
Abstract
Background:
Patients with serious chronic illness are at a greater risk of depersonalized, overmedicalized care as they move into later life. Existing intervention research on person-focused care for persons in this transitional period is limited.
Objective:
To test the effects of LifeCourse, a team-based, whole-person intervention emphasizing listening to and knowing patients, on patient experience at 6 months.
Design:
This is a quasi-experimental study with patients allocated to LifeCourse and comparison groups based on 2 geographic locations. Robust change-score regression models adjusted for baseline differences and confounding.
Setting/Participants:
Patients (113 intervention, 99 comparison in analyses) were individuals with heart failure or other serious chronic illness, cancer, or dementia who had visits to hospitals at a large multipractice health system in the United States Midwest.
Measurements:
Primary outcome was 6-month change in patient experience measured via a novel, validated 21-item patient experience tool developed specifically for this intervention. Covariates included demographics, comorbidity score, and primary diagnosis.
Results:
At 6 months, LifeCourse was associated with a moderate improvement in overall patient experience versus usual care. Individual domain subscales for care team, communication, and patient goals were not individually significant but trended positively in the direction of effect.
Conclusion:
Person-focused, team-based interventions can improve patient experience with care at a stage fraught with overmedicalization and many care needs. Improvement in patient experience in LifeCourse represents the sum effect of small improvements across different domains/aspects of care such as relationships with and work by the care team.
Keywords
Introduction
Patients with serious chronic illness face multiple challenges as their conditions worsen later in life. Preventing or addressing symptoms and complications requires ongoing, at least some, disease management via treatment and self-management regimens, even in later years. 1 –4 However, moving toward later stages of serious conditions such as heart failure, cancer, or dementia also may entail transitions to palliative care in or out of hospice, end-of-life care, and considering the social psychological impact of impending mortality among patients, their caregivers, and loved ones. 5 –8
Although patients with serious illness have many needs in later life, they typically do not receive whole-person care of sufficient quality to meet those needs. 7 –13 Instead, individuals may be simply overtreated medically, 14 –16 resulting in a depersonalized, fragmented experience. Patient experience, part of the health care’s triple aim increasingly tied to value-based payment, 17,18 is perhaps most important among patients with serious illness who have frequent contact with health care.
The need for better care for serious conditions, oriented toward the whole person, has not gone unnoticed. However, studies of whole-person approaches to care in later life have been mainly limited to circumscribed palliative or hospice care at the end of life or for single conditions (eg, cancer). 19 –24 Much literature on understanding and treating patients with serious illness from a whole-person standpoint has been exploratory, with limited or no follow-up. 23 –26 A smaller number of controlled studies testing multicomponent interventions suggest promising results for quality indicators, family-rated care after death, or quality of life. 27 –29 They have generally not focused on improving patient experience.
Meanwhile, approaches to understanding patient experience primarily rely on the Consumer Assessment of Health Plans and Services 30,31 or other encounter or setting-specific (eg, hospice or hospital) measures. This results in findings that do not examine the long-term relationships with a care team. Likewise, the literature on team-based or integrated care generally 32,33 does not help understand the specific needs of patients in later life, when managing conditions gives way to end-of-life and palliative care.
There is a need for interventions for whole-person care for serious chronic illness in late life and rigorous evaluations to establish their effects on care. This article presents results of a quasi-experiment studying the effect of LifeCourse, a whole-person, longitudinal approach to care in late life, on patient experience versus usual care. Our contributions include length of follow-up, a dedicated experience measure, and a focus on patients’ needs upstream starting with long-term chronic care.
Methods
This quasi-experimental study assesses a model of whole-person care for patients with serious chronic illness. The study was approved by Quorum institutional review board. Supplemental material (deidentified data and participant questionnaires) are available from the authors on reasonable request.
Intervention
LifeCourse is a team-based intervention designed to improve the lives and care of patients and caregivers. Its design was informed by national expert and local patient advisory panels, patient stories, and input by local experts in team-based care, aging, and chronic condition management. Designers also used key pieces from National Consensus Project (NCP) Clinical Practice Guidelines for Quality Palliative Care, 34 which organize practices around domains of palliative care. Specifically, LifeCourse domains include physical, psychological, social, family/caregiver, cultural, spiritual, legacy/bereavement, end of life, ethical, and financial/legal.
A key piece of the whole-person approach is the involvement of care guides, who are lay health-care workers acting in support, relationship, and navigation roles. Care teams consist of these care guides, with support from clinicians, including a registered nurse, social worker, marriage and family therapist, chaplain, and pharmacist. LifeCourse extends care by using care guides as patients’ and caregivers’ primary contact on the care team. LifeCourse designers, therefore, adapted select practices from the NCP guidelines for palliative care as appropriate for delivery by lay health-care workers. The manual and training sessions for new LifeCourse care guides include training modules on these adapted domains and practices to orient care guides to the LifeCourse model of whole-person care.
In practice, care guides have monthly, hour-long visits with patients and friends/family. Visits can be telephonic but are typically in-person at patients’ homes. Care guides aim to identify patients’ whole-person needs and then provide practical and emotional support. This whole-person focus arises via structured conversations designed to help patients identify and articulate medical and nonmedical concerns. In these conversations, care guides follow a discussion guide that includes question sets and assessments align with the whole-person domains in the NCP guidelines
34
noted above. This helps surface medical and nonmedical concerns to support the whole person. Care guides then either support patients in contacting their medical provider team or linking to community resources that meet needs such as food scarcity or transportation. Care guides also help navigate visits to hospitals and clinics and help empower patients by articulating or updating their preferences and goals. Finally, care guides also document the patient’s story in the medical record, including notes on whole-person domains. The overall goal is to orient care toward the patient as a whole person, provide patients with key competencies (eg, advanced care planning), and engage patients in decision-making. An example of transformation to a whole-person model of care is as follows: A LifeCourse patient awaiting a kidney transplant received notification that she was no longer a transplant candidate. Prior to this, the patient’s care guide had accompanied her to the kidney transplant clinic for a social evaluation. After removal from the transplant list, the care guide supported the patient as she grieved the loss of a life without dialysis, discussed her concerns with a LifeCourse clinical manager, assisted with making lifestyle changes, and reviewed the patient’s support system to identify needs.
Eligibility and Recruitment
Patients were recruited at 8 hospitals and clinics in Minneapolis and St Paul, Minnesota, associated with a large, private not-for-profit health system. Eligible patients had at least one of the following: advanced cancer, dementia or Parkinson disease, heart failure, chronic obstructive pulmonary disease, chronic kidney or end-stage renal disease, cardiovascular disease, liver disease, and diabetes. Patients were identified using a medical record–based algorithm, with a further eligibility check by an experienced registered nurse. Nondementia patients had to have a combined Charlson-Elixhauser score 35 greater than 3. We used 2 further inclusion criteria. First, patients had to have 6 possible months of observation (some patients were not yet 6 months postbaseline). Second, individuals had to have received the final outcome survey tool. Initial patients (who received a noncompatible pilot survey) and those requiring proxies (no proxy tool was available) were not eligible for this analysis (despite receiving the intervention).
Recruitment occurred between October 2012 and June 2015; all eligible patients were approached in person and offered participation in the study (convenience sample). Patients provided written informed consent.
Allocation
Patients were allocated to treatment (“LifeCourse”) and usual care (“comparison”) based on the geographic location of intake site. Patients in Minneapolis were allocated to LifeCourse, whereas those in St Paul were allocated to comparison. Individuals initially allocated to LifeCourse who refused were asked to participate as comparisons to maximize the sample size.
Measures and Data Collection
The dependent variable was the LifeCourse experience tool, 36 a patient-reported survey measure administered quarterly in person beginning at enrollment. This tool was developed specifically for evaluating the LifeCourse intervention. Other experience tools were deemed not suitable for tracking patients with serious chronic illness over time. As such, based on the input from professional expert and patient panels, we adapted or created items based on other experience tools geared toward patient experience in late life or serious illness. 37 –39 We revised the tool during prepilot and pilot testing, including cognitive debriefing and exploratory and confirmatory factor analyses.
The LifeCourse experience tool consisted of 21 items asking about aspects of care regarding interpersonal issues, access, and personal goals and biography. At baseline, α reliability was 0.915. Although designed as a single scale, the tool did encompass 3 domains: Care team (13 items, α reliability = 0.917) pertained to person centeredness in the care team’s work (example item: “The care team kept my wishes at the center of my care”); Communication (5 items; α reliability = 0.827) pertained to communication and information/knowledge sharing (example item: “I had unanswered questions about how my illness affected my everyday life”); and Goals (3 items; α reliability = 0.773) pertained to having recognized, personalized goals (example item: “I have a good understanding of my goals of care”). Most items used 4-point, frequency-based responses (“never” to “always”), but Goals used agreement-based responses (“strongly disagree” to “strongly agree”). Individuals had to have answered at least 80% of items to have a valid response recorded (missing values were prorated based on nonmissing items). Items were summed for total and domain scores.
Other measures, collected from patient records, included age (<65, 65-74, 75-84, 85+), sex, race/ethnicity (white vs other), primary diagnosis (heart failure and other chronic conditions, cancer, dementia), being married (vs not), education (high school or less, some college/bachelor’s, graduate/professional school), and comorbidity index. 35
Analysis
Due to nonrandom allocation, we used nonergodic change-score regression to control for baseline differences while assessing the effect of LifeCourse on change in patient experience. Change scores (Time2 − Time1) in summary and domain-specific patient experience were regressed on all independent variables. These included all covariates, as well as baseline experience to adjust for ceiling/floor effects. We used robust regression to adjust for outlier effects.
To assess possible attrition bias, we attempted using Heckman regression to treat attrition as a selection bias process. However, we found nonsignificant or only marginally significant tests for selection in these models. Moreover, these models did not change the direction or size of treatment effects. Therefore, for parsimony, we simply present the robust regression results here.
Results
In total, 556 eligible patients (351 intervention and 205 comparison) were identified. After excluding those inactivated due to death or other reasons and those with missing experience measures or covariates (Figure 1), final valid/nonmissing sample size was 212 (113 intervention and 99 comparison).
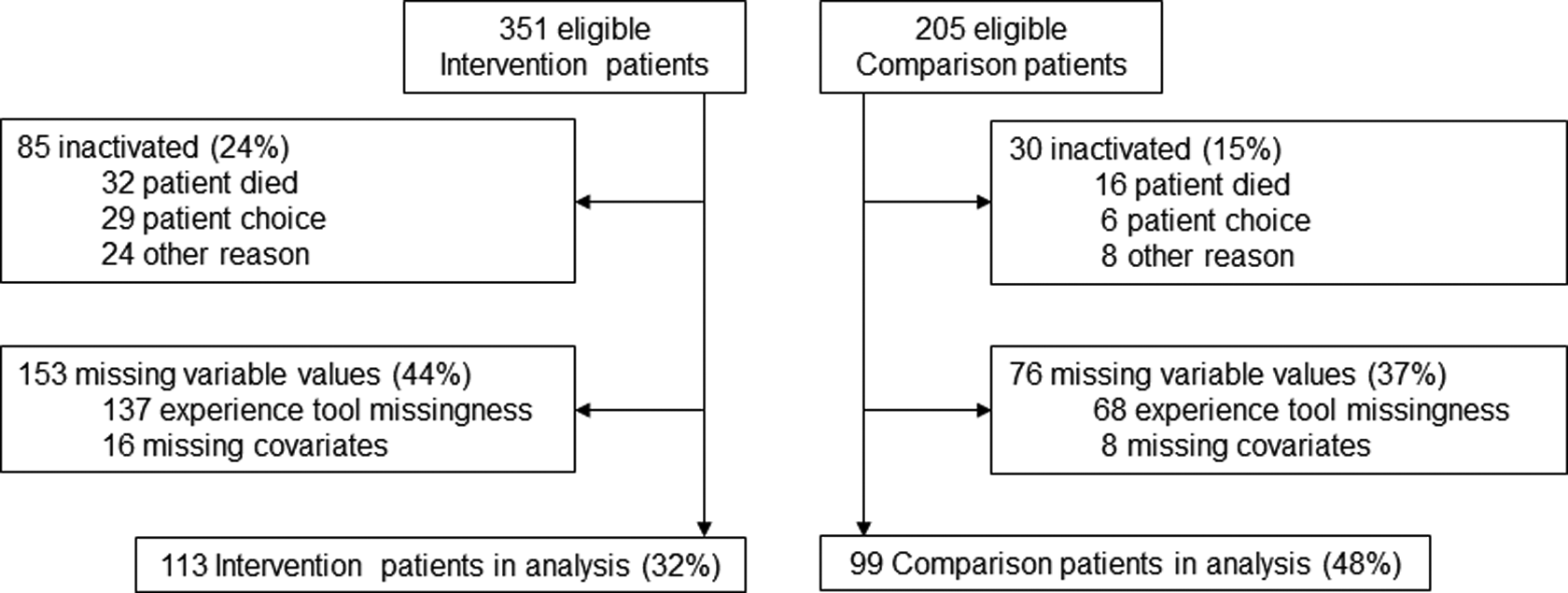
Initial eligible count, exclusions, and final analytic sample for a practice-based evaluation of the LifeCourse intervention and its impact on patient experience.
Group characteristics were similar in most cases (Table 1). However, compared to usual care, intervention patients were more educated (P = .007) and more likely to have dementia as primary diagnosis (P < .011). Sensitivity analyses (not shown) removing individuals with dementia as primary diagnosis from the analysis did not change the overall effect size or significance.
Sample Characteristics.
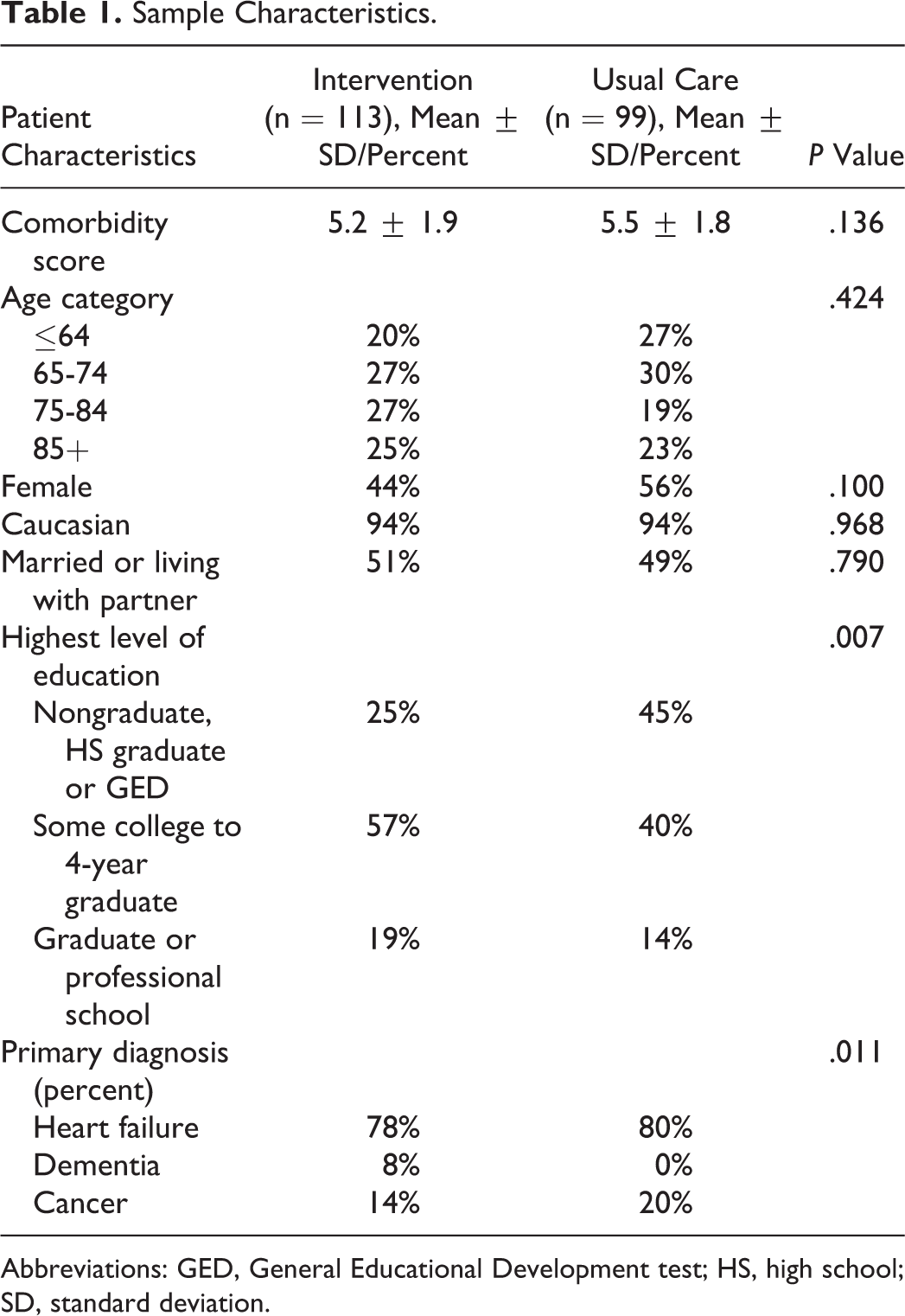
Abbreviations: GED, General Educational Development test; HS, high school; SD, standard deviation.
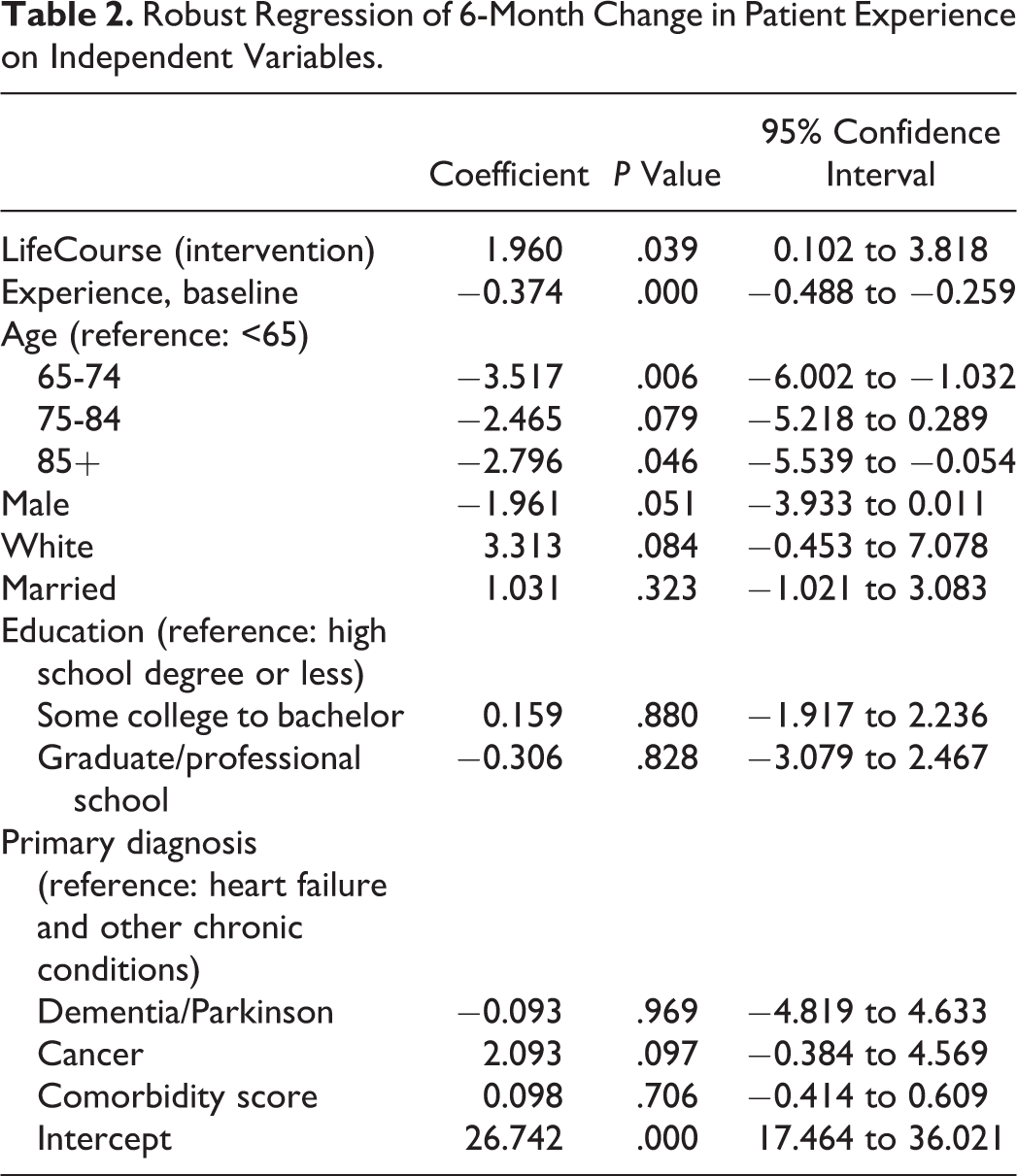
At 6 months, controlling for covariates and baseline experience (Table 2), LifeCourse had a positive change of 1.96 points on the experience scale versus usual care (95% confidence interval: 0.102-3.818, P = .039). Baseline experience had a negative effect on the change score; this is common in such models due to regression to the mean. Patients who were older, nonwhite, and more educated had worse change in experience.
Robust Regression of 6-Month Change in Patient Experience on Independent Variables.
Domain-specific findings (Figure 2) showed all effects trending positively in direction (indicating better experience for LifeCourse vs comparison) but not significantly (P < .05).
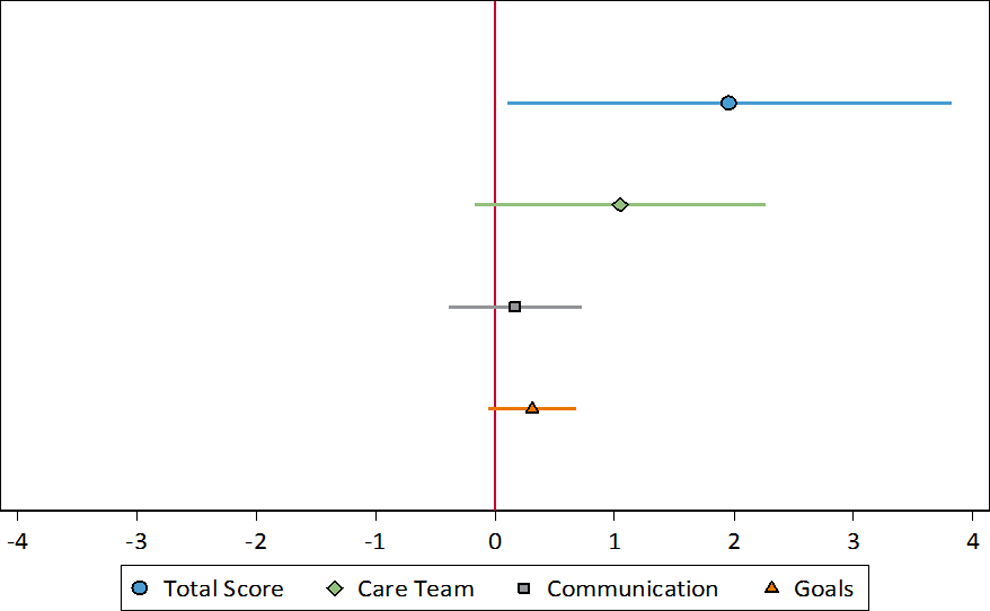
Regression-adjusted change in patient experience by domain. Vertical line represents null hypothesis equals zero.
Discussion
In this quasi-experimental, practice-based study, we found that LifeCourse—a whole-person, approach to care for serious chronic illness—was associated with better patient experience. Various statistical adjustments and sensitivity analyses did not remove this overall association, suggesting a robust, if modest, treatment effect.
Although not a primary concern, testing domains separately was informative. Findings suggest that the overall treatment effect represents a sum of effects across domains of patient experience. Individual domains had positive, but nonsignificant, effects. Further work on individual domains, with larger samples or qualitative assessment, may help further understand the strengths and limitations of the intervention. Teasing out such domains may be particularly important for patients with complex chronic illness, whose treatment burden often goes unaddressed in usual care. 40 Moreover, discussions and communication tools (generally and in late life) do not guarantee patient–clinician concordance or decisions oriented to the whole-person. 25,41,42
Patients with complex illness face high treatment volume, sense-making, and other demands that threaten to overwhelm personal capacity and disrupt everyday life. 5,14,43,44 For these patients especially, it is vital that care models include teams who know and communicate with patients around their goals. It is important to avoid late response to treatment intensification and overmedicalization and improve person-focused care. To do so, moving care models upstream from end-of-life care may be useful, provided transitions and relationships can be supported. We plan to assess care transitions and new services needed (items not part of the main experience tool analyzed here) in future work.
Limitations of this study primarily relate to the use of a nonequivalent comparison group. Although we adjusted for confounding and preexisting differences, residual selection bias and residual differences between sites may remain. In future studies, large cluster randomized studies would greatly help establish effectiveness. Of course, given the realities of practice, such a design might be unfeasible for providers and come with a potential loss in external validity. Our use of a new measure may be another source of concern. In addition, attrition bias is likely; while sensitivity analyses suggested only limited attrition bias in the treatment effect, unobserved correlates of attrition may still shape results. Although improving patient experience is a key goal of LifeCourse, studying this outcome does mean that we cannot afford space to address the costs or sustainability. Another issue for further research is generalizability to other disease sets. We did examine patients with cancer, heart failure or other chronic conditions, and dementia or Parkinson disease. However, these conditions have unique challenges, and individuals can have additional conditions beyond their primary diagnoses. Most in this study had heart failure or other chronic conditions. Therefore, examining LifeCourse among specific condition sets may help detail its differential impacts. However, we hope to address those in future analyses. Finally, this 6-month follow-up study period, while reasonable, does not examine patient experience in long term.
Despite limitations, this study addressed selection and attrition while quasi-experimentally evaluating a novel intervention for late-life care. It found benefits for overall patient experience and also found that this overall experience effect is likely a sum of modest effects across care team, communication, and care goals domains. These findings suggest that LifeCourse, as a team-based, whole-person, longitudinal approach to care, deserves further attention as a way of improving patients’ experience with care at the later stages of serious chronic illness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Robina Foundation.