
Abstract
Coordination among health professionals across levels of care is essential for safe treatment, yet fragmented digital systems complicate the obtaining and sharing of patients’ medication information. This ethnographic study explores how medication information is coordinated in everyday work and how tools are involved. We observed 145 hours of work and conducted 24 interviews with physicians, pharmacists, and nurses in Norwegian primary and specialized care. Data were analyzed thematically, informed by sociocultural and boundary work perspectives. We found that coordination is continuous, situated work that can be supported, but not replaced, by digital tools. The observed health professionals engaged in both competitive and collaborative boundary work. Competitive strategies (disengagement, opposing established responsibilities, and delegating work tasks) rendered coordination of medication information “dirty work.” Collaborative strategies (requesting information, cleaning up, and preventing discrepancies) restored alignment and enabled the sharing of accurate information. Digital medication lists operated as boundary objects: they facilitated the sharing of patients’ medication use but sometimes failed to align perspectives, contributing to fragmentation and the construction of “dirty work.” Conceptually, we extend boundary work understandings by documenting the defense against jurisdiction as a competitive strategy and by demonstrating how this boundary work may produce “dirty work.” This study thus contributes to understanding the interplay between structural fragmentation, professional practices, and digital tools in healthcare coordination. Policy and system design should recognize and support the boundary work that enables the coordination of medication information.
Introduction
Coordination among health professionals across levels of care is essential for safe and coherent patient treatment (Report No. 9 (2023-2024)). Patients with complex conditions often move among different levels of healthcare services and require an exchange of information to ensure that comprehensive care can be provided. These patients often take multiple medications, which are frequently adjusted and thereby require continuous updates if an accurate and up-to-date medication list is to be maintained. Insufficient coordination remains a fundamental challenge in modern health services, where transfers of care are associated with increased risk of medication discrepancies and patient harm worldwide (Bonaudo et al., 2018; Graabæk et al., 2019; Park et al., 2024; World Health Organization, 2019). The coordination of medication information requires interaction among healthcare professionals in primary and specialized healthcare (Wadmann et al., 2009) and involves continuous work to connect fragmented systems (Allen, 2015).
Policy efforts increasingly emphasize the use of digital tools to strengthen coordination. In Norway, attempts to improve access to medication information have introduced digital tools such as local electronic health records (EHRs), the Summary Care Record (SCR), and the Shared Medication List, currently in pilot (Report No. 7 (2019–2020); Report No. 9 (2012-2013); Report No. 23 (2024-2025)). These systems build on the assumption that coordination can be achieved through standardization and digitalization (Report No. 9 (2023-2024)).
Despite digital efforts, coordination challenges persist. Local EHR systems remain disconnected from other institutions, creating challenges for health professionals (Manskow & Kristiansen, 2021), and health professionals often experience the SCR as incomplete or outdated, reducing their trust in it (Lundhaug et al., 2024). Fragmented information flow across care levels (Kleppe et al., 2017; Sogstad & Bergland, 2021; Wang & Manskow, 2024), differing work cultures and perspectives (Persson et al., 2022; Tønnessen et al., 2016), unclear responsibility allocations (Kleppe et al., 2017), and the need for verbal communication to ensure continuity, clarification, and nuance even when digital channels exist (Brattheim et al., 2016; Hellesø et al., 2019; Sogstad & Bergland, 2021), all suggest that coordination is not only a technical integration problem that can be solved through digitalization and standardization, but one that remains deeply embedded in everyday interactions.
Rather, coordination efforts must be understood as social and situated practices, shaped by the contexts in which they occur. These practices often consist of social interactions among health professionals, for example, contacting other health professionals or levels of care to gain clarity about patients’ medication use (Wind et al., 2025). Such practices serve as checkpoints to ensure the accuracy of medication lists (Ellingsen et al., 2024; Hertzum & Ellingsen, 2023; Nybakke, 2025). Coordination requires health professionals to establish shared meanings across levels of care (Håland & Osmundsen, 2015) and develop strategies that align care efforts across both professional and organizational boundaries (Hedqvist et al., 2024; Weber et al., 2022). In other words, the professionals engage in boundary work (Langley et al., 2019) to establish shared understandings and aligned medication lists across care levels. The cited studies show that coordination challenges are not only technical but are embedded in everyday interactions. Addressing coordination challenges may require a practice-level understanding of boundary production and related sociocultural dynamics such as hierarchies, local routines, and how tools are enacted in context (Conn et al., 2016).
Coordination unfolds through participation, negotiation, and interaction in everyday work. From sociocultural perspectives (Vygotsky, 1978; Wenger, 1998), coordination across professions and levels of care is understood as social practices enacted in situ through interactional work, where health professionals mediate knowledge through language and artifacts and negotiate meaning. Artifacts are part of practice, which is always social and embedded in historical contexts (Wenger, 1998), further emphasizing that technology alone cannot solve coordination challenges. Building on this perspective, this study explores how the coordination of medication information unfolds in everyday work, focusing on how professionals interact to facilitate continuity across levels of care. Specifically, we ask how health professionals coordinate medication information across care levels, and how digital tools are involved in this work. Here, coordination is approached as a situated practice in which professional interaction and the use of artifacts are closely intertwined. This study illuminates how professionals interact to manage coordination challenges in digitally mediated work across healthcare settings. This knowledge is essential for understanding the sociocultural conditions under which coordination is achieved, thereby contributing to situated approaches to digitalization in healthcare.
Despite substantial research on coordination during transfers, little is known about how medication information specifically is coordinated. Nybakke (2025) conceptualized the medication list as a multiple object reshaped by professionals’ priorities as it moved across levels of care. By contrast, this study centers on sociocultural practices, not the object itself, examining how health professionals navigate the coordination of medication information both within institutions (preparing medication lists for internal/external use) and across care levels (sharing and constructing medication lists). This study thus contributes to understanding the interplay between structural fragmentation, professional practices, and digital tools in healthcare coordination.
The Context of the Coordination of Medication Information in Norway
This study was conducted in the Norwegian healthcare system, characterized by a division between primary and specialized care. Primary care, managed by municipalities, includes general practitioner (GP) offices, nursing homes, and home-based care, while specialized care, managed by regional health authorities, consists of hospitals and hospital pharmacies (Nylenna, 2020). The primary and specialized care institutions participating in this study do not share EHR systems, and the GP offices used different systems from nursing homes and home-based care. These systems did not communicate, and medication information was not automatically shared across care levels. The coordination of medication information therefore relied on health professionals’ efforts.
Practices surrounding the coordination of medication information varied across professions and settings. Norwegian legislation does not specify how responsibility should be distributed but requires that an updated medication list follow the patient in transitions of care (Norwegian Ministry of Health and Care Services, 2008). It is further stated that GPs are responsible for updating their medication lists when receiving information about changes from other care levels (Norwegian Ministry of Health and Care Services, 2012). Responsibility is thus defined in general terms, leaving the practical coordination of medication information to be negotiated in everyday work. However, in Norway, the prescribing authority is restricted to physicians, positioning them centrally in the coordination of medication information.
Medication information refers to information about a patient’s medication treatment that circulates across professionals and care levels. This information is produced, interpreted, negotiated, and shared in everyday work interactions between health professionals. Medication lists are artifacts that materialize medication information by attempting a systematic overview of a patient’s medication use (type, dosage, and timing). They are produced locally within institutions, typically during patient admission, based on medication information from other care levels, and can be both paper-based and digital. As such, medication lists can be understood as artifacts through which medication information is shared across professional and organizational boundaries.
Practice Boundaries, Boundary Objects, and Boundary Encounters
Coordinating medication lists entails complex, collaborative processes that require the navigation of multiple information sources and alignment of knowledge across organizational boundaries. From a sociocultural perspective, organizational knowledge is situated in practice, mediated by artifacts, rooted in interaction, and continuously negotiated (Gherardi & Nicolini, 2000). Practice boundaries emerge in the workplace through mutual engagement, joint enterprise, and a shared repertoire, creating discontinuities between insiders and outsiders (Wenger, 1998). Boundaries separate both professions (e.g., nurses, physicians, and pharmacists) and organizations (e.g., nursing homes, home-based care, GP offices, and hospitals). Collaborative work is shaped by the boundaries between professional groups and levels of care as well as the artifacts and interactions that mediate knowledge (Figure 1). Illustration of organizational and professional boundaries in this study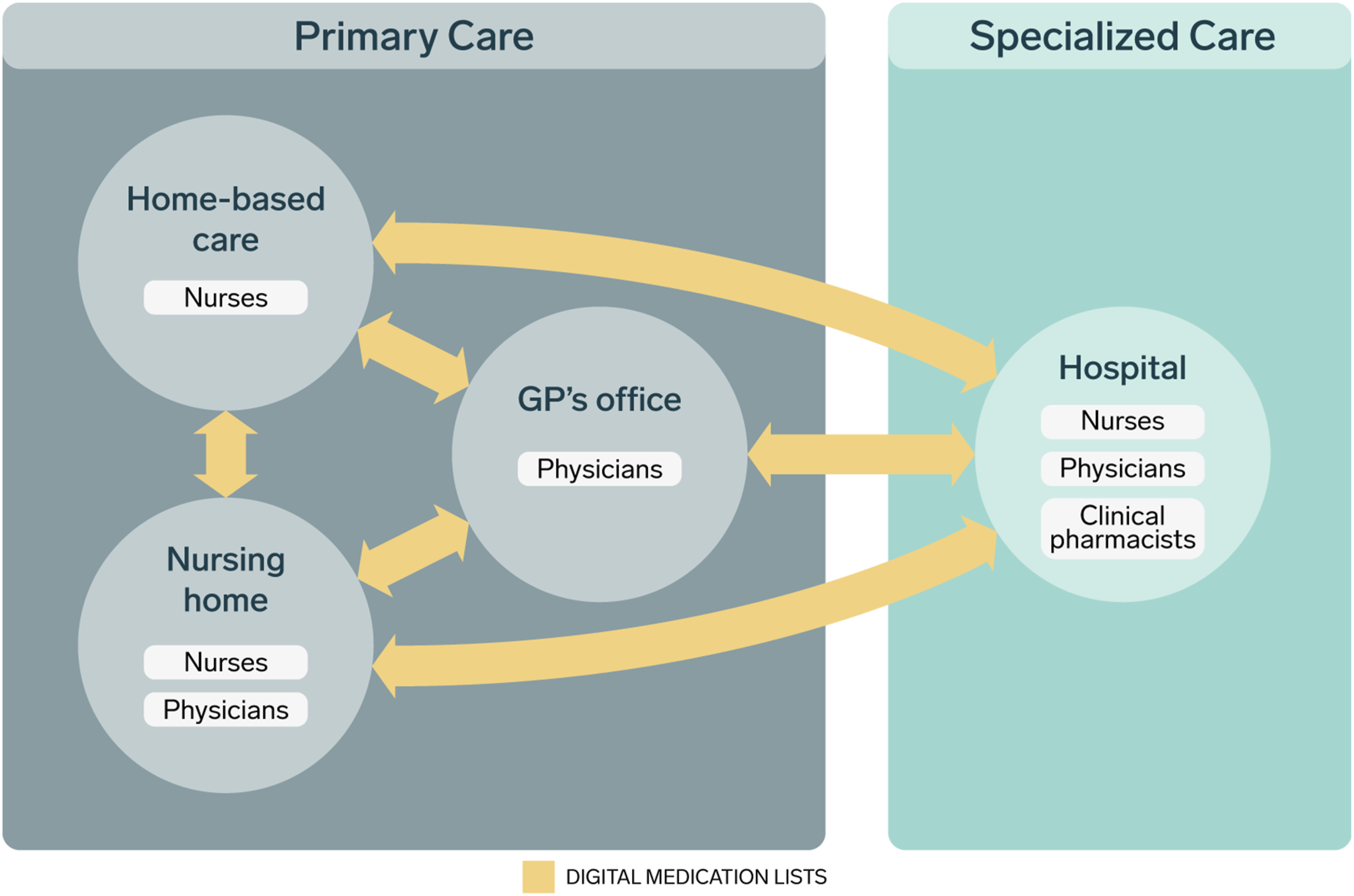
While boundaries separate professions and organizations, tools and language may connect them (Wenger, 1998, 2000). Within practice boundaries, actors produce artifacts—for example, IT systems that mediate medication lists—that are useful means to organize collaboration within the practice (Wenger, 2000). When tools enable alignment by providing a shared reference point for collaboration across practices, they are considered boundary objects: “artifacts, documents, terms, concepts, and other forms of reification around which communities of practice can organize their interconnections” (Wenger, 1998, p. 105). In this article, medication lists are considered boundary objects, as they mediate patients’ medication use and facilitate coordination and alignment across boundaries.
Boundary encounters are interactions between two or more members of separate practice boundaries, often unfolding through discourse where a matter is being negotiated (Wenger, 1998, 2000). Discourse refers to a mutually intelligible “common language” which enables communication and negotiation across practices (Wenger, 2000). In this article, discourse refers to the talk professionals use to negotiate the contents of medication lists and the division of responsibilities in medication information coordination. In boundary encounters, boundary objects and discourses are central to mediating knowledge and to negotiating and aligning meaning. By anchoring participation around shared objects and coordinating action through language, they also support learning-in-practice (Wenger, 1998, 2000).
Collaboration and Competition in Boundary Work
Boundary work is “purposeful individual and collective effort to influence the social, symbolic, material, or temporal boundaries (…) affecting groups, occupations and organizations” (Langley et al., 2019, p. 704). Initially introduced to show how scientists demarcate science from non-science (Gieryn, 1983), boundary work has expanded to capture professions and organizations more generally.
In healthcare, boundary work studies have illustrated how health professionals both compete and collaborate across boundaries through various strategies (Allen, 2000; Apesoa-Varano, 2013; Cain et al., 2021; Conn et al., 2016; Farchi et al., 2023; Ingebrigtsen & Warth, 2025; Johannessen, 2018; Mannsåker et al., 2022; Meier, 2015; Omori et al., 2019; van Muijden et al., 2025; Weber et al., 2022). For example, contextual constraints may facilitate collaboration across boundaries to ensure appropriate patient treatment (Apesoa-Varano, 2013), but they can also lead health professionals to limit rather than expand or protect jurisdiction by defending micro-strategies (Weber et al., 2022).
Building on an extensive literature review on boundary work, Langley et al. (2019) provide a framework that captures both collaborative and competitive strategies among professionals. Competitive boundary work involves distinguishing one’s professional contributions as superior to those of others to gain an advantage. Professionals may defend their boundaries discursively (highlighting differences in contributions) or through practice (various strategies to express resistance to other professional groups), protecting and potentially extending established jurisdictions. Furthermore, they may contest existing boundaries by challenging established jurisdictions (Langley et al., 2019, p. 712).
Collaborative boundary work, in contrast, involves efforts to enable collaboration across professional boundaries (Langley et al., 2019). Professionals negotiate boundaries through workplace interactions and conversations, which are often underpinned by tensions even as they enable collaborative work. Professionals may also downplay boundaries by minimizing distinctions between them to foster collaboration, ensuring work gets done in high-pressure environments.
This study introduces “dirty work” (Hughes, 1958) in the approach of boundary work. “Dirty work” refers to tasks perceived as undesirable yet essential, in which taking on such tasks entails proximity to physical or moral impurity (Galazka & Wallace, 2023), and may be followed by stigmatization of the worker (Galazka & Wallace, 2023; Simpson et al., 2012). Workers may develop strategies to mitigate stigmatization, such as delegating dirty work tasks to other groups (Simpson et al., 2012; Swan, 2012), and is therefore tied to boundary work. We show how health professionals, through boundary work, construct coordination of medication information as “dirty”—not due to impurity (Galazka & Wallace, 2023) but because of its complexity and time-demanding nature.
Methods
Data Collection
This study employed a qualitative ethnographic approach using negotiated interactive observation (Wind, 2008) and in-depth interviews. Data were collected between May and December 2023 and included 145 hours of observation and 24 in-depth interviews with 25 informants (23 individual and one paired interview) across two GP offices, four nursing homes (48 hours), two home-based care facilities (47 hours), and two hospitals (50 hours).
As this study is part of a larger project, data collection was carried out in collaboration with a colleague. This collaboration enabled the collection of extensive observational data and fostered in-depth discussions. Some situations were observed jointly, while others were observed independently. In the joint observations, our separate field notes provided complementary accounts that, when combined, yielded a fuller description of the same situation.
The first author began data collection by observing medication-related tasks, such as prescribing, preparing, double-checking, and administering medications. Over time, practices of collecting, evaluating, and sharing medication information stood out due to their centrality in organizational collaboration and the use of digital tools. These practices included clinical pharmacists’ and physicians’ reconciliation of medication lists, nurses assisting in the sharing of medication information, nurses in home-based care receiving and managing information from other care levels, and GPs’ sharing and updating of medication lists. Health professionals often problematized the digital tools involved in these work tasks. Consequently, this work was selected as a case to investigate the complex sociocultural practices of coordination across levels of care.
The observations provided insights into the situated practices and interactions of health professionals (Creswell & Creswell, 2018). Observational data were recorded as detailed field notes (Nicholls et al., 2014), capturing contextual details such as locations, times, work activities, and the professions present, as well as accounts of what was seen and heard. These notes were predominantly descriptive; analytic insights were recorded separately to maintain rigor. Subsequently, the preliminary field notes were processed into full field notes in Word for analysis.
Semi-structured interviews were conducted to complement the observations by exploring informants’ accounts of their experiences and reflections (Silverman, 2020). The interviews lasted approximately 50 minutes and involved health professionals from various disciplines and levels of care, including resident physicians (n = 1), nursing home physicians (n = 3), GPs (n = 3), clinical pharmacists (n = 4), nurses (n = 12), and head nurses (n = 2). Informants were asked about their work with medications, collaboration both within and across institutions, tools used for coordination of medication information, and perceived challenges and opportunities.
Data Analysis
The data were analyzed using thematic analysis—a six-step method for identifying, organizing, and gaining insight into patterns of meaning (“themes”) in qualitative data (Braun & Clarke, 2012). The first author combined inductive coding with deductive coding. Inductive coding allowed for the emergence of new insights beyond theoretical presumptions. Deductive coding was guided by the boundary work framework (Langley et al., 2019) to capture complex workplace dynamics involving both professionals and organizations (Fehsenfeld et al., 2024).
The first author began the analysis with familiarization through repeated readings of the data, followed by systematic coding in NVivo (version 14) and in physical clustering (“wall mapping”). In NVivo, data were coded as either collaborative or competitive boundary work, in addition to some inductive codes (e.g., lacking resources, strategies to get in touch with other levels of care, and language as a challenge). During wall mapping, the coded data from NVivo were printed and, after careful analysis, organized into six subthemes representing different strategies for coordination work. In this process, inductive codes that aligned with these subthemes were incorporated, whereas inductive codes that remained standalone were discarded.
The remaining codes were then organized into initial themes, initially labelled “competitive boundary work” and “collaborative boundary work” before they were iteratively reviewed and refined. During this process, both main themes and subthemes were renamed, merged, and split, while others were reverted to codes or discarded if they lacked sufficient empirical support. The first author then defined the final themes, clarifying what each theme contributed to the analysis before producing the report. Throughout the process, the two authors engaged in discussions to ensure analytical rigor. Thematic analysis is not linear, but iterative (Braun & Clarke, 2012). Consequently, the first author moved back and forth between the steps.
The analysis produced two main themes: (1) constructing dirty work tasks and (2) cleaning up medication lists. The themes do not refer to specific work tasks but capture different patterns and strategies of situated practices through which boundary work in the coordination of medication information is enacted. The first theme primarily reflects competitive boundary work (explored through the subthemes of disengaging from the coordination of medication information and opposing established responsibilities), culminating in the construction of the coordination of medication information as “dirty work.” A transitional subtheme, taking over delegated coordination work, bridges the two main themes: physicians delegate coordination-related tasks to other professionals (competitive boundary work), while nurses and pharmacists enact the work required for safer coordination (collaborative boundary work). The second theme captures collaborative boundary work and safeguarding practices that foster coordination both within and across levels of care by requesting information (obtaining missing or uncertain medication information) and both correcting (identifying, communicating about, and resolving medication discrepancies) and preventing medication discrepancies (anticipatory practices oriented toward avoiding future misalignment of medication lists). Together, these themes illuminate the diverse strategies health professionals employ in the coordination of medication information.
Reflexivity
As a first-time researcher and PhD candidate, the first author approached the study with a novice perspective, unencumbered by prior experience in health services research. This position facilitated an open approach to the field, allowing for exploration of work practices with few preconceived notions. However, the lack of experience also posed initial challenges, such as interview techniques and focusing observations. To address these challenges, the first author engaged in continuous reflexivity throughout the process, including separate documentation of descriptive and analytic thoughts in field notes and regular discussions with the co-author, who has extensive experience in qualitative research. These practices ensured that the first author’s position as a novice researcher contributed to, rather than constrained, the depth and quality of the data.
Ethical Considerations
Ethical approval was obtained from the Norwegian Agency for Shared Services in Education and Research (ID: 117489) and the data protection officers of the participating hospitals (ID: 3791-3791, ID: 313244). The study followed their ethical standards for informed consent, confidentiality, and data management. In the municipal healthcare services, institutional leaders approved the study. All participants received detailed information about the study and provided informed consent. Written consent was obtained for interviews, while verbal consent was given for observations. The participants were informed of their right to withdraw consent. To ensure confidentiality, all personal identifiers have been anonymized in this article. All quotations were translated from Norwegian to English by the first author, and occupational titles were standardized to US usage.
Findings and Analysis
Interpreted within a sociocultural perspective, the coordination of medication information appears as situated practices, in which artifacts and discourse mediate knowledge in everyday interactions across practice boundaries (Gherardi & Nicolini, 2000; Wenger, 1998, 2000). Coordination is not static but continuously shaped and renegotiated through the challenges and demands of everyday work. Health professionals across levels of care engage in both competitive and collaborative efforts, wherein “dirty work” (Galazka & Wallace, 2023; Hughes, 1958) is constructed and medication lists are cleaned up.
Constructing Dirty Work Tasks
When coordinating medication information, health professionals employed competitive boundary work strategies (Langley et al., 2019) by shifting responsibilities onto other professions and levels of care. These strategies included disengaging from the coordination of medication information, opposing established responsibilities, and delegating coordination tasks to hierarchically lower professional groups and levels of care who take over coordination work.
Disengaging From Coordination of Medication Information
A recurring theme in the empirical material was that hospital physicians distanced themselves from jurisdiction over the coordination of medication information, creating competitive responses from other health professionals. Although the physicians themselves did not explicitly mention this, it was frequently raised by other health professionals across levels of care. The latter often had the impression that physicians did not perform medication reconciliation sufficiently and relied on outdated sources. This practice led to inaccuracies and uncertainty in medication lists that other professional groups were ultimately tasked with cleaning up: Typically, we get the impression that they [hospital physicians] didn’t really reconcile [the list] when the patient was admitted. They simply based the reconciliation on an old discharge summary stored in their system (…). Then we can see that things have been done in the meantime [between the two hospital stays], which have not been considered [by physicians], for example, medications that have been discontinued or prescribed. Then we must untangle that. (…). And we file incident reports upon incident reports. But it never gets better. (Interview, nursing home physician 1)
The nursing home physician explained that hospital physicians left critical information sources unexplored, and that nursing home physicians had to clean up the list. The health professionals in the nursing home had tried to formally address this issue by filing incident reports, but they were unsuccessful. The physicians’ failure to provide complete medication information can be interpreted as a competitive boundary work strategy (Langley et al., 2019) of defending professional boundaries, whereby physicians disengage from responsibilities in coordination of medication information and “pass the buck” onto other professions and other levels of care. Here, the digitally mediated boundary objects (Wenger, 1998, 2000) are not neutral: the absence of a shared, trusted artifact ultimately shifts the burden onto others and triggers boundary negotiations. Through this strategy, hospital physicians signaled that the coordination of medication information was undesirable work. In turn, these processes emerged as “dirty work” (Galazka & Wallace, 2023; Hughes, 1958), which other health professionals had to solve by investigating discrepancies that ideally should have already been resolved during the hospital stay. Although many informants largely considered physicians’ coordination of medication information to be inadequate—even sloppy—the resident physicians themselves emphasized structural challenges: I am in the emergency department with a resident physician. (…) He tells me that he has little or no contact with the GP, as getting in touch with them takes too much time. Sometimes, they [physicians] must wait for the electronic message from municipalities, and in these instances, they reconcile to the best of their ability, and someone in the hospital ward must double-check the medication lists after the electronic message arrives. (…). He tells me that they are lucky to have clinical pharmacists working at the hospital wards, as they can double-check the reconciliation. (…). Only acute issues are addressed in the emergency department. (Field notes, hospital)
The resident physician emphasized structural challenges in medication reconciliation, such as a lack of time and delayed medication lists, as a reason for incomplete reconciliation in the emergency department. This highlights how the digital systems for sharing of boundary objects can fail to align perspectives between municipalities and hospitals, leaving physicians without a complete understanding of patients’ medication use and hindering coordination. Delays in the sharing of boundary objects reconfigure interactional patterns and, over time, may shift divisions of responsibilities. Whether this boundary work was an intentional competitive strategy or a response to structural hindrance, it inevitably created challenges that had to be navigated by other health professionals, such as nurses and clinical pharmacists.
Similar challenges were present within hospitals when medication lists were prepared for discharge. Resident physicians prepared discharge summaries that had to be formally approved by attending physicians, which could take several days. In the meantime, nurses stepped in to ensure that medication lists were shared. Observations revealed how nurses responded to physicians’ disengagement: We are sitting in the break room in the hospital ward with several nurses and certified nursing assistants. Two of the nurses are working on a computer within the EHR. They are talking about a digital medication list that they are supposed to copy from the EHR into the electronic messaging system [to municipalities] but say that it will be very difficult to read and understand, as the medication list is messy. A physician has written the discharge summary, including the medication list, but it is not “tidy,” according to the nurses. (…). They say that they filed an incident report on the physicians yesterday. The physician created a new list after this, but this one is incorrect, too, according to the nurses. One of the nurses decides that she will send it as is after a few minor improvements and that the physician in the municipality will have to tidy the list up. She says that going through the medications of patients who are ready for discharge is not the nurses’ responsibility; it’s the physicians’ job. She is clearly frustrated. (Field notes, hospital)
In this case, nurses were tired of cleaning up the mess left by resident physicians in the medication list. After filing incident reports without seeing results, they decided not to exceed their professional responsibility and instead sent the medication list as it was. Furthermore, the nurse explicitly stated that this task was not a nursing responsibility; hence, they used discourse as a tool to reestablish their professional boundaries (Wenger, 2000). This competitive boundary work strategy reflects resistance: nurses protected their time and limited their jurisdiction by disengaging from coordination work, and they forwarded the messy boundary object. By refusing to take on additional tasks, they passed the “dirty work” to the next link, shifting the burden to others. For instance, a nursing home physician explained how they navigated incomplete or missing medication lists from hospitals: The hospital is required to send an updated discharge report that follows every patient admitted to our facility. There we can find the [medication] list, and we are very consistent that if the discharge summary with an updated medication list is not included and finished, we will not admit the patient. We are quite strict about that. (Interview, nursing home physician 3)
The health professionals working in the nursing home protected themselves against the mess of insufficient coordination: they were not willing to go beyond their boundary-specific responsibility and instead demanded that the hospital deliver a complete and accurate medication list upon admittance. This appeared to be an effective negotiation strategy, where hospital staff met their demands. A hospital nurse said, “We must send an electronic medication list to them [municipal health services], before the patient leaves the hospital. (…). And that is done because it has to be done, or else … They won’t admit the patient” (Interview, hospital nurse 4).
By setting clear boundaries and establishing consequences, the nursing home pushed the hospital to provide the required medication information. These dynamics make visible how jurisdiction is enacted in practice, as boundaries are redrawn through discursive negotiations of boundary objects across levels of care. Negotiating the content and the structure of the boundary object led to the negotiation of divisions of responsibility as well. This illustrates how defending boundaries can function as a collaborative negotiation strategy and how negotiations are underpinned by power relations and tensions that affect how they play out (Langley et al., 2019).
Opposing Established Responsibilities
Where hospital physicians disengaged by performing their responsibilities inadequately, GPs negotiated their role in medication coordination in other ways. GPs have a legal responsibility to coordinate medication information, and the informants expressed that they experienced immense pressure: The GP Regulation states that the GP should act as the coordinating link between different parts of the healthcare service. So, specifically, when it comes to medications, this is quite an important task. (…). When you are centrally positioned in the middle of the healthcare system, you find yourself in the midst of an information flood, and it’s not always easy. There is a lot of chaos at times. (Interview, GP 1)
The GP quoted above found it challenging to coordinate medication information because it involved navigating many incoming digitally mediated artifacts—some with and some without medication information—from various levels of care. This “chaos” rendered the task disorganized. Managing digitally mediated medication lists from multiple sources was challenging, as explained by another GP: People often consider it the GPs’ responsibility to have a complete overview of the medication list (…). If other physicians in other institutions have added or discontinued something, we are supposed to make sure that it is right. That is completely wrong, it’s not possible (…). As GPs, we do not have responsibility over the medication list before the patient comes to us for a consultation. (…) Sometimes, if they [nurses from home-based care] say, “Your list is not the same as the one we got,” then I suppose there are other physicians in the picture. And then I think, “(…) the patient hasn’t been in my office for three months; then it is my right to say that the patient is supposed to use the medications in my list.” I don’t have any other information. And then I write back: “This is the list.” Then I get a warning in return that I must tidy up the list soon, or else … What they are asking me to tidy up is things I don’t know anything about. (…). This is a weakness in coordination; it’s been there the whole time, and there is an arrogance over (…) the GPs’ situation. (Interview, GP 2)
This GP expressed resistance to the professional boundaries through both discourse and practice, attempting to make other health professionals understand that the GPs’ responsibilities were unrealistic. The GP engaged in competitive boundary work by contesting the GP’s jurisdiction and rejecting the responsibility ascribed to the role. Thereby, the interviewee sought to shift responsibility for coordinating medication information by displacing the work onto other levels of care. This situation illustrates how responsibility for the medication list is continuously negotiated in interactions, especially when artifacts provide partial or conflicting versions of patients’ medications. In theoretical terms, boundary objects that are supposed to align perspectives across organizational boundaries can fail in their purpose, or only partially succeed (Wenger, 1998), requiring health professionals to correct them.
Taking Over Delegated Coordination Work
While the first subtheme addressed health professionals’ competitive disengagement and responses to this disengagement, this subtheme entails the collaborative responses. To enable the coordination across levels of care, other health professionals stepped in when physicians disengaged or were otherwise unavailable. Clinical pharmacists, for example, participated in medication reconciliation in emergency departments to alleviate resident physicians’ workload. In nursing homes, nurses stepped in in other ways: They [the patients] may arrive in the evening, and then there are usually just two nurses here. We must print out a new [medication] list, and then two nurses go through the list, and then we are allowed to sign. (Interview, nursing home nurse 3)
Nurses frequently created medication lists upon admission, as physicians were often unavailable. This illustrates a more general theme of how other health professionals step in to support workflow and safety when physicians “let go” or disengage from their jurisdictions and delegate coordination tasks. The task is renegotiated and re-enacted through interactions. Boundaries were reconfigured as nurses took on responsibilities traditionally belonging to physicians to enable admission and the construction of a medication list, when necessary. Health professionals exceeded their responsibilities further by investigating possible medication discrepancies, as explained by a hospital nurse: It happens that … we bring medications, because that’s what the medication chart states, and then they [patients] tell us “No, I don’t take this one anymore,” or “this is the wrong dosage.” For those who are aware of it. And then we must alert the physician, that “he says he doesn’t use this one” (…). But we don’t … have any authority to change any medications (…). We can help the physicians (…). But it is their responsibility to ensure that the medication list is correct. (…). Of course, we can help them to be nice. (…). We may call the home-based care (…) and [ask]: What is the correct medication? (Interview, hospital nurse 3)
Nurses supported physicians by going the extra mile to establish accurate medication lists, taking on coordination work that extended beyond their professional boundaries. Here, the cell phone could function as an artifact facilitating boundary encounters (Wenger, 1998), enabling discourse and negotiations of the medication list across sites. By downplaying professional boundaries and jurisdiction, nurses enacted coordination practices that enabled collaboration and continuity of care, despite lacking formal responsibility.
These practices, while analytically approached as collaborative, are underpinned by power dynamics that affect how they unfold (Langley et al., 2019). Nurses’ and clinical pharmacists’ willingness to take on coordination work does not necessarily reflect an expansion of formal jurisdiction but rather a response to gaps in responsibility and availability. When physicians disengage from work tasks, and these work tasks are allocated to hierarchically lower groups, coordination practices are further constructed as “dirty work” (Galazka & Wallace, 2023; Hughes, 1958) emerges.
Cleaning Up Medication Lists
Building on a sociocultural perspective, this theme captures how professionals work together to ensure accurate and up-to-date medication information. Health professionals employ collaborative boundary work strategies (Langley et al., 2019) to “clean up” medication lists and enable the sharing of accurate medication information across organizational boundaries. This work involves organizing, sharing, and validating—or adjusting—medication lists across care levels until they are aligned. The subthemes describe distinct yet interrelated practices involved in this work: requesting information, correcting medication discrepancies, and preventing medication discrepancies.
Requesting Information
When health professionals encountered missing information, inconsistencies, or potential errors in medication lists from other levels of care, they were prevented from constructing an accurate medication list independently. Instead, they negotiated the contents of medication lists by contacting colleagues across levels of care, by phone or through electronic messages, to address potential inaccuracies: A nurse in home-based care is in the office managing incoming electronic messages from other levels of care. (…). The nurse sees that patients have been discharged from the hospital (…). When the nurse looks at the [medication] lists, she comments that many changes have been made [during the stay], which are not marked as changes. There are also “illogical” changes. She tells me that she must call the hospital and ask or send an electronic message to the GP. (Field notes, home-based care)
The nurse took measures to clarify the received medication information by using the available tools to communicate with health professionals at other levels of care. The nurse initiated digitally mediated boundary encounters through artifacts (cellphone/electronic messaging system), using discourse to negotiate the content of the medication list and achieve accuracy and alignment across levels of care (Wenger, 1998, 2000). By doing so, the nurse bridged the apparent information gap across the organizational boundaries. Once contact was established, health professionals engaged in negotiation strategies to restore a shared understanding of the medication list: In the emergency department, we must frequently call them [municipal care] and request an electronic message [with a medication list] to reconcile the medication. This is usually because they haven’t had the time to send it yet. (…). Sometimes, to speed things up, I ask them to read aloud what’s in the electronic message, and then they ensure it [the medication list] gets sent later that day. (…). Then it’s very efficient, where they may say, “Paracetamol three times a day, morning, noon, evening,” and I can check off, “Yes, that matches what I had on my list.” (…). Of course, it would be easier if the electronic message was just there from the start. But I understand that if it’s home-based care, they might be out visiting other patients, and it … takes some time. (Interview, clinical pharmacist 1, hospital)
The clinical pharmacist contacted municipal care because the hospital had not yet received medication information from them. Here, the negotiation strategies involved not only requesting the sharing of the medication list but also relying on discourse to secure a verbal report as a temporary solution until the boundary object became available in the electronic system. Health professionals in municipal care collaborated by sharing the information in the requested format. This collaborative strategy is a workaround when delays in digital information-sharing hinder coordination of medication information, in contrast to the disengagement strategies observed among some resident physicians in similar situations.
Correcting Medication Discrepancies
Another strategy was to correct the medication list when discrepancies arose. Nurses and clinical pharmacists emerged as the primary professions taking on these tasks. For example, one clinical pharmacist, who double-checked the reconciliation performed by resident physicians, described an instance where multiple health professionals collaborated across levels of care to correct discrepancies in a medication list: I had a case where a GP admitted a patient and sent us a [medication] list. But the home-based care provided a different list. It turned out that the GP had the most correct and up-to-date list. But the medication list was created and reconciled with [the list from] the home-based care. Because (…) one thinks that home-based care is always correct. But we managed to sort it out because I reviewed everything and let them know that the lists didn’t match up. In the end, the GP tidied it up, really. That’s how it was resolved. And I discovered the issue because of the SCR. I could see what medications had been dispensed. And it didn’t quite match anything that was in front of me in terms of the reconciled [medication] lists. (Interview, clinical pharmacist 3, hospital)
The clinical pharmacist identified discrepancies between the two medication lists, contacted health professionals in both institutions, and alerted them to the issue through discourse. The information in the digital medication lists from home-based care and the GP was unaligned, and the medication lists as boundary objects failed to mediate knowledge in a meaningful way. However, the clinical pharmacist employed collaborative boundary work by using the SCR to uncover the discrepancies and initiating negotiation processes across practice boundaries. Here, the SCR functioned as a mediating artifact that facilitated realignment across practices in combination with discourse between health professionals across levels of care, underscoring the importance of thorough coordination of medication information and the potential of digital tools in identifying discrepancies.
Preventing Medication Discrepancies
While most negotiations occurred across levels of care, negotiation of professional boundaries also took place within institutions, when health professionals sought to ensure that the information they shared with other levels of care was clear and accurate. Physicians used to have sole responsibility for writing the discharge report; however, nurses and certified nursing assistants have taken over parts of these tasks. This change resulted in further negotiations as nurses navigated challenges in sharing medication information with other levels of care upon discharge: We essentially copy and paste that part [the medication list] of the discharge summary from the physician, so that once it has been approved, we include it in our report. This ensures that home-based care and the nursing homes receive an updated medication list. (…). We’re supposed to wait [with copying the medication list from the discharge summary] until it’s been [officially] approved, unless the physician is busy and tells us, “I am done with it [the discharge summary], I just haven’t had the chance to approve it yet.” (…), if we know that it is completely done and there will be no changes, then we can do it. But ideally, we should wait until the document has been approved. (Interview, hospital nurse 1)
As discharge summaries had to be approved by an attending physician due to the formal division of labor, it could take several days before medication lists were ready to be sent out because of high work pressure. Hence, nurses and resident physicians relied on discourse to negotiate workarounds, allowing nurses to share medication lists after approval from physicians to ensure that crucial medication information was sent out. These practices highlight how health professionals actively took measures to prevent discrepancies in the first place. In another example, home-based care received these nursing reports and discharge summaries from hospitals: I’ve experienced cases where something is missing from the nursing [report]… (…). Then they [patients] come back home with additional medications (…). If a patient comes home [from the hospital], and they have a [physical copy of a] discharge summary, I always take it with me to the office to check that it matches the nursing report. (Interview, home-based care nurse 3)
Despite preventive work by hospital nurses to ensure the correct medication information was shared, changes to medication lists were still made after the nurses sent information to other levels of care, creating challenges that had to be navigated by others. The nurse in this example could not blindly trust medication lists in nursing reports and therefore always double-checked them against discharge summaries. This example highlights how preventive work, such as consistently double-checking sources, serves as a safeguard to catch potential discrepancies early, preventing them from impacting patient care. Across these cases, coordination of medication information appears not as a matter of simple transfers but as the ongoing, situated, and negotiated production of medication lists through interactions and the use of artifacts (Gherardi & Nicolini, 2000; Wenger, 1998, 2000).
Discussion
The findings show that health professionals coordinate medication information across care levels through situated work, in which they negotiate medication list contents and professional responsibility in boundary encounters. In these interactions, health professionals employ both competitive and collaborative boundary work strategies. Digital tools are involved as mediating artifacts that sometimes convey complete information, but oftentimes mediate discrepancies and thereby produce misalignment across practice boundaries.
Although boundary work serves as the primary analytical lens in the findings, the empirical material revealed that these strategies were consistently linked to gaps, misalignments, and redistributions of responsibility. On this basis, the following discussion moves from boundary work to fragmentation as an umbrella concept that captures how these interactional strategies collectively produce and respond to discontinuities in coordination.
Fragmentation Through Structure
The coordination of medication information unfolded within a structurally fragmented healthcare system shaped by organizational specialization and disconnected digital systems. These conditions made it challenging to establish a single, trusted medication list across care levels. Health professionals therefore had to navigate inconsistencies and information gaps both between digital tools and across organizational boundaries when reconstructing medication information.
Where Galazka and Wallace (2023) argue that interactions between clients and workers can both alleviate and reinforce dirty work stigma, this study suggests that interactions between digital tools and health professionals have a similar effect. When functioning as intended, digital medication lists operate as boundary objects that mediate knowledge across practices and support alignment across organizational boundaries (Wenger, 1998), creating a manageable experience of coordination. When tools fail to align perspectives, however, professionals are left with incomplete or unreliable medication information and must bridge these gaps to reconstruct coherence. Such situations intensify experiences of the coordination of medication information as undesirable and contribute to the construction of this work as “dirty.” Fragmented structures thus not only add complexity but also shape how professionals enact coordination through boundary work strategies.
Fragmentation Through Practice
Within these structurally fragmented conditions, health professionals developed strategies to manage coordination work. While coordination ideally depends on collaboration across care levels (Report No. 9 (2023-2024)), the findings show that professionals engaged in boundary work aimed at withdrawing from jurisdiction and transferring responsibility. This contrasts with boundary work literature, which often emphasizes strategies to claim and protect jurisdiction (e.g., Abbott, 1988; Allen, 2000; Ingebrigtsen & Warth, 2025; Langley et al., 2019; Omori et al., 2019). When health professionals disengaged, contested responsibilities, or passed work along—whether intentionally or due to structural constraints—they redistributed responsibilities to other professions and care levels. Such defensive strategies not only redistributed tasks but also contributed to the fragmentation of practice, as coordination work was left incomplete and passed on to others. Competitive boundary work thus became both a symptom and a source of fragmentation in coordination practices.
The findings align with Weber et al. (2022), who showed how contextual constraints led health professionals to limit their responsibilities in patient care. This study extends that knowledge by showing how such strategies interact with digital conditions, fragmenting coordination further. This focus shifts the attention from professional tactics to the systemic consequences of boundary work and demonstrates how competitive boundary work contributes to fragmentation under digital and organizational complexity.
Through these boundary work strategies, medication information coordination emerged as “dirty work” (Galazka & Wallace, 2023)—not for reasons of physical or moral impurity but because of its complex, time-demanding nature under fragmented digital systems and multiple professional perspectives. However, the opportunity to disengage from dirty work tasks depends on resources, which vary with professional background. Swan (2012) shows that middle-class women have the financial means to outsource domestic work to other groups, enabling them to remove their identities from stigmatizing work and build identities as career women. Similarly, the physicians in this study were positioned to delegate undesirable work tasks through professional status, autonomy, and jurisdiction (Abbott, 1988). These resources vary among physicians, however, where especially GPs often carried the burden of resolving discrepancies generated elsewhere. Nurses and clinical pharmacists, as well as physicians in such positions, did not have the same opportunity to disengage and thus sustained this work, revealing how power asymmetries shape the distribution of dirty work.
Mending Fragmentation
While some professionals contributed to fragmentation, others worked to restore alignment across practice boundaries. This collaborative work was characterized by safeguarding practices, in which health professionals sought to clean up and align medication lists and create continuity across care levels. Health professionals enabled coordination by exceeding formal responsibilities, requesting missing medication information, and correcting and preventing medication discrepancies, despite fragmentation.
Collaboration involved sharing and negotiating medication information across professional and organizational boundaries and downplaying professional boundaries in pursuit of a joint enterprise (Wenger, 1998). This aligns with research illustrating the collaborative efforts of health professionals (e.g., boundary blurring and humility strategies) (Ingebrigtsen & Warth, 2025; Johannessen, 2018) and demonstrates that communication strategies mitigating boundaries may result in enhanced experiences of collaboration (Conn et al., 2016). Such efforts temporarily mended fragmentation, but also revealed how coordination is dependent on the continuous efforts and negotiations of health professionals. Similar patterns appear in hospital settings, where Ellingsen et al. (2024) describe work practices to maintain reliable medication lists as collective repair work, although the present study shows that such efforts also extend across organizational boundaries.
Implications: Holding the Fragmented Systems Together
The findings imply that coordination cannot be reduced to purely technical or procedural tasks. Rather, coordination unfolds through participation in everyday work, where meaning is negotiated rather than merely executed. Coordination should therefore be recognized as relational work dependent on negotiation, mutual understanding, and alignment across practice boundaries, where meaning is established through interaction. This sociocultural perspective shifts the focus from digitalization and standardization (Report No. 9 (2023-2024)) toward supporting the conditions that enable coordination in practice, particularly the boundary work carried out by health professionals.
Across levels of care, coordination is mediated by digital tools for information-sharing intended to support work practices. However, as shown here and elsewhere (Ellingsen et al., 2024; Hertzum & Ellingsen, 2023; Nybakke, 2025), it is the compensatory boundary work of health professionals that truly enables coordination. While digital tools aim to bridge practices, they often introduce new complexities that necessitate boundary work. Digital tools thus both support and depend on the situated practices they seek to replace, expanding our understanding of how boundary work unfolds in increasingly digitized healthcare settings.
This highlights the limitations of current digital systems, which should ideally reduce the need for such work but often add complexity. If the Shared Medication List functions as intended, it could simplify the coordination of medication information and reduce direct interactions between health professionals across levels of care. To do so, however, it must be adapted to work practices rather than introducing additional complexity. At the same time, transfers of care serve as important checkpoints for ensuring accuracy in medication lists (Hertzum & Ellingsen, 2023; Nybakke, 2025). Reducing opportunities to evaluate and negotiate medication information may remove crucial moments for identifying and repairing medication discrepancies. Ultimately, coherence in medication information is maintained through these continuous, situated efforts.
Limitations
Although this study used extensive ethnographic data, recruiting hospital physicians proved challenging. The limited participation of this group may have led to an overly critical portrayal of their contributions in coordination work, as their perspectives were underrepresented. The authors nevertheless sought to nuance this representation through careful interpretation and inclusion of physicians’ perspectives despite the limited data.
The study aimed to explore coordination across institutions, but it was not possible to observe the same interactions from multiple organizational sites simultaneously. Consequently, some interactions could not be observed, as the researchers were only present in one of the involved institutions at the time.
Finally, as the focus was on health professionals’ work practices, patients were not included. This design enabled a detailed exploration of the coordination of medication information across care levels, but it left out the patient perspective. Future studies could extend these findings by including patients who also mediate medication information in transitions of care.
Footnotes
Acknowledgements
We would like to extend our gratitude to the institutions and health professionals who participated in the study. We also acknowledge the Research Council of Norway for funding the project. Finally, we thank the graphic designer at the Norwegian Centre for e-Health Research, Jarl-Stian Olsen, for visual assistance with ![]() .
.
Ethical Considerations
Ethical approval was obtained from the Norwegian Agency for Shared Services in Education and Research (ID: 117489) and the data protection officers of both participating hospitals (ID: 3791-3791 and ID: 313244). The study adhered to their ethical standards, including informed consent, confidentiality, and proper data management. In the municipal healthcare services, institutional leaders approved the study and facilitated field access and the recruitment of informants.
Consent to Participate
All participants received detailed information about the study and provided informed consent. Written consent was obtained for interviews, while verbal consent was given for observations. The participants were informed of their right to withdraw at any time. To ensure confidentiality, all personal identifiers have been anonymized in this article.
Author Contributions
Stine Agnete Ingebrigtsen developed and detailed the study within an existing project framework; operationalized the design and methodological approach; recruited informants; conducted all data collection; performed data analysis; drafted the initial manuscript; and carried out revisions throughout the process. Line Lundvoll Warth established the overarching project, topic, and methodological framework; contributed to conceptual development and theoretical direction throughout the study; contributed extensively to the development of the introduction; provided language editing and critical revisions (feedback on argumentation, structure, theoretical clarity, and interpretation of findings); and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Research Council of Norway (Grant Number: HELSEVEL 314382).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.