiving in 2015 found that individuals providing care to older adults had been in the role for an average of 4 years and were spending over 20 hours per week in caregiving. 2 A random urban survey identified 380 households where informal caregiving was present, extended over more than a year, and lacked formal caregiver help. 4 Until recently, caregivers have received little direct support, either for their caregiving role or for their own needs. Lack of readiness on the part of caregivers to provide services is frequently cited as a contributor to caregiver burden. 5 –7 Only 1 in 6 caregivers report being asked what they needed to take care of themselves. 2 The American cultural norm of self-reliance perpetuates the obligation of families to provide care, abetted by social policy decisions that limit public expenditure on the aging. 8
Research related to caregiving has evolved from negative assumptions toward caregiving to more balance in understanding the caregiving experience. 9 Assessment tools, such as the Caregiver Burden Index (CBI), were designed based on items previously identified as problematic for caregivers. 10 Similar tools include the Parkinson Disease Caregiver Burden assessment and the American Medical Association Caregiver Self-Assessment Questionnaire, which contains only a single positively framed item. 11,12
Studies of caregiver morbidity and mortality reinforce negative perceptions of caregiving. 13,14 Reanalysis of these data emphasizes that caregiving may actually confer a survival advantage to the majority of caregivers not experiencing high stress. 15 A better understanding of these positive factors is emerging. One such example is embedded in the Caregiver Well-Being Scale that assesses how caregivers’ experiences across multiple domains of personhood provide insight into these beneficial factors of caregiving. 16 –18 Others have described positive aspects of caregiving (PAC). 19 –21 However, factor analysis of positive items introduced into the Caregiver Strain Index suggested that the positive items relate to an entirely different dimension of experience. 22,23 Early conflation of concepts such as caregiver gain, caregiver well-being, and caregiver reward has given way to an understanding that the positive caregiving experience is descriptively complex. Qualitative approaches, such as the one presented here, have been recommended as means for identifying positive measures of caregiving. 9
The current study aims to shed light on the serious illness experiences described by caregivers, assuming neither burden nor reward. The interviews were part of a user-centered approach to creating a supportive care intervention for serious chronic illness. 24 The semistructured group interview sessions were designed to explore the experiences of caregiving; for that reason, they were relatively open ended. This article will illuminate the caregiver contexts that shape critical experiences in caregivers’ lives.
Methods
Participants and Procedures
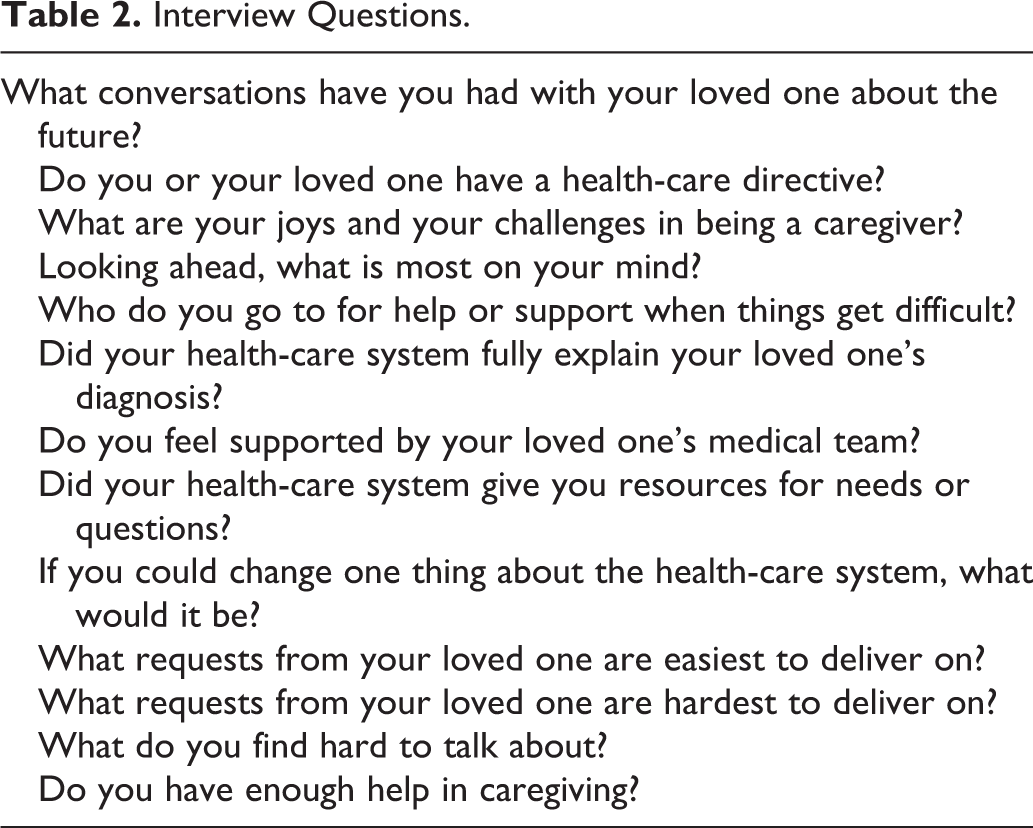
Twelve semistructured group interviews were conducted with groups of 2 to 8 participants between March 3 and June 30, 2012. Participants with personal experience dealing with chronic medical conditions as patients, caregivers, or both were recruited from senior living communities, faith communities, provider organizations, and disease advocacy associations. The participants are characterized in Table 1. Of 73 individuals, 23 were patients, 29 were family, and 19 were health professionals. Ages of the participants were not elicited, but almost all were spouses or adult children of older patients. Of the professionals interviewed, 4 were palliative-trained clinicians: 2 physicians, 1 social worker, and 1 chaplain. Diagnoses relevant to the patients and caregivers were dementia (28), cancer (16), chronic respiratory disease (11), heart failure (5), and other (3). Participants received no compensation. Interview groups were facilitated by a family physician using a semistructured discussion guide (see Table 2) and lasted between 90 and 120 minutes. Eight of the professionals related personal experiences caring for loved ones; these quotes were included in the data set.
Interview Participants.
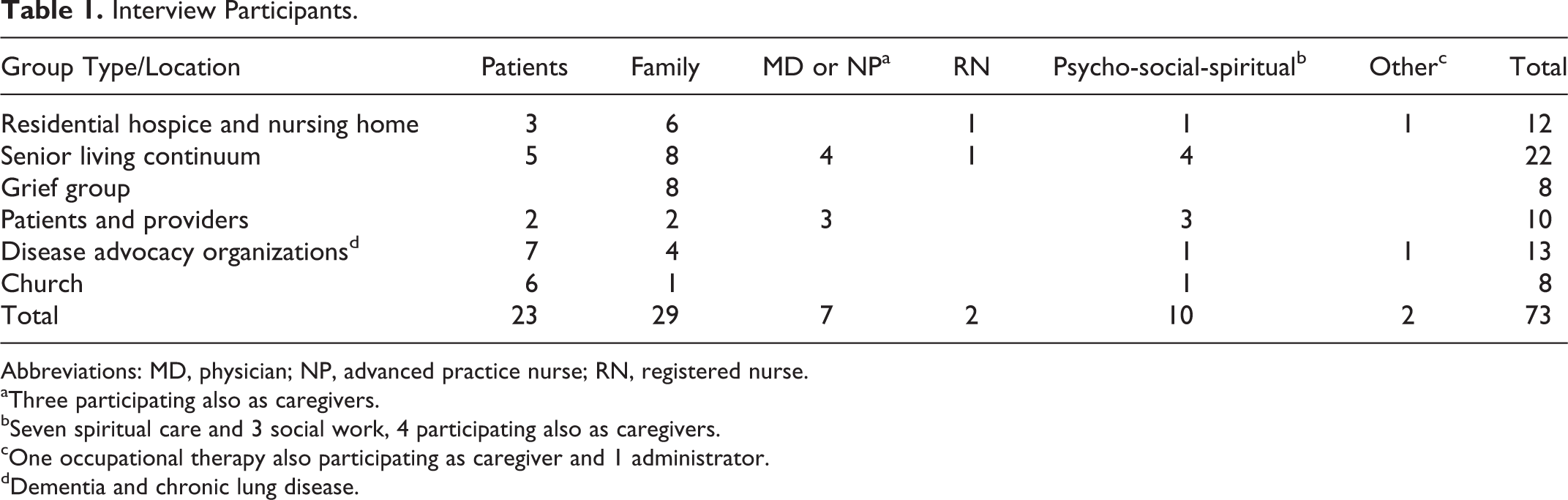
Abbreviations: MD, physician; NP, advanced practice nurse; RN, registered nurse.
aThree participating also as caregivers.
bSeven spiritual care and 3 social work, 4 participating also as caregivers.
cOne occupational therapy also participating as caregiver and 1 administrator.
dDementia and chronic lung disease.
Interview Questions.
A public television crew filmed the sessions and edited recordings to remove unrelated content. Dialogue from the videos was transcribed for textual data. Institutional review board approval was obtained for use of the transcripts.
Analysis
Qualitative Method
Two researchers (E.W.A. and K.M.W.) conducted first-order coding on the data from all 12 semistructured sessions. In reviewing the transcripts, an inductive approach was employed in determining codes and generating the codebook to capture major themes. The question set was not used in generating codes. Both researchers then analyzed 20% of transcript contents to generate subcodes for second-pass analysis.
Completion of second-pass coding was independently performed by assigning textual content to the major codes and subcodes; coding was then reconciled between investigators. The coding relationship of interview items to nodes and subnodes was one-to-many, reflecting the multiple issues represented in individual comments. 25 All transcripts were individually coded by 2 researchers (E.W.A. and K.M.W.) using the method described above. Once final coding was achieved, successive passes through the coded passages and text queries were used to establish the major themes. NVivo software was used to manage data analysis. 26 Deidentified transcripts and coding assignments are available from the authors.
Results
The 12 interviews yielded 474 unique quotes of varying length, relating to experiences arising in the course of serious illness. These quotes yielded 640 codes, averaging 1.35 coding assignments per quote. Several major themes emerged from the first-pass coding, as shown in Table 3. In response to interview questions, such as “What are your joys and your challenges in being a caregiver?,” participants reported both rewards and challenges. Caregivers also commented on how they had learned to deal with challenges; the question set did not prompt responses for this theme. These 3 themes of rewards, challenges, and learnings were further analyzed for subthemes.
Major Themes From Family/Caregiver Interviews.
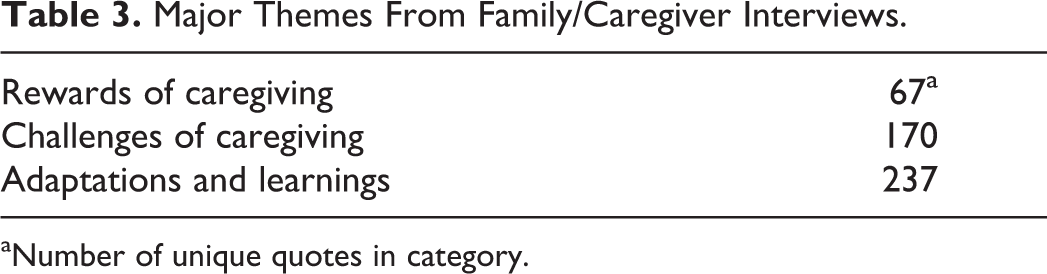
aNumber of unique quotes in category.
Rewards of Caregiving
Rewards reported by the interview participants followed 3 major subthemes: gratitude, a sense of accomplishment or self-advancement, and rewarding relationships (see Table 4). These accounted for 49%, 28%, and 23% of the 76 quotes, respectively.
Subthemes in Rewards of Caregiving.
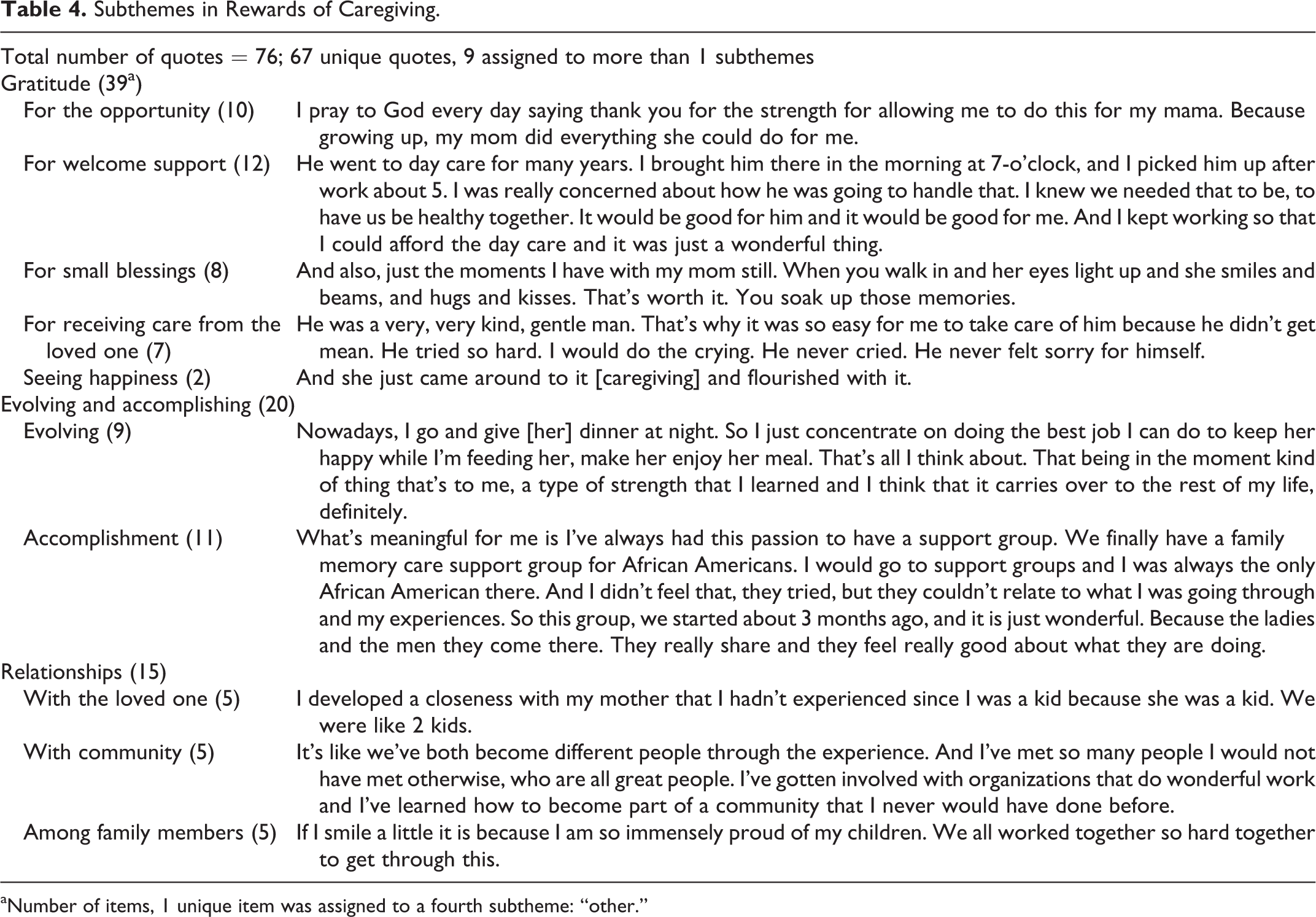
aNumber of items, 1 unique item was assigned to a fourth subtheme: “other.”
Gratitude, often expressed as “gift” or “blessing,” was applied to expressions of emotion that came from receiving unasked-for gifts, as opposed to the rewards of actively acquiring knowledge or skill. It often came from closeness in relationships and more generally for the opportunity to do caregiving. Children reflected on the parental love they had received in life and were now able to reciprocate. Even transient episodes could elicit a profound sense of gratitude, such as moments in dementia care when a parent’s eyes lit up with recognition or pleasure. Participants expressed gratitude for support from family members, the health-care system, friends, and peers. This could take the form of day care, an accessible electronic health record, or compassionate providers. Friends encouraged caregivers to pursue self-care. Caregivers also spoke of their debt of gratitude when the ill person took the initiative to create a positive caring experience, whether clarifying wishes or remaining cheerful in the face of decline.
The second major rewards subtheme reflected personal development or satisfaction with accomplishing difficult tasks. Several participants mentioned how they had learned to appreciate life in the moment or to draw boundaries between work and home life. The sense of accomplishment could not only relate to acquiring skills but also relate to others in new ways, for example, holding difficult conversations or establishing a support group.
Rewarding relationships constituted the third major subtheme. Participants reported that the time with the ill person deepened their relationship, increased appreciation for the role of family members, and enhanced nonfamily relationships, including peer groups and volunteer opportunities.
Challenges of Caregiving
These 170 unique items were coded a total of 228 times to the subthemes of physical and emotional stress (39%), feeling unprepared or unsupported (30%), transitions (11%), cognitive failure (10%), and honoring the loved one’s wishes (9%; Table 5).
Subthemes in Challenges of Caregiving.
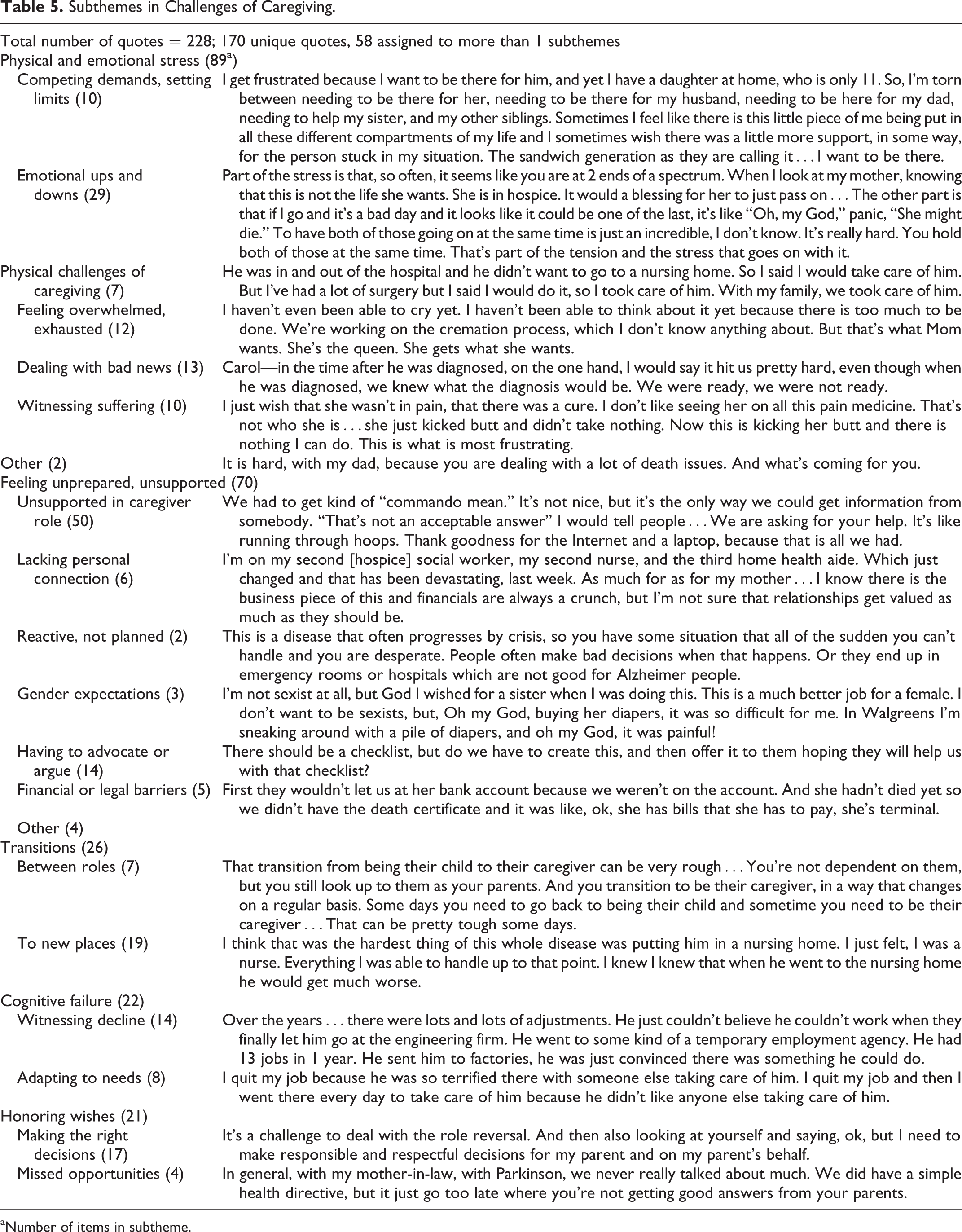
aNumber of items in subtheme.
The majority of challenges of caregiving quotes related to emotional distress. Some caregivers identified themselves as the “sandwich generation,” worrying more about shortchanging their dependents than attending to their own physical and emotional needs. Additional sources of emotional stress included new interpersonal experiences: receiving bad news and witnessing the suffering of loved ones.
Within the subtheme “feeling unprepared, unsupported,” participants articulated a broad set of challenges. Flares of chronic illness caught families unaware, initiating a chain of reactive events without a trusted health-care relationship to call upon. Caregivers described aggressively advocating for assessment and treatment in the hospital setting. Perceived flaws in the system, such as lack of a checklist, seemed to go unattended. Finally, several participants noted the legal and financial challenges of comanaging the affairs of a loved one with progressive physical/cognitive impairment.
Transitions were usually described by participants as stressful. Both parents and their caregiving children felt the strangeness of changing parent−child roles. Patients struggled to adapt to new living environments, and their families often described the experience as difficult or even anguishing. At the same time, family caregivers struggled to cede day-to-day caregiving to facility staff.
Of the 50 patients and caregivers who provided quotes, 28 involved dementia care. Several participants described the emotional toll in witnessing a loved one’s decline. Caregivers reported changing their behaviors, their choice of words, and even their work lives to accommodate a loved one’s life with dementia.
About 13% of the unique comments regarding challenges pertained to honoring wishes. This often occurred in the context of waning cognition. As expected, families labored to allow their loved ones to express wishes, while working out complex medical and life decisions based on those wishes.
Learning and Adaptations
Quotes falling under the learning and adaptations subtheme included statements of understanding and stories of personal change arising from the experience of caregiving. Although rewards and challenges described the context of the care experience, learnings and adaptations emerged from experiencing the events, and they helped to shape care going forward (Table 6).
Subthemes of Learnings and Adaptations.
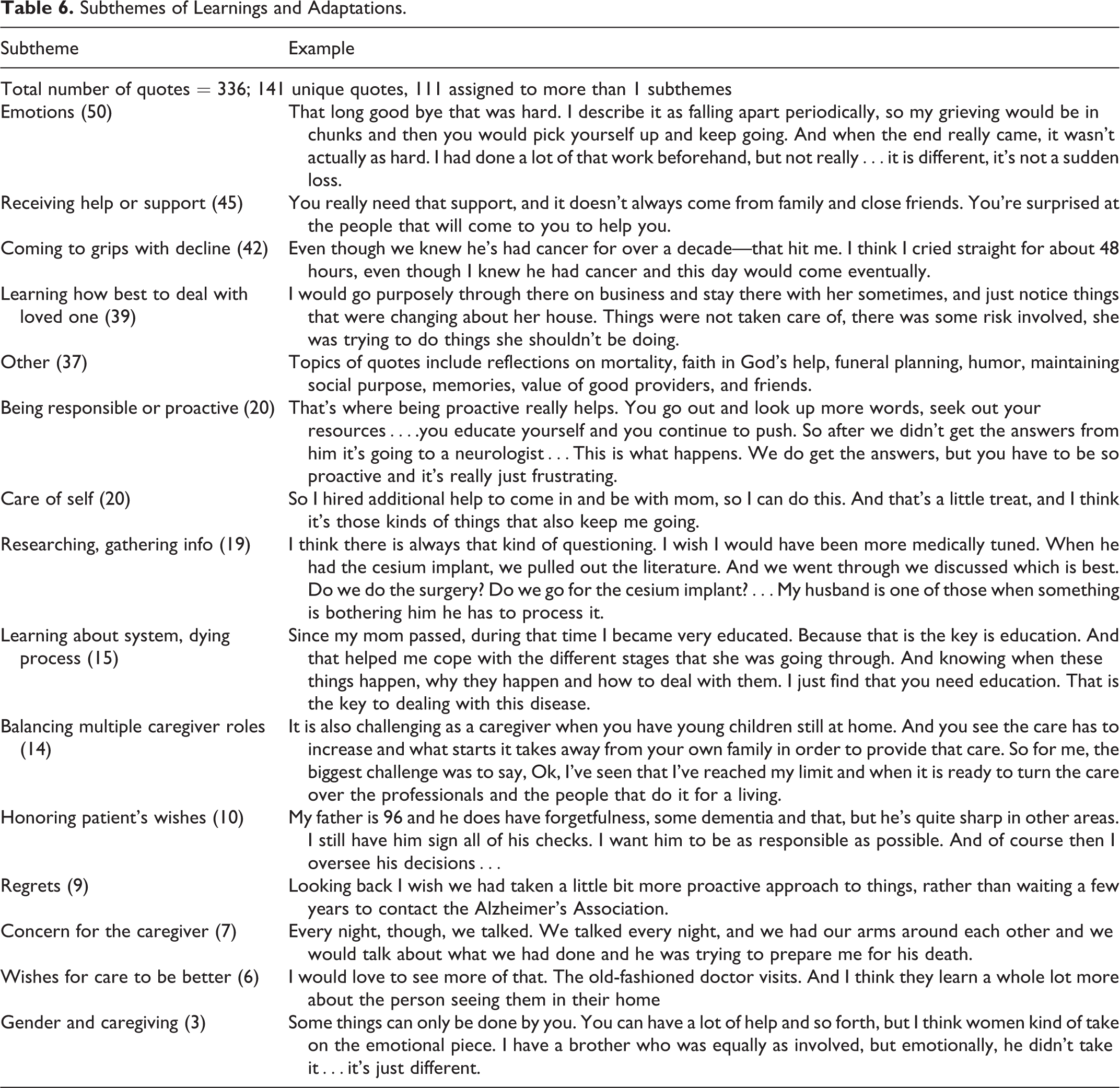
Reflections on emotional experiences were common. Grief and loss include witnessing cognitive decline, missing opportunities for closeness, feeling surprised when death finally comes, and recalling the loved one with deep sadness. Negative emotions arose from frustration and powerlessness in the face of decline. Nineteen of the 50 quotes regarding individual emotions reflected positive learnings, arising from supportive friends, organizations, compassionate providers, and faith in the divine.
Caregivers learned to reach out to others for support. This was often task specific, such as help with completing an advance directive. Individuals commented positively on stable, personal connections with care providers, peers, and friends. “Sandwich generation” caregivers learned to balance competing generational demands.
Caregivers looked back on disease progression, recalling a static/dynamic tension. (“I’ve noticed that where [we] have hope that things are very normal again…all of a sudden it starts to degrade again.”) Families were challenged at both ends of this trajectory spectrum.
Caregivers acquired newfound skills required for their role: coping with decline, becoming proactive, and gathering information. Most reflections on being proactive and many regarding gathering information were described in scenarios of confrontation, requiring that individuals or families demand information or action, making them feel “commando-mean.” These comments were tempered by 2 aspects of the care experience: positive relationships with informative, proactive support systems such as a hospice team and the need to refrain from overweening intervention that would compromise the loved one’s right to choose.
In reflecting deeply on their experiences, caregivers provided a window into their personal transformations, embodied in the comment, “It has changed my life.” The relationship with oneself evolved, developing inward focus characterized by self-care, self-compassion, setting limits, seeking rewarding work outside caregiving, becoming a model for one’s children, or sharing oneself in a support group setting.
Discussion
From a set of semistructured group interviews, over 400 quotes were analyzed in an attempt to understand the caregiving experience. Caregivers reported rewards and challenges, and they described the learnings gained from their labors. Under each of these broad categories, opportunities present themselves for future efforts to aid caregivers in meaningful ways.
Three major themes encompassed rewards of caregiving. Gratitude included the privilege of providing care and appreciation for helpfulness of the person in care. 27 Caregivers appreciated their acquired sense of accomplishment or mastery. Mastery and the related concepts of self-esteem and preparedness are often juxtaposed to feelings of being overwhelmed in the interplay of rewards and challenges. 28 –30 The third subtheme—closeness in the relationship—has been cited as contributing to rewards and, when absent, to stress. 20,31 –34 This dynamic affects generations differentially: spouses experience challenges in the relationship with the loved one, while children tend to gain rewards. 27,29,30,32,35 In evaluating factors contributing to PAC, a regression model for PAC increased the ability to explain variability in the Zarit CBI when self-efficacy was included, while closeness of the relationship with the loved one correlated with reduced caregiver depression. 34,36,37
Participants at times used language suggesting that their positive experiences were profound, for example, “This is an incredible thing; it’s just a real gift.” These comments reflect the importance of positive psychological states in coping, even during times of prolonged or severe stress. 38,39 Rewarding emotions are posited as fundamental to the human ability to flourish, by providing windows of opportunity to broaden one’s responses and integrate adaptive behavior. 40 Recognizing and fostering such emotions is a testable aim of a comprehensive model of supportive care.
The most commonly reported theme of caregiving challenges was stress to the caregiver, more often emotional than physical. Previously cited factors of time constraints, inability to care for self, lack of control, lack of choice in the caregiving role, guilt in placing the loved one outside the home, gender-specific issues, and employment were all reflected in the comments. 28,30,32,33,41 –49 So too was the challenge attendant to witnessing their loved one’s suffering and decline. 50 –53 Although some sources of this stress may be inevitable in serious illness, such as witnessing the loved one’s suffering, others may be amenable to support, including respite or the emotional support of peers.
The other major subtheme of caregiving challenges—feeling unprepared or unsupported in the role—constitutes a nosology of caregiver strain arising largely from the structural priorities of the medical/social support system. Participants felt ill equipped for disease progression, medical crises at home, or encounters with an unresponsive delivery system. This gulf separating caregivers from the resources and expertise of the health-care system is a well-documented, unfilled gap. 43,54 –57 Parallel comments in this study relate a sense of not being seen by providers, despite the caregiver’s expertise in the person and their disease. 58
In the course of rising to challenges and appreciating rewards, caregivers were changed. Their comments of learning and adaptation give a window into the nature of this experience. At a personal level, they learned the value of self-care. They were able to forge meaning from a complex emotional experience; examples of this internal development included valuing personal relationships at deeper levels or understanding their own regrets. Outwardly, they tackled the work of caring with newfound personal competencies, sometimes extending these learnings by volunteering with other individuals and organizations. This combination of personal growth and the positive psychological effects of rewarding experiences referenced earlier contribute to a new perspective on care—a new internal frame. The significance of this internal framing has been demonstrated in caregivers. Individuals who envision becoming caregivers in the future posit more future rewards than those who do not see themselves becoming caregivers, suggesting that expectations engender subsequent framing. The importance of internal perspective is reflected in the observation that caregiver stress relates more to the sensed need for physical or emotional support than it does to objective measures of caregiver burden. 59,60 In this study, some participants articulated a broader vision of caregiving as a newly appreciated and ongoing purpose of the family, a reframing that could affect the work of future generations.
Research into the needs of caregivers has been slow to yield useful supportive strategies. Early reviews of interventions for caregivers noted both the paucity of caregiver outcomes and the systematic or circumstantial exclusion of caregiver input found in study designs. 61,62 More recently, reviewers concluded that while the number and quality of interventions have increased, better understanding of strategies that provide practical support for caregivers is needed. 63,64 Current psychoeducational and relational interventions provide modest but durable benefit and should be further developed. 65 Key elements of future research strategy include a clear definition of needs and measurement of outcomes, preventive rather than reactive support, attention to meaning-making and family relationships, and rapid testing of possible strategies. 66,67 The present study informs this process by directing the focus of measurement and support to specific areas of caregiver experience. These areas include the importance of rewarding experiences to caregivers, the gulf of unmet medical and social support for managing serious illness at home over months and years, and the conceptual substitution of “the caregiving family system” in place of the limiting descriptor “caregiver.”
Conclusions
When asked about caregiving for a loved one with serious illness, individuals describe a life-altering journey involving stress, self-reflection, learning, and reward. Their experiences of intensive caregiving often proceed without acknowledgment or understanding of their role from the formal health-care system. The desire to be supported at every step of the way contrasts with comments about feeling unprepared and unsupported. Despite these negative experiences, caregivers express true gratitude for their roles, for discovering positive attributes such as creativity, and for a sense of accomplishment in themselves. Fostering these attributes could promote the adaptive behaviors likely to allow a person to remain in care at home longer. Understanding the interplay of rewards, challenges, and personal development is a necessary step in creating the adaptive and programmatic solutions that will better support the caregiving family system.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a grant from the Robina Foundation.