
Abstract
Highly experienced allied health professionals possess extensive knowledge and skill developed through sustained professional practice and have the potential to support the development of others. However, their willingness, capacity, or opportunity to enact an identity as an expert varies. This study explored how highly experienced allied health professionals in Aotearoa New Zealand construct and negotiate expert identity through narratives of critical workplace incidents. Focusing on therapy professionals across disciplines, the study examined how expertise is narrated, recognised, and sustained within professional communities rather than treating expertise as a fixed individual attribute. Using an interpretive, critical pragmatic methodology, critical incident narratives were collected from 45 highly experienced practitioners, most of whom were women and did not identify as Māori or Pacific peoples. Affirming, challenging, and transformative incidents provided insight into how participants made meaning of their professional experiences and positioned themselves as experts in relation to colleagues, organisations, and professional norms. Analysis showed that professional confidence was central to the construction and expression of expert identity. Confidence functioned both as an outcome of experience and as a narrative resource that enabled practitioners to act, share knowledge, and navigate uncertainty and vulnerability. Affirming incidents often reinforced expert identity through role clarity, professional recognition, and value alignment, while challenging incidents prompted reflection, narrative reframing, and changes in practice. The findings highlight expertise as a relational and socially supported identity, constructed through storytelling, professional interaction, and collective recognition, offering a nuanced understanding of how expert identity is sustained in allied health practice.
This study explored the nature of professional expertise amongst highly experienced allied health professionals in Aotearoa New Zealand. Focusing on therapy professionals across disciplines, we examined how expertise was constructed, recognised, and sustained within workforce communities. Using a mixed-methods design, we collected and analysed critical incident narratives from 45 participants, most of whom were women and did not identify as Māori or Pacific peoples. These narratives – affirming, challenging, and transformative – provided insight into how allied health professionals made meaning of their work and how this meaning shaped their professional identity and expert performance.
Professional confidence was closely linked to the development and expression of expertise. Confidence was both an outcome of experience and a resource that enabled practitioners to navigate complexity, uncertainty, and vulnerability. Affirming incidents often reinforced confidence through role clarity, peer support, and alignment with professional values. Challenging incidents, by contrast, revealed how threats to confidence prompted reflection, adaptation, and growth which are key processes in the development of expertise.
The findings highlight the value of expert allied health professionals and the critical role of professional communities in fostering their development. Expertise was shown to be not only an individual achievement but also a socially supported process, cultivated through knowledge-sharing, reflective practice, and narrative reframing. This study offers a multidimensional understanding of expertise in allied health, emphasising the dynamic interplay between confidence, meaning-making, and professional identity.
Introduction
Approximately 27 allied health professions in New Zealand are client-facing, including physiotherapy, occupational therapy, social work, speech-language therapy, and psychology. Collectively, these professions comprise a workforce of over 30,000 practitioners, hereafter referred to as allied health professionals (AHPs). Highly experienced AHPs possess substantial knowledge and skill, developed through broad and deep professional experience (Jackson et al., 2017). As such, they have the potential to contribute significantly to the ongoing professional development of their colleagues. However, they may be more or less willing, able, or available to take up an identity as an ‘expert’.
Professional identity is understood as the evolving integration of personal values, professional knowledge, ethical responsibilities, and social roles that shape how individuals think, feel, and act as members of a profession. Expert AHPs are typically sought out by their professional communities for their advanced knowledge, skills, and experience. To be recognised as an expert, a highly experienced AHP must have a positive professional reputation and be willing to share their knowledge and skills with others (Jackson et al., 2017). Knowledge-sharing may involve articulating what one knows as well as asking about what they do not know, which may leave them feeling vulnerable (Treem & Leonardi, 2015). Expert AHPs are therefore also characterised as active learners, who reflect on mistakes, recognise gaps in their knowledge, and deliberately seek new learning opportunities (Alderson, 2010; Ericsson, 2008).
Confidence can influence the knowledge-sharing behaviours of AHPs, despite proven competence and substantial experience (Jackson et al., 2019). AHPs develop professional confidence through ongoing reflection and reflexivity in relation to their own understanding of and belief in their role, scope of practice, and significance of their profession, intertwined with their capacity to competently fulfil role, scope, and professional expectations (Holland et al., 2012). Professional confidence is threatened when one of these elements is incomplete or unfulfilled. For example, a limited capacity to fulfil their expected role either through a clash of boundaries with another professional or through a lack of resources (equipment, time, or evidence-base) can lead to low professional confidence (Hsu et al., 2006). Confidence can be diminished by ambiguities of role and scope of practice, the most frequently cited sources of conflict in a health organisation (Kim et al., 2017). Interprofessional practice requires a practitioner to know their own scope of practice and be comfortable exploring the overlap with others (Lawlis, 2014). When the status and significance of a whole profession is questioned, by other professions or by an organisation, practitioners may question their own role in the organisation and their ability to contribute (Canrinus et al., 2012; Weitz, 2017). Where professional confidence is threatened, it seems likely that knowledge-sharing behaviours will be reduced, resulting in poor visibility amongst the professional community.
Confidence develops through reflection on all kinds of experiences, not just positive ones. For nurses and occupational therapists with more years of experience in the workplace, reflecting on negative experiences was useful in building confidence (McMullen et al., 2014; Wilding et al., 2012). The reframing of these negative experiences added positively to the identities of these practitioners. Feeling confident as a professional is likely to encourage knowledge-sharing behaviours, which in turn help the community recognise the experts amongst them (Chen & Hung, 2010).
Using Narratives to Explore Identities in the Workplace
If we want to deeply know someone, then hearing their authentic voice is a great start (Mann, 2016). In-depth interviews can be designed to give the interviewee space to explore more deeply their self rather than following a predetermined fixed set of questions developed by the researcher, which may or may not gather the required data. In-depth semi-structured interviews are reflexive, and the interviewee makes choices about what to say about their life and how they live it (Mann, 2016; Schostak, 2006). Interviews are a valuable method to collect narratives.
Narrative and identity are connected, with narratives or stories seen as a primary form of self-expression, revealing our multiple identities. The constructionist view of identity means that different and contradictory identities can co-occur within the same individual (Barreto & Ellemers, 2011). Analysis of stories shows how storytellers create and represent their selves, both their actions and their knowing. Narrative analysts consider that our stories make us who we are, reflecting our identities through a process of creation, re-creation, negotiation, and reward (Schiffrin, 1996). For AHPs, their work stories can show how they construct positions in their workplaces amongst their colleagues and clients and how they display their social identities as experts (Barreto & Ellemers, 2011; Schiffrin, 1996). Researchers in organisational and management studies have used narrative analysis to investigate the experiences of health service leaders and managers (Gabriel, 2015; McKenna & Richardson, 2003). There has been a little work focused on the narratives of the workers themselves – mainly social workers (Savaya et al., 2011) and nurses (Blomberg & Welander, 2019).
Narrative analysis offers a powerful lens for understanding how identities are constructed through storytelling. Within this framework, the Critical Incident Technique enables focused exploration of significant, real-life events that shape professional confidence and identity. Critical incidents are stories of events that might change the way a person is; that is, the incident is transformative. Each incident is critical in the sense of being significant rather than specifically a crisis or emergency (Fridlund et al., 2017). Incidents may be mundane, a highlight or a low point. For example, the realisation of ordinariness maybe a turning point and therefore transformative (Ferguson et al., 2010). Critical incidents are stories about the self and practice embedded in social and organisational contexts.
It is particularly effective for capturing the emotional and cognitive intensity of affirming, challenging, and transformational experience, where identity negotiation is most visible. These incidents can reveal how AHPs respond to professional challenges and affirmations, offering insight into the dynamic processes of identity construction.
Aims
This study aimed to explore how highly experienced AHPs construct and negotiate professional identity, particularly the identity of expert, through narratives of critical incidents. Using an interpretive critical pragmatic methodology, we examined how professional confidence shaped knowledge-sharing behaviours and the visibility of expertise within professional communities.
Method
This project was approved by The University of Auckland Human Participants Ethics Committee (approval no. 019482).
Personal Statement
All members of the research team are highly experienced AHPs: one is a speech-language therapist with a clinical caseload, one an audiologist, and one a registered psychologist. The idea of the native researcher, an insider, stems from anthropology, and going native is suggested as a way to become a participant rather than an observer of people (Kanuha, 2000). As an insider conducting research within a community where you are a member, there are both challenges and opportunities (Brannick & Coghlan, 2007; Chen, 2011). Often insider research is conducted with groups that are marginalised, and it is our view that allied health is a marginalised group within New Zealand. It is common amongst native researchers to begin (at least) with narratives, life histories, and interviews as research methodologies, and this research follows that tradition (Kanuha, 2000). Additionally, as a health professional, the primary investigator has training in history taking and interview techniques that were of benefit to this methodology (McGrath et al., 2018).
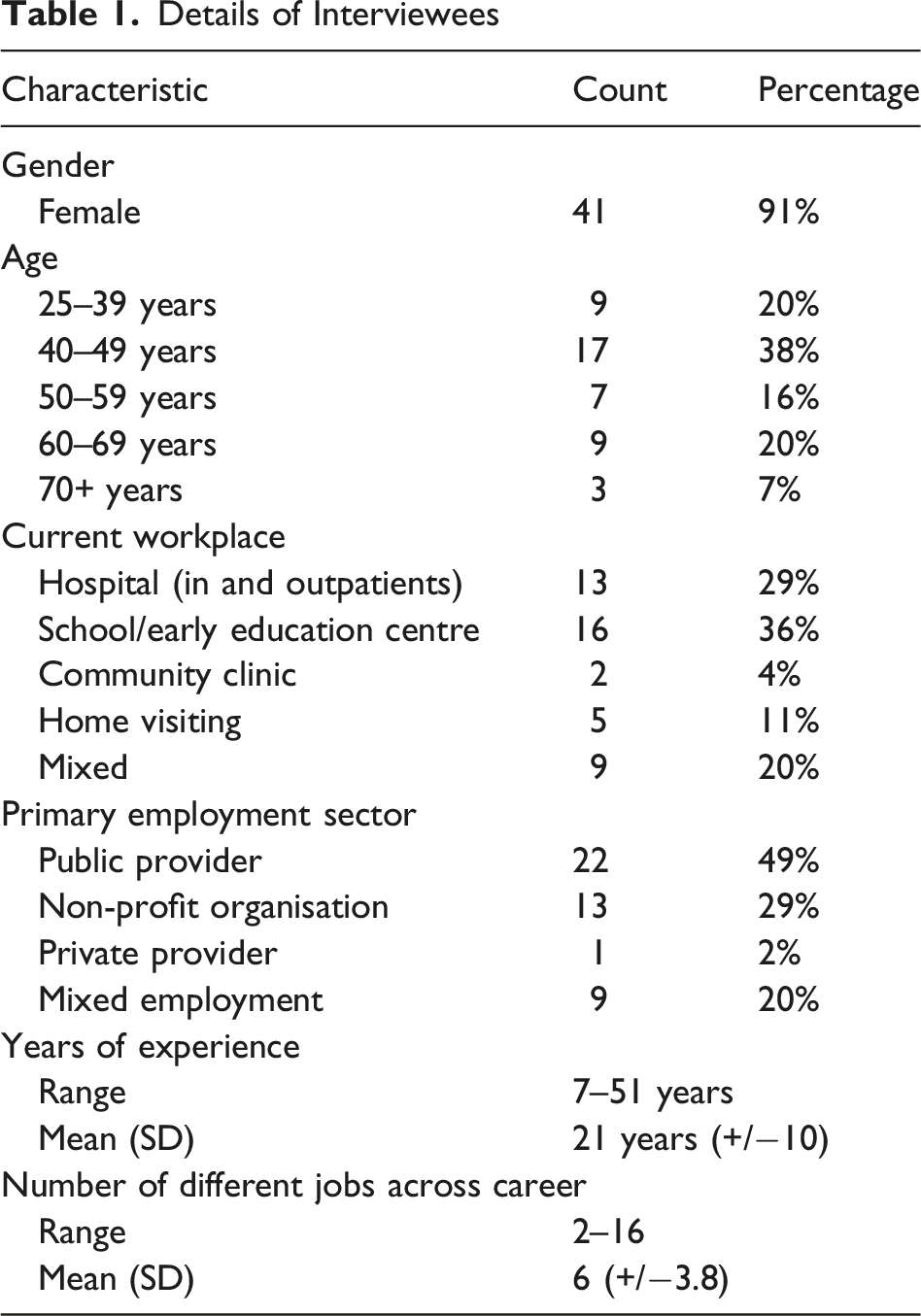
Interviewees
Details of Interviewees
Process
A topic guide was created (see Figure 1). Prior research suggests interviewees need time to identify the incidents, and hence the key questions were sent out a week in advance of the interview (Hughes, 2012). The topic guide remained the same for each interviewee although the exact questions presented in each interview changed in response to previous and current interviews. Topic guide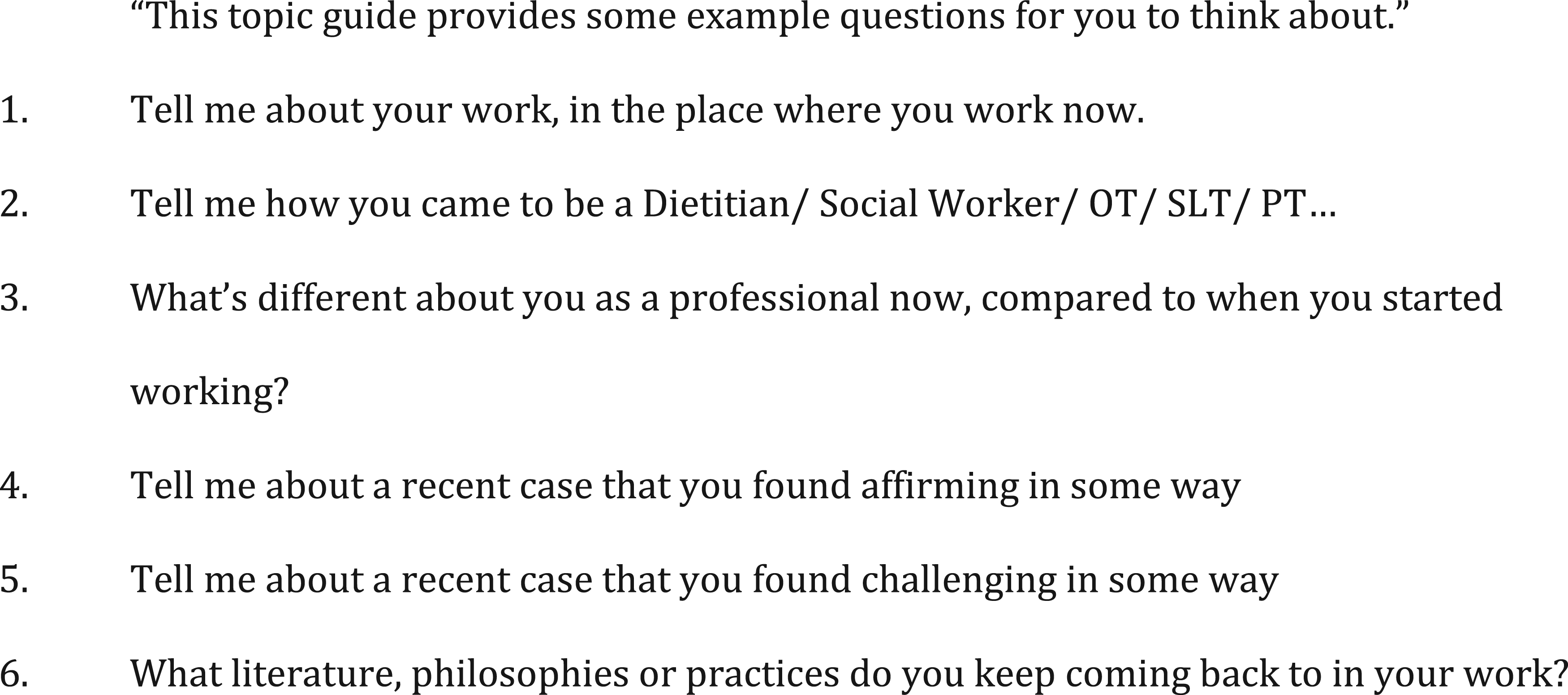
Interviewees provided a recent curriculum vitae and took part in a face-to-face semi-structured interview in a location of their choice. Interviews took place across one year, in many locations across both rural and urban New Zealand. Typically, interviews were at the interviewees’ workplace, often in a bookable multi-use space as most did not have their own private space at work. The remaining interviews took place either in cafés, at the interviewee’s home, by phone, or at the researcher’s office, according to interviewees’ preferences. Interviews were between 45 and 90 minutes long. The primary investigator conducted all interviews. This shared ground was intended to fostered trust, openness, and richer data.
Each interview was audio-recorded and later transcribed by a professional transcriber, checked for accuracy by the primary investigator, and returned to the interviewee for checking. One interviewee made a minor change to the content of their transcript and no additional interviewee involvement was sought.
The primary investigator engaged in reflexive journaling throughout data collection and analysis, using it to inform regular supervisory discussions and enhance analytical rigour (Levitt et al., 2018). Narrative inquiry has been critiqued for overlooking local contexts, including institutional constraints, power dynamics, and cultural discourses, despite its focus on broader societal narratives (Riessman, 2008). In response, the researcher personally conducted all interviews, verified transcripts against recordings, and documented contextual details and participants’ educational, professional, and personal histories.
Analysis
Critical Incident Technique involves an iterative analytic process that is concurrent with data collection (Hughes, 2012). The analysis was informed using the expanded critical incident approach of Hughes (2012). Two analyses of critical incidents are reported here – thematic analysis of all the incidents and a performative narrative analysis (PNA) of selected incidents. We combined thematic and performative narrative analyses, to gain a holistic view of both the content and the expression of these critical experiences. The dual analysis approach enabled a comprehensive understanding of both the content and the way AHPs narrate their experiences. It captured not only what incidents are considered critical but also how these narratives are constructed to reflect professional identities.
While participant characteristics were considered during sampling to ensure diversity of professional backgrounds and experience, these characteristics were not used as analytic variables. Our interpretive narrative approach prioritised how experiences were storied and made meaningful rather than who experienced them in demographic terms. We therefore chose not to stratify or interpret findings by demographics, as doing so would have implied an analytic intent beyond the scope of the study and the data collected.
Identifying the Critical Incident Narratives
Critical incident narratives emerged from semi-structured interviews covering various career-related topics. Transcripts were repeatedly reviewed by the primary researcher (‘I’) to identify narratives, incorporating both interviewer and interviewee utterances in recognition of the co-constructed nature of interviews. Narratives typically began with direct prompts (e.g., ‘Tell me about a case or client that was challenging’) and ended with summarising or forward-looking statements. When stories arose unprompted, I identified their boundaries using linguistic cues or my own transitions (e.g., ‘right, moving on’). Entire transcripts were reviewed to capture stories that resumed later. Stories were identified by first-person language (e.g., ‘I did …’ and ‘I thought …’) and were not edited beyond transcription. These narratives were entered into NVivo for storage and analysis.
Some interviewees shared discrete incidents, while others offered more generalised accounts lacking specific details. These were still included, as they conveyed meaningful insights, possibly reflecting efforts to protect themselves or their clients.
Thematic Narrative Analysis
Thematic narrative analysis primarily focuses on ‘what’ is said rather than how or why (Kim, 2016; Riessman, 2008). Our analysis emphasised the meanings participants attributed to their experiences rather than the linguistic structure or causal explanation of the narratives. As such, thematic analysis does not seek to explain why narratives were constructed in particular ways but rather to identify recurring thematic content within the stories told. It differs from the reflexive thematic analysis of Braun and Clarke (2019) in that it aims to organise whole narrative cases, and maintains a more distant position from the interviewee (Kim, 2016). It differs from PNA which helps the reader understand how and why things happened the way they did for a particular protagonist (Kim, 2016).
Two different categorisation strategies were used, one being quantitative and one thematic. The quantitative categorisation identified more concrete or factual details, for example, whether the work was in or outside of the practitioner’s scope of practice. The thematic categorisation describes more nuanced categories across the collected incidents. Coding was first at a semantic level, identifying surface meanings from the cases in order to organise the data (Kim, 2016). All cases were coded either Affirming, Challenging, or a Change of Practice. Incidents were read and re-read to code them confidently. All authors then read a subset of six of the narratives and came to agreement about the categories of experience before further analysis.
The cases were then all coded in relation to elements of professional confidence using a small number of predetermined categories (Scope of Practice, Role Clarity, Significance of the Profession, Sufficient Resources, Competency and Knowledge) drawn from an earlier literature review (Jackson et al., 2019). After several re-readings, each narrative was also condensed into a very short summary, to capture the essence of the plot. These summaries are used to exemplify the categories derived in the analysis. Again, after initial coding and summarising, all authors discussed the analysis until alignment was attained.
Whilst reading and re-reading the incidents, themes were constructed from the data that offered a more nuanced understanding of the narratives. Thematic narrative analysis shows commonalities and differences of categories and themes across cases, providing a description of the context of the narratives (Kim, 2016). This broad context supports the further interpretations of particular cases through PNA (Shukla et al., 2014).
Performative Narrative Analysis (PNA)
PNA research considers how people talk about what they do, which can tell us about their identities, values, and possible future actions. It focuses on ‘why’ stories are used (Riessman, 2008). Particularly, we could ask why is this incident storied? We attended closely to word choices, interrogating language for meaning rather than taking it at face value (Kim, 2016; Riessman, 2008). Direct speech was highlighted for its role in conveying agency, enhancing credibility, and expressing otherwise difficult experiences (Schiffrin, 1996). It also dramatises the narrative and fosters a sense of shared understanding between the interviewer and interviewee. Conversational asides, repetition, and expressive sounds were noted as markers of emphasis or engagement. The positioning of characters within narratives was also considered (Riessman, 2008). Each narrative was read at least six times, with evolving interpretations documented, acknowledging that meaning can shift with the reader’s context. Interpretations were grounded in both textual features and interview context to enhance plausibility. Initial analyses were discussed with co-authors, whose reflections informed the final interpretations presented here.
Four narratives were chosen out of the total, to highlight different identities of AHPs in different scenarios: challenging, affirming, and transformational. Stories can be seen as a life created through dialogue, and the researcher has power in selecting, rejecting, and neglecting specific stories (Frank, 2012). We actively sought situations that may be unresolved or in fact negative, to counter the concern that the choice of narratives may seem to support the investigators’ theoretical interests, for example, by only reporting positive instances (Frank, 2012; Riessman, 2008). The four narratives were not intended to be representative of other AHPs but were chosen because of their potential to inform our understanding of behaviours and attitudes as they relate to professional confidence and expertise. In this narrative analysis, identity construction is examined through action and interaction within organisational and interprofessional contexts. The analysis sought to discern how, in their narratives, the interviewees positioned themselves in their work relationships and work tasks, key aspects of identity (Jackson et al., 2019; van Os et al., 2015).
Findings – Thematic Narrative Analysis
The nature of the interviewee’s experiences is described (Affirming, Challenging, Change of Practice), and the elements of professional confidence (Scope of Practice, Role Clarity, Significance of the Profession, Sufficient Resources, Competency and Knowledge) are discussed.
Categories of Experiences
Whilst some stories were clearly affirming or challenging, some were both affirming and challenging while some were neutrally conveyed or had a complexity of emotion that resulted in a change of practice but could not easily be categorised. For the analysis, 40% of the stories were clearly affirming based on interviewee categorisation or comment, sometimes following a clarification prompt from the interviewer. A further 40% were clearly challenging, with comments such as ‘it was really tough’ and ‘I hope it never happens again’. The remainder were ambiguous, with both reward and challenge present or no strong overall feeling in either direction, and were included in Change of Practice.
Challenging Incidents
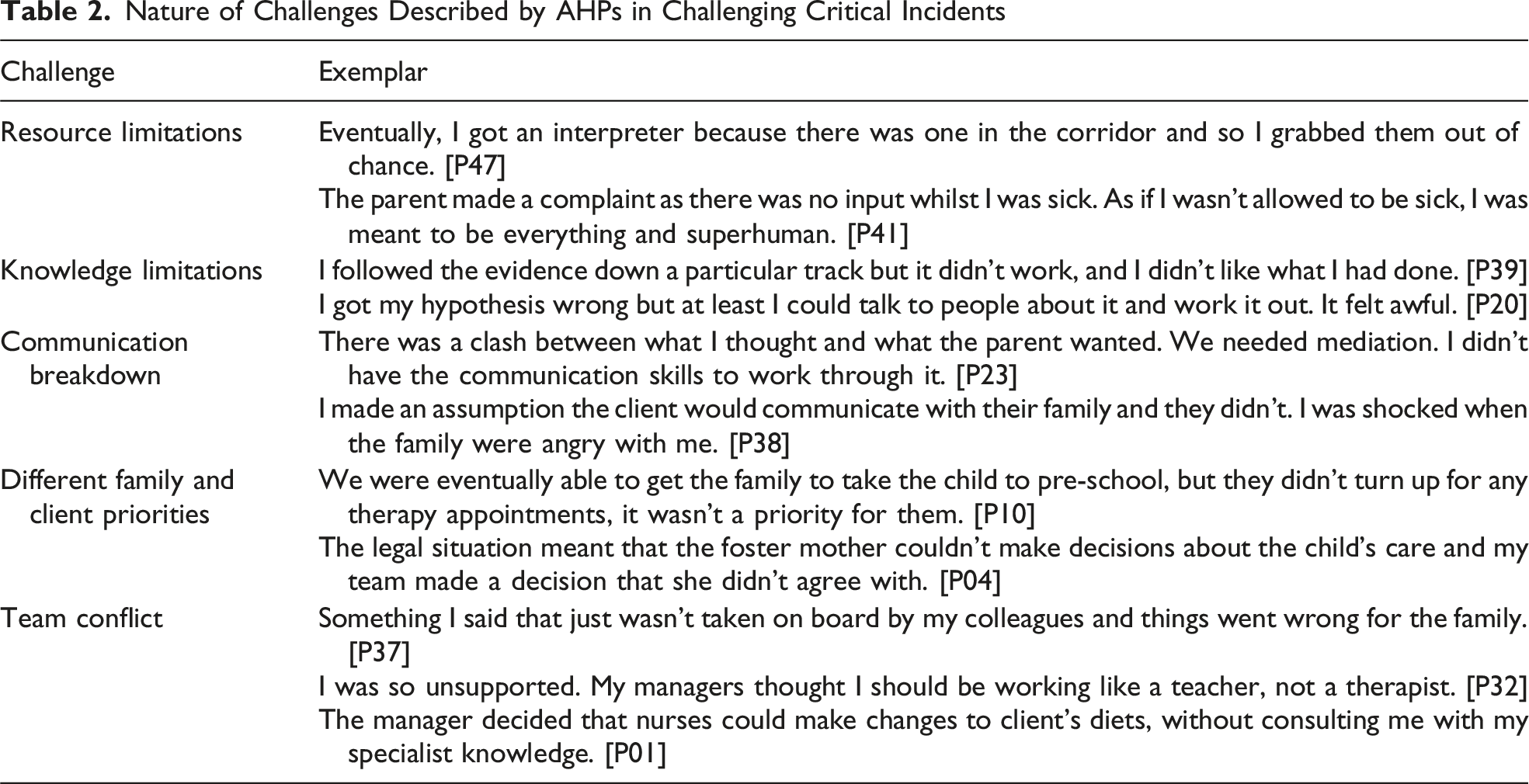
Five broad themes of challenge were developed from the data analysis: (1) Resource limitations – due to lack of evidence-base/literature, money, time, or obstructive service delivery models, what needed to happen could not happen. (2) Knowledge limitations – insufficient or inaccurate technical skill or knowledge to say ‘I knew what to do’ in that situation. This may reflect either an individual practitioner’s current understanding or an absence of established knowledge within the wider evidence-base. Often textbook knowledge was known but could not be successfully applied given the uncertainty or complexity of the situation. (3) Communication breakdown – a breakdown in understanding/negotiation led to a breakdown in trust/relationships. (4) Different family/client priorities – the whanau/client had different priorities to the practitioner, not primarily a communication breakdown. (5) Team conflict – one or more people in the wider multidisciplinary team (not the family or client) were at odds with the practitioner in regard to roles, responsibilities, and boundaries ultimately seeming like a lack of trust.
Nature of Challenges Described by AHPs in Challenging Critical Incidents
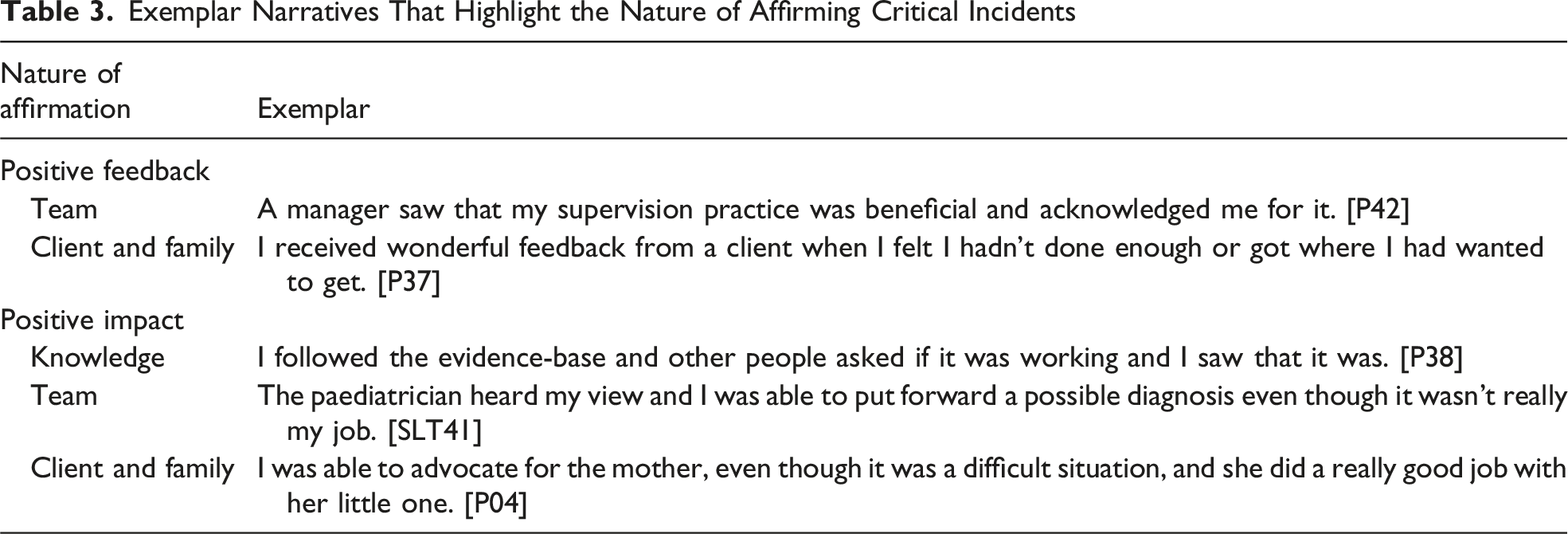
Affirming Incidents
Exemplar Narratives That Highlight the Nature of Affirming Critical Incidents
Change of Practice Incidents
Change of Practice incidents were not fundamentally different from affirming or challenging ones, often involving the same teams, clients, and issues related to resources, knowledge, skills, and communication. Whilst still transformational, the narratives tended to be more nuanced, blending affirming and challenging elements, or interpreted in more complex ways. Further themes were not identified. Some experiences were vicarious – for example, P08 observed a family being ‘railroaded’ in a meeting, prompting her to adopt a more family-centred communication style, despite not being directly involved. Other incidents involved unexpected learning, such as insights gained from clients or personal experiences. P33, for instance, described how becoming a parent reshaped her expectations of families in therapy – a common theme amongst participants.
Elements of Professional Confidence
The Nature of Interviewees’ Experiences in Relation to Elements of Professional Confidence Positively Present
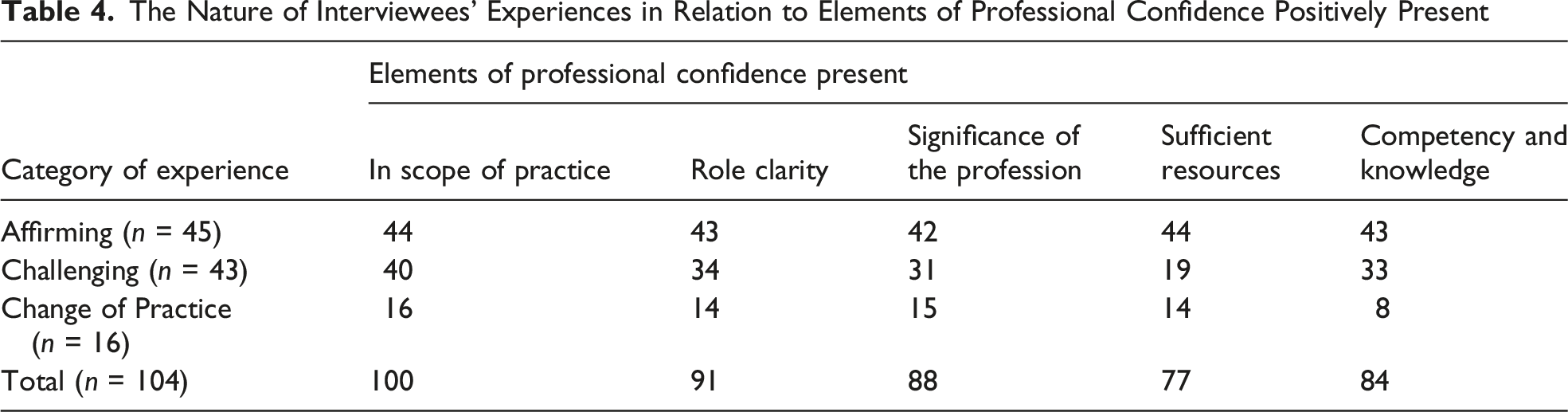
Most affirming incidents had all professional confidence elements positively present, although seven had some potential threats present. These seven potentially negative situations are valuable to keep in mind as they reflect the ability of the seven different narrators to gain affirmation despite these shortcomings. Challenging incidents presented greater threats than affirming incidents, as might be expected: 13 incidents involved multiple threats to professional confidence. Challenging incidents often involved a shortage of resources, but in nearly half of the narratives this was not of concern. Four narratives classed by the interviewees as Challenging did not include any of the anticipated threats and instead reflected a personal clash with either the team or the family they were working with. The elements within professional confidence are discussed here for all cases, and the potential threats are highlighted.
Scope of Practice
In this analysis, scope of practice refers to formal, profession-defined boundaries around permissible activities. Most narrated incidents were clearly within the practitioners’ scope of practice, indicating a strong understanding and commitment to professional boundaries. However, four narratives presented potential scope-related concerns. In two cases, practitioners temporarily assumed roles beyond their scope – one purchased prescribed medication for a client, and another pursued equipment outside their professional remit. The other two involved the use of newly acquired skills (e.g., sensory integration and behavioural approaches), which were questioned by colleagues or the broader professional community. While one of these was framed as affirming, the others were experienced as challenging. Notably, only the medication-related action was team-sanctioned; the remaining incidents reflected individual interpretations of scope that diverged from team consensus, highlighting tensions around professional boundaries.
Role Clarity
Role clarity refers to how a practitioner’s contribution is understood, negotiated, and enacted within a specific workplace or team. Thirteen narratives involved role conflict or ambiguity, primarily arising from unclear expectations about participants’ contribution within multidisciplinary or organisational contexts. Unlike scope-related incidents, these narratives did not question the legitimacy of the work itself but rather how the practitioner’s role was positioned, recognised, or coordinated in relation to others.
These fell into three broad categories: exclusion by others, being left to work alone, or personal uncertainty about one’s role. Exclusion examples included being omitted from multidisciplinary teams despite relevant expertise or having tasks reassigned to less-qualified colleagues. In contrast, some practitioners were left to manage alone, often when they were the sole representative of their profession. Others described mismatches between their expectations and client needs – either underestimating their potential contribution or overestimating their ability to resolve complex issues.
Four narratives framed role ambiguity positively, as opportunities for growth. For instance, one practitioner helped establish a new service where roles were initially undefined but evolved collaboratively. Another gained role clarity through affirming feedback after commencing a new position with unclear expectations. In these cases, role clarity emerged through interaction and negotiation rather than pre-existing definitions.
Significance of the Profession
In about one-sixth of incidents, the significance of the profession was questioned, resulting in the practitioner feeling their profession was undervalued. Unlike role-clarity incidents, which focused on uncertainty about individual responsibilities, these narratives centred on the status, legitimacy, and collective recognition of the profession within the organisation or interprofessional environment.
These incidents were often narrated using a collective ‘we’, reflecting shared experiences of exclusion. A typical example involved professional groups who were routinely not consulted regarding clients’ diagnosis or prognosis, despite being members of the hospital ward team. Participants reported emotional responses including sadness and anger, interpreting this exclusion as a devaluation of their profession rather than a misunderstanding of their individual role.
Other narratives involved more explicit challenges to professional status, including intimidation by individuals – most commonly senior medical staff – who were known to dismiss or undermine the profession as a whole. In these cases, the threat was not to role execution but to professional legitimacy, affecting practitioners’ confidence to speak or act on behalf of their discipline.
Most incidents where professional significance was threatened were experienced as challenging. However, three narratives had affirming outcomes, where participants acted despite feeling professionally marginalised, resulting in positive consequences for their self-belief and sense of professional worth.
Sufficient Resources
Consistent with prior literature, a number of critical incidents involved a lack of resources (Foster et al., 2014; Pring et al., 2012). Twenty-seven incidents were impacted by, or caused by, a shortage of resources and most were categorised as challenging experiences. These included shortages of hands-on staff, and of money to purchase equipment, but also included a shortage of time to do high-quality clinical decision-making, and a lack of supervision and managerial support. Also, interviewees noted service delivery models did not match the evidence-based practice that the research literature recommended. However, in one affirming incident, a client complaint led to a substantial increase in resourcing which left a long-lasting positive impact on the confidence of the interviewee. In all other affirming incident narratives, resource limitations were not mentioned.
Competency and Knowledge
In about one-fifth of incidents, practitioners described issues relating to competency or knowledge. This ranged from a lack of knowledge that led to a problem, to how they had learnt valuable knowledge in a surprising situation. Ten narratives, categorised as challenging, were included in this category and highlight the stress and distress that insufficient knowledge and skills can cause, particularly when it results in poor decision-making that impacts the client and family. One interviewee described that she ‘wasn’t incompetent, but there’s so many things we don’t know’. Learning new knowledge was often from an unexpected source. For example, some practitioners noted how having their own children had provided valuable insights into parenting that had transformed their practice. Half of the Change of Practice narratives included an element of knowledge acquisition. Change of Practice incidents, including having to retrain to meet registration requirements, were seen by some interviewees as a ‘blessing’. Attending courses on the edges of their scope of practice, for example, counselling, also resulted in positive changes of practice.
Findings – Performative Narrative Analysis
Across all 104 incidents, interviewees mostly provided specific details, and only 13 narratives were generic. They tended to refer to incidents that occurred only once, for example, ‘So a critical moment for me, it all happened at the same time’ [P06], but interviewees also suggested there were multiple incidents, for example, ‘Do you want a tricky one or an easy one?’ [P04], ‘It’s probably a couple of patients’ [P03], and ‘There’s a few’ [P01]. A few interviewees struggled to initially think of specific incidents and reported on events from very early on in their working life, for example, ‘Um, there was one when, does it matter if it was from a long time ago?’ [P10]. All these stories have been included in the narrative collection as the interviewees considered them important (van Os et al., 2015).
Four narratives are presented here to highlight different relationships and positioning of AHPs in different scenarios: one clearly affirming and the others presented as challenging by the interviewees. In the four narratives that follow, where possible, quotation of the interviewees’ words is presented. Square brackets indicate words inserted for clarity.
Erica’s Story: ‘That’s One Person That’s Not Going to Pick on Someone Else’
Erica was a social worker who qualified after having her own children. She worked at a large public hospital. She was a dynamic and detailed narrator. An important theme in her account of an affirming incident was teamwork. As part of the team, she was highly valued: E: Part of the team, what I’m doing on the floor is very important and I know they miss me when I’m gone because I know I’ve got a lot of the knowledge and the skills and I can just go, go, go all the time.
In the incident, she knew what to do and was well connected to make things happen. She explained in detail how an elderly person was being abused in their own home, became very sick, and was finally admitted to hospital. Erica was instrumental in getting the person into a safe environment at discharge. She positioned herself as central to connecting the team of people that needed to be involved: E: Then the brother said … This is what the situation is, this is what’s going on. And so I rang the agency to find out more. And they didn’t realise that the person had actually moved in and taken over. I rang another family member to find out more.
Despite this central position, she included the team in her narrative, referring to ‘we’. E: So, we ended up having a family meeting with the brother, [and his family] who gave me the bigger picture of things as well. B: Right. E: And, um, we ended up activating the enduring power of attorney and getting her put into a rest home where she was getting cared for. So I knew I was getting one person safe. B: Yeah, yeah. E: Safe, and cared for, and supporting the brother and he said at least someone’s listened. No-one on the previous ward, no-one anywhere has listened to us.
For herself, the priority was keeping the person safe and she made a unique difference by listening and taking action to connect relevant family and services. Erica’s narrative of saving the elderly person and their family positions her as strong and confident professional, with high standards and ethics. Once the person was safe, Erica continued to address the abuse, acting on her strong sense of justice and caring: E: So, even the Police had done nothing about it! B: Done nothing about it? E: So, so I thought well, you know, this is just not okay and ethically where does this sit? So okay, we’ve got the patient safe, the brother’s a happy person and everything and he’s doing everything, he’s got a huge job on his hands. How do we get this person out, and is she going to do this to somebody else because living [there], she’s going to pick on the next person and get another victim. So I thought, ‘No this is just not okay’.
Once the client leaves the hospital ward, Erica is usually no longer involved, but in this case she was able to use her close connection with a local agency to make further difference. She used the manager’s first name in her recount, to emphasise the relationship power she was bringing to the situation, even though the person was unknown to the interviewer: E: And so I got [agency] involved and I said ‘[name] do you want to know about this situation? This is my emails, my evidence on this. Do you want to know what’s going on? because I think this person needs to be struck off ...’
The incident narrated was one of several similar situations for Erica. The incidents were complex legally, ethically, and logistically. They were also emotionally tiring. She acknowledged the training she has had that has been invaluable and ultimately, she needs time to think things through for herself: E: Um, I’ve had similar ones like that too, where I’ve just had to be really clear, really think through, what’s the outcome I want to achieve?
Veronica’s Story: ‘The Sense of Failure’
Veronica was a dietitian working in the community. This was her third job after qualifying after high school. Central to her recount of a challenging incident was a struggle to have an impact. As a confident and knowledgeable practitioner, she wanted to make a difference: V: Um, I think it’s also feeling more confident because when I was younger I felt like I was too young to be telling people what to do, or advising people or counselling people on life issues, complicated life issues.
Veronica told a generic story about ‘a couple of patients’ who were obese. A technical solution was available to help them – bariatric surgery, but it was often not funded. Her story was one of being competent but constrained. Her use of repetition and direct speech from the client emphasised her shared sense of unfairness and frustration. Initially, she reported how the situation was for the clients, but on questioning she revealed her own feelings, part of a larger picture of sadness. V: Um, so you’re basically starving them to get them to lose weight. Um, but yeah, because of not being able to do exercise because of bilateral knee arthritis or, um, or back pain from spinal damage or something, um, so, yeah it is really challenging. Especially cause, I might see someone for two or three times, and give them healthy eating advice and if they don’t lose any weight and they will say this is very disappointing because they’ve been trying really hard, they haven’t let themselves have takeaways, they haven’t, well sometimes they do, but they haven’t let themselves have snacks and things like that, and they say ‘I’ve tried really hard this is so unfair. I haven’t lost any weight’ and just have to say ‘well actually it is the case for a lot of people who are in the same situation um, it is just the weight that, when you get to that weight it is very hard to do any exercise and metabolism is very slow. Um, and the healthy eating just isn’t going to work for weight loss’. So it is very disheartening for them. B: And how is it for you? V: It’s the, the sense of failure or you take on their disappointment. Yeah. B: Because you can’t, there isn’t really an alternative- V: You can’t help them, no. B: -that’s actually going to make a difference. V: Yeah.
She framed the situation in two contrasting ways. Individually, the work seemed clearly within her scope of practice, and her role was clear but ineffective at times. The evidence-base and service delivery models were insufficient to make a difference, and this led to a shared sense of failure with the client. Veronica used direct speech to convey her competence and to give credibility to what she knew, but the conversational aside suggested resignation as even that option was not ideal: V: I will say to them ‘if you are willing to use the meal replacement drinks I’ll support you with that’, and they also have to be able to afford the meal replacement drinks.
However, as a professional abiding by a code of ethics and an employee of a large public health organisation, she took on some responsibility for the problem, placing herself with the organisation rather than with the client: V: Not [here], we don’t do many surgeries, they often get refused. B: Right, because they’re not well enough or- V: We just don’t fund it- B: -just haven’t got the V: -we put our funding in different areas.
Veronica’s unhappiness with the options available and lack of effective solutions for her clients were the focus of this story. By placing herself in the organisation, and not against it, her lack of power to make a difference could be absorbed by the substantial power of the organisation, but her disappointment was palpable.
Kirsten’s Story: ‘The Class That Broke My Heart’
Kirsten, a speech-language therapist, was clearly proud of the school where she worked and enjoyed her work. She was an active learner and told me she needed to be at least one step ahead of the other staff she consults to. She actively used social media and sought out information to keep herself abreast of new developments. She was clear that she was an experienced and knowledgeable therapist now, having been in a state of anxiety and feeling helpless for a while when first in the job more than 20 years ago.
As a person who pushed herself outside of her comfort zone, Kirsten was very aware of her own substantial skills and knowledge but was also not afraid to ask for help. She readily included her team in her story. Kirsten wanted to tell me about ‘the class that broke my heart’. Kirsten was passionate about her work and the children and compared herself with a particular class teacher who ‘refused to relate to any of her [children]’. Kirsten sought supervision with a colleague who suggested an approach that was effective. K: Um, and we sat down and we talked about this class and the lack of interest from the class teacher, the lack of support from the [team] leader who also pretty much told me um, just don’t pressurise the teacher, these kids are too hard basket anyway. So can you imagine the emotional impact. And I sat down with my [therapy] colleague um, and what she said to me was, pick one student who you think is most likely to make progress, and find somebody, I don’t know if she said this or if that’s kind of what came out of the conversation but basically find somebody to help you to achieve that success. Um, and so I picked one student [with behaviour that was challenging]. Um, and [another therapist], who believed in her. And long story short, was able to produce video evidence to the mother that if you pushed through the [behaviours] your daughter does have the ability to communicate and you’ll grin from ear to ear with pride when she successfully does so.
Not only was Kirsten passionate about success for children, she also positioned herself as emotional and relational. Whilst telling me the story, she mentioned, ‘I can feel myself about to cry now’. After only a short time working, the child’s mother gave Kirsten feedback that she is still proud of and again she identified herself here as a life-long learner: K: that was one thing that her mum had mentioned in terms of you know, what were my daughter’s favourite things in her life? Um, and one of the things she said was one-on-one time with [Kirsten] and interacting with [Kirsten] is what she saw as (pause). So that [incident], that changed my career in the sense that I learned that you don’t just keep pushing and keep pushing and keep pushing. Um, when you have no support.
Previously Kirsten would have kept pushing the class teacher to change her approach, but by making use of the wider team, she had achieved success without having to push the teacher further. Despite the story of success with the child and family, there was no conclusion or resolution of the initial conflict with the class teacher.
The theme of passion recurred throughout the entire interview and is summed up by Kirsten: K: I’m very passionate about my job which, which can have positive and negative effects in that sometimes it’s flippin’ hard um but yeah, I’m very passionate about what I do. B: Yep. What, what is it that you love about it? Or that you’re passionate about? K: I think it is the sheer joy of seeing somebody who has no voice, um, discover and be able to express who they are.
As an AHP who was learning and reflecting, she concluded the interview with further indication of herself on a journey that had not ended yet: K: My mind always tends to think, to focus on one thing and training myself in one thing. And if that is where I’m going then I need to make sure that I’m taking opportunities, um, when they arrive. Yeah, to move myself in that direction.
Chloe’s Story: ‘To Give the Patient the Best Chance’
Chloe was a speech-language therapist working in a regional hospital. She had collected diverse experience in locum positions outside of New Zealand. She now worked full-time with clients and had some leadership responsibilities. She was a specialist in an area of practice that she had come to love. She was a keen reader of the research literature. During the interview, our discussion about learning and what she did when things got difficult led to her telling a spontaneous story about a recent case. Initially, the story was short: There was a difficult case; the client had severe swallowing problems and was eager to try different options. Chloe referred him to a national specialist centre where the speech-language therapist came to the same conclusion as Chloe had done. Chloe made the referral because ‘I just felt I needed to exhaust all my options’. The national specialist centre had been helpful in the past and Chloe often suggested to more junior colleagues to make use of their help. In this brief narrative, Chloe was very committed to her client getting the best treatment and the relationship between Chloe and the national specialist centre seemed easy-going and open.
When prompted to expand on her short story, the desperation of her client became clear and Chloe in turn took on that desperation. She needed to provide hope in the face of a very limited prognosis, which she was able to do for a time by suggesting a treatment, but over time this was insufficient: C: So I just encouraged him to do that [treatment], coz it wasn’t too distressing for him. It became more and more distressing, but … So I had, when the time was right, I can’t remember exactly where, I had talked to him about the [national specialist centre], knowing that he would have to fund that himself. But I talked to him about that and he was at the point, ‘Well I just want to try whatever I can – B: Try every option. C: - To be able to reach that goal’ and I wanted to for his sake as well. So I, and I was very prepared if I’d missed something. I had that sort of ‘What if I have missed something that’s really major here?’ So I put the referral through and everything, and he went up there and yeah (pause), they, they, I can't remember exactly what they did, but I think they did some [tests] and tried a few different things. But pretty much came back with. B: The same conclusion.
It became apparent that making the referral to the national specialist centre was more difficult than was previously conveyed. Chloe had to prepare herself psychologically for having missed something in case she needed to protect herself later. Chloe highlighted her vulnerability and her willingness to make a referral for her client even though her reputation was at stake. C: So in a way it was good from the perspective that it confirmed what I, my management and my assessment and that I hadn’t missed anything. But it was really awful. I was kind of hoping that they, that I had (pause) – B: That they discovered something? C: Yeah, you know, you’ve put yourself on the line by putting you're, going to the [national specialist centre] as a therapist. B: Yeah you do. C: But then you, I wanted to for his sake. I just wanted to know that, coz yeah, just knowing what his future was going to look like.
Her reputation remained intact, but the news for the client was not positive. Comparing herself over time, what was different about her actions now was not a lack of fear, but she immediately positioned the client centrally and transcended herself. B: Do you think if that case had happened when you were newly qualified, you’d have dealt with it in the same way? C: Nope. I don’t think I would have ... But say I was a new graduate now, I think I would have been too scared to, thinking that ‘Well, what if I have got it wrong?’ B: Yeah, right. C: I think if I go back to, I don’t know (pause) I would have probably talked at length with my supervisor at the time and if everyone else was telling me to [make the referral] I would have done that. But it was my first reaction now just to think ‘Well, it’s not about me it’s about the patient’ and yeah, ‘I'll do whatever that works for him even if …’, yeah.
At the end, she told me that she did not have a lack of skill or knowledge, but a shortage of the right resources. She could recount some great successes that her team can be proud of, comparing these favourably with those of the national specialist centre. She was able to reflect on these successes to be positive about her own ability. Here, she positioned herself not only as skilled and knowledgeable but also as a champion for people’s health, with ambitions and a big vision: C: Yeah. But when you’ve been around for (pause) And I think it’s also knowing that we don’t have the right equipment. Or not the right equipment, but we don’t have as much as what the [national specialist centre] has. So to give the patient the best chance that’s what they need. And that probably comes back to ideally I’d love building a new hospital to be able to have everything at our fingertips. Wouldn’t that be amazing – B: Yes, yeah! C: If every place could just do that.
Discussion
Using the Critical Incident Technique within narrative analysis enabled the collection of rich, contextually grounded stories that illuminate how highly experienced AHPs construct and negotiate professional identity, particularly the identity of expert. Critical incidents provided a focused lens through which experiences could be examined, making visible how expertise is enacted, tested, and recognised in practice.
Affirming, challenging, and otherwise transformative incidents were discussed in relation to professional confidence and the role confidence plays in the development and expression of expert identity. Challenges stemmed not only from threats to self-belief but also from communication breakdowns across organisational, professional, team, client, and family levels. Some practitioners reframed these threats as affirming experiences, strengthening their sense of themselves as competent and credible experts. While affirming incidents were more likely to involve clear scope of practice, role clarity, professional recognition, and adequate resourcing, this was not universal. Several AHPs described affirmation emerging from complex, ambiguous, and resource-limited contexts, often accompanied by personal vulnerability.
Thematic narrative analysis revealed that AHPs frequently encountered human suffering, injustice, and systemic limitations. Within these ‘conditions of living’ (Frank, 2012), participants narrated a desire to belong, to make a difference, and to be valued as professionals. Through their stories, interviewees positioned themselves as knowledgeable agents of change, often describing moments where expertise was asserted, recognised, or contested. Narrative features such as direct speech, repetition, and shifts in verb tense conveyed agency and urgency, with present and future tenses signalling a forward-looking, action-oriented stance consistent with an expert identity (Riessman, 2008; Schiffrin, 1996).
These narratives reflected processes of meaning-making in professional life, aligning with Baumeister and Newman’s (1994) framework of purpose, values, efficacy, and self-worth. For example, Erica’s narrative centred on purposeful action to ensure client safety, positioning her expertise as morally grounded and necessary. Kirsten and Chloe emphasised justice and vulnerability in service of client wellbeing. Chloe’s account illustrated how acting without institutional resources, but still achieving positive outcomes, reinforced her self-belief and professional identity as an expert.
By contrast, Veronica’s narrative illustrated the emotional toll of working in isolation within a large organisation, where limited recognition and support undermined her sense of professional contribution. Her story highlighted how expert identity can be constrained when opportunities for collaboration and recognition are absent. In contrast, Erica and Kirsten described affirmation emerging through supportive colleagues and collaborative professional networks, reinforcing their confidence and visibility as experts.
Across the narratives, professional experiences were depicted as both distressing and rewarding. AHPs described challenging and supportive relationships with colleagues, managers, and families, often within the same incident. Several participants, including Erica, Kirsten, and Chloe, incorporated junior staff into their narratives, using these moments to enact expertise through mentoring, teaching, and community-building. Positive partnerships with families further reinforced participants’ sense of professional worth and expert identity.
When professional confidence was threatened, AHPs constructed their expert identities in different ways. Those with clarity around their role, scope of practice, and the significance of their profession were more likely to reinterpret challenges as affirming, strengthening their self-belief and willingness to share knowledge. In contrast, similar situations were experienced as damaging when role boundaries or professional recognition were unclear. Ultimately, how practitioners interpreted critical incidents was closely tied to their capacity to find meaning in their work. A sense of belonging, efficacy, purpose, and alignment with personal values emerged as central to sustaining expert identity and professional wellbeing.
The data represent narrative snapshots rather than objective accounts of events and reflect how participants chose to present themselves at a particular moment in time. As such, generalisation should be approached with caution. As an exploratory study, we do not claim to establish causality or make definitive recommendations for practice. Expertise was conceptualised as socially constructed, and participants may have portrayed themselves in ways that supported particular professional identities. Within an interpretive framework, such identity work is considered part of the data rather than a limitation.
The interviewees were predominantly female and did not identify as Māori or Pacific. Purposeful sampling is therefore needed in future research to include male AHPs and those who identify as Māori or Pacific. Although allied health professions are often grouped together, differences in professional culture and education suggest caution when transferring findings across disciplines. Finally, the distinctive employment and funding context of allied health practice in Aotearoa New Zealand limits direct transferability to other health systems.
This study demonstrates how highly experienced AHPs construct and negotiate expert identity through narratives of critical workplace incidents, revealing expertise as relational, contextual, and closely tied to professional confidence. Affirming and challenging incidents made visible how clarity of role, scope, and professional recognition shape knowledge-sharing behaviours and the visibility of expertise within professional communities. Attending to these narrative processes offers valuable insight into how expert identity is sustained and sometimes constrained, within contemporary allied health practice.
Footnotes
Ethical Considerations
This project was approved by The University of Auckland Human Participants Ethics Committee (approval no. 019482).
Consent to Participate
All participants provided written informed consent prior to enrolment in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded by The University of Auckland. There is no grant number.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.